
Abstract
Although primary surgery for cleft lip has improved over time, the degree of secondary cleft or nasal deformity reportedly varies from a minimum degree to a remarkable degree. Patients with cleft often worry about residual nose deformity, such as a displaced columella, a broad nasal floor, and a deviation of the alar base on the cleft side. Some of the factors that occur in association with secondary cleft or nasal deformity include a deviation of the anterior nasal spine, a deflected septum, a deficiency of the orbicularis muscle, and a lack of bone underlying the nose. Secondary cleft and nasal deformity can result from incomplete muscle repair at the primary cleft operation. Therefore, surgeons should manage patients individually and deal with various deformities by performing appropriate surgery on a case-by-case basis. In this report, we applied the simple method of single VY-plasty on the nasal floor to a patient with unilateral cleft to revise the alar base on the cleft side. We adopted this approach to achieve overcorrection on the cleft side during surgery, which helped maintain the appropriate position of the alar base and ultimately balanced the nose foramen at 13 months after the operation. It was also possible to complement the height of the nasal floor without a bone graft. We believe that this approach will prove useful for managing cases with a broad and low nasal floor, thereby enabling the reconstruction of a well-balanced nose.
Introduction
Primary surgery for cleft lip has improved over time. In cases of unilateral cleft lip, the common surgical methods include those reported by Millard and Randall. Therefore, methods including the use of rotation advancement or a triangular flap have been typically performed (Randall, 1959; Millard, 1960). In addition, Fisher has reported the anatomical subunit approximation technique (Fisher, 2005). However, the degree of secondary cleft or nasal deformity reportedly varies from a minimum degree to a remarkable degree. These deformities may appear as such patients with a cleft deformity continue to grow with age. Patients often worry about the presence of a residual nose deformity or asymmetry, such as a displaced columella, broad nasal floor, or deviation of the alar base on the cleft side (Allori and Mulliken, 2017; Bentz, 2016). Some of the factors associated with secondary cleft or nasal deformity include a deviation of the anterior nasal spine, a deflected septum, a deficiency of the orbicularis muscle, and a lack of bone underlying the nose (Krimmel et al., 2011). Secondary cleft and nasal deformity can result from incomplete muscle repair during the primary cleft operation (Bentz, 2016).
The ultimate goal of such surgery is to achieve a symmetrical or balanced lip and nose area. For the revision of alar base displacement, we may need to not only reconstruct the anatomical position but also address any alveolar bone defects and deformities of the orbicularis oris muscle.
We herein report a method of improving nasal deformities in cases of unilateral cleft accompanied a low alar base with lateral displacement and a broad nasal floor.
Case Report
An 18-year-old female with unilateral lip and alveolar cleft underwent primary surgery for cleft lip followed by an alveolar bone graft at another facility. She had been worried about nasal asymmetry, while demonstrating a low alar and the lateral displacement of the alar base and a broad nostril sill on the left side, and thus expressed a desire to improve her nasal deformity.
At 9 months after her muscle repair surgery and alveolar bone graft, the repositioned alar base showed a tendency to drift backward posteriorly (Figure 1). Nasal revision was thus performed using the nasal septal cartilage. This surgery was basically performed using the secondary nasal revision method reported by Nishimura and Ogino (1978). However, her alar base on the cleft side showed lateral displacement, and the nasal floor was broad (Figure 2). A third operation was therefore performed to improve the nasal deformity. Single YV-plasty was performed at the nasal floor, from the alar base to the septum. The important point with this surgery is to perform an excision into the septum and medially advance the V-skin flap to the septum via the nasal floor. Although moving the V-skin flap, Burow’s triangle excision was performed (Figure 3A and B). Following flap transfer, an overcorrection was noted, with the left nasal floor narrower than that on the right (Figure 3A and C). However, this overcorrection was found to have improved at one month after surgery (Figure 4A), and the symmetry of the nose was reconstructed and maintained at 3, 7, and 13 months after the operation (Figure 4B-D). In addition, the height of the nasal floor on the left side became almost the same as that on the right side (Figure 4).
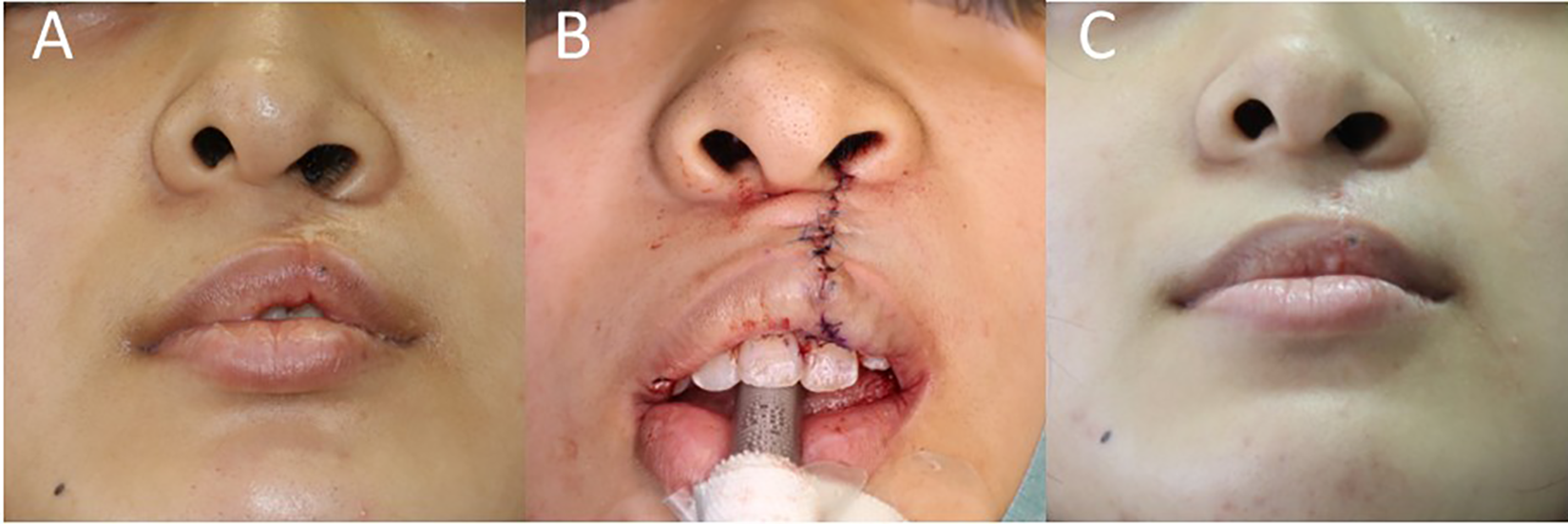
Change in the alar base on the cleft side before and after muscle repair and bone grafting. The repositioned ala base tended to drift backward posteriorly. Preoperative (A), intraoperative (B), and postoperative (at 9 months after the operation).

Preoperative photographs. The nasal cavity was broad, the alar basement was displaced outwardly, and the nasal floor was low on the left cleft side.
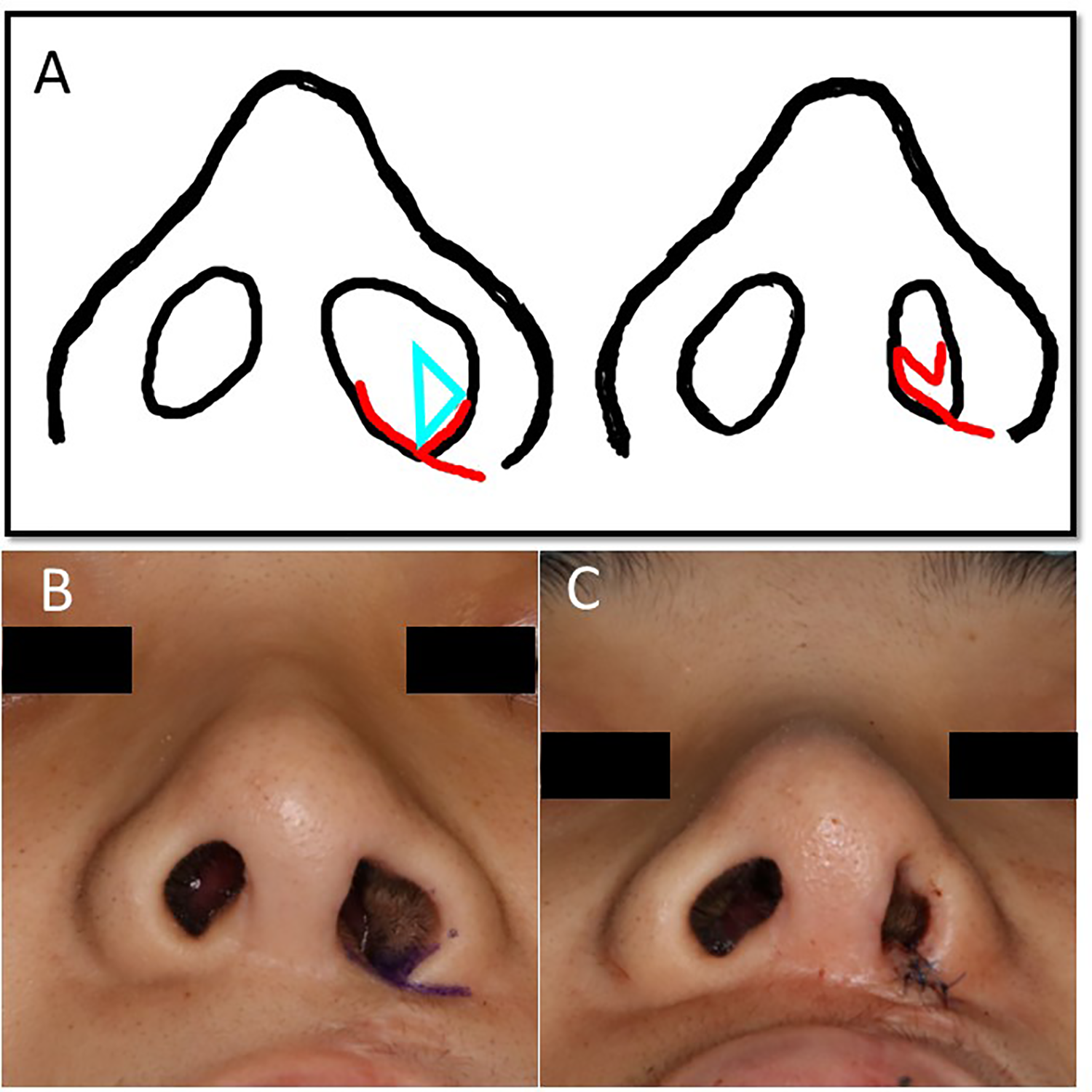
A schematic drawing of the procedure and intraoperative photographs. The design of YV-plasty from the alar base to the septum. The blue triangle indicates Burow’s triangle for excision (A left). The state after YV-plasty. V-skin flap is advanced to septum via nasal floor excising excision of Burow’s triangle. The nasal cavity remained narrow on the left cleft side due to an overcorrection (A right). Photographs before (B) and after (C) YV-plasty.
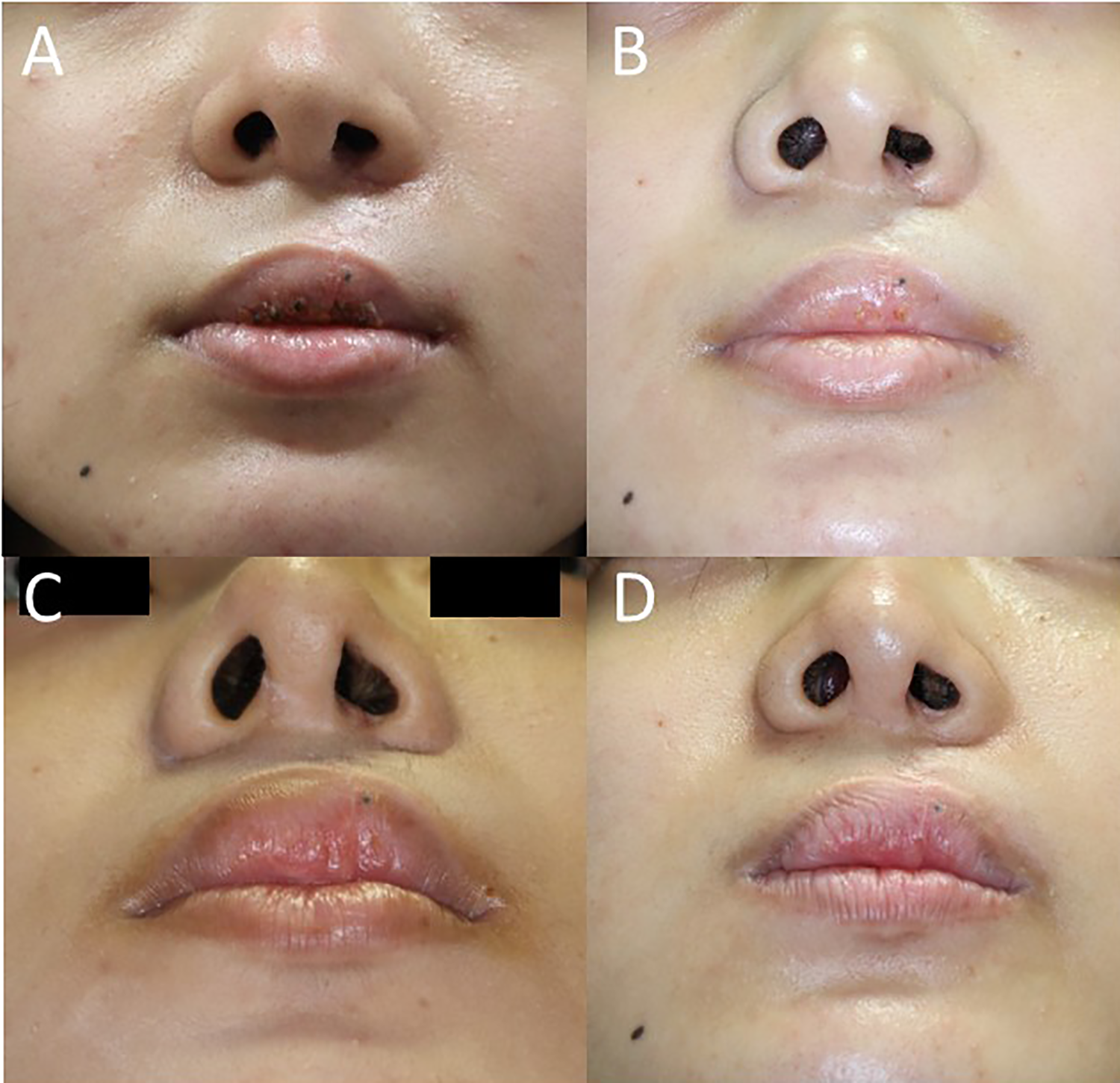
Postoperative photographs. A good balance and appearance were maintained. One month (A), 3 months (B), 7 months (C), and 13 months (D) after operation.
Discussion
Second nasal correction after primary cleft lip surgery should be performed depending on the grade of residual deformity. There are many variations that require minor or major revision, which makes secondary cleft or nasal correction difficult and also causes surgeons to sometimes worry about how best to reconstruct a patient’s facial structure. We must therefore choose the surgical method that best matches each individual patient’s condition.
Secondary revisions may be divided into 2 main approaches: reconstruction with hard tissue and reconstruction with soft tissue. Hard tissue refers to methods using bone or cartilage, wherein the transfer of bone and cartilage is performed to reconstruct the base of the hard tissue to provide support. In contrast, soft tissue revision includes approaches such as Z-plasty for alar base repositioning, Abbe’s flap and muscle repair (Bentz, 2016).
In this report, we needed to do more than simply improve the residual asymmetry with unilateral cleft after nasal revision via cartilage transfer and muscle repair.
A nasal deformity on the cleft side often results from a deficiency of bony support beneath the lip and nose. Bone grafts at the alveolar cleft can elevate the nasal floor, so successful bone formation at the alveolar cleft can improve nasal deformity. However, a low nasal floor may remain due to insufficient soft tissue after undergoing a secondary bone graft on the alveolar cleft. In contrast, a broad nasal floor is attributed to incomplete muscle repair during the primary cleft operation (Bentz, 2016). Secondary orbicularis oris muscle repair is sometimes used to improve alar base displacement and reconstruct the philtrum formation (Onizuka, 1975). The problem is that it is difficult to maintain the nasal position after a surgical operation, so the repositioned alar base tends to drift backward posteriorly (Bentz, 2016). Therefore, a strong overcorrection may be needed in order to prevent the base from slipping back to its original position.
VY-plasty and YV-plasty are common techniques used by plastic surgeons to release skin contracture and complement skin defects. Suzuki proposed the comprehensive classification of VY-plasty with the excision of Burow’s triangle (Suzuki et al., 1996), and some authors have suggested the utility of YV-plasty at the nasal floor to revise the alar base (Allori and Mulliken, 2017; Hamilton, 2014; Kiya et al., 2014). They did not emphasize “overcorrection,” which helped maintain the appropriate position of the alar base and resulted in a balanced nose foramen by 13 months after the operation in the present case. Furthermore, this technique makes it possible to increase the height of the nasal floor without an additional bone graft. The left ala on the cleft side was longer than the right one before revision. We therefore moved the long extra ala to the nasal floor using a V-Y advancement flap.
When we encounter a low nasal floor on the cleft side, we suspect that there might be an alveolar bone deficiency under the nasal floor. However, for appearance purposes, a method to increase the amount of hard tissue with bone or cartilage may not be absolutely necessary. We were able to manage the deficiency of the nasal floor in the present case by using excess alar base tissue to revise the nasal floor. We believe this approach will prove useful for managing cases with a broad and low nasal floor, thereby enabling the reconstruction of a well-balanced nose.
Conclusion
Performing single YV-plasty at the alar base and nasal floor on the cleft side enabled the reconstruction of a well-balanced nose for a unilateral cleft patient. An overcorrection on the cleft side may be helpful maintain the repositioned alar base. In addition, this method has the merit of complementing the nasal floor volume without the need for any additional hard tissue transfer.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.