
Abstract
Background:
Augmentation rhinoplasty with autologous fat grafting is a useful procedure to meet the demand for facial harmonization in the Asian population. We used this procedure during orthognathic surgery to address inadequate dorsum projection. This prospective study was conducted to determine the fat retention rate in patients undergoing simultaneous autologous fat injection augmentation rhinoplasty and orthognathic surgery.
Methods:
Nineteen patients were treated with simultaneous bimaxillary orthognathic surgery and autologous fat grafting of the nasal dorsum and tip. The paired t test was used to compare the nasal volumes before and at least 6 months after surgery measured by 3-dimensional computer tomography scans. All measurements were performed twice by the same evaluator at least 2 weeks apart for intrarater consistency.
Results:
Seventeen patients completed the study. The volume means before and after surgery were 22.3 ± 4.6 cm3 and 23.3 ± 4.7 cm3, respectively, with a mean difference of 1.0 ± 0.3 cm3 (P < .001). The mean retention rate was calculated to be 50.5% ± 7.0% (range: 40.5%-64.7%). Intrarater consistency was high with a Cronbach α of .97 (P < .001) and .98 (P < .001), respectively.
Conclusion:
This prospective study provides objective graft retention measurements for fat injection augmentation rhinoplasty combined with orthognathic surgery. All patients were satisfied with the results and no complications or additional morbidity was noted in the postoperative course. We consider this procedure to be a safe, reliable, and powerful adjunct to improve the aesthetic results of orthognathic surgery.
Introduction
Contrary to rhinoplasty in western countries, which is often characterized by procedures such as hump reduction or cephalic cartilage trimming, augmentation rhinoplasty is far more popular in the East Asian population (Ahn, 2006). However, the decreasing acceptance of longer downtime and convalescence after aesthetic surgery confronts surgeons with patient’s demands for less invasive alternatives. Soft tissue fillers for facial rejuvenation have been one of the most common outpatient procedures in recent years. Although some products have a short duration of efficacy, the use of nonbiodegradable fillers may result in foreign body reactions or tissue compromise, and removal of these materials can be difficult (Funt and Pavicic, 2013). Autologous fat injection on the other hand uses the patient’s own tissue as an abundant, inert, and readily available source, with the additional benefit of donor site contouring.
Many patients with dentofacial deformities may also benefit from simultaneous or subsequent rhinoplasty in addition to orthognathic surgery (Waite et al., 1988; Ronchi and Chiapasco, 1998; Seah et al., 2012). Because of nasal distortion and blockade of the possible surgical access due to nasal intubation, simultaneous implant insertion, or open rhinoplasty through a columella incision during orthognathic surgery is significantly impaired. Minimally invasive autologous fat injection is therefore an alternative to augment the nasal dorsum and tip (Lin et al., 2017). Since Gustav Neuber first described fat transfer in 1893 as a method to correct contour defects and also for appearance improvement of depressed facial scars (Neuber, 1893), the method has evolved to be one of the mainstays of plastic surgery. In the early 1990s, Coleman introduced his process of fat centrifugation and subsequent injection of small fat tissue parcels in different planes to enhance the surface area for better blood supply. However, fat survival rates are still a matter of controversy; while excellent graft survival rates up to 90% were reported based on histologic findings (Coleman, 1994; Coleman, 1995a; Coleman, 1997a; Coleman, 2006; Coleman and Katzel, 2015), some clinical studies report significantly lower retention rates (Gutowski and Force, 2009; Xie et al., 2010; Gerth et al., 2014a). A multitude of intrinsic factors such as patient age, location and condition of the recipient sites (Mojallal et al., 2009), and additional procedures (Gerth et al., 2014a) may affect the graft’s retention rate; extrinsic factors that influence the amount of graft survival include the type of fat harvesting, processing, and injection techniques (Pu et al., 2005; Zhu et al., 2013; Asilian et al., 2014).
Three-dimensional computer tomography (CT) is a reliable tool for measuring hard and soft tissue changes in orthognathic and facial plastic surgery procedures (Oh et al., 2013; Nur et al., 2016; Lo et al., 2018). The superimposition of pre- and postoperative imaging with subsequent measurement of the volumetric changes has been shown to be a reliable method for objectifying the results of facial plastic surgery procedures (Chang et al., 2017).
The objective of this study is to determine the fat retention rate in patients with simultaneous autologous fat injection augmentation rhinoplasty during orthognathic surgery. In this study, we try to provide objective graft retention measurements based on 3D imaging for orthognathic surgery combined with fat injection.
Methods
Ethics Statement
This prospective study was conducted and approved by (Institutional Review Board of Chang Gung Memorial Hospital.) and performed with the approval of the institutional review board (IRB) of (blinded institution) (IRB No. 201600134B0D001). The study methods were carried out in accordance with the approved guidelines of the IRB and the declaration of Helsinki. Institutional review board approved fully informed written consent was provided for all patients who included in this study. Patients depicted in the figures provided full written informed consent for the publication of their medical images.
Patient Population and Inclusion Criteria
Nineteen consecutive patients treated for dentofacial deformities by a combination of orthognathic surgery and simultaneous nasal dorsum augmentation with fat injection in the (BLINDED INSTITUTION) between 2016 and 2018 were enrolled in this prospective clinical study. All surgeries were conducted by a single surgeon. Inclusion criteria were (a) patients with maxillofacial anomalies undergoing orthognathic surgery with simultaneous autologous fat injection rhinoplasty, (b) patients who had pre- and postoperative (at least 6 months after surgery) CT scans. Exclusion criteria were (a) patients with craniofacial anomalies or syndromes, (b) patients with no simultaneous orthognathic surgery and autologous fat augmentation rhinoplasty, and (c) incomplete data. Two patients were excluded, one due to a failed Digital Imaging and Communications in Medicine (DICOM) transfer, the other because of refusing to have a 6-month postoperative CT evaluation. Therefore, the complete datasets of 17 patients were included in the evaluation.
Orthognathic Surgery (Surgical Planning and Techniques)
A preoperative CT scan (Toshiba TSX-301C, Toshiba Medical System Corporation) was performed pre- and at least 6 months postoperatively for every patient. Digital Imaging and Communications in Medicine data were transferred to the Dolphin 3D surgical planning tool (Dolphin Imaging 11.0) for 3D virtual surgery planning for all patients.
Single splint orthognathic surgery was conducted in all cases (Bergeron et al., 2008; Yu et al., 2009). All patients were treated with a combination of a Le Fort I Maxillary osteotomy and an Obwegeser type bilateral sagittal split ramus osteotomy with or without Genioplasty. All surgical complications were recorded.
Autologous Fat Injection Rhinoplasty
The autologous fat injection was conducted at the end of the orthognathic surgery in the same operative session. All procedures were performed with the face and abdomen prepped in a sterile fashion. After finishing the bimaxillary orthognathic surgery, the lower abdomen was infiltrated with 200 to 500 mL of tumescent solution, consisting of 500 mL of normal saline, 20 mL of 2% Xylocaine, 0.5 mL of Bosmin, and 10 mL of 7% sodium bicarbonate (sodium bicarbonate [NaHCO3] 7% [16.7 mEq] 20 mL/amp). The injection is carried out with 20 mL syringes and 18 gauge cannulas in the periumbilical area. After 10 to 15 minutes, liposuction of the abdomen was performed through 2 stab incisions in the belly button using a blunt tip 2.5-mm cannula with one side hole on 10 mL Luer-Lock syringes with the plunger pulled back gently about 2 cm to prevent adipocyte damage. The liposuction aspirate was filtered through a fine silicon mesh (CSD Co, Ltd) surrounded by a dry gauze, and then transferred from a 10-mL syringe to 1-mL syringe via the syringe transducer of the MAFT-Gun kit (Dermato Plastica Beauty Co, Ltd).
The midline of the nasal dorsum and the proposed areas of fat injection were marked out preoperatively. The nasal tip was infiltrated with 0.1 to 0.2 mL of 1% xylocaine with 1:100 000 epinephrine. The nasal tip was then punctured with an 18-gauge needle and the fat injection was performed using the micro-autologous fat transplantation (MAFT) Gun (Lin et al., 2014) through the puncture site (Video). The size of each delivered fat parcel was set at 1/60 mL. An 18-gauge blunt tip cannula with a side-facing injection port was used for fat injection. The fat graft was injected in different planes according to the structural fat grafting technique described by Coleman (Coleman, 1997b; Coleman and Katzel, 2015) (Figure 1). The amount and location of fat injected were recorded for each patient. Postoperatively, all patients received 35% humidified normobaric oxygen with a flow of 10 L/min to enhance fat graft survival, regeneration, and survival of the fat graft (Kato et al., 2014).
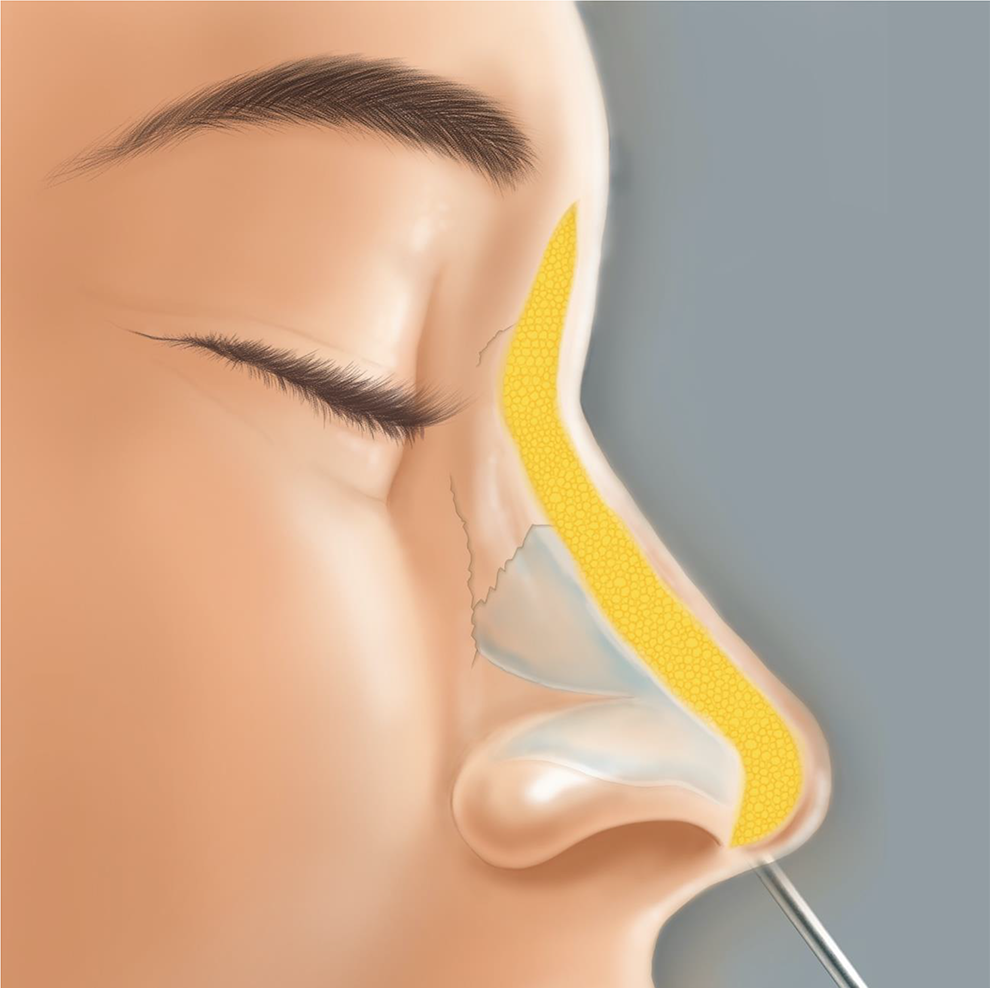
Autologous fat injection rhinoplasty. An 18-gauge blunt tip cannula with a side-facing injection port was used for fat injection. The fat graft was injected in different planes.
Three-Dimensional Computer Tomography Scans
The 3D CT scans before and more than 6 months after surgery were collected, as volumetric decrease of transferred fat in the craniomaxillofacial region has been shown to proceed up to 6 months after surgery (Guijarro-Martínez et al., 2011). The DICOM data were transferred to AVIZO version 7.0 software for further analysis. The images were oriented as following: the Frankfort Horizontal (FH) plane was used as the axial plane, defined by the best-fitting plane through bilateral orbitale and porion landmarks; the coronal plane was oriented perpendicular to the FH plane, and passed through the bilateral porion; the sagittal plane was set perpendicular to the FH and coronal planes, passing through the center of bilateral orbitale landmarks. The nasal dorsum soft tissue measurements were performed within the following borders (Figure 2): the upper limit being the most cephalad area of the bilateral orbital rim level; the lateral limits being the most medial area of the bilateral orbital rim; the inferior limit being the most inferior part of the columella; the posterior limit being the most posterior point of the radix; and the anterior limit being the most anterior part of the nasal tip (Figure 2). The data were transferred to a 3D reconstruction and finally adjusted to include only soft tissue by erasing all bony structures (Figure 3). After registration, 3D pre- and postoperative nasal soft tissue volumes within the aforementioned limits were subtracted to yield the resulting volumetric differences for further evaluation. All measurements were performed twice by the same evaluator with an interval of at least 2 weeks in a nonblinded fashion.
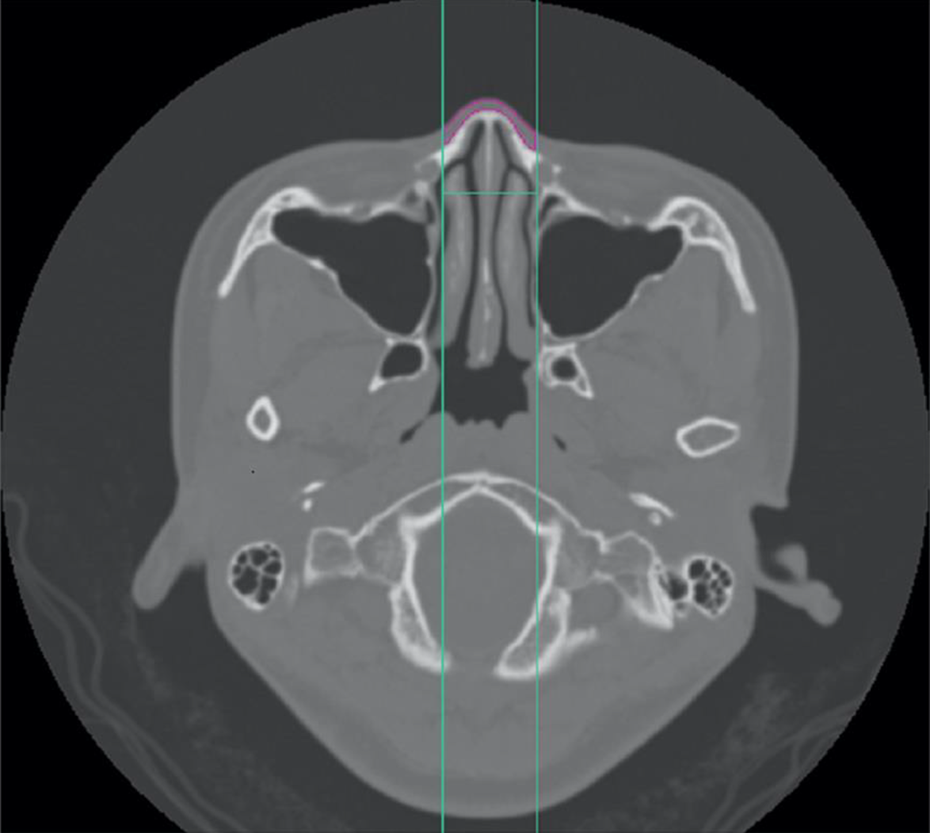
Three-dimensional computer tomography (CT) measurement conduction in the horizontal view; the lateral limit is set at the most medial part of the orbital rim, the posterior limit is the radix, and only the soft tissue of the nose is included in the measurement (red color tissue area).
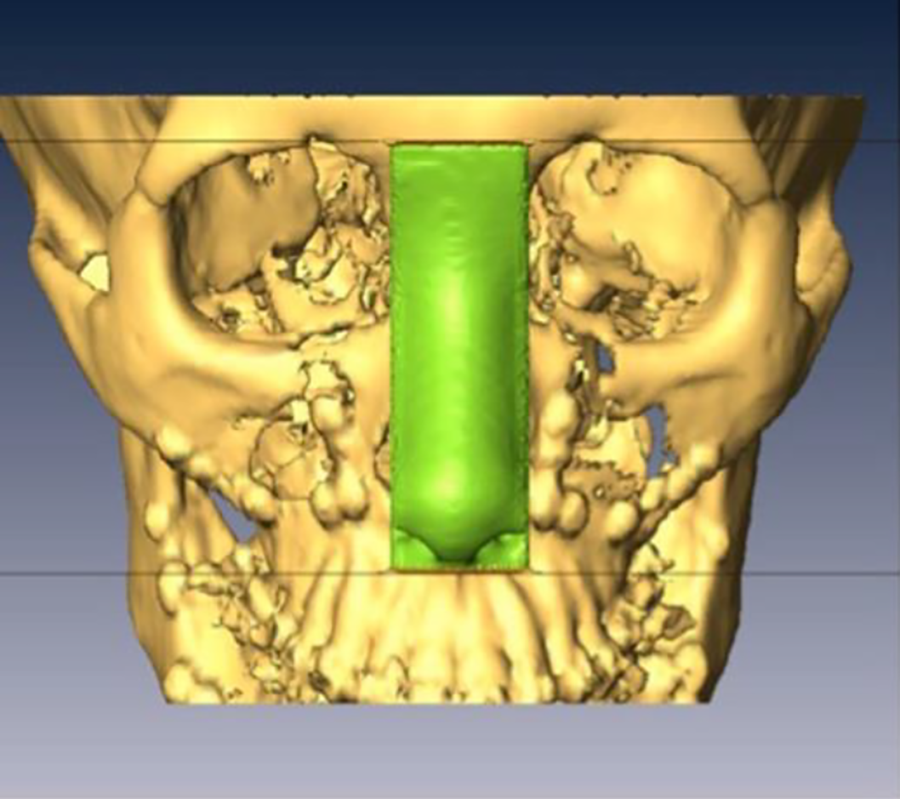
The data are transferred in a 3D reconstruction and finally adjusted to include only soft tissue by erasing all bony structures. After registration, 3D pre- and postoperative nasal soft tissue volumes within the aforementioned limits were subtracted to yield the resulting volumetric differences for further evaluation.
Statistical Analysis
Intraobserver reliability was assessed using the Pearson correlation by comparing 2 sets of measurements of marked areas and volume differences performed by the same evaluator.
The paired t test was used to compare the nasal volumes before and at least 6 months after surgery measured by 3D CT scan. The volume of injected and retained fat (according to 3D CT measurements) is compared, and the percentage of retention is calculated. A P value of less than .05 is considered a statistically significant difference. Mean results are calculated with standard deviations (mean ± standard deviations).
Results
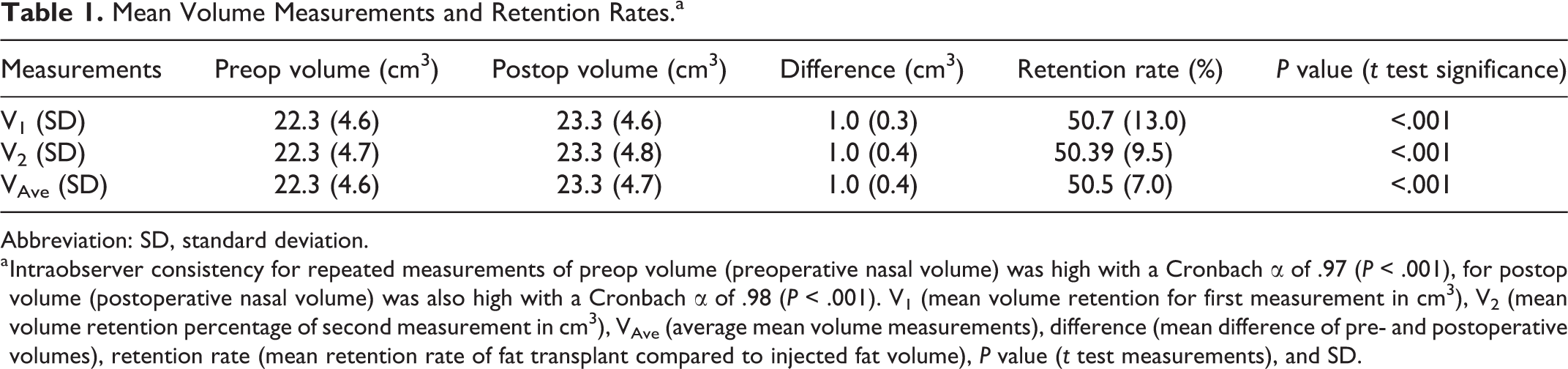
Seventeen patients completed the study, all patients were female. The mean soft tissue volumes of the patient’s noses measured with 3D CT before surgery were 22.3 ± 4.6 cm3 and 22.3 ± 4.7 cm3 in the course of repeated measurement. Intraobserver consistency was high with a Cronbach α of .97 (P < .001). The volumes of nasal soft tissues measured with 3D CT after surgery were 23.3 ± 4.6 cm3 and 23.3 ± 4.8 cm3 in the course of repeated measurement. Intraobserver consistency was high with a Cronbach α of .98, P < .001. The volume means before and after surgery were 22.3 ± 4.6 cm3 and 23.3 ± 4.6 cm3, respectively, with a mean difference of 1.0 ± 0.4 cm3 (P < .001). The mean retention rate was calculated to be 50.5% ± 7.0% (Table 1).
Mean Volume Measurements and Retention Rates.a
Abbreviation: SD, standard deviation.
a Intraobserver consistency for repeated measurements of preop volume (preoperative nasal volume) was high with a Cronbach α of .97 (P < .001), for postop volume (postoperative nasal volume) was also high with a Cronbach α of .98 (P < .001). V1 (mean volume retention for first measurement in cm3), V2 (mean volume retention percentage of second measurement in cm3), VAve (average mean volume measurements), difference (mean difference of pre- and postoperative volumes), retention rate (mean retention rate of fat transplant compared to injected fat volume), P value (t test measurements), and SD.
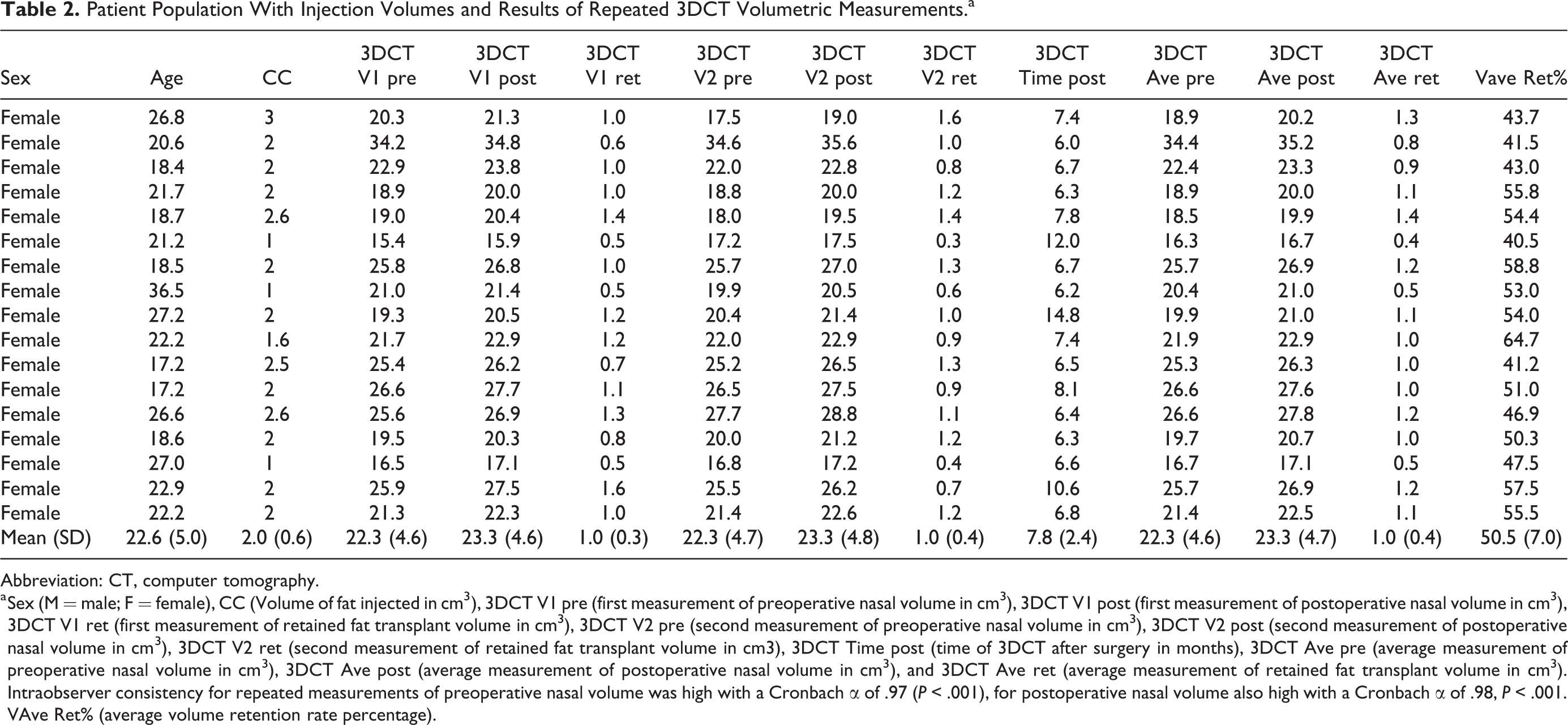
The mean patient age was 22.6 ± 5.0 years (range: 17.2-36.5 years). The amount of fat injected for nasal dorsum augmentation was 2.0 ± 0.6 mL of fat (range: 1-3 mL). The repeated volume measurements for all patients are shown in Table 2.
Patient Population With Injection Volumes and Results of Repeated 3DCT Volumetric Measurements.a
Abbreviation: CT, computer tomography.
a Sex (M = male; F = female), CC (Volume of fat injected in cm3), 3DCT V1 pre (first measurement of preoperative nasal volume in cm3), 3DCT V1 post (first measurement of postoperative nasal volume in cm3), 3DCT V1 ret (first measurement of retained fat transplant volume in cm3), 3DCT V2 pre (second measurement of preoperative nasal volume in cm3), 3DCT V2 post (second measurement of postoperative nasal volume in cm3), 3DCT V2 ret (second measurement of retained fat transplant volume in cm3), 3DCT Time post (time of 3DCT after surgery in months), 3DCT Ave pre (average measurement of preoperative nasal volume in cm3), 3DCT Ave post (average measurement of postoperative nasal volume in cm3), and 3DCT Ave ret (average measurement of retained fat transplant volume in cm3). Intraobserver consistency for repeated measurements of preoperative nasal volume was high with a Cronbach α of .97 (P < .001), for postoperative nasal volume also high with a Cronbach α of .98, P < .001. VAve Ret% (average volume retention rate percentage).
Discussion
Orthognathic surgery is one of the most powerful tools to alter facial appearance. However, when the facial relations are changed, disbalances and asymmetries of facial relations can sometimes be emphasized instead of alleviated; this may be the case for facial asymmetry in the frontal view (Yamaguchi et al., 2017) as well as for facial relations toward structures outside the surgical field such as the nose (Ronchi and Chiapasco, 1998). Several authors have described simultaneous or staged adjunct procedures to harmonize the facial appearance during or after orthognathic surgery. Bohluli et al. (2014) described submental fat transfer to other facial areas such as the lips or paranasal zones to correct submental lipomatosis and facial disbalances after orthognathic surgery. Hernandez-Alfaro et al. (2015) used the buccal fat pad for malar augmentation during orthognathic surgery to enhance prominent cheekbones that are regarded as a sign of beauty in western societies. Rubio-Bueno et al. (2013) conducted a controlled study for simultaneous augmentation of the upper lip and paranasal area in orthognathic surgery patients. In a preliminary study, Raffaini and Pisani (2015) showed a high patient satisfaction rate for simultaneous soft tissue correction with autologous fat grafting during orthognathic surgery. Also, facial bone contouring techniques are regularly used to improve the appearance after orthognathic surgery (Li et al., 2016; Chen et al., 2017; Qin et al., 2018). These approaches show that a simultaneous surgical approach can be applied safely with good results and reflect patient’s demands for fewer surgeries with less downtime and shorter convalescence.
The correlation between orthognathic surgery and changes to the overlying soft tissue structures is well established (Altman and Oeltjen, 2007; van Loon et al., 2015). In correspondence, the risks and benefits of simultaneous orthognathic surgery and rhinoplasty have been a subject of discussion (Seah et al., 2012; Sun and Steinbacher, 2018), and a number of authors have already reported their outcomes of these combined procedures (Posnick et al., 2016; Raffaini et al., 2018). However, larger cohort studies are needed to determine an algorithmic approach for extensive simultaneous septorhinoplasty (Sun and Steinbacher, 2018), especially in Caucasians, where hump reduction, nasal tip alteration, and osteotomies are standard components of rhinoplasty procedures. In contrast, our study is based in the Asian population and describes simultaneous orthognathic surgery and a minimally invasive rhinoplasty procedure previously presented in a pilot study of our group (Lin et al., 2017). This approach can be considered as an adjunct augmentation of the nasal dorsum and tip, which are facial zones that are not readily affected by orthognathic surgery (Worasakwutiphong et al., 2015). This enhances the possibility of controlling the postoperative aesthetic outcome, as fat augmentation is provided to areas outside of already operated and swollen tissue. As nasal dorsum augmentation is a very common procedure in the Asian population, our approach was well received by our patients. Especially in the profile view, the changes are significant (Figure 4), not only because of the lower face alteration but also the overall aesthetic harmonization of the facial profile by nasal dorsum augmentation (Figure 4). In addition, the procedure is conducted with minimal additional operating time, significant improvement of facial appearance, and therefore, a favorable risk–benefit ratio for the patient.

Before surgery, there is very limited nasal dorsum at all in the lateral view (left); after orthognathic surgery and simultaneous autologous fat injection, there is an increase in nasal dorsum projection. Notice that there was a nasal dorsum nevus that was removed during the same surgery.
Fat retention rates after autologous fat transfer have been the subject of many discussions. Also, the amount of fat graft needed for a stable result depends on the area of injection and varies considerably according to the literature reviewed by Shue et al. (2018). In facial procedures, the range of retention rates reflects the clinical range from just over 41% (Gerth et al., 2014b) to almost 90% based on histologic findings (Coleman, 1995b; Coleman, 1997b; Coleman, 2006; Coleman and Katzel, 2015). In our current clinical practice, we use the MAFT technique for autologous fat transfer as described by Lin et al. (Lin et al., 2014; Kao et al., 2016). In our previous study for minimally invasive rhinoplasty, we demonstrated a retention rate of 44.54% (range: 21%-74%) (Lin et al., 2017) in a nonorthognathic surgery patient group. In the orthognathic surgery group described here, we can report a slightly higher retention rate of 50.5% ± 7.1%. This might be due to multiple factors such as involuntary postoperative immobilization and less facial expression after orthognathic surgery. Postoperative pain and subsequent diminished use of the nasalis muscle may lead to less stress on the fat tissue and therefore increased survival rate. The nose itself is also outside the orthognathic surgical field, and therefore not submitted to tissue stress and less surface exposure due to dead space as much as the mid and lower face. Moreover, the postoperative application of normobaric hyperoxygenation may enhance the fat graft survival according to the study of Kato et al. (2014).
Our study has some limitations. Not all potential patients could be included in the study. Two patients were excluded; one patient completed the preoperative CT scan but was excluded due to a failed DICOM transfer. The patient data were omitted because we failed to retrieve the complete DICOM CT images. The other patient refused to have a 6-month postoperative CT evaluation. However, it has been rightly noted that the supporting science of fat grafting still lags behind the clinical use (Khouri et al., 2014). Objectifying the results in autologous fat transfer using 3D imaging methodology in combination with a prospective study design is very rare and in our opinion definitely needed to gather more evidence in one of the most dynamic fields of plastic surgery (Sinno et al., 2016). Thus, we believe that our study increases our knowledge about the fat graft retention rate of minimally invasive rhinoplasty in orthognathic surgery and demonstrates the feasibility of using this procedure as a simultaneous adjunct to further improve the postoperative results and patient satisfaction.
In this study, we provide objective graft retention measurements for fat injection augmentation rhinoplasty combined with orthognathic surgery in a prospective study setting. All patients were satisfied with the results, and no complications or additional morbidity was noted in the postoperative course. We consider this procedure to be a safe, reliable, and powerful tool to improve the aesthetic results for facial harmonization of patients undergoing orthognathic surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by Chang Gung Research Grant CMRPG5F0191.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.