
Abstract
Ectomesenchymal chondromyxoid tumor (ECT) is a rare oral lesion first described by Smith et al. in 1995. These tumors are typically painless, slow growing and benign masses occurring predominantly on the anterior tongue dorsum. Prior to this seminal report, many ECTs may have been misdiagnosed due to the histological similarities with other lesions. Immunohistochemical stains aid in definitive diagnosis of an ECT. A total of 39 papers since published have reported 96 patients with ECT. Most lesions involve the anterior aspect of the tongue, with only 6 occurring in the posterior tongue and 2 involving the hard palate. ECTs are considered to develop from ectomesenchymal cells of neural crest cells that have migrated to the tongue during embryological development. This paper is of a rare case of ECT of the posterolateral tongue occurring in association with an unusual asymmetrical soft palate cleft. It is postulated that since the tongue develops before the formation of the soft palate, an ECT lesion occurring on the posterior aspect may have a causal contribution to the development of the soft palate cleft.
Introduction
Ectomesenchymal chondromyxoid tumors (ECTs) are rare benign neoplasms first reported by Smith in 1995 as a new subset of chondromyxoid lesions occurring on the anterior tongue. Smith et al. reviewed 10 male patients and 9 female patients between 9 and 78 years of age (mean age: 32 years), all with tumors of anterior two-thirds of the tongue. The tumors varied between 3 and 20 mm in size, and the duration of the lesion since initial presentation ranged from months to up to 10 years (Smith et al., 1995).
Prior to this seminal publication, many such lesions were probably misdiagnosed due to marked similarity and overlapping clinical and histological features shared with other lesions. Many studies have hereafter focused on identifying pertinent morphological and immunohistochemical characteristics for differentiating ECT from other lesions (Allen, 2008; Leeky et al., 2011; Kato et al., 2017).
ECTs are asymptomatic slow-growing swellings with a predilection for the anterior dorsum aspect of the tongue (Leeky et al., 2011). Histologically, the lesion presents as a circumscribed nonencapsulated lobulated mass with nests, cords or sheets of round, fusiform or polygonal cells in a myxoid or chondromyxoid stroma (Woo et al., 2005; Kannan et al., 1996). The myxoid or chondromyxoid stroma may be very similar to that seen in the mucous extravasation phenomenon, oral focal mucinosis, ossifying fibromyxoid tumor, pleomorphic adenoma, myxoma, nerve sheath myxoma, myoepithelioma, chondroid choristoma, myxoid neurothekeomas, and papillary meningiomas (Leek et al., 2011; Woo et al., 2005; Kannan et al., 1996; Van der Wal and Van der Waal, 1996). ECT may also resemble myxoid malignant tumors such as chondrosarcoma, liposarcoma, and clear cell carcinoma (Riju et al., 2019).
The World Health Organization classifies ECT as a subtype of a myoepithelioma (El-Naggar et al., 2017). Immunohistochemically, ECTs are positive for glial fibrillary acid protein (GFAP), S-100 protein, and vimentin (Almeida et al., 2018).
There are 2 theories proposed in the literature on the development of ECT. The first theory is centered around a minor salivary gland origin. Since the ECT has a high propensity for the anterior two-thirds of the tongue dorsum, the minor salivary gland theory is unlikely due to the absence of minor salivary glands in this region. Lingual salivary gland tissue is normally only found in the posterior dorsolateral tongue (von Ebner glands) and anterior ventral tongue (Blandin and Nuhn glands) (Portnof et al., 2009; Yoshioka et al., 2003).
The second theory is based on the development of ECT from uncommitted ectomesenchymal tissue that originates from neural crest ectomesenchymal cells from the first branchial arch (Smith et al., 1995; Allen, 2008; Laco et al., 2016). This conforms to the site of the lesion as the first branchial arch contributes to the formation of the anterior two-thirds of the tongue (Carlson 2014). These ectomesenchymal cells have the ability to differentiate into neurogenic, chondrogenic, myogenic, adipogenic, osteogenic, odontogenic, and epithelial lineages (Lin et al., 2006; Yan et al., 2006). This theory was reinforced by Yoshioka et al., who identified that ECT cells are morphologically similar to neuronal cells; with an expression of GFAP, Nanog, microtubule associated protein 2 (MAP2), octamer- binding transcription factor 3/4 (OCT3/4), sex determining region Y-boxtranscription factor 2 (SOX2), and natural killer marker (CD105), thus emphasizing the characteristics of undifferentiated stem cells; with multipotent cellular differentiation. The neural crest theory is reinforced by immunohistochemical expressivity related to neural tissue such as GFAP, S-100 protein, natural killer cell marker (CD 57), neuron-specific enclave (NSE), and protein gene product-9.5 (PGP-9.5) (Yoshioka et al., 2003; Tsai et al., 2012).
Case Report
A 2 year 4 months-old patient, from a rural location, presented with cleft soft palate. There was a history of nasal reflux during feeding and hypernasality with speech. Speech and audiology care was not accessible to the patient due to their remote location. Clinical examination revealed 2 abnormalities. The first was an asymmetry of the right soft palate, and the second was a nodular mass protruding from the right posterior lateral tongue/tonsillar region. The lesion was ∼12 mm × 4 mm in size. There seemed to be a correlation between the nodular lesion and the soft palate cleft (Figure 1).
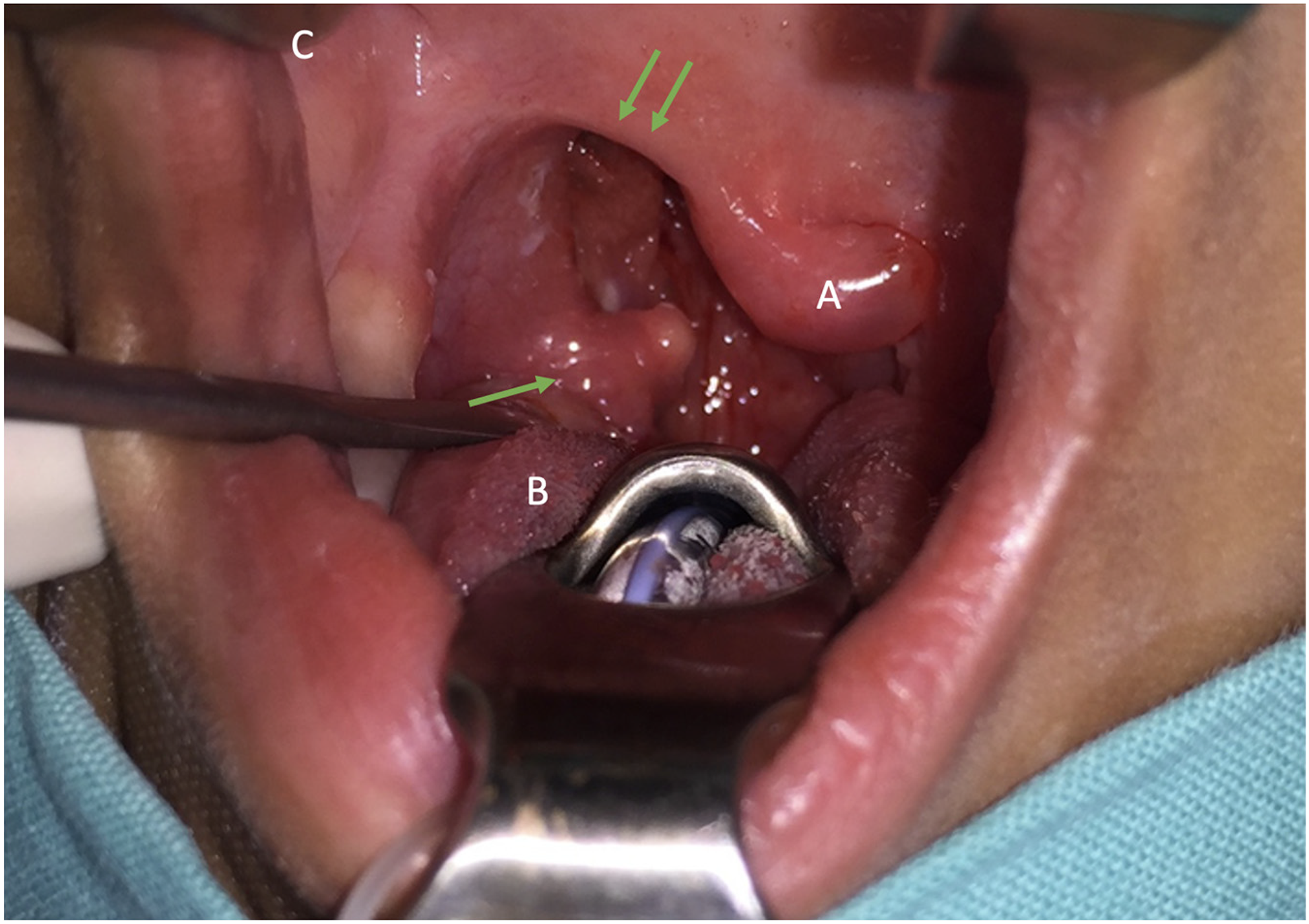
Ectomesenchymal chondromyxoid tumor (ECT) at right posterolateral tongue base (single arrow); asymmetrical cleft (double arrow): (A) uvula reflected, (B) tongue, and (C) tuberositas right.
Magnetic resonance imaging demonstrated a defect on the right soft palate lateral to the uvula. The lesion extended from the right posterior–lateral tongue encroaching into the region of the cleft palate (Figure 2).
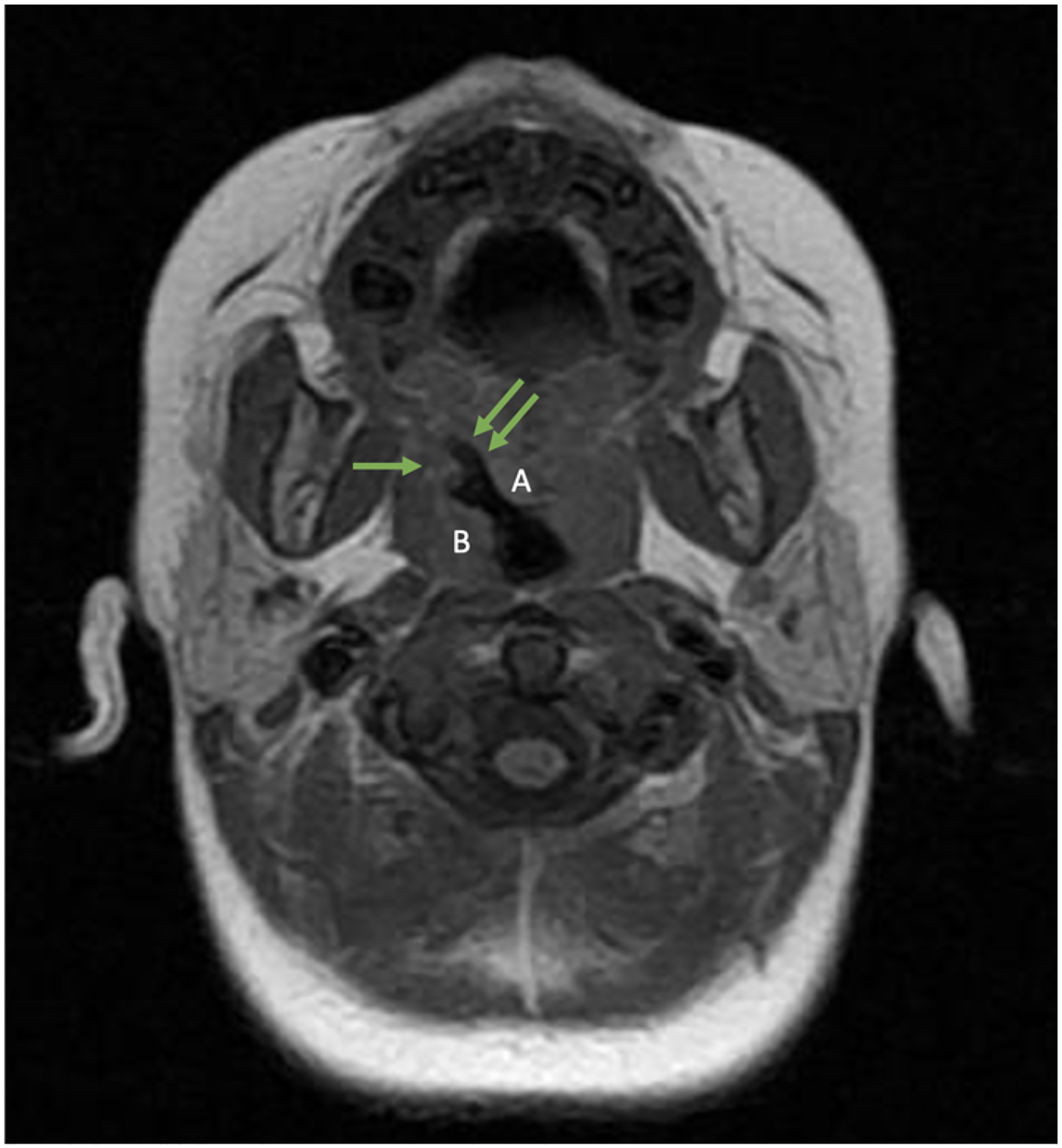
Axial magnetic resonance imaging (MRI) view indicating a mass protruding into the right oropharyngeal area (single arrow) with posterior shift of the right oral tonsil: (A) uvula and (B) asymmetrical cleft (double arrow).
The tumor was surgically removed under general anesthesia together with a right tonsillectomy and placement of a myringotomy (Figure 3). A soft palate closure was simultaneously performed utilizing the Parker-Furlowplasty technique; for soft palate lengthening to optimize on speech development (Bütow, 2015; Bütow et al., 2016). The base of the oral triangular flap on the cleft side was sutured in a more posterior position to achieve lengthening. The apex of the flap was rotated from an anterior to a posterior position as described by Furlow (Furlow, 1986). The soft tissue defects, which were created as a result of the posterior displacement of the base of the triangular flap, was filled with unilateral pedicled buccal fat pad.
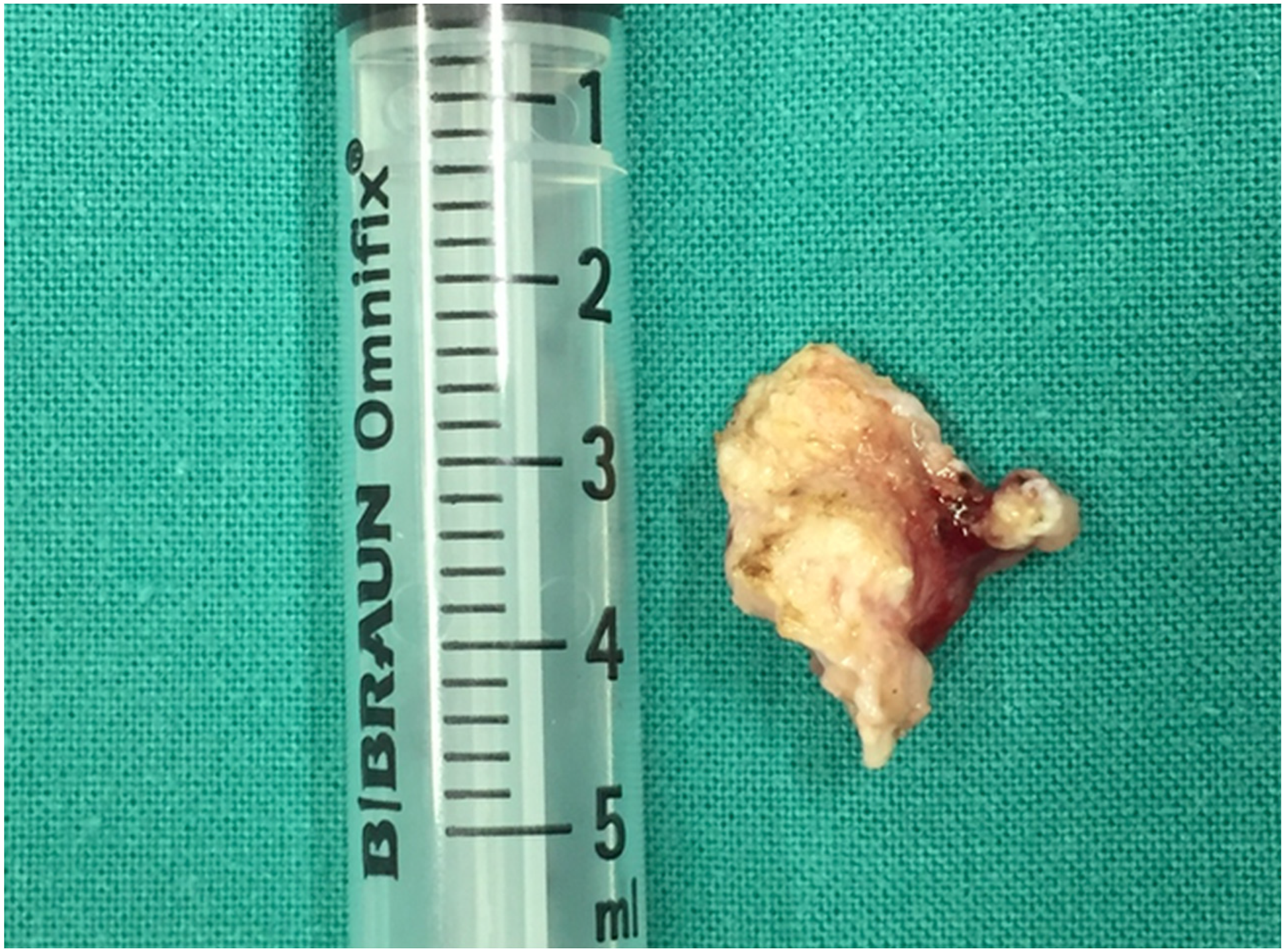
Biopsy specimen.
Histopathologically, the tumor presented within the deep soft tissue as a raised, polypoid relatively circumscribed yet unencapsulated solid mass of chondroid tissue in a myxoid background. The lesion was relatively paucicellular with elongated, spindled, and fusiform cells showing very little cytoplasm, suspended within a reticular myxoid stroma. The nuclei were small and uniform with no pleomorphism or hyperchromasia (Figure 4).
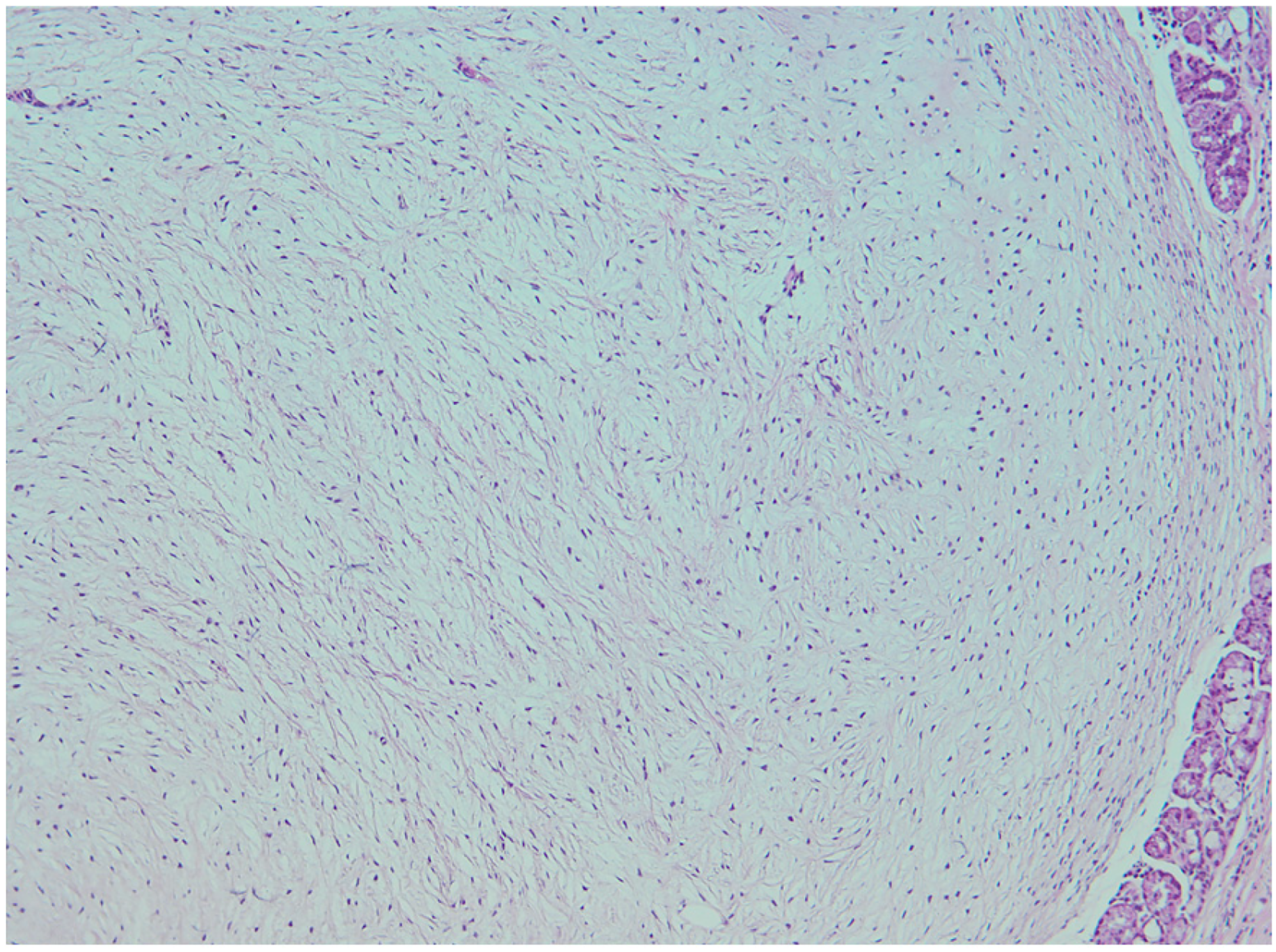
Histologic findings of excised tumor (hematoxylin and eosin [H&E], medium power, 20 × ), showing elongated, spindled, or fusiform cells suspended in a reticular myxoid stroma.
Immunohistochemical staining in the presence of adequate positive and negative controls showed focal positivity of the lesional cells with GFAP, S-100 protein, and cytokeratin AE1/AE3 (AE1/AE3) (Dako).
A diagnosis of ectomesenchymal chondromyxoid tumor of the tongue was confirmed.
The patient was followed up after 19 months with no tumor recurrence noted. Although the patient had received no formal speech interventions postoperatively (due to lack of accessibility), she presented with reduced hypernasality with improved speech intelligibility.
Discussion
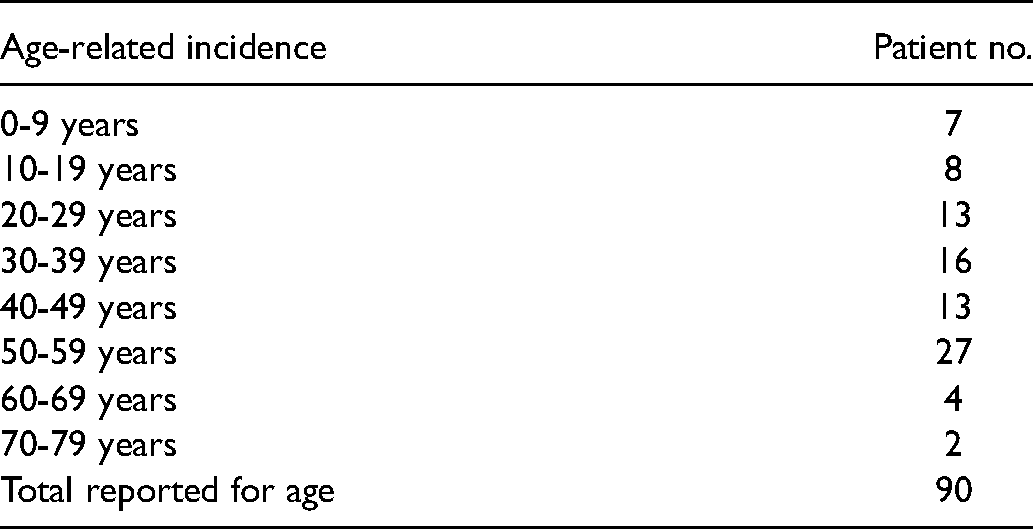
To the best of our knowledge there are at present approximately 96 ECT cases reported in 39 publications since the first description by Smith et al (Smith et al., 1995). Previous reports show ECT to occur between the first and 8 decades of life; 7 and 78 years (median age: 41 years). Most patients were in the third to the sixth decades. There was no gender predilection (male: n = 49, female: n = 47) (Table 1).
Age-Related Incidence of Ectomesenchymal Chondromyxoid Tumor (ECT).
Clinically ECT appears as a benign, submucosal mass that enlarges gradually and that usually ranges in size between 5 and50 mm (median: 12 mm, n = 50). (Kato et al., 2017) Most lesions present with an intact overlying mucosal covering. Seo et al. reported a case of an 8-year-old male patient with a polypoid lesion showing an ulcerated mucosal surface (Seo et al., 2010). This was possibly due to previous minor trauma. ECTs are usually asymptomatic; however, Kannan et al. found occasional pressure symptoms in a 51-year-old female with a 0.5 cm mass of the anterior tongue dorsum (Kannan et al., 1996).
ECTs usually present as slow growing, asymptomatic swellings with a predilection for the anterior dorsal aspect of the tongue (Leeky et al., 2011). The differential diagnosis of such an exophytic tongue mass includes reactive lesions (irritation fibroma, pyogenic granuloma, and mucocele), infections (tuberculosis and syphilis), immunological conditions (amyloidosis and sarcoidosis), and neoplasia (carcinoma, sarcoma, and salivary gland) (Allon et al., 2019).
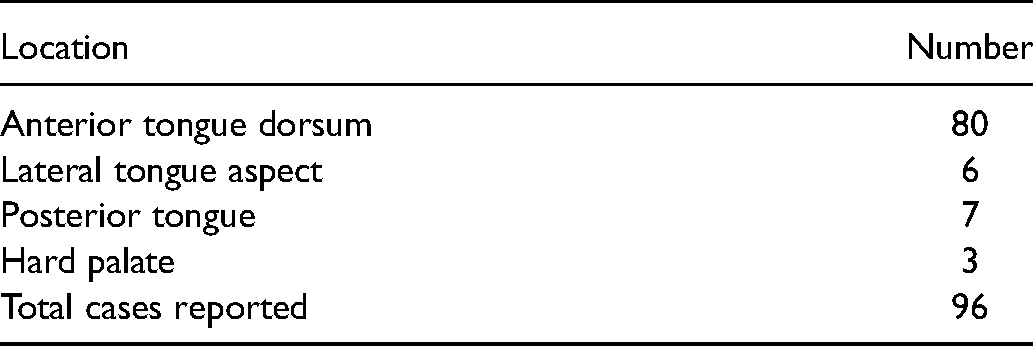
Although most ECTs are reported to occur in the anterior tongue dorsum (n = 80 of 96), 6 cases occurred in the lateral tongue (Smith et al., 1995; Carlson et al., 2014; Seo et al., 2010), 7 in the posterior tongue (Kato et al., 2017; Seo et al., 2010; Cardin et al., 2014; Carlos et al., 1999; Dickson et al., 2018), and 3 on the hard palate (Nigam et al., 2006; Gouvêa et al., 2012; Truschnegg et al., 2018) (Table 2).
Nigam et al. reported an ECT of the posterior hard palate. This lesion was diagnosed on an exclusionary histological basis without immunochemical analysis (Nigam et al., 2006). Thus, this diagnosis of ECT was questioned by Guzmán et al. and Ide et al. (Guzmán et al., 2012; Ide, 2006). Gouvêa et al. presented an ECT of the hard palate with phenotypic and immunohistochemical characteristics that did not completely meet the criteria for diagnosis (Allen, 2008; Kato et al., 2017; Portnof et al., 2009; Laco et al., 2016; Nigam et al., 2006). Truschnegg et al. reported the ECT of the anterior hard palate. This case resembled a reactive lesion clinically, and expressed variable positivity for S-100 protein and alpha-smooth muscle actin (α-SMA); with negativity for pancytokeratin, GFAP and cytokeratin (CK14) (Truschnegg et al., 2012).
Intra-Oral Regional Distribution of Ectomesenchymal Chondromyxoid Tumor (ECT).
The 2 cases reported by Seo et al. include an ECT of the posterior tongue dorsum. Although this lesion showed histologic similarities to the originally described ECT; it differed in its immunohistochemical profile, especially with regard to GFAP negativity (Seo et al., 2010).
The first case of an ECT occurring in the posterolateral tongue was described by Carlos et al in 1999 in a 16-year-old male patient (Carlos et al., 1999). Kato et al. also described a slow enlarging mass of the right posterior lateral aspect of the tongue in a 34-year-old male. This lesion measured ∼3 to 4 cm and extended along the lateral pharyngeal wall to the right side of the soft palate (Kato et al., 2017).
ECTs may display histological similarities to a pleomorphic adenoma due to its myxoid or chondromyxoid background; however, it lacks the ductal and epithelial components typical of pleomorphic adenoma (Chopra et al., 2010; Berry et al., 2004; Closmann et al., 2013).
The management of the lesions is simple excision (Dickson et al., 2018). Recurrences are uncommon; however, 4 cases of recurrence have been reported, possibly due to inadequate surgery (Smith et al., 1995; Portnof et al., 2009). Portnof et al. and Dickson et al. described 2 atypical cases in which the tumor presented histologically as highly cellular with infiltrative fronts, and invasion into the underlying muscle. This most likely contributed to the recurrence experienced by Portnof et al. due to inadequate excision (Portnof et al., 2009; Dickson et al., 2018). Tumor recurrence has been reported to occur up to 19 months after the original resection. Although the incidence of recurrence is only 3% (3 of 96) this emphasizes the need for long-term patient follow-up (Kannan et al., 1996; Angiero, 2010).
Preoperative imaging was only performed in 3 studies. Gouvêa et al. reported having taken pre and postoperative radiographs, while both Cardin et al. and Kato et al. performed preoperative computed tomography (CT) scans (Kato et al., 2017; Cardin et al., 2014; Gouvêa et al., 2012).
The development of the tongue begins in the fifth week of embryological life from paired lateral swellings of the first pharyngeal arch and 2 median swellings: the tuberculum impar (first and second pharyngeal arches) and the copula (second and third pharyngeal arches). The lateral swellings and tuberculum impar contribute to the development of the anterior two-thirds of the tongue. The posterior third of the tongue originates from the second median swelling, the copula. The root of the tongue develops from the copula and ventromedial tissue between the third and fourth pharyngeal arches. Tongue growth occurs through a major contribution from the lateral lingual swelling and a lesser contribution from the tuberculum impar.
The embryological development of the palate occurs between 6 and 10 weeks of life. The secondary palate forms at the beginning of the seventh week of gestation from a median palatine process and a pair of lateral palatine processes that grow as vertical extensions of the maxilla on either side of the tongue. Elevation of the palatal shelves occurs with a change in orientation from vertical to horizontal. Growth occurs in a medial direction above the tongue toward the midline.
The regulation of fusion of the hard and soft palate are independently controlled. Hard palate fusion occurs at 8 weeks gestation resulting in separation of the oral cavity from the nasal cavity; while fusion of the soft palate that separates the oropharynx from the nasopharynx occurs at 10 weeks gestation (Carlson, 2014; Kulbersh and Wiatra, 2015; Danescu et al., 2015). While the mechanism of closure of the soft palate is unclear, the soft palate is known to play a key role in speech and sound production. Inadequate soft palate closure or uncoordinated soft palate movement during speech and swallowing can result in velopharyngeal incompetence (VPI) and nasal reflux, respectively.
VPI is defined as an abnormality of the structure of the velopharyngeal valve. Hypernasality or nasal air emission may occur as a consequence of VPI dependent on the extent of the defect (Kummer et al., 2015).
Conclusion
This report of an ECT in the posterolateral tongue of an infant is unique as it documents the youngest patient with ECT. The youngest child previously reported was in a 7-year-old male, and only 7 other cases have been reported in the first decade. Secondly, the lesion presented in the posterolateral aspect of the tongue, an uncommon site for ECT, with only 7 previous cases reported in this site. This is also the first presentation of an ECT in association with an asymmetrical cleft palate, raising the possibility of a causal effect of the ECT on the development of the cleft.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.