
Abstract
Objective
The primary goal of maxillary alveolar cleft reconstruction in patients with cleft lip/palate at the phase of mixed dentition is to build bone in the cleft area which in turn allows closure of the oronasal fistula, establishes arch continuity, and improve maxillary stability. This study aimed to evaluate the double iliac corticocancellous bone plates grafting technique for initial alveolar cleft grafting.
Design
This prospective study was conducted on 12 consecutive patients with unilateral complete alveolar cleft and previous cleft lip and palate corrective surgery.
Intervention
For all patients, the iliac crest graft was harvested and cut into 2 cortical bone plates and adapted labially and palatally. Both plates were fixed with screws then the gap between the 2 plates was filled with cancellous bone. The grafted side was compared to the contralateral side 9 months postoperatively regarding labio-palatal alveolar width and bone density, while the 9 months postoperative graft height was compared to the immediate postoperative height using computed tomography scans.
Results
All grafted sides showed similarity to the contralateral sides regarding both alveolar width and bone density with minimal crestal bone resorption.
Conclusion
The double iliac corticocancellous bone plate grafting technique seems to be a reliable method for alveolar cleft reconstruction with adequate bone quality and contour.
Introduction
Maxillary alveolar clefts induce several problems including oronasal communication, maxillary arch discontinuity, prevention of normal permanent teeth eruption with subsequent affection of maxillary stability. Alveolar bone grafting in the mixed dentition phase prevents these complications and permits the permanent dentition to migrate and erupt normally through the cancellous bone, maintain bony support of teeth adjacent to the cleft and prevent the collapse of alveolar segments (Boyne and Sands, 1972; Akahashi et al., 1999; Dempf et al., 2002; Bagheri et al., 2012; Cho-Lee et al., 2013).
The ideal bone graft material for alveolar cleft reconstruction remains controversial. Various bone grafting materials were introduced including autogenic, allogenic, xenogenic, and alloplastic grafts (Ochs, 1996; Horswell and Henderson, 2003). Nevertheless, autogenous bone graft harvested from the anterior iliac crest is considered the optimal source of autogenous bone for alveolar cleft reconstruction, so it is termed the “gold standard bone graft.” The anterior iliac crest has the advantage of providing a large quantity of cancellous bone and easy surgical access. Furthermore, it has great osteogenic potential especially in the early phase following grafting due to abundant pluripotent osteogenic precursor cells. However, particulates of cancellous bone from the ilium placed in the alveolar cleft without covering membrane have unpredictable outcomes and a high rate of resorption if compared to corticocancellous blocks (Swan and Goodacre, 2006; Rawashdeh and Telfah, 2008; Baqain et al., 2009).
Several techniques for alveolar cleft augmentation using autogenous bone had been reported in the literature. These techniques include cancellous bone grafting with nasal flap suturing (Kindelan et al., 1997; Long et al., 2000; Feichtinger et al., 2007), pyramidal iliac corticocancellous block placement with the cortical aspect facing the nasal mucosa and filled with cancellous chips (Cho-Lee et al., 2013), autogenous iliac particulate bone housed within resorbable or nonresorbable membrane (Peled et al., 2005) or titanium mesh with screw fixation (Akahashi et al., 1999), iliac cortex bone plate grafted into the palatal deficiency and particulate marrow and cancellous bone packed between the cortical bone and the reconstructed nasal flap (Ishii et al., 2002), 2 labio-palatal cortical bone plates from the mandibular symphysis without screw fixation or particulate bone in between (Mikoya et al., 2010), and finally 2 iliac corticocancellous blocks with interspaced cancellous bone was reported as a regrafting technique for dental implant placement in residual alveolar clefts in adult patients (Van Nhan et al., 2018).
The aim of this study was to evaluate the double iliac corticocancellous bone plates grafting technique for initial alveolar cleft grafting in patients with complete unilateral alveolar clefts at the phase of mixed dentition.
Patients and Methods
This was a prospective study conducted on 12 patients consecutively recruited from the outpatient clinic. The study was approved by the Research Ethics Committee and it followed the Declaration of Helsinki on medical research. Patients were selected according to the following criteria: complete unilateral alveolar cleft patients at the phase of mixed dentition with corrected cleft lip and palate. All enrolled patients did not receive pervious orthodontic treatment. Patients with cleft palate, fistulae, and bilateral alveolar cleft were excluded. For all eligible patients, alveolar cleft reconstruction was performed using the double iliac corticocancellous bone plates grafting technique.
Preoperative Measurements of Alveolar Cleft Size
Preoperative computed tomography (CT) was obtained from all the patients using a multislice helical CT machine (I-CAT®Precise™ from I-CAT®Technology) to assess the defect and to estimate the desired graft dimensions. Labial and palatal maximum mesiodistal width of the alveolar cleft was measured at the widest area between the cleft margins, and the craniocaudal height of the cleft was measured from the crest of the alveolus to a point above the apex of the central incisor.
Surgical Procedures
All surgeries were performed under general anesthesia with nasotracheal intubation and controlled hypotension. Mepivacaine hydrochloride with 1:200 000 of Adrenaline solution (Scandonest 2% by Septodont) was injected at the surgical site for hemostasis.
Two vertical elliptical incisions were performed along the cleft margin from the labial to the palatal sides around the labial fistula if present. In the absence of a fistula, a medially placed vertical incision was performed over the alveolar cleft close to the premaxilla. The labial sulcular incision was carried along with 2 adjacent teeth medially and laterally; then, 2 vertical releasing incisions were performed. Those releasing incisions were then extended upwards and backwards into the buccal vestibule and brought forwards by about 5 mm to give the appearance of a hockey stick. Palatal sulcular incision was performed to the second premolar laterally and the central incisor medially. Full-thickness labial and palatal flaps were reflected and scar tissue within the bony cleft was excised. The labial flaps were carefully dissected ensuring an adequate nasal lining for watertight closure and sufficient sliding of the flaps allowing bone plate placement and flap closure (Figure 1).
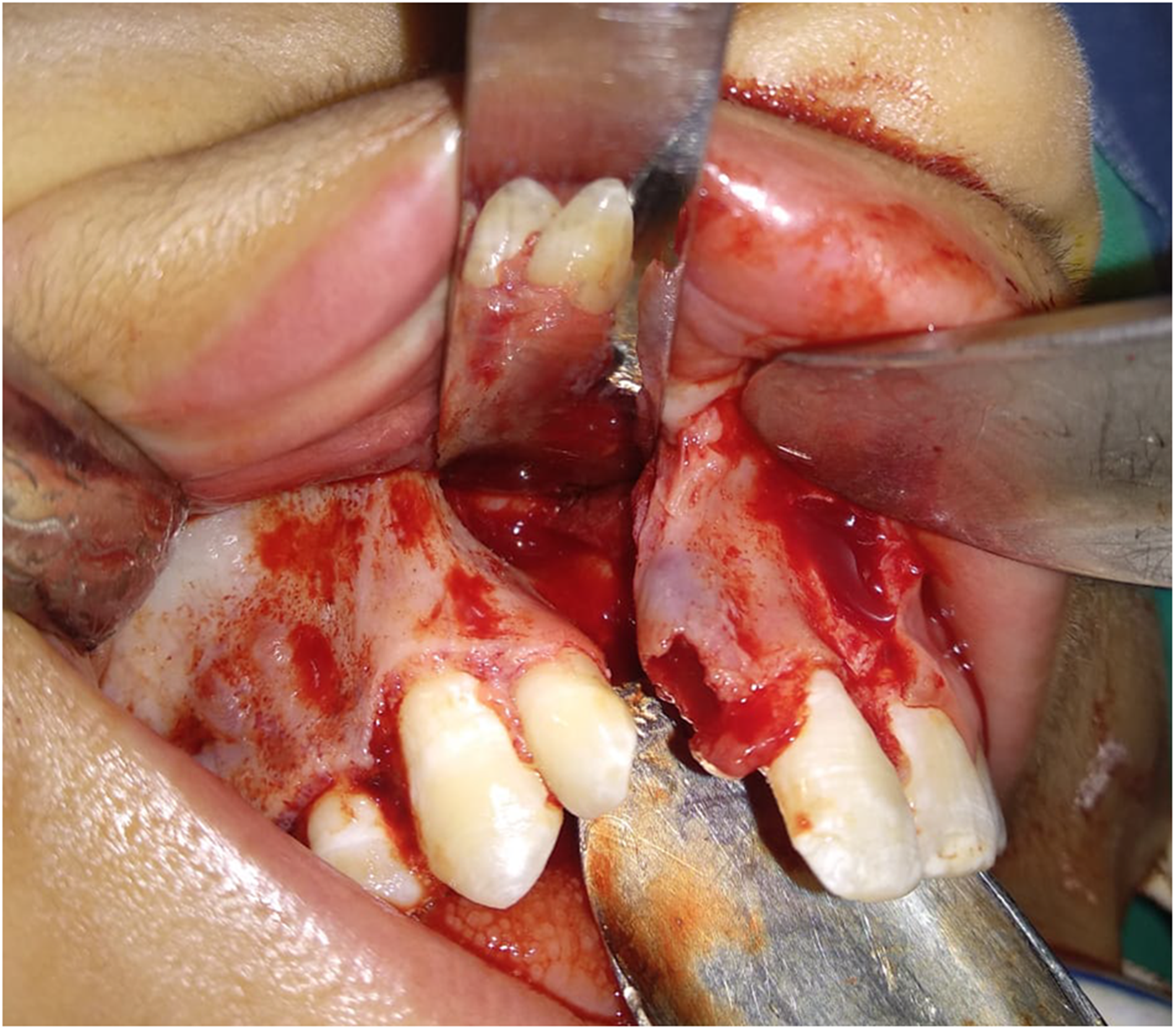
Intraoperative clinical photograph showing flap reflection with wide cleft exposure to accommodate the bone plates.
For iliac graft harvesting, the location of the anterosuperior iliac spine was marked and the skin incision was performed about 1 cm posterior to the spine. The margin of the anterior iliac crest was exposed and the external oblique muscle was subperiosteally elevated by cutting the fascia and periosteum. The subperiosteal elevation was extended medially to expose the medial aspect of the anterior iliac crest, and a medial monocortical bone window was performed using reciprocating saw and cutting discs. The dimensions of the window were measured correlated with the defective area labially and palatally based on the preoperative measurements of the cleft size. The osteotomies were then confirmed using a curved chisel. Finally, the medial window was opened and the medial cortical plate was harvested using spatula chisels. The cancellous bone was harvested using a large bone curette, as needed. A hemostatic sponge was placed, and layered closure of the wound was performed using Vicryl 4.0 (Polyglactin 910; Ethicon) for deep tissues and proline 4.0 for the skin layer.
Graft bed was prepared through 3 superficial bone fenestrations at the interior sides and edges of the cleft using a size 2 round bur. The harvested monocortical bone plate was cut into 2 cortical bone plates. The 2 cortical bone plates were trimmed to wall the defective cleft area labio-palatally. One bone plate was fixed labially using 2 mini-screws to wall the defective gap and rest on 3 to 5 mm sound bone mesial and distal to the cleft margins creating the labial bone plate (Figure 2). Similarly, the other bone plate was fixed palatally using 1 or 2 mini-screws creating the palatal bone plate, the inserted screws were monocortical and placed in areas of sound bone (Figure 3). The created walled gap was then tightly packed with harvested particulate cancellous bone. Finally, the flaps were approximated, and tension-free closure was achieved in an interrupted fashion using Vicryl 4.0 (Polyglactin 910; Ethicon).
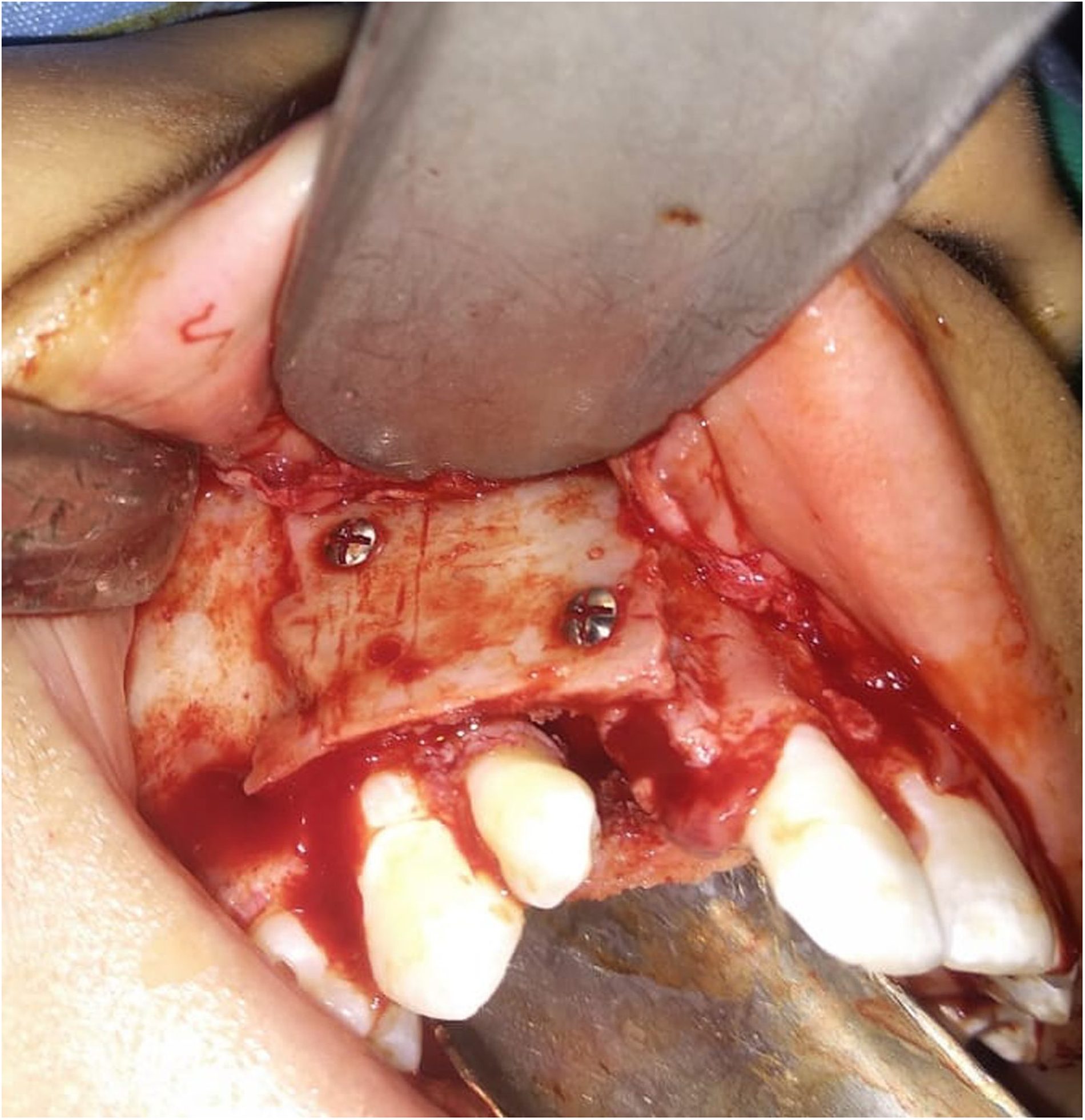
Intraoperative clinical photograph showing the labial bone plate fixed in place using 2 mini-screws.

Intraoperative clinical photograph showing the palatal bone plate fixed in place using 1 mini-screw.
Postoperative Follow-up and Outcomes
A dressing was applied to the donor site for 48 h postoperatively and the suture was removed 7 days postoperatively. While for the recipient site, the patients were instructed to apply icepacks over the upper lip area for 20 min every hour for 6 h postoperatively and to rinse their mouth with warm saline solution starting on the second day after surgery, 3 times per day during the first week postoperatively. The patients were kept on a soft diet for the first 48 h. Postoperative antibiotics, analgesics, and antiinflammatory drugs were prescribed for 5 to 7 days. Postoperative clinical follow-up was carried out every day for the first week and then every month for 9 months to evaluate wound healing at both the donor and recipient sites and to assess the presence of any complication as flap dehiscence, infection, and fistula formation
CT scans were obtained within 1 week, and 9 months postoperatively to assess the bone width, height, and density. Labio-palatal alveolar width and bone density were measured on the 9 months CT at the grafted side and compared to the contralateral side (Stasiak et al., 2021). On the axial cut at the center of the grafted side; a line was drawn from the mid-sagittal plane reaching the lateral periphery of the grafted area and passing through its center. Another line of the same length was drawn at the contralateral side. Three different points were selected at equal distances along the created central lines bilaterally. Labio-palatal alveolar width was measured at these points bilaterally through drawing lines passing labio-palatally through these points and perpendicular to the previously constructed 2 central lines (Figure 4). On the same axial cut; bone density was measured at the center of the grafted area and the same area of the contralateral side (Figure 5). Bone height change assessment was performed through reorientation and superimposition of the immediate postoperative CT images over the 9 months postoperative CT images. On the sagittal view at the center of the grafted side, the crestal difference between the superimposed images was recorded to evaluate the amount of crestal bone resorption (Figure 6).
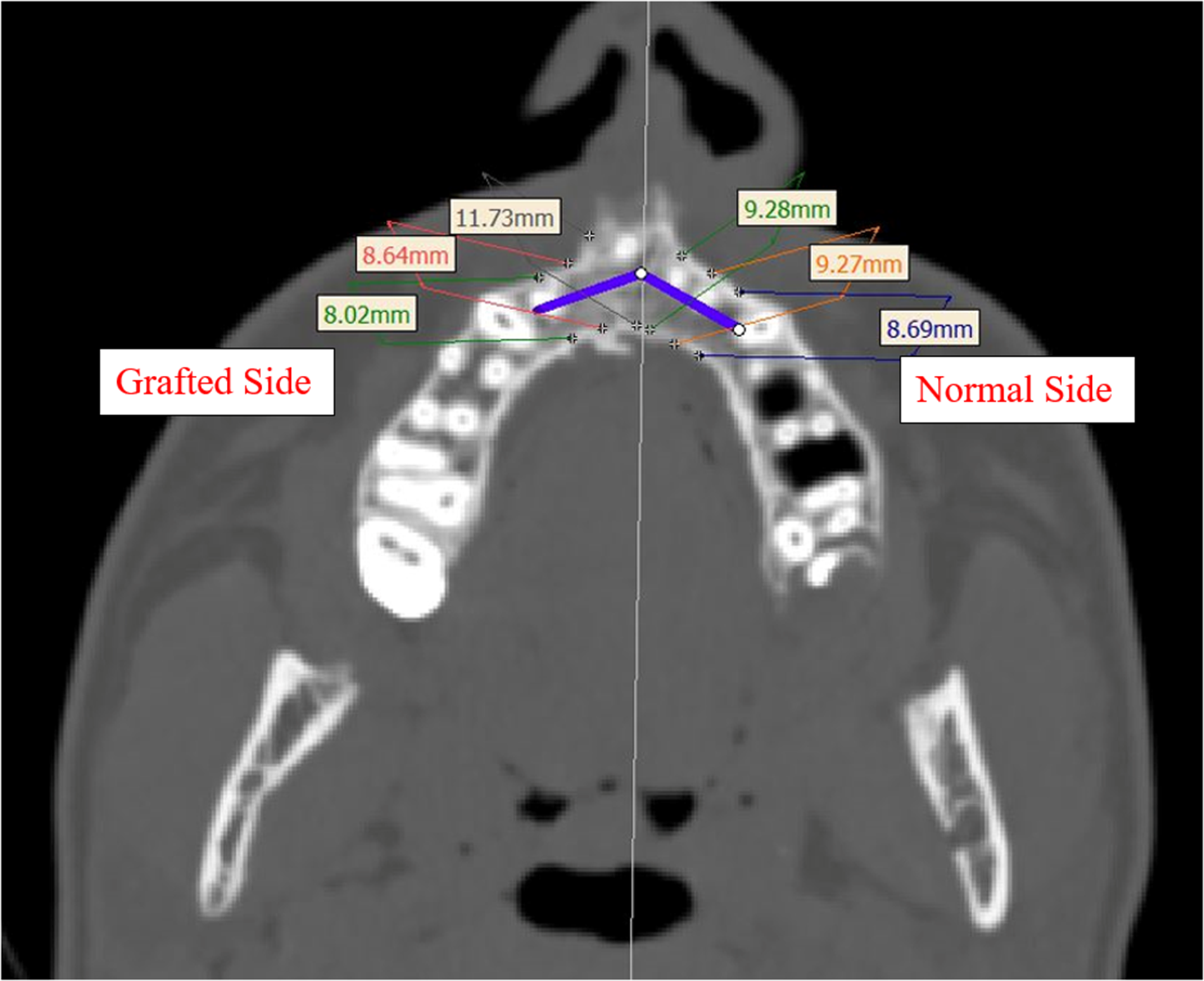
Nine-month postoperative computed tomography (CT; axial view) showing the assessment method of labio-palatal alveolar width compared to the contralateral side.
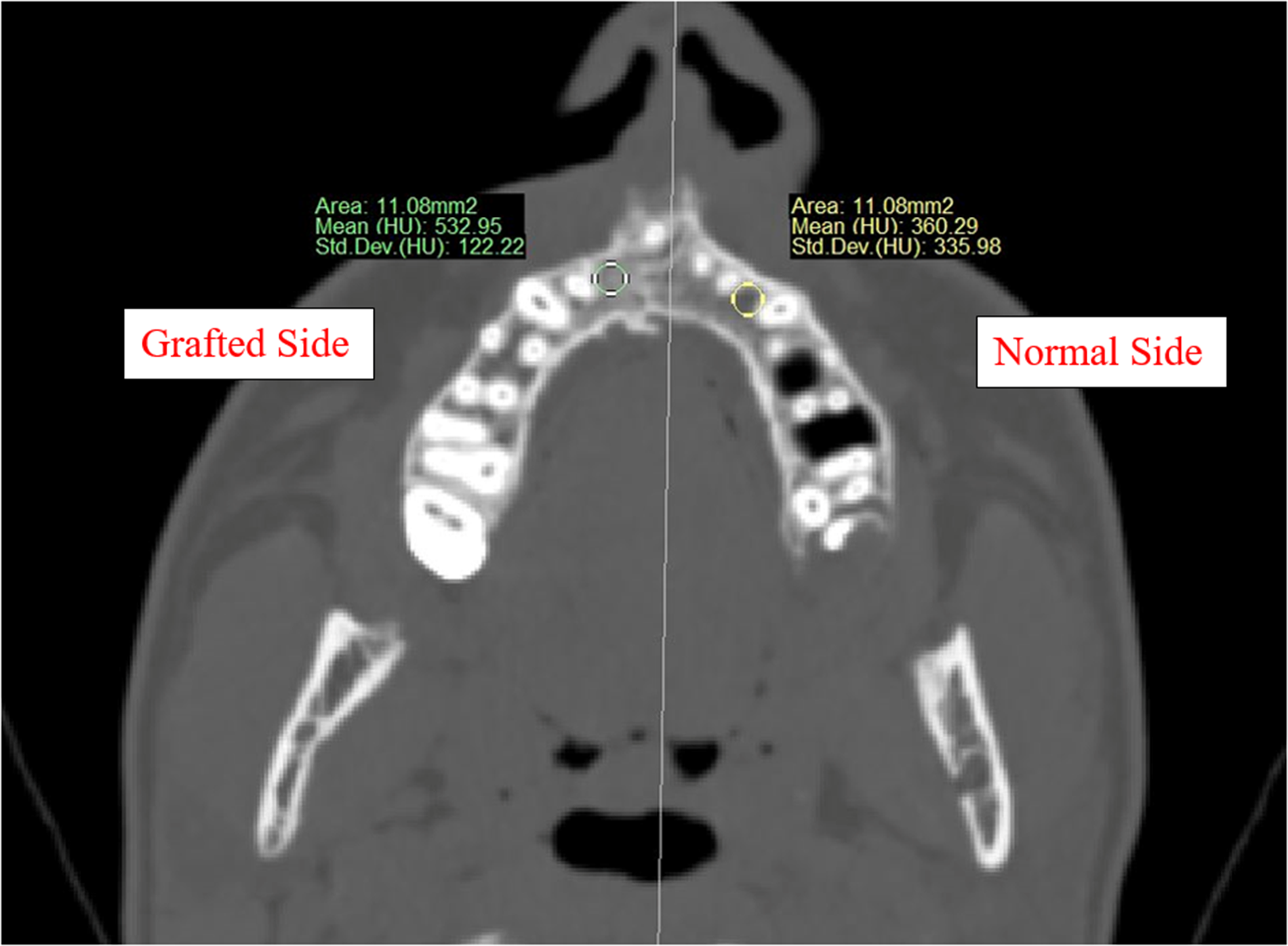
Nine-month postoperative computed tomography (CT; axial view) showing the assessment method of alveolar bone density compared to the contralateral normal side.
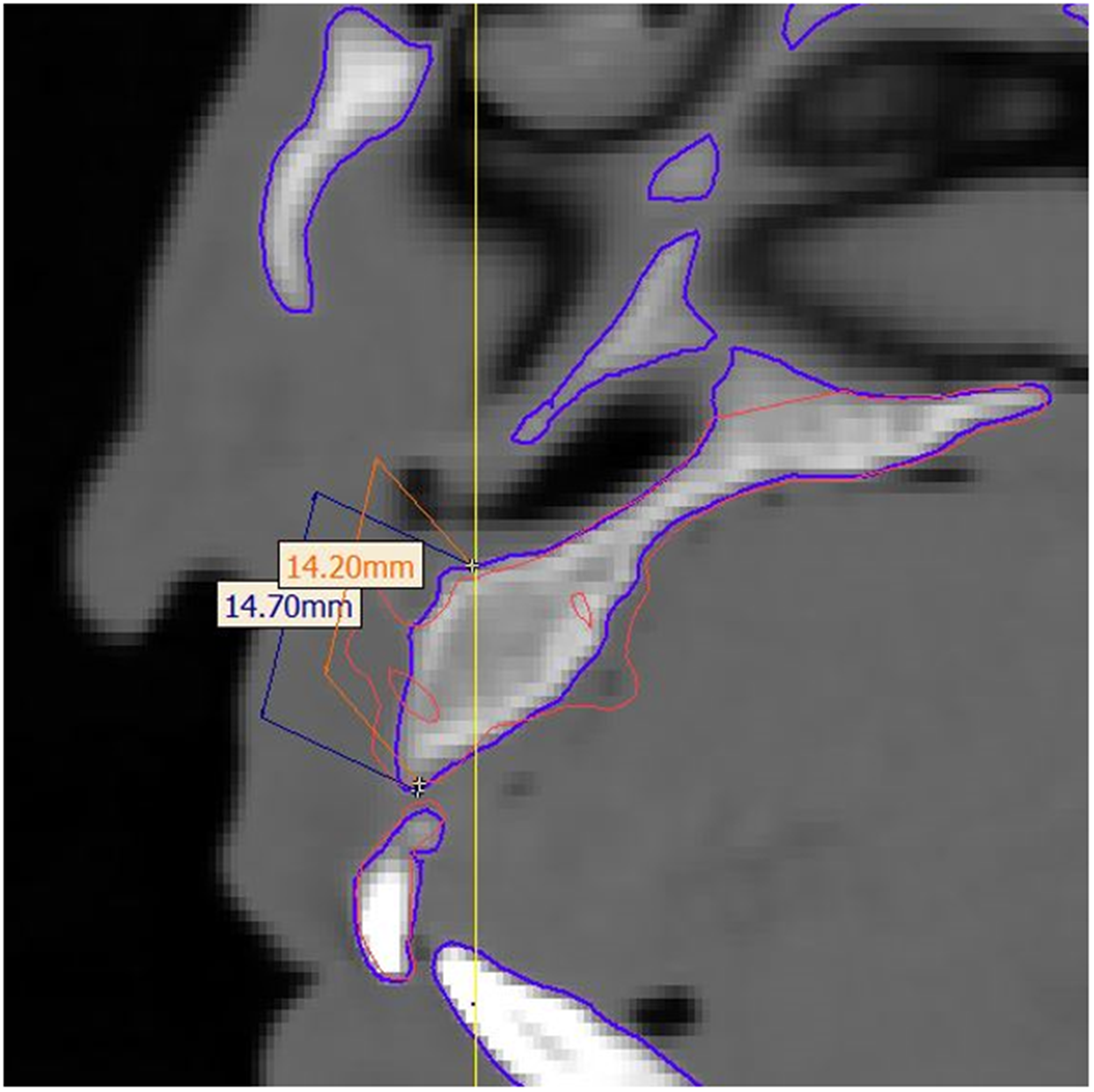
Computed tomography (CT; sagittal view) showing the height difference between the immediate postoperative versus 9 months postoperative graft height.
Statistical Analysis
Statistical analysis was performed using SPSS (Statistical Package for the social sciences—IBM® SPSS® Statistics Version 22 for Windows, IBM Corp.). Quantitative data were represented as mean ± standard deviation. Qualitative data were represented as proportion. Data were explored for normality using Kolmogorov–Smirnov and Shapiro–Wilk tests. Data were normally distributed and paired t-test was used to compare variables between the cleft and normal sides. The results were considered statistically significant if the p-value was <.05.
Results
This study was conducted on 12 patients (7 males and 5 females) with unilateral complete alveolar cleft and previously closed cleft lip and palate, with a mean age of 10.1 ± 2.2 years. The defect was extended labio-palatally in the 12 patients. The mean defect height was 17.2 ± 1.5 mm, and the mean defect width was 13.1 ± 2.1 mm labially and 7.2 ± 2.4 mm palatally.
Double iliac corticocancellous bone plates grafting was performed for alveolar cleft reconstruction in all cases. The mean of the harvested graft dimensions was 17.7 ± 1.6 mm height and 29.6 ± 4.5 mm width. The surgical procedures were uneventful. Flap dehiscence was observed in 2 cases (16.6%).
A radiographic assessment after 9 months showed good bone bridge formation in the defective gap, with evidence of normal bony architecture. The labio-palatal alveolar width was comparable in the cleft and the normal sides (8.2 ± 0.9 and 8.4 ± 0.6 mm, respectively), and there was no statistically significant difference between both sides (p-value 0.174). The grafted side has a lower bone density (423.3 ± 80.1 HU) compared to the normal side (543.6 ± 90.2 HU), and there was a statistically significant difference (p-value .001). Ten patients showed minimal graft height loss after 9 months except the 2 dehiscence cases showed 1.9 and 2.4 mm bone loss. The average bone height loss for all cases was 0.97 ± 0.65 mm.
Discussion
Initial alveolar cleft grafting during mixed dentition phase prevents several complications and permits the permanent dentition to migrate and erupt normally through the cancellous bone with subsequent avoidance of secondary grafting (Boyne and Sands, 1972; Akahashi et al., 1999; Dempf et al., 2002; Bagheri et al., 2012; Cho-Lee et al., 2013). The double iliac corticocancellous bone plates technique had been used for regrafting of residual alveolar cleft for dental implant placement in adults and showed promising results (Van Nhan et al., 2018). In this study, we apply this technique early for initial alveolar cleft grafting to provide early oronasal closure, adequate bony support of teeth adjacent to the grafted defect, preventing the collapse of alveolar segments, and providing sufficient alveolar bone of good quality and quantity for future teeth migration or implant placement without the need for secondary grafting (Van Nhan et al., 2018).
The iliac crest was selected as a donor site as it provides the large bone volume required for the double corticocancellous bone plate grafting technique performed in the current study. Iliac bone harvesting is relatively simple. However, several potential complications had been reported ranging from pain and buttock anesthesia to gait disturbances (Swan and Goodacre, 2006; Sudhakar et al., 2017). but these complications are of low incidence and present for only a short time (Van Nhan et al., 2018).
Spongy bone derived from the iliac crest showed the highest amount of cellular marrow with abundant osteogenic cells that allow rapid vascularization of the graft, but the high resorption rate of the iliac spongiosa lowers its quality for bone grafting compared to iliac cortical bone (Canady et al., 1993; Swan and Goodacre, 2006). Thus, in the double corticocancellous bone plates technique, cortical bone plates were used to cover the defect buccally and palatally, and the spongiosa was used to fill the gap between the 2 plates. This technique aims to get benefit from the low resorption rate of the cortical bone plates and rapid vascularization of the spongy bone (Van Nhan et al., 2018). Moreover, cortical bone plates provided guided tissue regeneration as they act as a barrier that prevents the soft tissue migration into the graft and provides a favorable environment for bone formation (Bosshardt and Schenk, 2009), eliminating the need for membrane placement. Moreover, the flat anatomical architecture of the medial iliac cortex allowed easy bone plate harvesting, customization, adaptation, and fixation. The fixation method was depending on monocortical screws inserted in areas of sound bone to prevent adjacent teeth injury and provide adequate graft stability with subsequent proper healing.
In this study, complete oronasal fistula closure and alveolar cleft reconstruction were achieved in all cases. One-week postoperative flap dehiscence occurred in 16.6% of the cases. This was higher than flap dehiscence reported by Van Nhan et al. (9.4%) in their study on the double corticocancellous bone plates technique in residual alveolar cleft grafting for implant placement (Van Nhan et al., 2018). However, a recent systematic review showed that flap dehiscence with corticocancellous bone graft in cleft lip and palate patients occurred up to 16% (Ma et al., 2021). In our study, flap dehiscence was observed only in 2 cases, later follow-ups showed normal healing in all cases. In 1 case, the area of dehiscence was small and the wound healed spontaneously with close follow-up, chlorhexidine mouth wash, and daily warm saline irrigation. In the other case, healing occurred 14 days after superficial bone shaving using egg-shaped bur in addition to daily follow-up and irrigation.
Flap dehiscence in the current study can be explained by the significantly larger bone volume placed labially to overlap the defect margin, potentially increasing flap tension and leading to dehiscence compared with grafting of cancellous bone or a bone block only within the cleft defect (Feichtinger et al., 2007; Cho-Lee et al., 2013).
According to radiographic assessment after 9 months, all cases showed good bone bridge formation with normal bony architecture. The alveolar bone width was comparable to the contralateral side providing normal ridge contour and symmetry. The grafted side showed statistically significant lower bone density compared to the normal side, However, the difference is considered acceptable and has no clinical significance, as both sides lie within the average density of the bone in the anterior maxilla (Fuh et al., 2010; Wakimoto et al., 2012). The final alveolar height loss was 1 mm providing adequate bone around the neck of the adjacent teeth.
Conclusion
Within the limitations of this study, the double iliac corticocancellous bone plates technique is considered a promising technique for alveolar grafting in patients with complete unilateral alveolar clefts at the phase of mixed dentition. This technique can eliminate the need for delayed grafting, facilitate normal teeth eruption, and provide adequate bone for future implant placement, subject to further studies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.