
Abstract
Introduction
Furlow double-opposing Z-plasty (DOZ) lengthens the soft palate; however, this lengthening is achieved at the expense of increased mucosal flap tension. Thus, its use is limited in patients with severe tension applied on mucosal flap after DOZ. In this study, DOZ was combined with a buccal fat pad (BFP) flap to maximize palatal lengthening and muscle repositioning.
Methods
This study included patients who underwent surgical correction for velopharyngeal insufficiency between December 2016 and February 2019. Patients with more than moderate degree hypernasality following primary palatoplasty were included in the study. Patients younger than 4 years of age, those with a submucous cleft palate, or syndromic patients were excluded. Speech outcomes were investigated for those who underwent DOZ only (DOZ group, n = 17) and those in whom a BFP was used (BFP group, n = 15) pre- and postoperatively. The velopharyngeal gaps between the uvula and pharyngeal wall were measured before and immediately after surgery to estimate the palatal length.
Results
Most patients who received a BFP showed improvement in hypernasality. However, the hypernasality of the DOZ group was more severe than that of the BFP group (p = 0.023). The extent of palatal lengthening was 4.4 ± 1.7 mm and 7.5 ± 2.1 mm in the DOZ and BFP groups, respectively (p = 0.001).
Conclusions
BFPs reduced the tension of the DOZ mucosal flap and maximized palatal lengthening and muscle repositioning. They promoted velopharyngeal closure in patients with moderate and moderate-to-severe velopharyngeal insufficiency. Hence, our method improves the surgical outcomes of patients with velopharyngeal insufficiency after primary palatoplasty.
Introduction
In velopharyngeal insufficiency (VPI), the velum and pharyngeal wall are not in contact with each other; hence, they cannot close the nasopharyngeal space (Gart and Gosain, 2014). This results in air leakage through the nose and hypernasality while speaking, which hinders speech intelligibility (Perry, 2011). Velopharyngeal insufficiency is seen in a large number of patients who have undergone primary palatoplasty for a cleft palate. The VPI rate after primary palatoplasty varies from 5% to 36% (Yamaguchi et al., 2016).
Surgical correction of VPI is indicated in patients refractory to speech therapy. Various surgical methods have been introduced for the correction of VPI. Commonly performed procedures include pharyngeal flap surgery, sphincter pharyngoplasty, posterior pharyngeal wall augmentation, and Furlow double-opposing Z-plasty (DOZ). Pharyngeal flap surgery and sphincter pharyngoplasty are reportedly effective in severe VPI. However, they may result in airway problems (Glade and Deal, 2016). In contrast, DOZ shows excellent results in patients with mild-to-moderate VPI. However, the extent of palatal lengthening in DOZ is limited in severe cases.
The Furlow DOZ achieves palatal lengthening at the expense of increased tension in the midline and right-side oral mucosal flap (Hsu et al., 2015). The defect caused by posterior rotation of the left-side oral musculomucosal flap during DOZ surgery is covered by the right-side oral mucosal flap. With the need for more extensive palatal lengthening, a larger defect is caused on the anterior side. In addition, increased tension is applied on the right-side oral mucosal flap. This increased tension can lead to an oronasal fistula and severe scarring (Qiu et al., 2019). This severe scarring limits palatal lengthening and muscle repositioning, and results in poor speech outcomes in patients with VPI.
The buccal fat pad (BFP) is suitable for palate surgery. The BFP flap can provide additional tissue for the soft palate and can release the tension on the right-side oral mucosal flap. We hypothesized that DOZ with a BFP flap could maximize palatal lengthening and muscle repositioning, and improve surgical outcomes. In line with this, this study aimed to compare the speech outcomes between patients who underwent palatoplasty with the Furlow technique with and without the BFP flap. Additionally, we also analyzed the efficacy of DOZ with a BFP flap in patients with moderate and severe VPI, which was assessed via speech analysis.
Methods
This retrospective chart review included patients who underwent DOZ or DOZ with a BFP flap for VPI correction after primary cleft palate repair. Patient demographics, primary palatoplasty type, and speech analysis outcomes were reviewed. VPI surgeries were conducted by a single senior surgeon (T. S. Oh) at Asan Medical Center between December 2016 and February 2019.
Patients who had undergone VPI surgery due to hypernasality of more than moderate degree were included in the study. Patients younger than 4 years of age at the time of surgery or those with syndromes were excluded because their language capabilities were not suitable for speech analysis. Patients with less than 6 months of follow-up, non-cleft VPI, an oronasal fistula, and a submucous cleft palate were excluded. Patients who underwent DOZ surgery in their primary palatoplasty were also excluded. Finally, 32 patients were included. Among them, 17 and 15 patients underwent DOZ only (DOZ group) and DOZ with a BFP flap (BFP group), respectively. The single DOZ procedure was used for patients who underwent VPI correction between December 2016 and January 2018. The BFP flap has been used since January 2018 in patients with more than moderate VPI.
Speech assessment was performed every six months after primary palatoplasty. At 3 years of age, patients with mild hypernasality underwent speech therapy based on the results of the speech assessment. In patients with severe hypernasality, visual intraoral examination was conducted. Patients who showed minimal soft palate contracture in intraoral examinations were evaluated for pharyngeal wall motion using a nasopharyngoscopy. If the soft palate showed contracture and decreased mobility, the VPI was surgically corrected. Since November 2017, DOZ with a BFP flap has been performed for the correction of more than moderate VPI.
Speech therapy was initiated in all the patients one month after their surgery. This continued for one year. The postoperative speech therapy protocol was similar in both groups. Their speech was assessed twice at 6 and 12 months after the surgery. The findings obtained 12 months after the surgery were used for analysis. At one year after the VPI correction, a nasal endoscopy was conducted in patients who still showed VPI on speech assessment. If the pharyngeal wall motion was within the normal range, DOZ was repeated. However, if the pharyngeal wall motion was compromised, VPI was corrected via posterior pharyngeal flap surgery.
The diagnosis of VPI was made by intraoral examination and perceptual speech assessment. The perceptual speech assessments included articulation, nasal emission
The velopharyngeal gap in relaxation was subsequently measured. The velopharyngeal gap was defined as the shortest distance from the uvula to the pharyngeal wall. The gap was measured in the operating room before and immediately after surgery, under general anesthesia. The amount of palatal lengthening was calculated as the difference in the velopharyngeal gap before and after the surgery.
Surgical Technique
The surgical technique performed in DOZ was similar to that described by Furlow (1986). After the Z-plasty incisions on the oral mucosa, the levator muscle was released from the scar tissue and separated from the oral and nasal mucosa. The levator veli palatini muscles were thoroughly dissected. After that, a nasal-side Z-plasty was conducted. The BFP flap was not used for nasal lining closure in both groups. The end of the levator was then sutured to the base of its counterpart for overlapping intravelar veloplasty. The levator muscle was retro-positioned in the transverse direction with adequate tension.
In the BFP group, a longitudinal incision was made in the buccal mucosa just posterior to the maxillary alveolar ridge to harvest the BFP flap. The incision line was located posterior to the parotid duct opening. This opening should not be injured, which was why care was taken in performing this step. The buccopharyngeal fascia and buccinator were exposed and dissected. Pressure was applied to the cheek, and the BFP was gently pulled through the incision with smooth forceps. After obtaining a sufficient length, the flap was tunneled submucosally into the palatal repair site.
The BFP flap was then fixed to the posterior side of the hard palate. Part of the BFP flap filled the dead space between the nasal and oral mucosa. The oral mucosal flap was transposed and sutured. In the BFP group, the anterior triangular defect between the hard and soft palates was covered with a BFP flap. The BFP flap was then sutured to the surrounding oral mucosal margin (Figure 1). Both groups were fed with a liquid diet until postoperative day three. Both groups then switched to a soft diet until postoperative day 14. The diet was gradually changed to a more solid one after postoperative day 14.

Buccal fat pad flap surgical procedure. (a) The Z-plasty was designed using the left musculomucosal and right mucosal flaps on the oral-side mucosa. The lateral limb of the Z-plasty was extended to the medial side of the maxillary tuberosity. (b) The superior pharyngeal constrictor and levator veli palatini muscles were released from the scar tissue. The levator veli palatini muscles were sutured in the transverse direction with adequate tension. (c) After repairing the oral mucosal flap, the defect persisted on the left anterior side. The buccal fat pad flap was harvested through a longitudinal incision of the buccal mucosa around the second molar. (d) The buccal fat pad flap filled the dead space between the nasal and oral mucosa and was sutured to the oral mucosa.
Statistical Analyses
Continuous and ordinal variables, including age, follow-up period, and hypernasality grade were analyzed by conducting a Mann–Whitney U test. Categorical variables, including sex, palatoplasty type, and speech analysis outcomes were assessed via the Fisher’s exact test. Differences with p values of < 0.05 were considered statistically significant. Statistical analyses were conducted using the IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA).
Results
This study included 17 and 15 patients treated with DOZ alone or DOZ with a BFP flap, respectively (Table 1). The patients’ mean ages were 6.0 ± 3.5 years and 4.8 ± 1.4 years for the DOZ and BFP groups, respectively. The mean follow-up periods were 13.4 ± 3.2 and 12.1 ± 3.0 months in the DOZ and BFP groups, respectively. There were no differences in age, sex, and follow-up periods between the two groups. The distributions of the Veau classes in both groups were not different (p = 0.65). For the repair of the hard palate in the primary palatoplasty, the vomerine flap (three flap) was used in patients with a bilateral or wide cleft palate, while the Bardach two flap (two flap) was used in those with a unilateral cleft palate. Radical intravelar veloplasty and straight-line repair were performed for soft palate repair in primary palatoplasty. The levator muscle was dissected, repositioned, and reapproximated at the midline. There was no significant difference in the primary palatoplasty type between the two groups (p = 0.44).
Characteristics of Patients with Velopharyngeal Insufficiency (VPI).
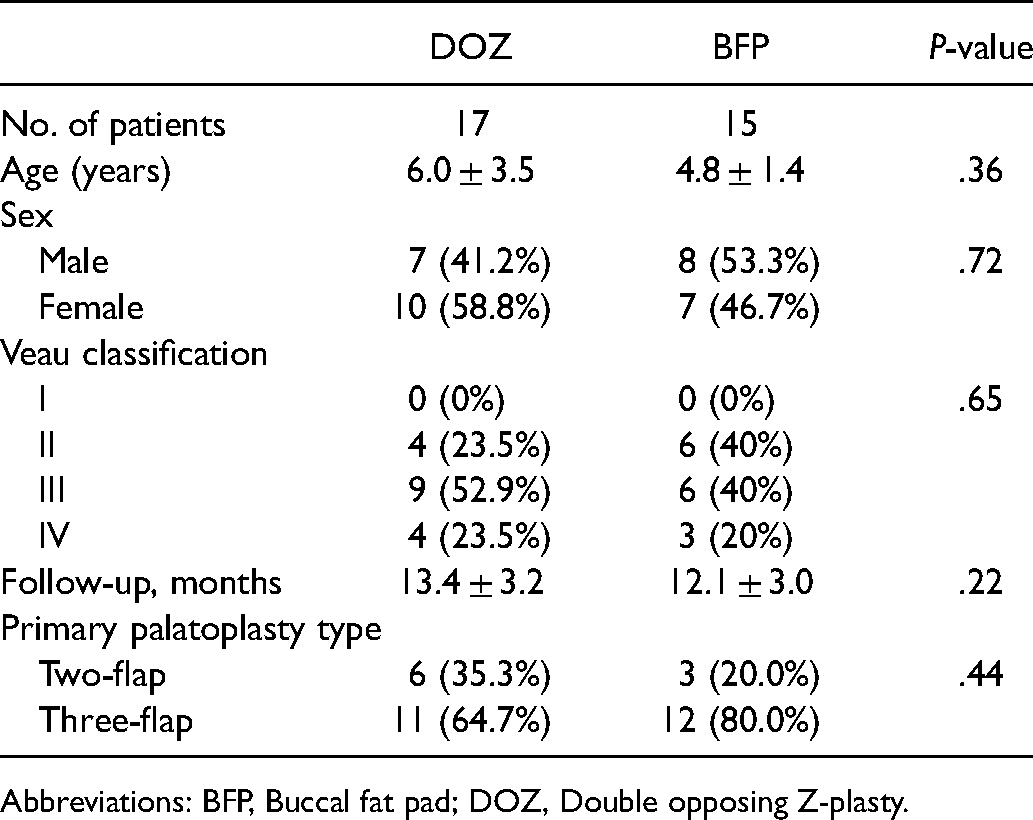
Abbreviations: BFP, Buccal fat pad; DOZ, Double opposing Z-plasty.
The preoperative hypernasality severity in the BFP and DOZ groups is presented in Table 2. Before the surgery, severe hypernasality was the most common in both groups (DOZ: n = 7 vs BFP: n = 7). This was followed by moderate-to-severe (DOZ: n = 6 vs BFP: n = 2) and moderate VPI (DOZ: n = 4 vs BFP: n = 6). The distribution of the hypernasality severity was not different between the groups (p = 0.78). Patients with articulatory problems and compensatory, developmental, and obligatory errors did not differ between the two groups preoperatively.
Speech Analysis and Velopharyngeal gap Before Surgery.
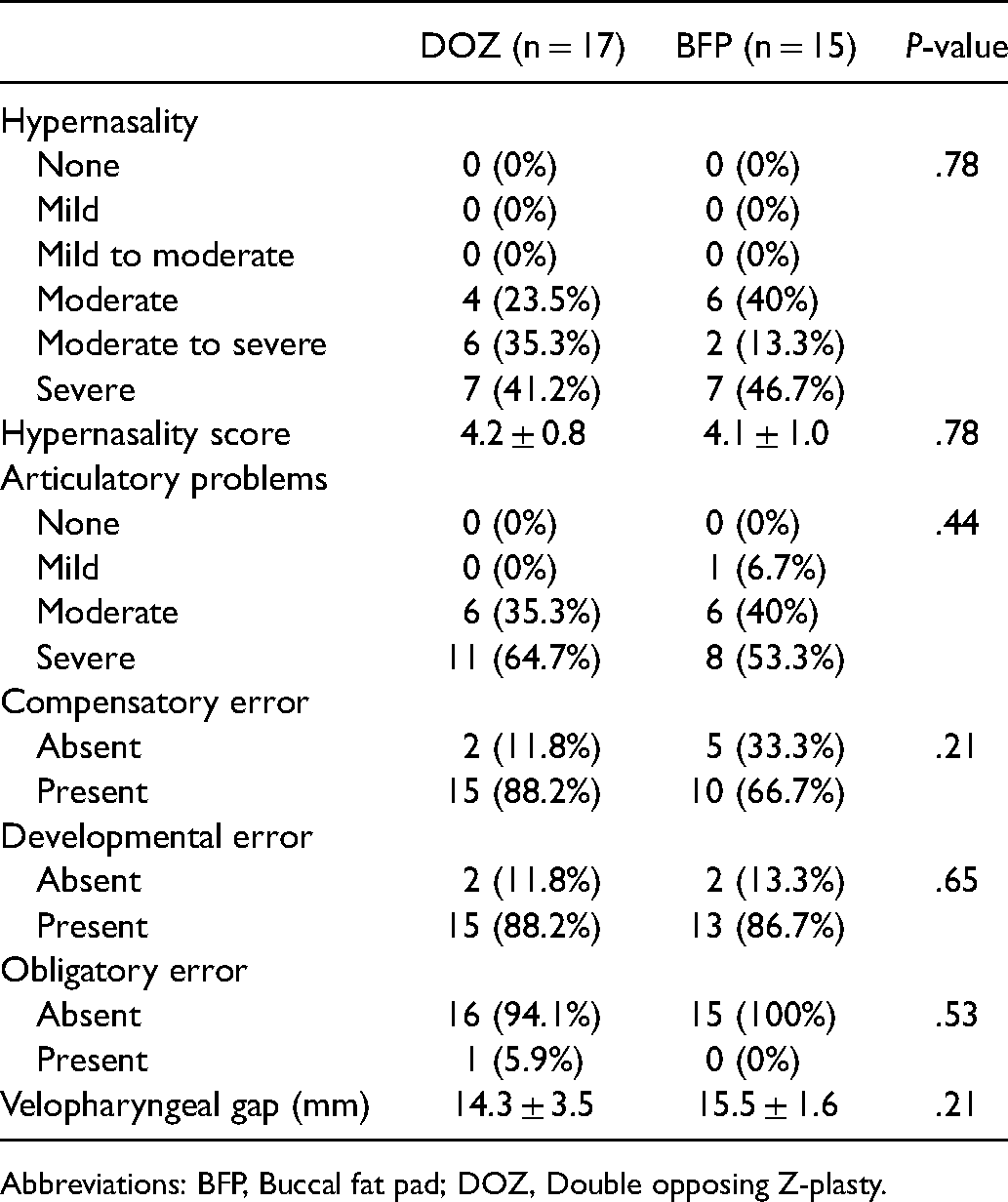
Abbreviations: BFP, Buccal fat pad; DOZ, Double opposing Z-plasty.
Speech analysis results showed that hypernasality improved. In addition, there was a shift to a milder state in both groups after surgery (Table 3). There were more patients with mild (DOZ: n = 3 vs BFP: n = 5) and mild-to-moderate (DOZ: n = 6 vs BFP: n = 6) hypernasality postoperatively than preoperatively. However, the DOZ group had more severe hypernasality than the BFP group (p = 0.023). Several patients still had moderate-to-severe (DOZ: n = 4 vs BFP: n = 1) hypernasality.
Speech Analysis and Velopharyngeal gap After Surgery.
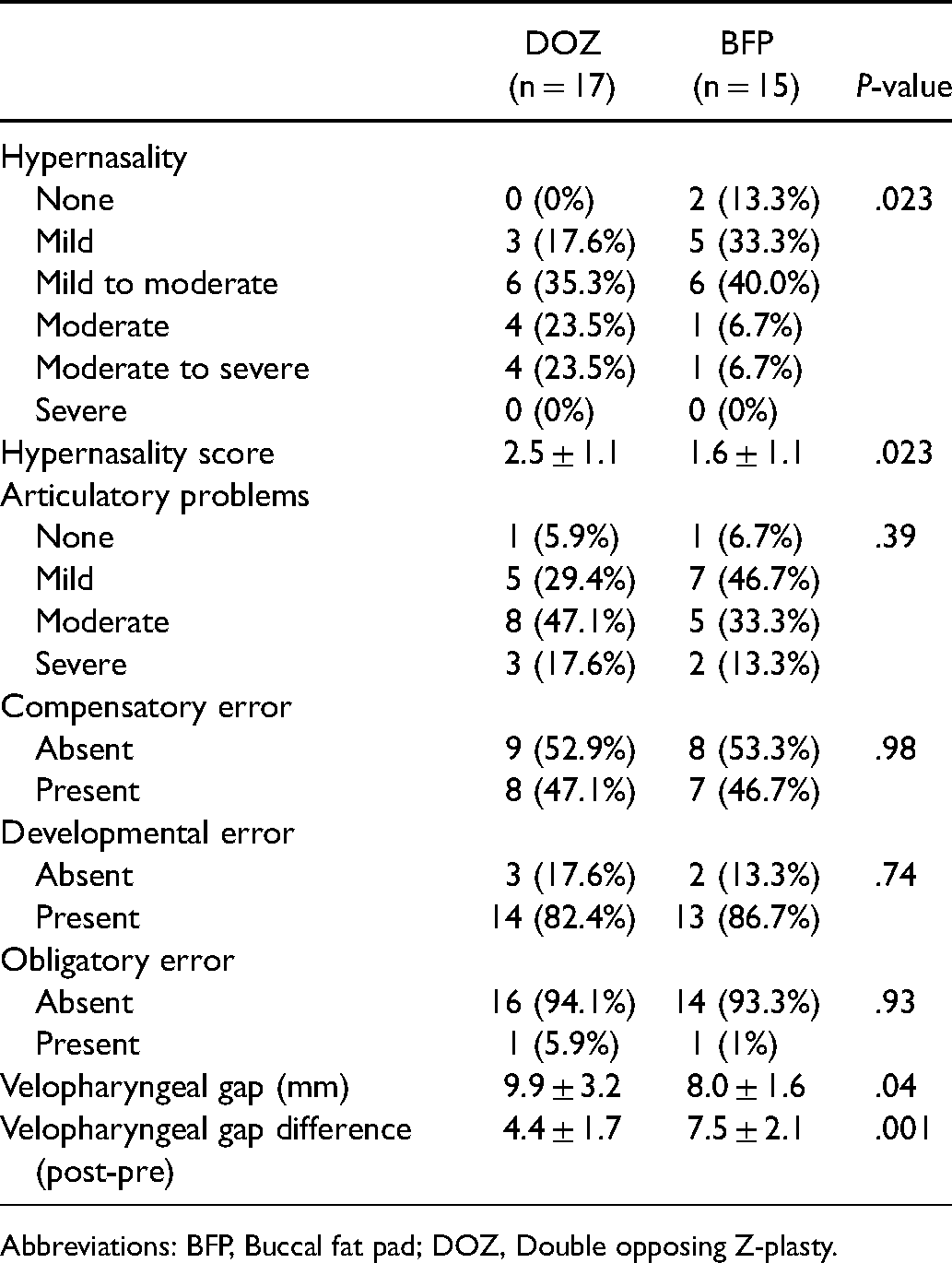
Abbreviations: BFP, Buccal fat pad; DOZ, Double opposing Z-plasty.
The articulatory problems were also improved after surgery in both groups. There were more patients with no (DOZ: n = 1 vs BFP: n = 1) and mild (DOZ: n = 5 vs BFP: n = 7) articulatory problems postoperatively than preoperatively. The compensatory, developmental, and obligatory errors did not differ between the two groups after surgery.
The mean hypernasality scores before surgery were 4.2 ± 0.8 and 4.1 ± 1.0 in the DOZ and BFP groups, respectively (p = 0.78). The hypernasality scores decreased after surgery. Moreover, they were significantly low in the BFP group (DOZ 2.5 ± 1.1 vs BFP 1.6 ± 1.1; p = 0.023).
The velopharyngeal gap before surgery was not different in both groups, as shown in Table 2 (p = 0.21). The differences before and after surgery were 4.4 ± 1.7 and 7.5 ± 2.1 mm in the DOZ and BFP groups, respectively. The extent of palatal lengthening was significantly larger in the BFP group than in the DOZ group (p = 0.001).
No surgical complications such as postoperative bleeding, infection, flap necrosis, flap dehiscence, oronasal fistula, or airway problems were observed in the BFP group. However, one patient in the DOZ group developed an oronasal fistula in the hard palate and soft palate junction 8 months after his/her VPI surgery, which required additional surgery for closure.
Discussion
A BFP is an encapsulated and vascularized fat tissue that is similar to the periorbital fat tissue (Saralaya et al., 2020). It is uniquely separated well from the surrounding tissues and is suitable for use in patients with palatal defects (Scott et al., 2004). Since the first introduction of the usage of the pedicled BFP flap in palatal defects, the use of BFP flaps in palatal or maxillary defects has gained popularity (Egyedi, 1977).
Various factors, such as levator position and function, palate length, and pharyngeal function, are correlated with VPI. DOZ has been a preferred method for the correction of VPI because it lengthens the soft palate via Z-plasty without a straight-line scar and repositions the levator palatini fibers into a more physiological direction. DOZ involves three mechanisms in improving VPI: velar elongation, levator retroposition, and velar tightening (Pet et al., 2015). However, in patients with a short palatal length or firm palatal tissue, the amount of velar elongation and levator retroposition is limited due to scanty healthy tissue. Furthermore, in those with an extremely short palatal length, a triangular defect may developed due to the size discrepancy between the two oral-side flaps (Figure 2). The defect can be closed by advancing and rotating the right-side oral mucosal flap. However, this imposes tension on the oral mucosal flap and limits palatal elongation and muscle retropositioning. Therefore, adding a healthy BFP flap on the triangular defect results in the reduction of tension in the oral-side mucosal flap, velar lengthening, and levator repositioning, which can be achieved even in patients with a short or firm soft palate.
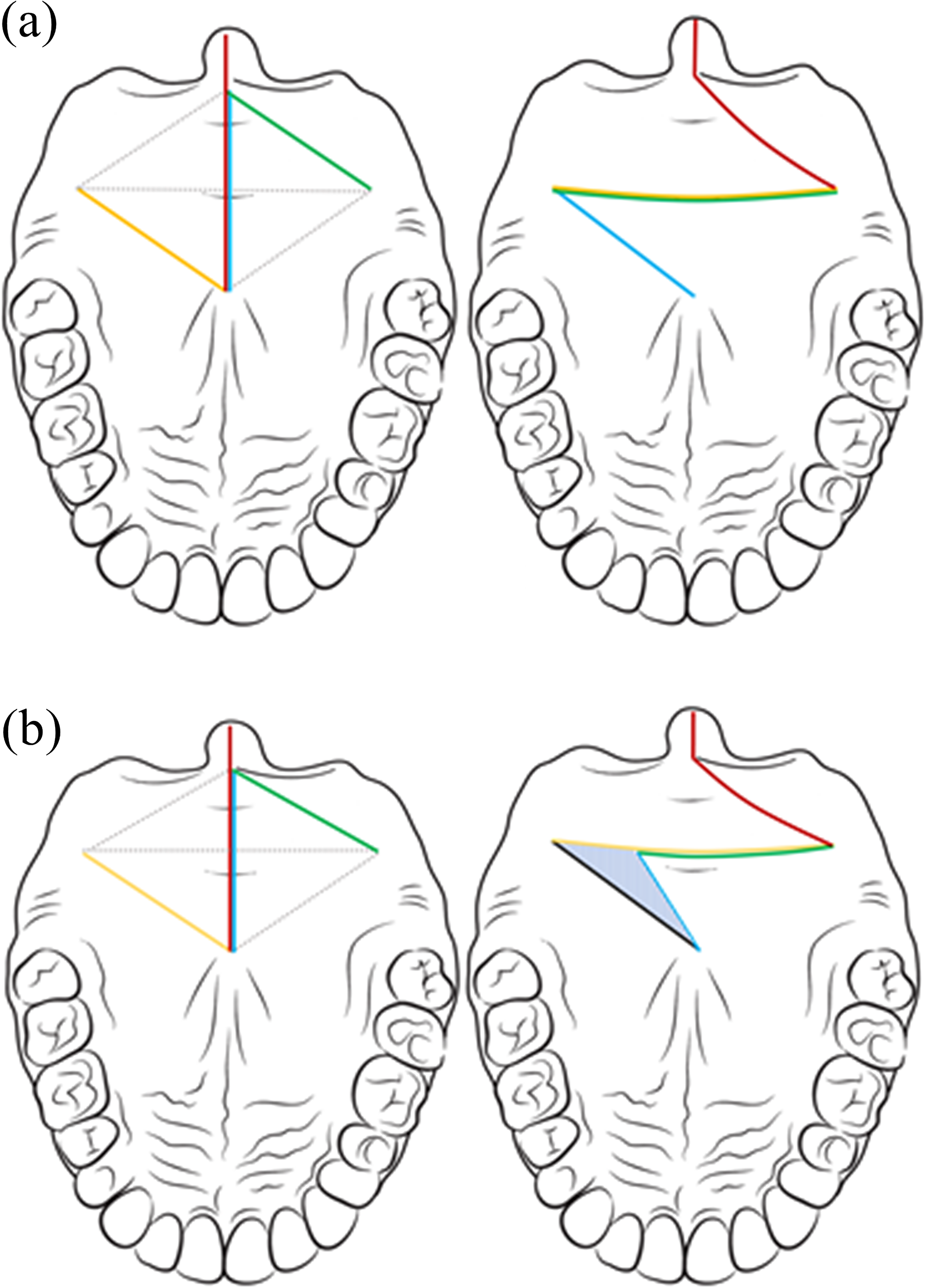
Flap design and postoperative appearance in patients with mild and severe velopharyngeal insufficiency (VPI). (a) In patients with mild palatal shortening, direct closure was possible because the size difference between the oral mucosal and oral musculomucosal flaps was minimal. (b) However, in patients with severe palatal shortening, the difference in the lengths of the green and yellow lines was larger than that in mild palatal shortening. After flap transposition, a triangular defect (blue striped area) occurred due to the difference in size between the two flaps. The shorter the length of the palate, the greater the difference in length between the yellow and green lines. The defect size also became more extensive.
Various attempts have been made to overcome the limitations of the DOZ method. For instance, a buccal flap, a random-pattern mucosal flap, can be used in patients with VPI to supply additional tissue (Mann et al., 2017). However, this requires buccal flap division and inset in the second stage of the operation, which leaves a long scar on the buccal mucosa. The facial artery musculomucosal (FAMM) flap can also be used. However, it entails a long surgery and requires dissection, which leaves significant scar tissue around the maxilla (Lee and Alizadeh, 2016; Mannino et al., 2020). An acellular dermal matrix (ADM) has been used for its quick incorporation into tissues and its resistance to wound contracture (Aldekhayel et al., 2012). However, the long-term safety of the ADM remains unknown. Additionally, in the authors’ experience, the ADM is mostly absorbed and replaced by scar tissue, which results in poor long-term VPI patient outcomes. Thus, the buccal flap, FAMM flap, and ADM are not our first-line courses of treatment in patients with VPI.
In our study, most of the patients who received BFP flaps showed improvement in hypernasality. The BFP flap showed favorable results in patients with moderate, moderate-to-severe, and severe hypernasality. The speech results were much improved in the BFP group compared with those in the DOZ group.A total of four patients still had moderate-to-severe hypernasality even after VPI correction in the DOZ group. They had a history of a bilateral cleft palate, where the cleft width was wider than that in patients with a unilateral cleft palate. In a bilateral cleft palate, available healthy tissue is usually scanty. In addition, the single DOZ surgery has limitations in terms of palatal lengthening and muscular repositioning. They eventually underwent a pharyngeal flap surgery to improve the VPI. On the other hand, one patient in the BFP group also showed moderate-to-severe hypernasality despite the usage of the BFP flap. This patient had a dysfunctional velum, which was detected on examination after the VPI correction. The patient eventually underwent a pharyngeal flap surgery.
The BFP flap promotes mucosalization and results in less scarring (Baumann and Ewers, 2000; Saralaya et al., 2020). The BFP flap was replaced with red granulation tissue within 1 week after surgery and was mucosalized with mild contracture within 3 to 4 weeks (Figure 3).

Mucosalization of the buccal fat pad flap. The buccal fat pad flap right after surgery (a) and at the 3-week follow-up (b). The flap was covered with red mucosa.
Using a BFP flap with DOZ has several advantages. When performing DOZ, the right-side oral mucosal flap has less redundancy and has limited flap advancement because the flap base is located near the hard palate. In contrast, the left-side oral musculomucosal flap is easy to advance because the flap base is located on the soft palate. As mentioned above, in patients with severe VPI, a defect remains after DOZ. Otherwise, excessive tension is applied to the oral mucosa. If the defect is covered with a BFP flap, palatal scarring is reduced, and the palate is maximally lengthened with well-vascularized tissue.
The BFP flap can fill the dead space between the nasal and oral mucosa. Since the muscle is transposed to the posterior side, a dead space is created between the nasal and oral mucosa. By filling the dead space with the BFP flap, the palate volume increases. In addition, fibrosis in the dead space is reduced. Ultimately, BFP flaps lengthen the soft palate without creating stress from the mucosal flap and accordingly reposition the levator muscle more posteriorly, thus resulting in successful velopharyngeal closure. This led to excellent speech outcomes in our study.
Finally, the BFP flaps are quick to harvest and show almost no complications at the donor site (Qiu et al., 2019), which is herniated only by gentle pulling. The surgery time increased by only 10 to 15 min for the BFP flap harvest. Bennett et al., analyzed the cheek volume before and after BFP harvest using a three-dimensional camera and reported no difference between the donor and non-donor-side cheek volumes (Bennett et al., 2017).
Several studies have described the use of the BFP flap for primary cleft palate repair and oronasal fistula closure. Ashtiani et al., reported several cases of palatal fistula repair with BFP flaps and suggested that a BFP flap was suitable for medium-sized palatal fistulas located in the middle or posterior palate but not for anterior defects (Ashtiani et al., 2011). Qiu et al., used BFP flaps and primary Furlow palatoplasty to improve mucosal healing and minimize flap dehiscence (Qiu et al., 2019). They transposed a BFP flap between the oral and nasal mucosa and reported decreased wound problems due to additional vascular tissues. However, no other studies have reported the effect of BFP flaps in VPI patients.
This study has several limitations. First, measuring the uvula-pharynx gap is a static analysis that may not reflect the dynamic motion. Furthermore, the gap size may not correlate with the severity of VPI. However, the primary goal of VPI correction is palatal lengthening and muscle repositioning. As the palate is lengthened and muscle is physiologically repositioned, VPI symptoms should improve. In future studies, nasopharyngoscopy can be helpful in evaluating the dynamic motion. Additionally, after surgery, the velopharyngeal gap is further decreased due to tissue swelling and local anesthesia infiltration. These may contribute to the palatal lengthening amount since the palatal length may be further increased than the actual length. However, since the DOZ and BFP groups were assessed under the same condition, the comparison between the two groups was valid. Second, the changes in the BFP flap-covered area due to healing were not assessed in this study. In future studies, changes in the BFP flap-covered area could be as valuable as the amount of palatal lengthening that was measured in this study. Third, the study sample size was small. The outcome interpretation might have been limited by the small sample size, which did not provide adequate power to discern small effects. Lastly, due to the retrospective nature of the study, only results from a single pathologist were available. A bias might be possible since the results of a single observer were assessed without conducting an inter-rater evaluation. Nonetheless, the one who performed the perceptual speech analysis was a 10-year experienced professional speech pathologist. Additionally, at the time of the evaluation, the speech pathologist was blinded to the surgical methods used for VPI correction.
Conclusion
To our knowledge, this study is the first to assess the effects of a BFP in VPI patients. Our result emphasizes the significant advantages of adding a BFP flap to the standard DOZ repair. The BFP flaps maximized the palatal length, retro-positioned levator muscle, and promoted velopharyngeal closure even in moderate and moderate-to-severe VPI cases. Thus, our method improves the surgical outcomes of VPI correction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
This study was performed in accordance with the principles of the Declaration of Helsinki.
Patient Consent
The patients provided written informed consent for the publication and the use of their images.