
Abstract
Objective
To provide the prevalence and an overview of cleft lip and palate (CL/P) in the period of 2008 to 2017, as well as the profile of care provided for this condition in Brazil.
Design
Cross-sectional study of epidemiological character.
Setting
Brazilian government website.
Participants
National Live Birth and Hospital Information System.
Intervention
Organization of the end databases and performance-based statistical analysis.
Main Outcome Measure(s)
Analysis of the prevalence of CL/P in newborns, sociodemographic condition of the mothers, surgical procedures and hospitalizations, and specialized hospitals in Brazil within a 10-year period.
Results
The average prevalence of CL/P in Brazil was ∼52 children per 100 000 live births in the covered period, corresponding to 1 per 1924 newborns. The presence of cleft was associated with preterm birth, being underweight, and the male gender. The highest prevalence was found in the South region, while the lowest was found in the Northeast region, with increasing rates in the North region of Brazil. The states with the highest prevalence were not those with a great number of hospitalizations and surgical procedures for live births with CL/P.
Conclusion
In the 10-year study period, the prevalence of CL/P was 0.52 newborns per 1000 live births, a result which differs among the states of Brazil. The need to reinforce the national monitoring of the prevalence and surgical procedures of cleft patients have also emphasized the need to improve public medical care for CL/P subjects.
Introduction
The most common congenital orofacial cleft includes the cleft of the lip and/or palate (CL/P). It results from malformation in the process of facial development and growth between the 4th and 12th weeks of pregnancy (Smarius et al., 2017; Vyas et al., 2020) with genome-wide association (Mangold et al., 2010). The presence of the cleft can cause impairment of speech, hearing, esthetics, occlusal development, quality of life, and psychosocial disorders in the individual with the fissure (Aljohani et al., 2021; De Cuyper et al., 2019; Hardin-Jones and Jones, 2005; Liao and Mars, 2005; Ma et al., 2021; Vyas et al., 2020).
The etiology of CL/P is associated with genetic factors, such as mutations and polymorphism, as well as environmental factors, including nutritional deficiencies, alcoholism, lifestyle, use of drugs, and smoking during pregnancy (Angulo-Castro et al., 2017; Candotto et al., 2019; Dien et al., 2018). Specific factors, such as viral infections, endocrine changes (obesity, low weight, diabetes), and teratogens (pesticides), have also been investigated but with inconclusive results (Dixon et al., 2011; Gil-da-Silva-Lopes and Monlleo, 2014). Epidemiological studies have identified seasonality, ethnicity, parents’ age, birth weight, and social class as associated factors related to CL/P in newborns (Maranhao et al., 2021; Mossey et al., 2009; Silva et al., 2018). The prevalence of CL/P varies according to the geographic region and ethnic group (Costa et al., 2006; McLeod et al., 2004; Mossey et al., 2009; Sousa and Roncalli, 2017; Tanaka et al., 2012). The lowest occurrence occurs in African individuals, when compared to Whites, and has proven to be similar among Japanese and Chinese individuals (Butts, Reynolds, Gitman, Patel, and Joseph, 2018; Croen, Shaw, Wasserman, and Tolarova, 1998; Martelli et al., 2010). The most affected is the male gender (Freitas et al., 2004; Hagberg et al., 1998; Ravichandran et al., 2012; Shibukawa et al., 2019; Vyas et al., 2020).
In Brazil, it is estimated that there was a ratio of 0.6 for every one thousand live births in 2017, with an increased tendency of CL/P malformation, especially in less developed regions of Brazil (Sousa and Roncalli, 2017). Brazilian studies often use small samples, the vast majority of which are related to hospital statistics or few locations in the country (Costa et al., 2006; Maranhao et al., 2021; Ravichandran et al., 2012). In the early 90s, the Brazilian Live Birth Information System (SINASC in Portuguese) and the Hospital Information System (SIH in Portuguese) were created by the Unified Health System (SUS in Portuguese) were implemented throughout the territory. These database systems improved the control of the national analysis of vital events and coverage of medical and hospital care, respectively, with the development of reliable demographic indicators of health data (Shibukawa et al., 2019; Sousa and Roncalli, 2017).
The importance of providing health surveillance, primarily in patients with CL/P, is to diagnose time-course changes in prevalence that may well be able to reveal alterations in environmental risk factors. Thus, this study aims to describe the history of a 10-year period (2008-2017), the current prevalence, and the relationship between the presence of cleft and variables related to the mother (such as the state of residence, and prenatal and newborn care) and the child (such as birth weight, ethnicity, gender, and preterm birth) in 2017 in Brazil and by state. The number of hospitalizations and outpatient surgical procedures, as well as the number of specialized centers for CL/P patients, were compared to the prevalence rates in the states of Brazil in 2017.
Methods
Data Source
This is an epidemiological study that used the records from the Brazilian government website by means of the Brazilian public health system's (SUS) Computer Department (DATASUS) from the Brazilian Ministry of Health. This study did not require an ethical appraisal, since the data comes from secondary databases.
Prevalence Rate
SINASC was used to extract the prevalence of newborns with CL/P palate in the 10-year period from 2008 to 2017 of the 27 states of Brazil. The prevalence rate of CL/P was calculated by dividing the number of live births with fissures according to the mother's residence by the total number of live births in the same place and period, multiplying by 100 000 inhabitants and measuring the average change (95% confidence interval—CI) (Abreu et al., 2016).
Prevalence Rate With and Without CL/P in 2017
SINASC was also used to extract the socioeconomic conditions of the mothers, demographic characteristics, and characteristics of childbirth for 2017 alone. These variables were organized based on the proportion of live births with and without CL/P under the following conditions: preterm (birth with gestational age less than 37 weeks), mothers with schooling up to 8th grade, the marital status of the mothers (single, divorced, or widowed), mothers aged 35 or over, mothers with insufficient prenatal care (less than 7 consultations), children with low birth weight (up to 2500 g), gender (male), and the color/race according to the genetic background of the Brazilian population (Souza et al., 2019) (Europeans plus Afro-descendants) of the newborn.
The Proportion of Municipalities With Cases of CL/P in 2017
The proportion of municipalities with cases of CL/P was calculated by counting the number of municipalities in each state that had at least one case of CL/P only in 2017 divided by the total number of municipalities in that state.
Hospitalization and Surgical Procedures
The data of hospital procedures and hospitalizations were collected from SIH. Following, the number of hospitalizations to perform surgical procedures related to the CL/P, and the number of procedures accomplished by mother's place of residence from 2008 to 2017 were tabulated. Thereafter, the per capita ratios, the number of hospitalizations/number of live births with cleft, and the number of surgical procedures/number of live births with cleft were then calculated. The list of procedures performed by reference centers authorized by the Ministry of Health is listed in Supplemental Table 1.
Statistical Analysis
The databases, such as the estimated point of the percentage of prevalence and the CI were organized using the Excel 365® software (Microsoft Office 365, Redmond, WA, USA), while statistical analysis was performed using the Statistical Package for the Social Sciences software (SPSS for Windows, Version 23.0, SPSS Inc., Chicago, IL, USA). The longitudinal normal, negative binomial, and beta regression models were used to analyze the data, incorporating the explanatory variables of region and time in the models. A Z-test for 2 populations was used to compare the CL/P and no CL/P groups. P < .05 was considered statistically significant.
Results
According to data obtained from SINASC, 15 418 births of children with CL/P were recorded in Brazil between 2008 and 2017. The average prevalence of orofacial clefts in Brazil was ∼52 per 100 000 live births, which equals 1 child for approximately every 1924 live births in this period.
The prevalence in the different regions of Brazil was demonstrated during the 10-year period (Supplemental Figure 1). In the period from 2008 to 2017, the lowest prevalence in the North region was 39 per 100 000, while the highest was 58 per 100 000 live births. In the Northeast region, these values were 32 and 45 per 100 000 live births, respectively. In the Southeast Region, the prevalence varied between 45 per 100 000, which occurred in 2008, and 62 per 100 000 live births in 2016. In the South and Midwest regions, the minimum prevalence values were 61 per 100 000 and 46 per 100 000 live births, and a maximum of 79 per 100 000 and 61 per 100 000 live births, respectively. Analyzing the results of the binomial model and considering the Midwest region as a reference category/class, the North, Northeast, and Southeast regions were significant in the model when compared to the Midwest region. The North and Northeast regions witnessed a reduction of −4.87 and −10.75 units, respectively, in the average CL/P prevalence when compared to the Midwest, while the South region exhibited an increase of 19.01 units. The Moran test was performed to assess the presence of spatial correlation, but this factor was not observed (P=.123) (Supplemental Figure 1). The residual diagnostic analysis showed no violation of the model's assumptions. The best model in terms of fit was the normal model, with an explanation of data variability of ∼80% (R2-adj=0.80).
Regarding the prevalence rates in the Brazilian states, Santa Catarina, located in the South region, showed the highest prevalence, with 74.6 per 100 000 live births, followed by the Rio Grande do Sul, with 71.8 CL/P per 100 000 live births, and Paraná, with 68.4 CL/P per 100 000 live births (Table 1). The prevalence from the Southwest states in ascending order were: Minas Gerais, with 43.1 per 100 000 live births; Espírito Santo, with 37.9 per 100 000; Rio de Janeiro, with 46.3 per 100 000; and São Paulo, with 63.6 per 100 000 live births (Table 1). Regarding the prevalence of estimated cases in municipalities in 2017, the state in which the cases are most widely disseminated is Amazonas, where 38.7% of the municipalities had at least 01 cases, followed by Rio de Janeiro, with 38% (Table 1).
Number and Percentage of Municipalities With at Least one Case of Cleft Palate in 2017, and the Prevalence of Live Births with CL/P per 100 000 Live Births in the 2008 to 2017 Period by State.
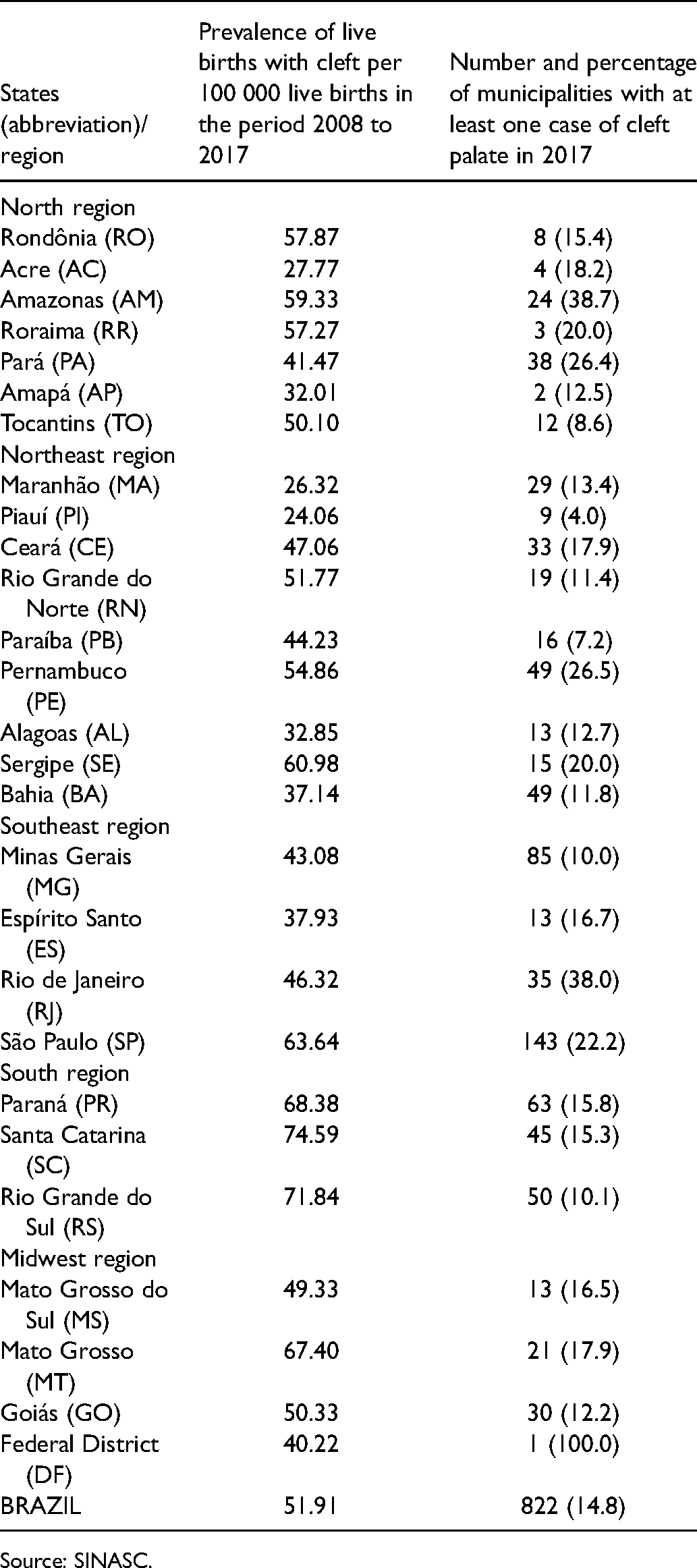
Source: SINASC.
In Brazil, at the national level, the prevalence of all analyzed variables was higher in children with cleft when compared to live births without cleft (Table 2). However, variables with a statistically significant difference in prevalence between the groups with and without cleft included low-weight, showing a prevalence of 19.3% (95% CI [16.8–21.8]) in the group with a cleft and a prevalence of 8.2% (95% CI [8.1–8.4]) in the group without a cleft, and male CL/P children, showing a prevalence of 60.7% (95% CI [57.7–63.7]) in the group with a cleft as compared to 51.3% (95% CI [51.1–51.5]) in the group without a cleft (Table 2). Moreover, an enhanced proportion of preterm births was found in Brazil, showing a prevalence of 19.9% (95% CI [17.4–22.4]) in the group with a cleft and a prevalence of 11.2% (95% CI [10.9–11.4]) in the group without a cleft (Table 2). No statistical difference was exhibited between Europeans plus Afro-descendant children born with or without CL/P (Table 2).
Prevalence of Life Birth Children With and Without CL/P According to the Birth Weight, Ethnic, Gender, and Preterm Birth in 2017 in Brazil and by State.
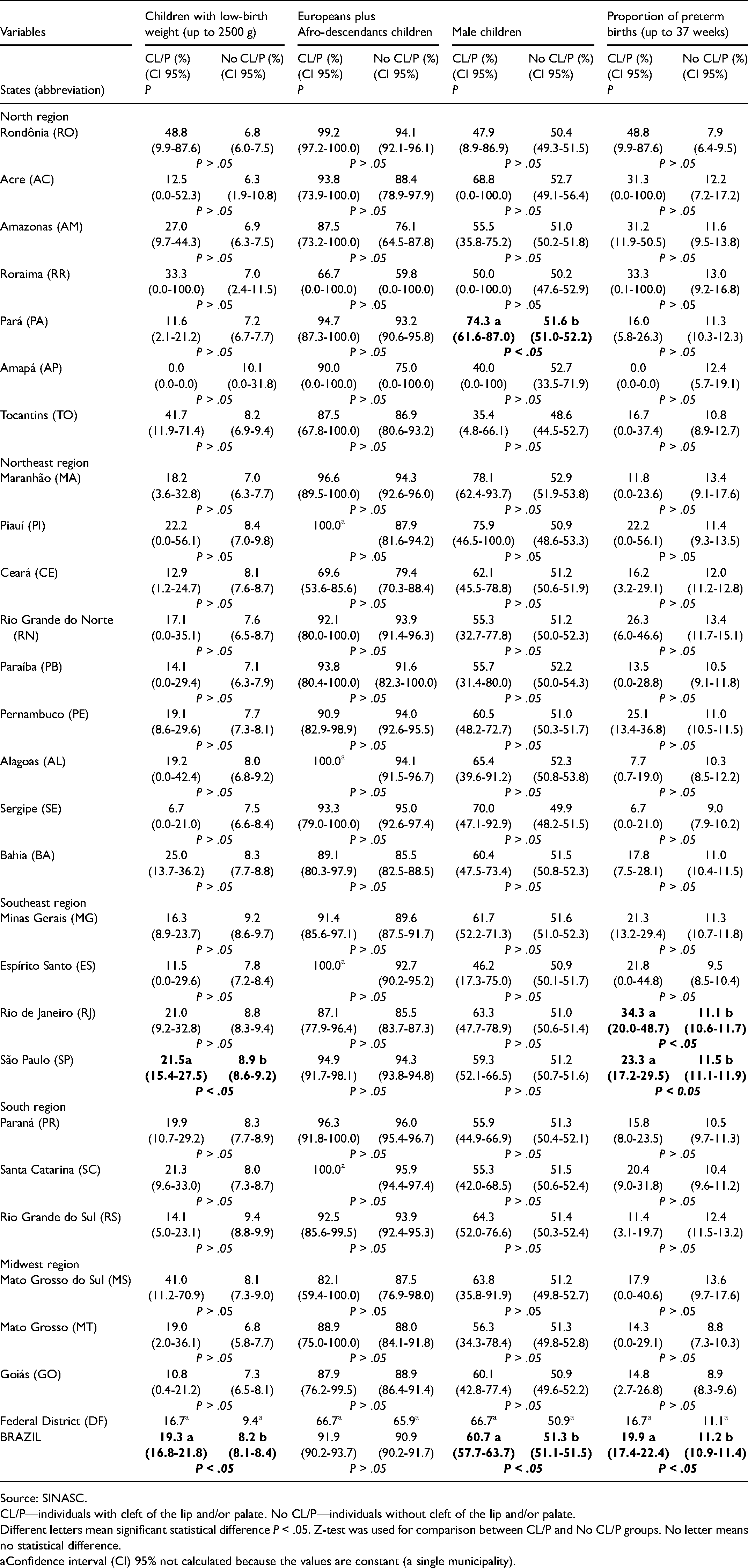
Source: SINASC.
CL/P—individuals with cleft of the lip and/or palate. No CL/P—individuals without cleft of the lip and/or palate.
Different letters mean significant statistical difference P < .05. Z-test was used for comparison between CL/P and No CL/P groups. No letter means no statistical difference.
Confidence interval (CI) 95% not calculated because the values are constant (a single municipality).
Significant results were also found in low weight among the states (Table 2). A higher prevalence of live births with cleft with low-birth weight was observed in the Southeast region, in the state of São Paulo. Considering the ethnicity factor (Europeans plus Afro-descendants) of the newborns, no difference in the prevalence was verified among the states (Table 2).
Regarding gender, the prevalence of the male sex was significantly higher in children with CL/P in the North region in the state of Pará (Table 2). The proportion of births of children with cleft with a gestational age of less than 37 weeks, in descending order, were Rio de Janeiro (Southeast) with 34.4%, and São Paulo (Southeast region) with 23.3%. The negative binomial regression model was used to analyze the children's data and check the relationship between prematurity and birth weight in patients with CL/P. Only the Southeast region was significant when compared to the Midwest region (base category) for premature patients with CL/P. A statistically significant relationship was found between preterm births and low-birth weight in patients with CL/P (P < .01) (Table 2).
The socioeconomic factors of the mothers, such as mothers with up to 8 years of schooling, without a spouse present, mothers aged 35 years and over, and the insufficient amount of prenatal care had no statistical significance within the Brazilian states (Table 3).
Prevalence of Sociodemographic Conditions of the Mother in 2017 in Brazil and by State.
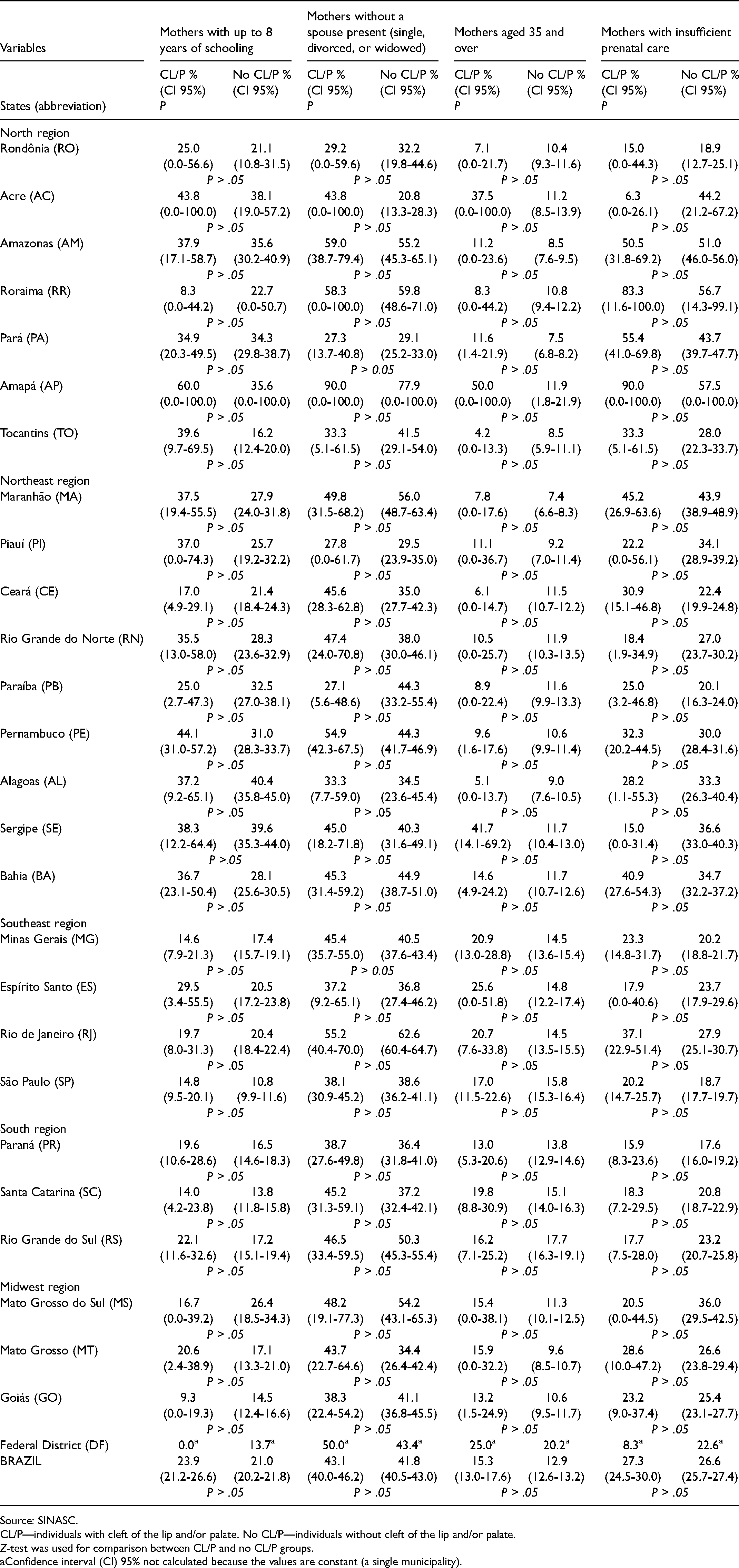
Source: SINASC.
CL/P—individuals with cleft of the lip and/or palate. No CL/P—individuals without cleft of the lip and/or palate.
Z-test was used for comparison between CL/P and no CL/P groups.
Confidence interval (CI) 95% not calculated because the values are constant (a single municipality).
The states with the highest prevalence are not those with the highest number of hospitalizations and surgical procedures (Figure 1), nor did hospitals specialize in children with CL/P treatment (Supplemental Table 2 and Figure 1). The state of Santa Catarina, which had the highest prevalence of live births with a cleft, showed 2.07 hospitalizations and 6.34 surgical procedures per live birth with a cleft during the same period, an average lower than that of other states with lower prevalence values (Table 4). The state of Minas Gerais presented an average of hospitalizations and surgical procedures of 3.33 and 6.91 per live birth with CL/P, respectively. In Espírito Santo, these values are 2.66 and 7.31; in Rio de Janeiro, 1.47 and 3.60; in São Paulo, 2.47 and 5.22; in Paraná, 3.85 and 9.93; and in the Rio Grande do Sul, 1.78 and 4.08 per live birth with CL/P. By contrast, the state of Piauí, located in the Northeast region, showed a low prevalence of 24.06 children with a cleft per live birth, but with a high average of hospitalizations (6.98) and procedures (8.38) per live birth with a CL/P (Table 4).
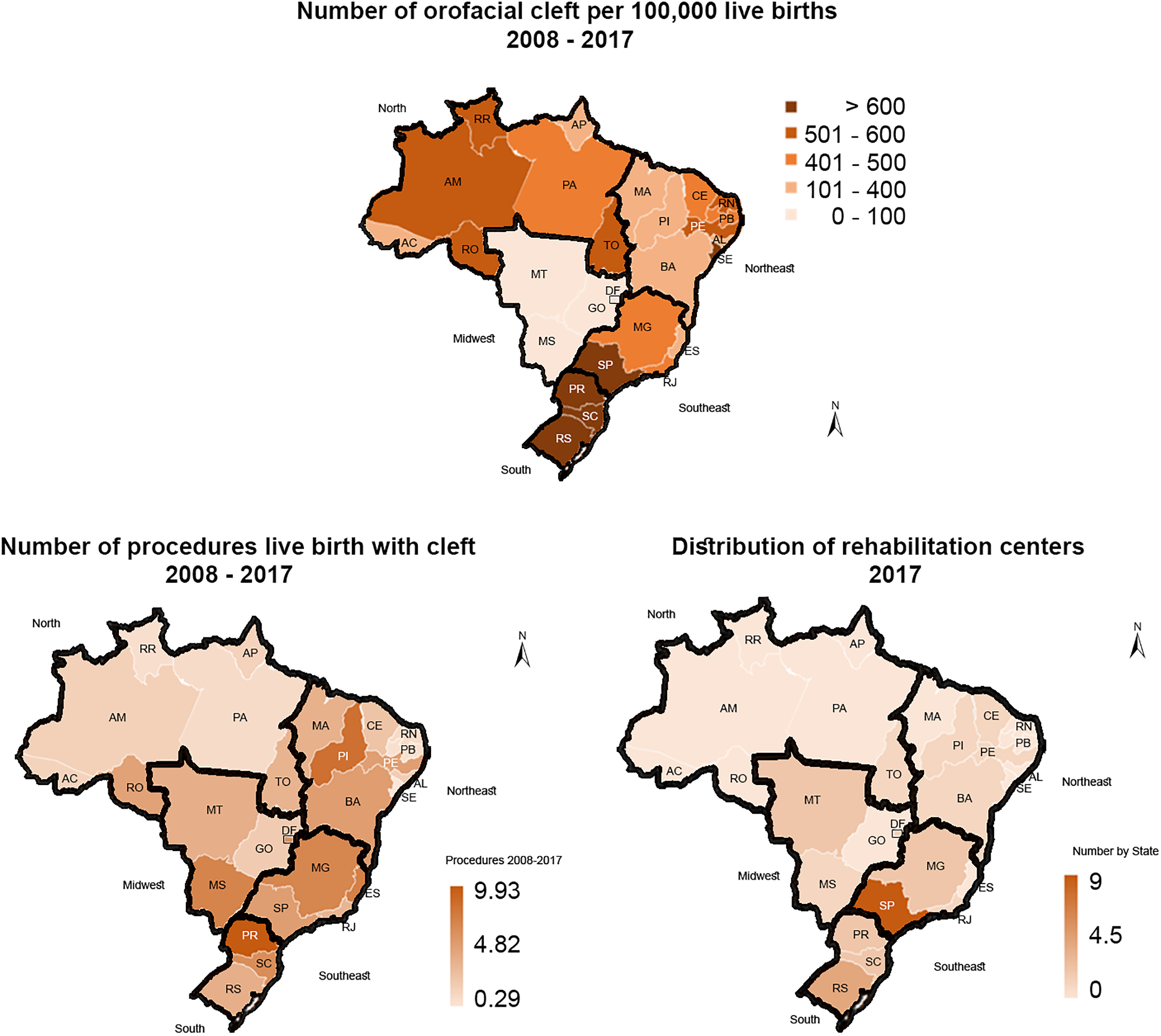
Inequality between prevalence, distribution of rehabilitation centers, and number of procedures per live birth of children with CL/P in the states of Brazil, 2008 to 2017, SINASC and SIH.
Number of Hospitalizations per Live Birth With CL/P, and the Number of Surgical Procedures per Live Birth With Cleft in the Period of 2008 to 2017 by State.
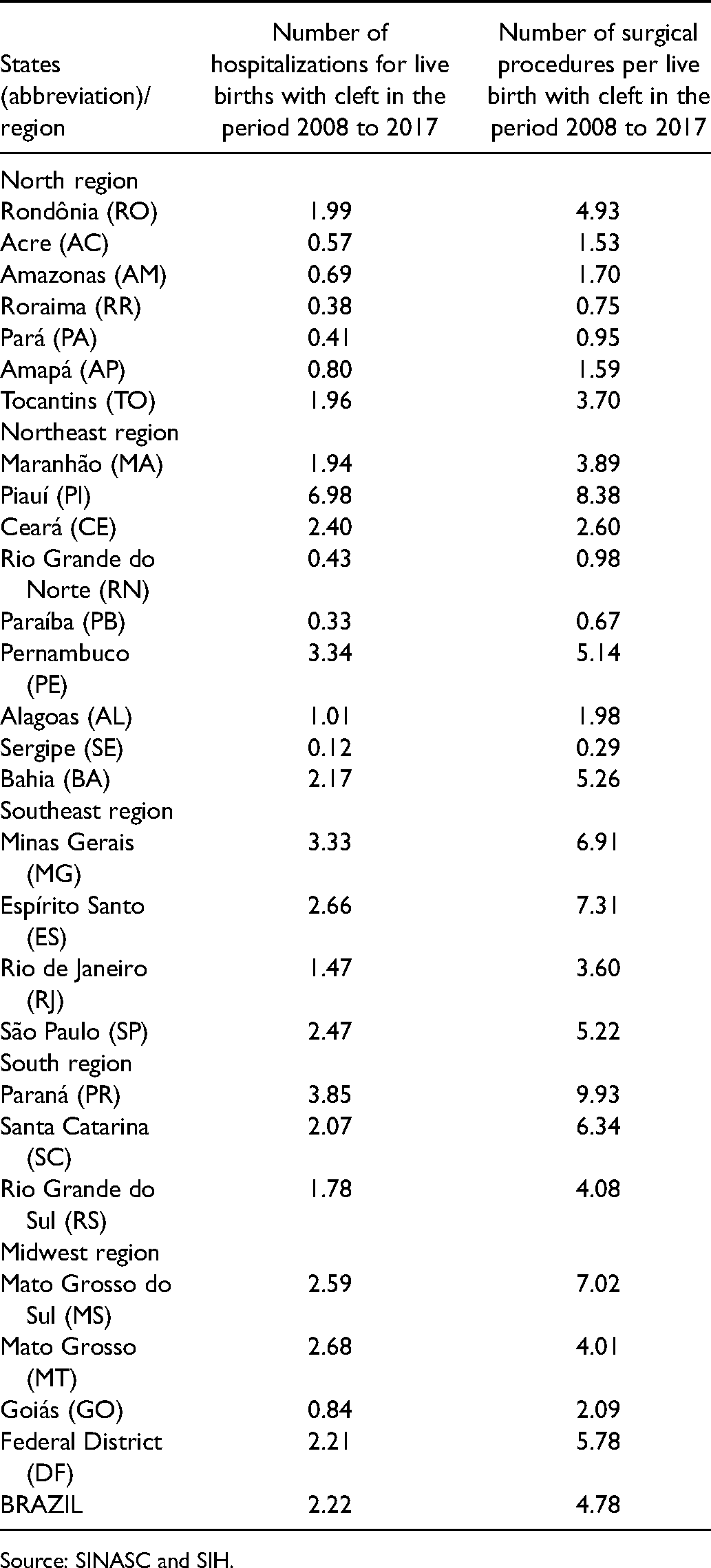
Source: SINASC and SIH.
Discussion
The prevalence of birth and surveillance system of children with CL/P is unknown in some parts of the world (Mossey et al., 2009). In Brazil, SINASC and SIH enable data collection on births and hospitalizations reported throughout the national territory, providing data for all levels of the public health system (Sousa and Roncalli, 2017). In this study, the Brazilian information of the birth of CL/P children was gathered, and the results showed that the average prevalence of CL/P in Brazil was ∼52 newborns with CL/P per 100 000 births in the 10 years from 2008 to 2017. The presence of cleft was associated with preterm birth, being underweight, and the male gender. The highest prevalence was found in the South region of Brazil, while the lowest was found in the Northeast region. The states with the highest prevalence were not those with a great number of hospitalizations and surgical procedures for live births with a cleft.
In recent years, some Brazilian authors have devoted themselves to studying the prevalence of CL/P. However, some of these studies have not covered all regions of the country or used the health information systems in a transition period, and are thus considered to be of a reduced reliability from a national point of view (Costa et al., 2006; Maranhao et al., 2021; Silva et al., 2018). Prevalence investigation in the field of CL/P is essential to quantify the problem in a specific country. Countries with higher income can gather with great accuracy the necessary data for the national health control of patients with CL/P. However, this not be feasible in developing nations worldwide, and epidemiology should seek to diagnose the gaps in these information gaps in order to improve this scenario (Mossey and Modell, 2012). The SINASC and SIH information systems in Brazil make the data from the Brazilian country available for all citizens and researchers, enabling comparability among the different Brazilian states (Abreu et al., 2016; Sousa and Roncalli, 2017).
This study showed that the Brazilian prevalence of CL/P was 52 children per 100 000 live births from 2008 to 2017. Similar results were demonstrated by Sousa and Roncalli (2017) with a national average of 58 per 100 000 live births from 2009 to 2013, and Shibukawa et al. (2019) with 51 CL/P per 100 000 births from 2005 to 2016. These results are below the global average, with the prevalence of 1 in 700 live births worldwide [Mossey and Castillia, 2003].
Concerning Brazilian regions, the South Region had the highest rate of CL/P and the Northeast region the lowest. In corroboration with our study, the South and Southeast regions registered higher rates than the national rate (Shibukawa et al., 2019). The overall prevalence between 2008 and 2017 was higher in the North, Northeast, and Southeast regions and lower in the South and Midwest regions of Brazil. A tendency towards the enhancement of the prevalence of CL/P in the Northeast, North, and Midwest regions of Brazil was evidenced by Abreu et al. (2016), which may be associated with changes in risk factors and improvements adopted in Brazilian information systems in the last few years (Sousa and Roncalli, 2017).
The presence of cleft was associated with prematurity, low-birth weight, and gender (Hagberg et al., 1998). In corroboration with other Brazilian and international studies (Angulo-Castro et al., 2017; Freitas et al., 2004; Hagberg et al., 1998; Mossey et al., 2009; Ravichandran et al., 2012; Shibukawa et al., 2019; Vyas et al., 2020) the male gender prevailed in Brazil from 2008 to 2017. The highest prematurity among children born with a cleft was also present in another Brazilian study (Shibukawa et al., 2019). This factor may be related to an increase in the option for Cesarean delivery in Brazil (Behague et al., 2002), which may contribute to higher rates of prematurity (Wood et al., 2017). In the Cesarean, unlike vaginal delivery, there is no obligation to wait for maturity and the natural phenomena linked to childbirth (Shibukawa et al., 2019; Wood et al., 2017). An enhanced risk of low-birth weight is found in newborns with CL/P, although the chance of having a premature birth is not (Wyszynski et al., 2003). There is a clear need to expand the discussion among professionals working in prenatal care with the mothers and their families concerning the growing preference for Cesarean sections and to explain the risks and benefits of this type of delivery in comparison to vaginal delivery (Domingues et al., 2014).
The states of São Paulo and Rio de Janeiro showed increased rates of newborns with CL/P prematurity, which corroborates with a study that points to an increased national tendency from the 1990s onwards of premature births in the Southeast and Northeast regions (Silveira et al., 2008). However, SINASC information from the 90s was pointed out as a limitation in the period covered by the study, despite the progressive improvement in data quality acquisition in Brazil (Silveira et al., 2008).
Low-birth weight also showed great prevalence in the group of children born with a cleft (Angulo-Castro et al., 2017; Hagberg et al., 1998; Shibukawa et al., 2019; Wyszynski et al., 2003). This factor can also be explained by the increase in the performance of Cesarean deliveries in Brazil (Behague et al., 2002; Domingues et al., 2014). Associated with higher rates of prematurity, there may not be enough time for the baby to gain weight before birth (Wood et al., 2017; Wyszynski et al., 2003).
The higher prevalence in Europeans plus Afro-descendant children with CL/P was pointed out, including in association with a genetic component (Croen et al., 1998; do Rego Borges et al., 2015; Martelli et al., 2010). Brazilian individuals have a highly variable genetic admixture, which may affect the signals to susceptibility for CL/P (Dixon et al., 2011; Mangold et al., 2010). This extensive ethnic heterogeneity in Brazil, with a wide variation in the proportions of ethnicities of the individuals, might explain why our study did not find this relationship at the national level.
Prenatal care is essential for the development of a healthy pregnancy (Behague et al., 2002), though the diagnosis of CL/P during prenatal care is associated with a worsening of family conflicts (De Cuyper et al., 2019). The ultrasound screening at 20 weeks of pregnancy provides a more accurate diagnosis to encounter the CL/P malformation (Smarius et al., 2017). In this study, no local specificities were found among the states concerning maternal and care factors regarding the age of the mother and the insufficient number of prenatal consultations in children with CL/P. Maternal age equal to or greater than 35 years has been associated with the development of congenital anomalies due to the aging of eggs and the presence of chronic diseases (Costa et al., 2006; Dien et al., 2018; Shibukawa et al., 2019).
Low schooling of the mothers and absence of a spouse were pointed out as possible risk factors associated with CL/P (Shibukawa et al., 2019). In corroboration with Shibukawa et al. (2019), this study demonstrated that parental education had no impact on the prevalence of CL/P. However, education might be an important factor mainly about anticipated genetic consequences of consanguinity as an essential prevention manner of CL/P malformations (Maranhao et al., 2021; Ravichandran et al., 2012).
Brazil is a continental-sized middle-income country, with large socioeconomic discrepancies and great disparities in the allocation of income, which are the outcome of a historical heritage that demarcates the territorial use and the political and economic structure of the country (Diaz, 2002; Rocha et al., 2021). These social inequalities may affect people's health status, both directly and indirectly, by limiting their access to and use of health services (Albuquerque et al., 2017; Diaz, 2002; Landmann-Szwarcwald and Macinko, 2016; Rocha et al., 2021; Szwarcwald, Souza Junior, Marques, Almeida, and Montilla, 2016). Although in the 2000s the Brazilian government provided advances in reducing poverty and inequalities (Albuquerque et al., 2017; Szwarcwald et al., 2016), many limitations still remain regarding SUS throughout Brazil, including the health care for patients with CL/P (Sousa and Roncalli, 2017).
Sousa and Roncalli (2017) verified a positive correlation between the prevalence of CL/P and the number of medical procedures in the period of 2009 to 2013, and that increased prevalence areas are receiving greater funding for CL/P treatment (Sousa and Roncalli, 2017). These results are in contrast with the findings of this study in which states with low prevalence, such as Piauí [Northeast region], showed increased hospitalization averages. In the aforementioned period, SINASC was presenting improvements in the reports on the prevalence of CL/P, with no reference to SIH enhancement (Abreu et al., 2016), which could justify the discrepancy of the results. The lack of synchronism among the healthcare needs of an individual with CL/P, the large territorial distances to the centers, and the high cost of travel, can also make many families give up on the treatment or monitoring provided.
Comprehensive care for people with CL/P is very challenging, especially in such a vast country like Brazil. This study revealed a concentration of rehabilitation centers in the Southeast, occurring particularly in the state of São Paulo. The number of accredited centers has increased recently, which favors the expansion of medical care. Therefore, a Brazilian population-based surveillance program associated with hospital statistics is necessary, which may well contribute to the equity management of services in the area of craniofacial anomalies (Gil-da-Silva-Lopes and Monlleo, 2014). The lack or insufficient care provided for the complete rehabilitation of a patient with CL/P can generate losses, including morbidity, emotional disorders, exclusion, and stigmatization for the individual, his family, and society (De Cuyper et al., 2019; WHO, 2004). Multidisciplinary care and early surgical interventions are essential for the healthy development of people with CL/P (Webb et al., 2001; WHO, 2004).
Studies regarding CL/P are highly concerned with finding methods through which to improve the evidence base for information for the population and the therapeutic interventions to enhance the quality of care with primary prevention of CL/P malformation (Mossey and Modell, 2012). Finally, we reinforce the importance of health surveillance and evaluation, in the context of CL/P, to identify and correct possible failures in the health system. The prevalence of CL/P has been increasing in Brazil and SUS should offer comprehensive medical care to these individuals and their families through qualified healthcare centers.
Conclusion
In the past 10 years, the prevalence of CL/P was 0.52 newborns per 1000 live births, representing 1 per 1924 newborns, which differs among the states of Brazil. The discrepancy between prevalence and surgical procedures performed revealed the regional health inequalities in Brazil for individuals with CL/P, suggesting a poor distribution of resources and opportunities. The need to reinforce the national monitoring of the prevalence and surgical procedures of cleft patients has also emphasized the need to improve public medical care for patients with CL/P. The results of this study may contribute to aid the Brazilian health system in planning the long-term sustainability of public finances for individuals with CL/P.
Supplemental Material
sj-tif-1-cpc-10.1177_10556656211050004 - Supplemental material for The Panorama of Cleft Lip and Palate Live Birth in Brazil: Follow-up of a 10-Year Period and Inequalities in the Health System
Supplemental material, sj-tif-1-cpc-10.1177_10556656211050004 for The Panorama of Cleft Lip and Palate Live Birth in Brazil: Follow-up of a 10-Year Period and Inequalities in the Health System by Raquel S. Silva, Soraia Macari and Thiago R. dos Santos, Marcos A.F. Werneck, Rafaela da Silveira Pinto in The Cleft Palate-Craniofacial Journal
Supplemental Material
sj-xlsx-3-cpc-10.1177_10556656211050004 - Supplemental material for The Panorama of Cleft Lip and Palate Live Birth in Brazil: Follow-up of a 10-Year Period and Inequalities in the Health System
Supplemental material, sj-xlsx-3-cpc-10.1177_10556656211050004 for The Panorama of Cleft Lip and Palate Live Birth in Brazil: Follow-up of a 10-Year Period and Inequalities in the Health System by Raquel S. Silva, Soraia Macari and Thiago R. dos Santos, Marcos A.F. Werneck, Rafaela da Silveira Pinto in The Cleft Palate-Craniofacial Journal
Supplemental Material
sj-pdf-4-cpc-10.1177_10556656211050004 - Supplemental material for The Panorama of Cleft Lip and Palate Live Birth in Brazil: Follow-up of a 10-Year Period and Inequalities in the Health System
Supplemental material, sj-pdf-4-cpc-10.1177_10556656211050004 for The Panorama of Cleft Lip and Palate Live Birth in Brazil: Follow-up of a 10-Year Period and Inequalities in the Health System by Raquel S. Silva, Soraia Macari and Thiago R. dos Santos, Marcos A.F. Werneck, Rafaela da Silveira Pinto in The Cleft Palate-Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.