
Abstract
Objectives
Non-syndromic cleft lip with or without cleft palate (NSCL ± P) is one of the most common birth malformations. Currently, numerous susceptibility SNPs have been reported by GWA studies, however, the replications of them among NSCL ± P from Han Chinese were very limited.
Design
In this study, we selected 16 SNPs around 1q32.2 based on the published GWA studies and replicated them among 302 trios with NSCL ± P from Han Chinese Population. The genotypic data was analyzed with FBAT, PLINK and R package.
Setting
The study was conducted in a tertiary medical center.
Patients, participants
302 patients with CL ± P and their parents.
Main outcome measures
To ascertain the genetic variants in 1q32.2 in patients with CL ± P in Han Chinese Population.
Interventions
Blood samples were collected.
Results
We found T allele (Z = 4.26, p = 0.00002) and T/T homozygotes (Z = 4.4, p = 0.000011) at rs12063989 was significantly over-transmitted among non-syndromic cleft lip with or without cleft palate (NSCL ± P).
Conclusions
We found rs12063989 exhibited significant association with the occurrence of NSCL ± P, which would provide new evidence for the future study in the etiology of NSCL ± P.
Introduction
Non-syndromic cleft lip with or without cleft palate (NSCL ± P) is a congenital craniofacial deformity with high morbidity and mortality (Dixon et al., 2011), and it ranks fourth in China in terms of birth defects (Yu et al., 2015). Currently, according to the statistics data of 15,094,978 perinatal infants in China, the incidence of NSCL/P is around 1.67‰, non-syndromic cleft lip only (NSCLO) is 0.56‰ and that of non-syndromic cleft lip and cleft palate (NSCLP) is 0.82‰. There are significant differences in the regional incidence rate; for example, Southwest China has a relatively high occurrence rate (Fan et al., 2018).
Patients with NSCL ± P have an increased incidence of mental health problems and higher overall mortality rates during all stages of their life. Like other complex disorders, NSCL ± P occurs due to the complex interplay of multiple genes and environmental modifiers (Mossey et al., 2009). But there is compelling evidence that genes play a major role in the etiology of NSCL ± P (Grosen et al., 2011; Beaty et al., 2016; Ladd-Acosta and Beaty, 2018). However, it is very difficult to define any single etiologic mechanism because many genes or loci can influence the risk of NSCL ± P, and significant progress has been made in identifying the underlying genes and pathways in large population-based samples available for studies (Rahimov et al., 2012).
Genome-wide association (GWA) studies have successfully identified more than 14 000 loci at which common variants influence the disease risk or quantitative traits (Welter et al., 2014). From 2009 onwards, 13 independent GWA studies for NSCL ± P have been published, and more than 50 different genes/loci achieving genome-wide significance have been identified, which influence the risk of NSCL ± P (Birnbaum et al., 2009; Grant et al., 2009; Beaty et al., 2010; Mangold et al., 2010; Camargo et al., 2012; Ludwig et al., 2012; Fonseca et al., 2015; Sun et al., 2015; Wolf et al., 2015; Leslie et al., 2016, 2017; Yu et al., 2017; Huang et al., 2019). However, the loci identified by these GWA studies can explain only a small fraction of the heritable component of NSCL ± P, and it did not pinpoint the susceptible SNP at the associated loci. Moreover, it is unclear how the associated loci influence NSCL ± P and whether these findings are associated with NSCL ± P in other populations. Thus, the initial sets of GWA studies could serve as a starting point for future genetic and functional studies (McCarthy and Hirschhorn, 2008).
In this study, we selected the following 16 SNPs located on chromosome 1 based on the published GWA studies (Fonseca et al., 2015) and GWAS meta-analysis (Ludwig et al., 2012): rs4920522 (1p36.13; PAX7), rs766325 (1p36.13; PAX7), rs6695765 (1p36.13; PAX7), rs742071 (1p36.13; PAX7), rs560426 (1p22.1; ABCA4), rs6677101 (1p13.3; SLC25A24), rs2235371 (1q32.2; IRF6), rs642961 (1q32.2; IRF6), rs126280 (1q32.2; DIEXF), rs2064163 (1q32.2; DIEXF), rs12063989 (1q32.2; DIEXF), rs4844913 (1q32.2; DIEXF), rs9429830 (1q32.2; SYT14), rs11119388 (1q32.2; SYT14), rs227178 (1q32.2; SYT14), and rs2485893 (1q32.2; SYT14), to pinpoint the susceptible SNP among 302 case-parent trios with NSCL ± P from the Western Han Chinese population.
Materials and Methods
Study Population
The study recruited 302 case-parent trios with NSCL ± P, including 129 trios with NSCLO and 173 trios with NSCLP (the samples have not been used in the previous GWA studies). Sample size was calculated using Monte-Carlo simulation with PBAT, underlying an additive genetic model at 1% test level, MAF 0.20, genotypic risk 1.3, and population prevalence of the disease was set as 0.00182. Data of all subjects were collected from the Cleft Lip and Palate Surgery Department of the West China Hospital of Stomatology, Sichuan University. All patients recruited in this study were assessed as having NSCL ± P (without any other congenital malformation of the body or a family history of genetic disease) by a physician.
Human subject study protocols were reviewed and approved by the institutional review board (IRB) of West China Hospital of Stomatology, Sichuan University in 2016 (WCHSIRB-D-2016-012R1), and was conformed to the STOBE (strengthening the reporting of observational studies in epidemiology) guidelines. Informed consent was obtained from each participant prior to enrollment in this study.
DNA Extraction and Genotyping
EDTA-anticoagulated venous blood samples were collected from all individuals, and DNA was isolated according to a standard salting out procedure. For genotyping, genomic DNAs were diluted to a working concentration of 100 ng/ul. All SNPs were genotyped using the SNPscan method developed by the Genesky Biopharm technology Company (http://www.geneskies.com/) using the SNPscan technology.
Statistical Analysis
Each SNP was assessed by the Hardy Weinberg equilibrium (HWE) and the minor allele frequency (MAF) among the unaffected parents. HWE and MAF were calculated using PLINK software (Purcell et al., 2007). Allelic TDT, genotypic TDT and global TDT were performed by the FBAT program (Allison, 1997). Pairwise LD, which showed both D′ and r2, was computed for all the SNPs using the Haploview program (http://www.broad.mit.edu/haploview/haploview). We used the Bonferroni correction for 48 tests to determine the threshold for formal significance of p = 0.001.
Results
Allelic TDT
All 16 SNPs passed quality control (HWE P-value>0.01) and the MAF ranged from 0.05–0.49 in NSCL ± P, 0.05–0.49 in NSCLP, and 0.05–0.50 in NSCLO (Supplementary Table 1). Therefore, we included all SNPs in the following analysis, and allelic TDT results showed that allele T at rs12063989 (24kb 3′ of DIEXF) were over-transmitted among NSCLP (Z = 3.29, P = 0.001) and NSCL ± P(Z = 4.26, P = 0.00002), allele C at rs2235371 in IRF6 (Z = 4.07, P = 0.000047), allele A at rs11119388 (SYT14) (Z = 3.45, P = 0.00055) and allele G at rs2064163 (23kb 3′ of DIEXF) (Z = 4.01, P = 0.00006) were over-transmitted among NSCL ± P. It was interesting to note that significant signals for rs2235371 and rs11119388 were driven by NSCLO; but for rs2064163 and rs12063989, the significant p-value among NSCL ± P was driven by NSCLP based on their P values (Table 1).
Allelic TDT Results of the SNPs for NSCL ± P.
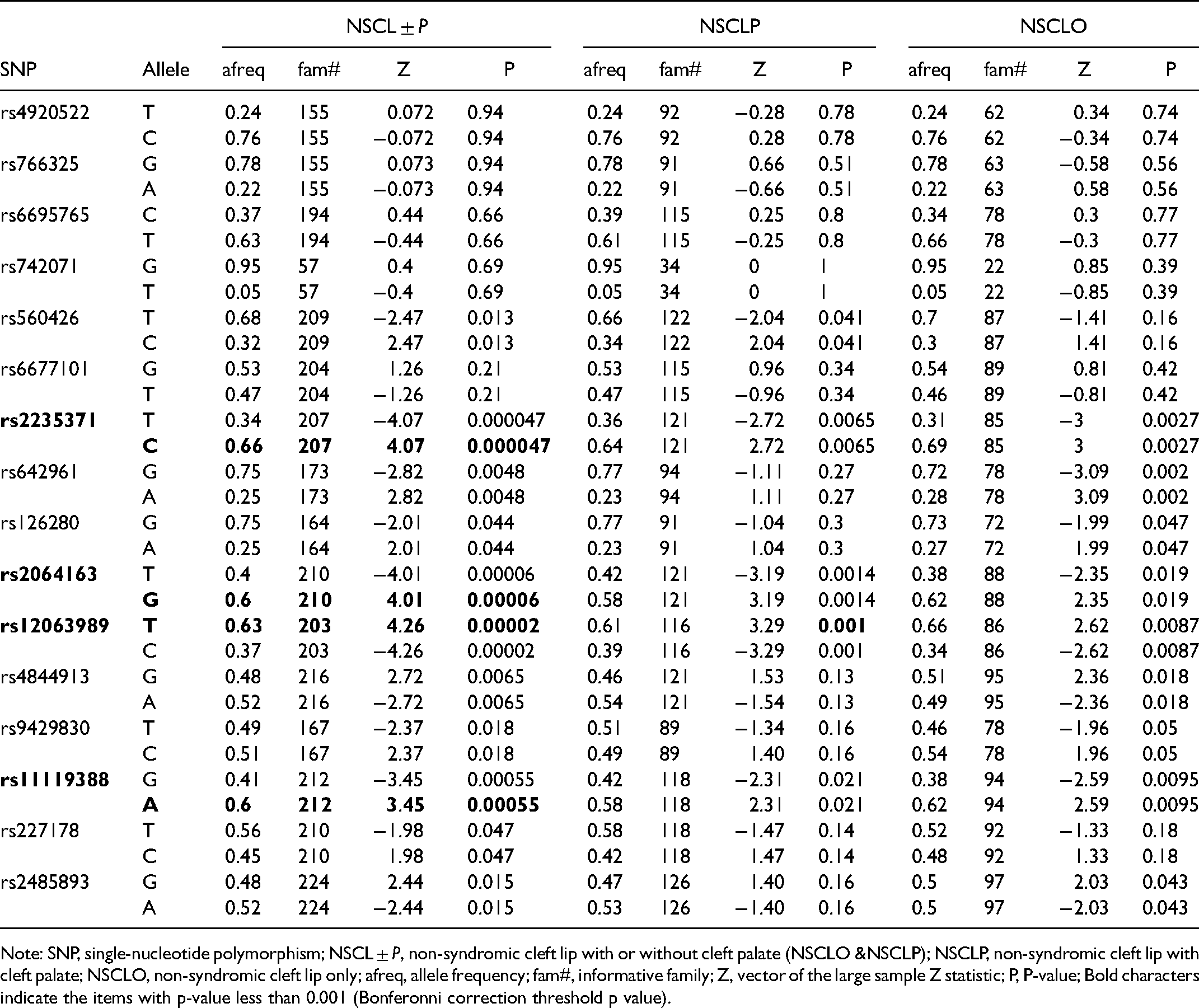
Note: SNP, single-nucleotide polymorphism; NSCL ± P, non-syndromic cleft lip with or without cleft palate (NSCLO &NSCLP); NSCLP, non-syndromic cleft lip with cleft palate; NSCLO, non-syndromic cleft lip only; afreq, allele frequency; fam#, informative family; Z, vector of the large sample Z statistic; P, P-value; Bold characters indicate the items with p-value less than 0.001 (Bonferonni correction threshold p value).
Genotypic and Global TDT
Genotypic TDT, which split the SNP into three genotypes, showed that the T/T homozygote at rs12063989 was over-transmitted in the NSCL ± P group (Z = 4.4, P = 0.000011) and the NSCLP group (Z = 3.65, P = 0.00026), respectively; the C/C homozygote at rs2235371 (Z = 3.95, P = 0.000079), the G/G homozygote at rs2064163 (Z = 3.87, P = 0.00011), and the A/A homozygote at rs11119388 (Z = 3.55, P = 0.00038) were over-transmitted among NSCL ± P (Table 2). Global TDT analysis confirmed that rs12063989, rs2235371 and rs2064163 were associated with NSCL ± P (lowest P = 0.000038) (Table 3).
Genotypic TDT for NSCL ± P Under Genotypic Models.
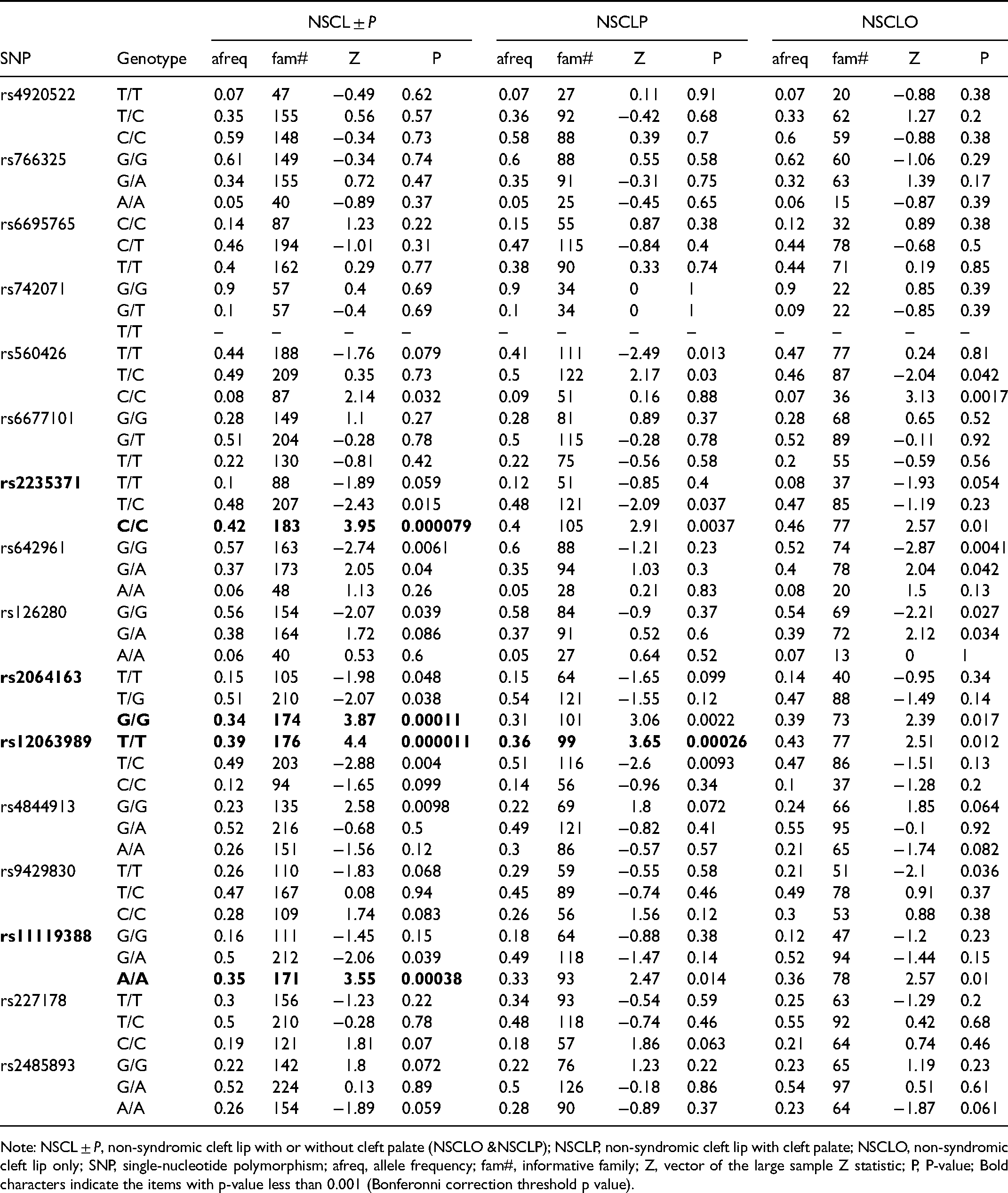
Note: NSCL ± P, non-syndromic cleft lip with or without cleft palate (NSCLO &NSCLP); NSCLP, non-syndromic cleft lip with cleft palate; NSCLO, non-syndromic cleft lip only; SNP, single-nucleotide polymorphism; afreq, allele frequency; fam#, informative family; Z, vector of the large sample Z statistic; P, P-value; Bold characters indicate the items with p-value less than 0.001 (Bonferonni correction threshold p value).
Global TDT of the SNPs in Trios with NSCL ± P.
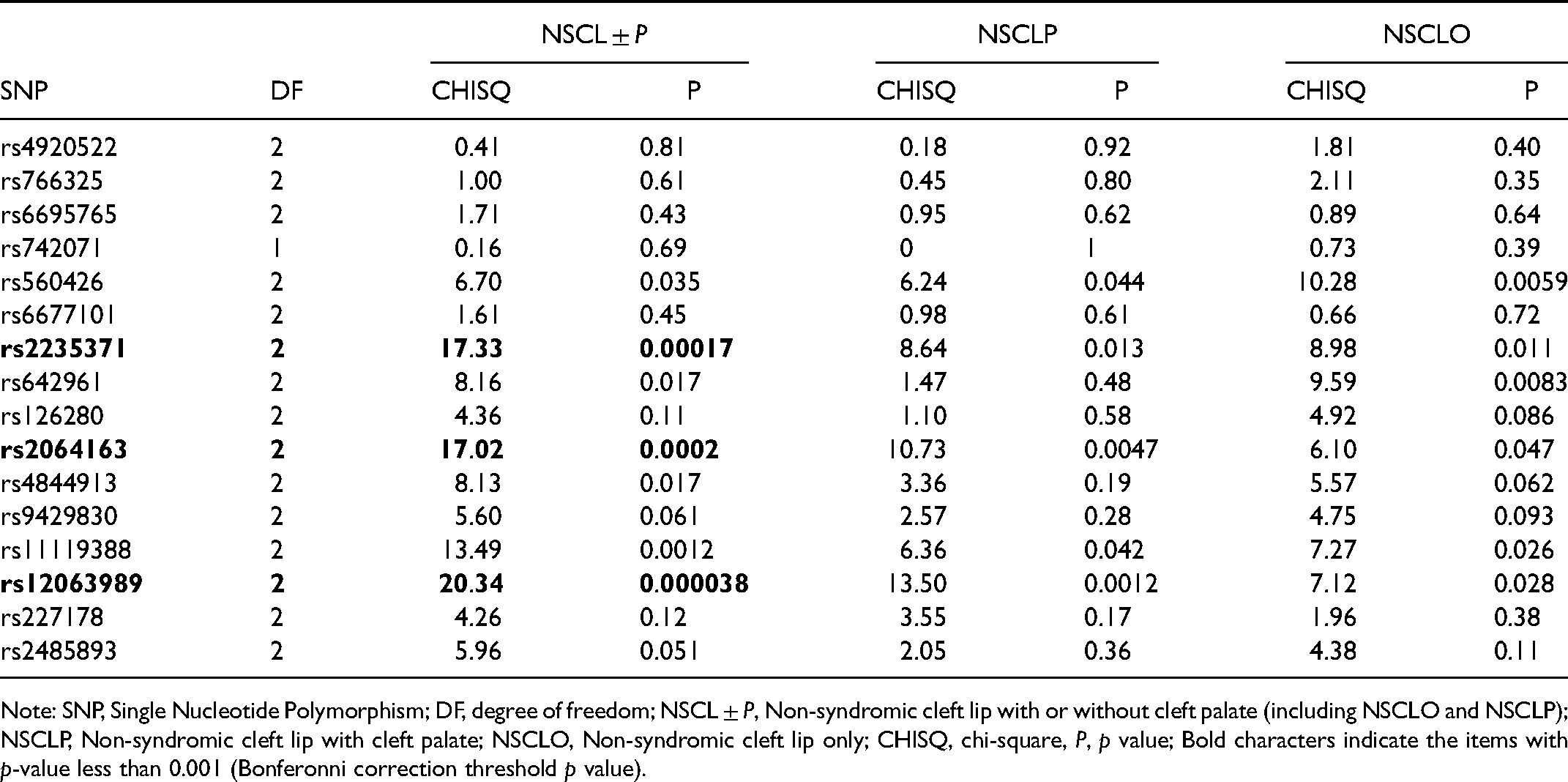
Note: SNP, Single Nucleotide Polymorphism; DF, degree of freedom; NSCL ± P, Non-syndromic cleft lip with or without cleft palate (including NSCLO and NSCLP); NSCLP, Non-syndromic cleft lip with cleft palate; NSCLO, Non-syndromic cleft lip only; CHISQ, chi-square, P, p value; Bold characters indicate the items with p-value less than 0.001 (Bonferonni correction threshold p value).
Pair-Wise LD
To assess if the associated SNPs (rs12063989, rs2235371, rs11119388 and rs2064163) on chromosome 1 in the same LD block and the adjacent SNPs travelled together from the parents to the affected kids, we performed the pair-wise LD analysis by the Haploview program. The results showed that rs12063989 and rs2064163 were tightly linked to each other among the trios of NSCL ± P (r2 = 0.86, D′ = 1.0), NSCLP (r2 = 0.89, D′ = 1.0), and NSCLO (r2 = 0.83, D′ = 1.0) (Figure 1); there was no strong linkage between the two most significant SNPs rs12063989 and rs2235371.
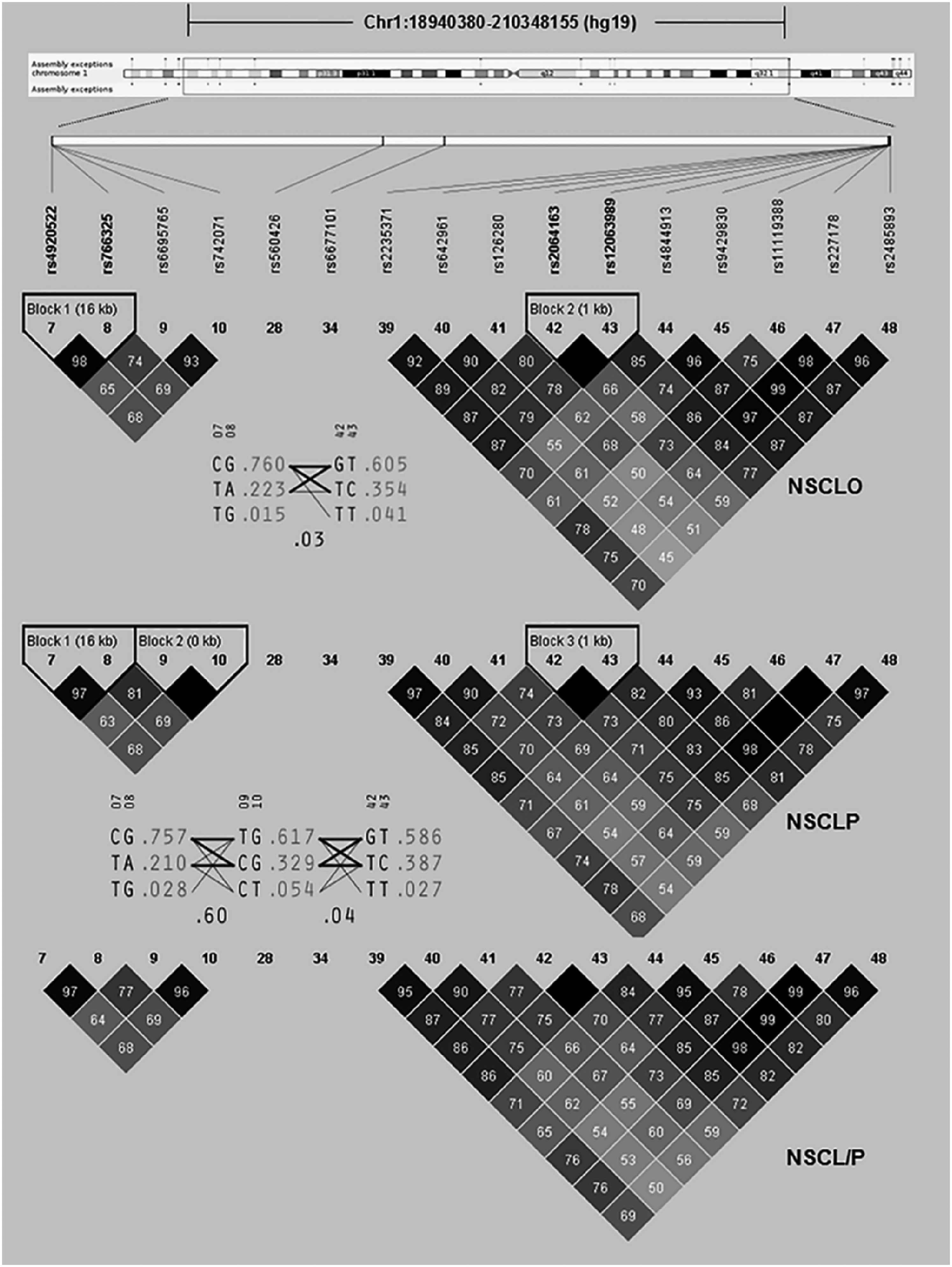
Pairwise LD block of the SNPs at chromosome 1 in trios with NSCL ± P. Note: NSCL ± P, Non-syndromic cleft lip with or without cleft palate (including NSCLO and NSCLP); NSCLP, Non-syndromic cleft lip with cleft palate; NSCLO, Non-syndromic cleft lip only.
Discussion
The identification of risk factors for NSCL ± P cross populations and regions is very important to promote understanding of the etiology of it. Although many susceptible genes have been discovered through GWA studies, they do not appear to be uniformly pathogenic in cases of different race. For example, 8q24 loci seems to be an extremely sensitive susceptible region for European populations (Welter et al., 2014; Fonseca et al., 2015); while IRF6 gene is more likely to increase the risk of NSCL ± P in Asian population (Beaty et al., 2010; Sun et al., 2015; Yu et al., 2017).
The composition of Chinese population is relatively complex involved 56 ethnic groups and population distribution is more extensive. Western China has high incidence of NSCL ± P (Fan et al., 2018), but there are limited genetic studies were focused on this population to identify the susceptible loci. It would be very effective method to locate the associate loci in Western Han Chinese population by replicating the GWAS signals reported in other populations.
In this study, all SNPs passed quality control, and they were included in the subsequent analysis. Four SNPs rs12063989, rs2235371, rs2064163 and rs11119388 achieved statistical significance after Bonferroni's correction (p = 0.001). The power analysis of NSCL ± P and its sub-phenotypes indicated the sample sizes are enough to prove the accuracy of the results.
IRF6 is the most important susceptible gene for NSCL ± P, which was firstly identified as the causal gene for syndromic and susceptible gene for non-syndromic CL/P with a contribution rate of up to 12%., for IRF6, rs642961 and rs2235371 are the most widely replicated across populations. Rs642961 was found to be a susceptible variant in the European populations. Haplotype G–A of rs2235371-rs642961 could increase the NSCL ± P risk among European, Hispanic, Norwegian, Danish, and Filipino ancestries (Rahimov et al., 2008; Blanton et al., 2010; de Souza et al., 2016), but it was not significantly associated with NSCL ± P in this study. Rs2235371is substituted for valine at amino acid position 274 (V274I) in the protein-binding domain of IRF6 gene. Currently, many replication studies on rs2235371 have confirmed its association with NSCL ± P (Jafary et al., 2015; Xu et al., 2016; Wu-Chou et al., 2018; Wu et al., 2019), and inconsistent results were noted in some populations; for example, Brazilian population(Paranaiba et al., 2010). Although a large number of population studies have confirmed the contibution of rs2235371 to NSCL ± P, but functional test on zebrafish indicates that p.V274I could retain protein function and potentially be non-pathogenic(Li et al., 2017). In this study, rs12063989 has lower p-values than rs2235371 and they were in the same LD block. So, we determined the relationship by conducting pairwise LD analysis. LD analysis did not show they were independent with each other.
T allele of rs12063989 were over-transmitted in the NSCL ± P (Z = 4.26, P = 0.00002) and NSCLP (Z = 3.65, P = 0.00026) (Table 1), which indicated that they could increase the risk for the carriers to have a cleft baby from Western Han Chinese population. Regulatory chromatin states from the DNAse and histone ChIP-Seq data showed that rs12063989 located in the regulatory region, and motif analyses indicated that different alleles of rs12063989 could greatly alter the affinity of ELF1_known1 (score:2.7 to 12.7) and GR_known3 (−4.3 to7.6). All of ELF1 (Guan et al., 2017) and GR (Kim et al., 2010) played a significant role in the regulation of apoptosis.
In summary, by replicating the SNPs identified by GWASs, we found that rs12063989 is significantly associated with the occurrence of NSCL ± P, allele T at rs12063989 has an increased risk for NSCL ± P, which would provide new evidence for the future study in the etiology of NSCL ± P.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656211052837 - Supplemental material for Association Between SNPs in 1q32.2 and NSCL ± P in Han Chinese Population
Supplemental material, sj-docx-1-cpc-10.1177_10556656211052837 for Association Between SNPs in 1q32.2 and NSCL ± P in Han Chinese Population by Bin Yin, Jia-Yu Shi, Bing Shi, Qian Zheng and Zhong-Lin Jia in The Cleft Palate-Craniofacial Journal
Footnotes
Acknowledgments
The authors thank all the participants who donated their samples in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Science Funds of China (No. 82170919 and No. 81600849), Sichuan Province Science and Technology support program (2020YJ0211) and National Key R&D Program of China (No. 2016YFC0905200).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.