
Abstract
Objective:
To analyse the morphological presentation of orofacial clefts, gender, syndromes and systemic anomalies associated with them.
Design:
This was an epidemiological study performed in the patients who were registered for cleft lip and palate surgeries in our centre. The data was evaluated both retrospectively as well as prospectively.
Patients/ Participants:
The patients registered from November 2006 to April 2021 were studied. Out of 5276 patients, data of 5004 cases were analysed, rest 272 patients were excluded due to lack of information. Statistical analysis and Chi square test were applied.
Results:
Cleft deformities were more common in males than females. Cleft lip with palate was the commonest phenotype (52.2%). It was followed by isolated cleft lip (22.9%), isolated cleft palate (22.1%), rare clefts (1.62%) and syndromic clefts (1.18%). Unilateral variants were more frequent than bilateral. In unilateral, left side was more common than the right side. Among bilateral, most of the cases had premaxillary protrusion. In the present study, 3.46% of all the patients had associated anomalies affecting their other organs. Less common cleft phenotypes like microform cleft lip and submucous cleft palate ± bifid uvula showed frequency of 0.62% and 0.64% respectively.
Conclusion:
Thorough examination of cleft deformity should be done as it may appear as an isolated deformity or part of a syndrome and have associated systemic anomalies. This may help us to deliver comprehensive care to the patients and can prevent potential operative complications.
Introduction
Orofacial cleft (OFC) or cleft lip and palate (CLP) is the commonest birth deformity of face. A cleft lip is a split in the upper lip, which can be just a small slit or a large opening that goes through the lip into the nose. This can be seen on one side (unilateral), both sides (bilateral), or in the middle of the upper lip (median). A cleft palate occurs when the tissue that makes the roof of the mouth does not join together completely during intrauterine life. Cleft palate may be restricted to the soft palate only or it may extend anteriorly up to the hard palate and lip (Redett, 2009; Watkins et al., 2014). Cleft lip can be diagnosed during the anomaly scan between 18–21 weeks of pregnancy, whereas it is very difficult to detect the cleft palate on an ultrasound scan. If a CLP does not get identified in the scan, it is usually diagnosed during the physical examination of the newborn, but certain types of cleft palate e.g. submucous cleft palate and bifid uvula might not be diagnosed until later in life. This deformity is seen in all the races, both sexes and all the socioeconomic groups and their distribution varies by ethnic group and geographic location. Africans have the lowest incidence rate (1:2500) whereas North American Indians and Orientals have the highest incidence rate (1:500). Its worldwide incidence has been reported as 1 in 600 (Schutte and Murray, 1999; Aljohar et al., 2008; Dvivedi and Dvivedi, 2012). According to Reddy et al., the incidence of clefts in India is 1:800–1:1000 and three infants are born with some type of OFC every hour, 78 every day and 28 600 per year (Reddy et al., 2010). Its aetiology has been attributed to various environmental, genetic and unknown factors (Wanjeri and Wachira, 2009). The important environmental factors include consanguinity, deficiency of vitamins, smoking, consumption of alcohol or certain drugs by mother, presence of infections and exposure to radiation during pregnancy (Chung et al., 2000).
OFC most commonly occur as an isolated birth defect but can also be associated with other anomalies. Approximately 70% of CLP cases are non-syndromic and occur as an isolated condition but 30% of oral clefts are syndromic and are associated with some anomalies such as 22q11 deletion syndrome and Pierre Robin sequence (Wang, 2004). Many epidemiological studies related to OFC have been reported in the literature from the different geographical locations across the globe but emphasis has not been given on such studies from central part of India. Therefore, the present study was conducted in our tertiary care hospital situated in central region of the country, with having an aim to study the morphological presentation of cleft deformities, gender, syndromes and anomalies associated with them.
Materials and Methods
This is a combination of prospective and retrospective study done on the patients registered for cleft lip and/or palate surgery in our centre from November 2006 to April 2021 (14 years 6 months). This study was started prospectively in March 2014 and the patient's data from November 2006 to February 2014 was studied retrospectively. A total number of 5276 patients with cleft lip and/or palate reported to our centre in last 14 years and 6 months. These patients were evaluated for the morphological details of cleft, gender, syndromes and associated anomalies. The patients were examined by the team of surgeons and paediatricians. The principles outlined in the Declaration of Helsinki were strictly followed during data collection. The desired information for 272 patients could not be obtained therefore they were excluded from the study. The collected data of 5004 patients was entered in Microsoft Excel and subjected to statistical analysis using Statistical Package for Social Sciences (SPSS, IBM version 20.0). The level of significance was fixed at 5% and p ≤ 0.05 was considered statistically significant. Kolmogorov-Smirnov test and Shapiro-Wilks test were employed to test the normality of data. Chi square test was performed for quantitative variables. This study was approved by the Institutional Review Board (Integrity Ethics Committee) of the hospital. Written informed consent was obtained from parents of all the patients.
Results
Among all the participants, majority of them had cleft lip and palate (CLP). Their total number was 2612 followed by isolated cleft lip (CL) and isolated cleft palate (CP) which were 1146 and 1106 in numbers, respectively. The rare cleft was seen in 81 patients whereas 59 cases had syndromic cleft. In the present study, male predominance was seen with having male to female sex ratio of 1.15:1. A statistically significant association between the gender and type of cleft was noted (p value 0.001). The CLP and CL were more common in males, whereas CP, rare clefts and syndromic clefts were more common in females (Figure 1). The male to female sex ratio for CLP, CL, CP, rare clefts and syndromic clefts were 1.39:1, 1.32:1, 0.67:1, 0.84:1 and 0.74:1 respectively.
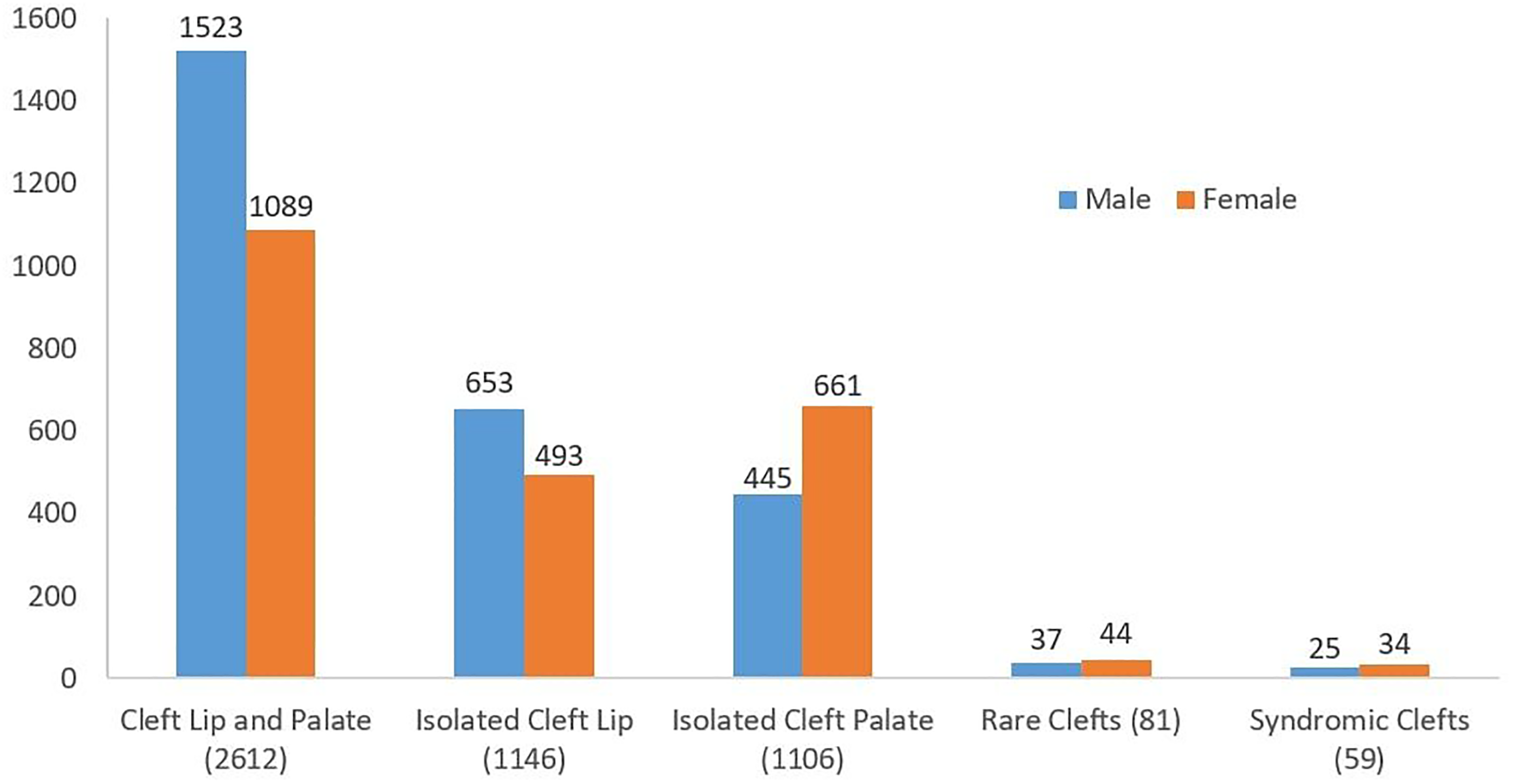
Gender wise distribution of different cleft phenotypes.
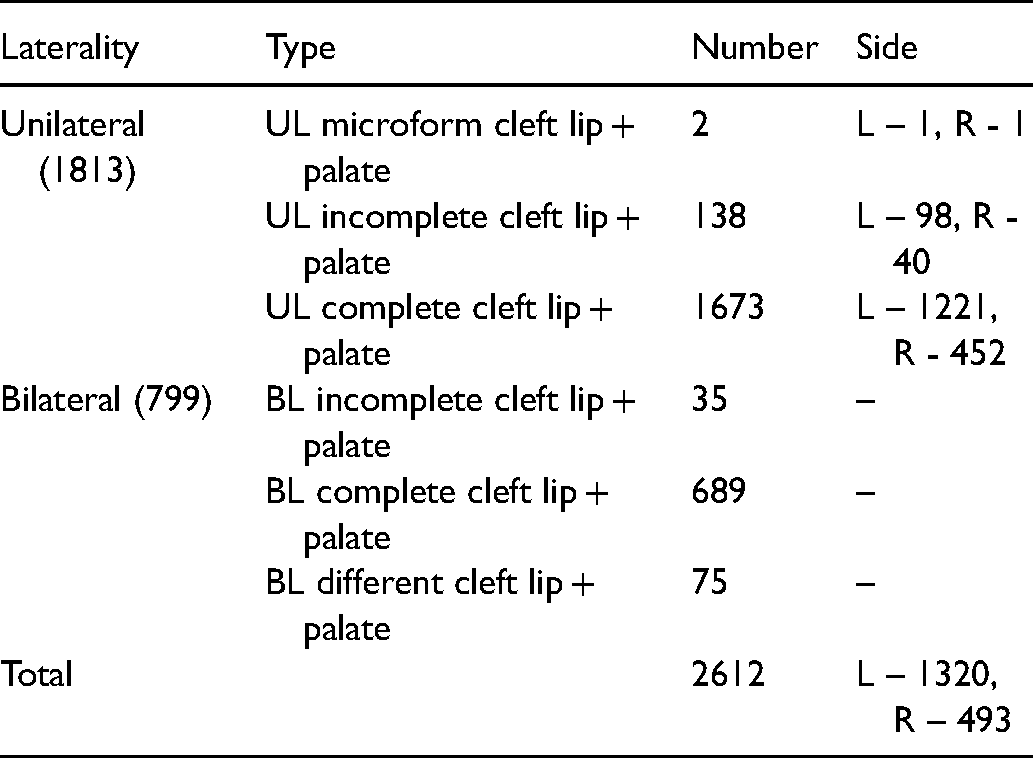
Among total number of CLP cases, 1813 were unilateral and 799 were bilateral. In unilateral CLP, 1673 patients had complete, 138 had incomplete whereas just 2 patients reported with microform cleft lip along with cleft palate. The cleft palate seen in these cases were complete (1758), cleft soft palate (47), submucous ± bifid uvula (8). The cleft was more common on left side as compared to the right side (p value 0.001). In bilateral CLP also, the majority of cases had complete cleft lip (689) followed by the patients who had combination of different types of cleft lip contralaterally (75). A total number of 35 patients reported with bilateral incomplete cleft lip. All these 799 cases had complete cleft palate (Table 1).
Cleft Lip and Palate (CLP).
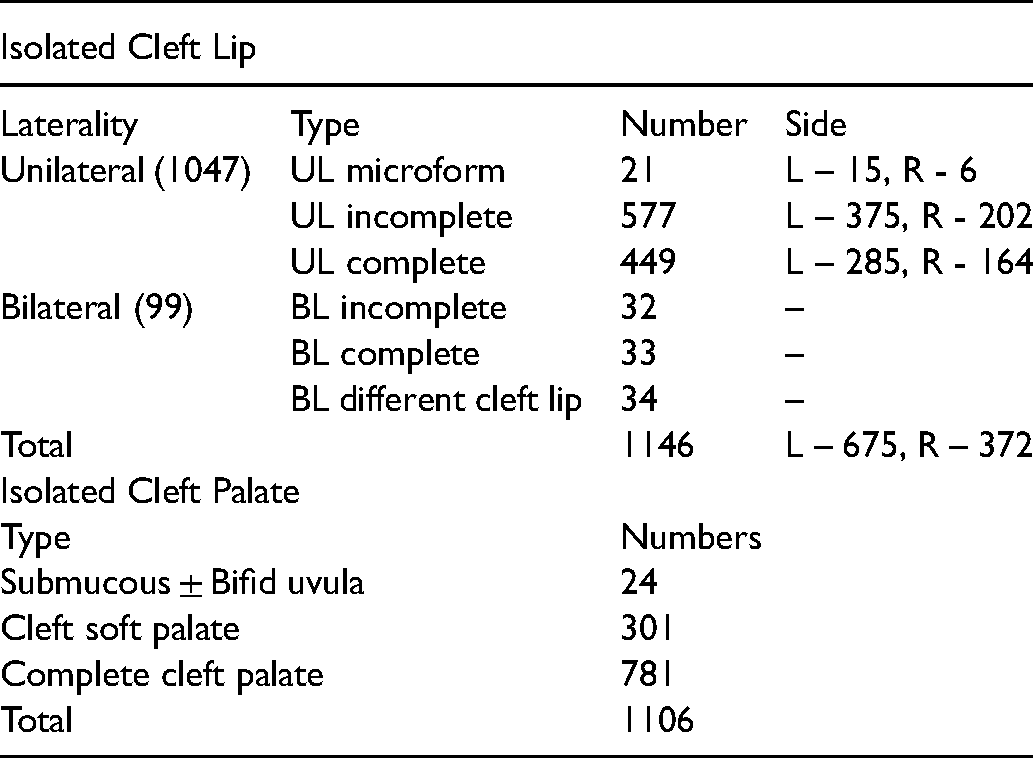
Similar to CLP, among the cases of CL, unilateral was significantly more in numbers in comparison to bilateral. In unilateral CL, the commonest type was incomplete (577) followed by complete (449) and microform (21). The left side was predominantly affected as compared to the right side (p value 0.001). As far as bilateral CL concerned, most of the patients had combination of different types of cleft lip contra-laterally (34) followed by complete (33) and 32 cases of incomplete (Table 2). The total number of patients who had CP were 1106, among which the complete cleft palate was most prevalent (781) followed by cleft soft palate (301) and 24 cases of submucous cleft palate + /-bifid uvula (Table 2). Rare clefts and syndromic clefts were seen in 81 and 59 patients respectively (Table 3). In the study group, a total number of 173 patients had associated anomalies which affected their other organs (Table 4).
Isolated Cleft Lip (CL) and Isolated Cleft Palate (CP).
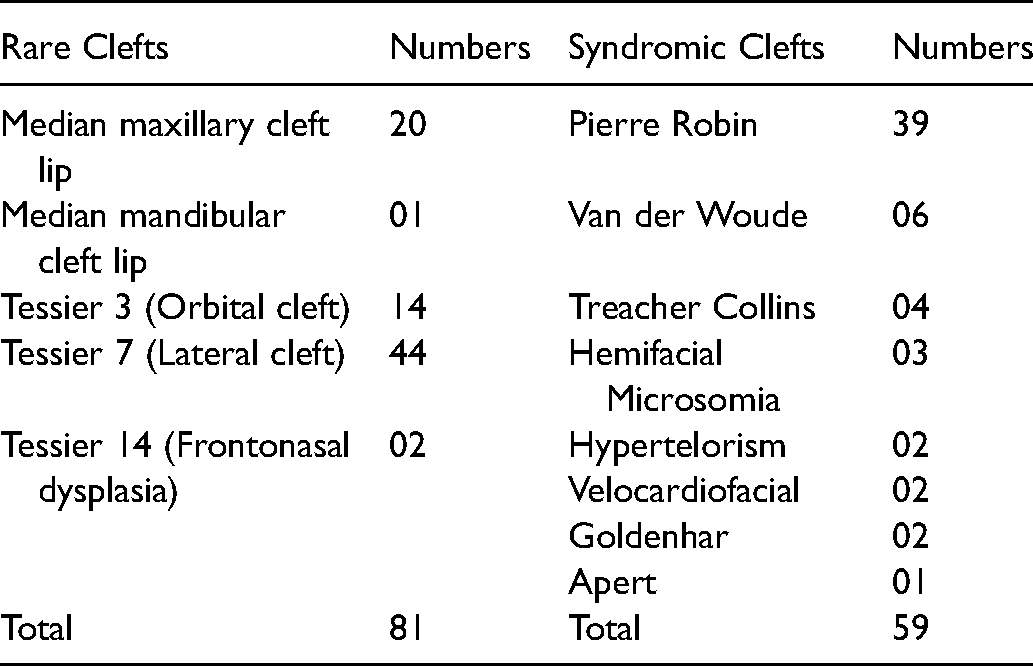
Rare and Syndromic Clefts.
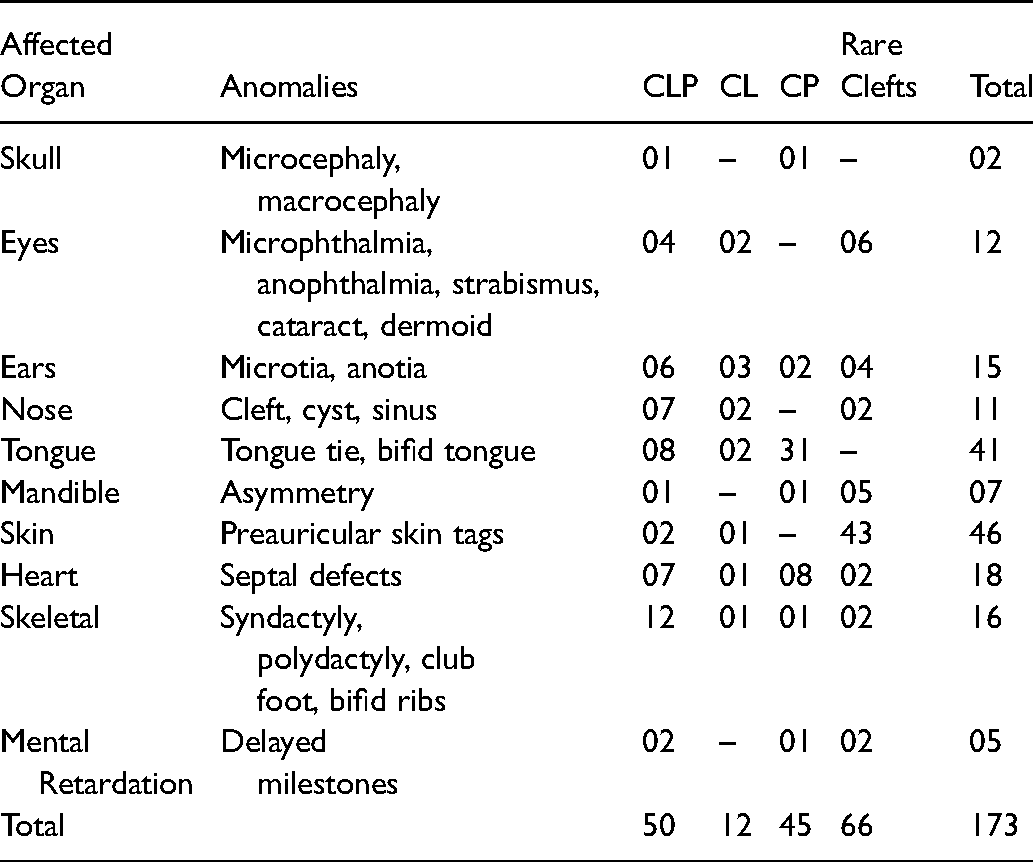
Associated Anomalies.
Discussion
OFC may have different types of morphological presentations and they may be associated with various syndromes and/or anomalies. Their prevalence may differ among different populations and gender. In our study, 53.61% of patients were males with having male to female sex ratio of 1.15:1, which is slightly lesser than the findings of Kim et al. (2002) in Republic of Korea [1.41:1] and Sah and Powar (2014) in South India [1.26:1]. Similar male predominance was reported in studies done in Denmark [Jensen et al., 1988], Kenya [Onyango and Noah, 2005], Saudi Arabia [Khalid and Al-Balkhi, 2008], Brazil [Menezes et al., 2010] and Japan [Nagase et al., 2010]. On the contrary, study conducted in Nepal showed female predominance over male [Singh et al., 2012]. The frequency of cleft phenotypes observed in our study was CLP [52.2%]>CL[22.9%]>CP[22.1%]. Similar frequency was noted in studies conducted in Jordan [Al-Omari and Al-Omari, 2004], Brazil [Menezes et al., 2010] and Iran [Yazdee et al., 2011] whereas in Japan, Nagase et al. (2010) observed CLP > CP > CL. In Nigeria [Iregbulem, 1982] and Kenya [Spritz et al., 2007], the frequency was found as CL > CLP > CP. Belliss and Gemuth (1999) noted CP > CLP > CL in Scotland whereas Kim et al. (2002) noted CP > CL > CLP in Republic of Korea. These findings suggest that there is a demographic variation in the frequency of different cleft phenotype, which can be attributed to the difference in race and ethnicity. In our study, CLP and CL were more common in males, whereas CP, rare clefts and syndromic clefts were more common in females. Comparable findings were seen by Kim et al. (2002), Murthy et al. (2014) and Uppal et al. (2016) in their studies. On the contrary, Sah and Powar (2014) reported male predominance in CP in their study of 2453 patients.
As far as cases of CLP concerned, we observed many combinations of different severity of cleft lip and cleft palate. We agree with Allori et al. (2017) who stated that the lip, alveolus and palate may each be affected in varying degrees, or not at all, and the total number of possible combinations is in the tens of thousands. Therefore, it was little difficult and complicated for us to report each and every phenotype of CLP, what we have observed in our study. Among CLP cases, both unilateral and bilateral, complete cleft lip and palate [CLP] was the most prevalent cleft phenotype. Unilateral complete CLP was seen in 33.4%, whereas bilateral complete CLP constituted 13.8% of all the cleft patients [Supplementary Table]. Thorough examination of the lip, alveolus and palate should be done by the surgeon during first surgery, when the child is under general anaesthesia to make definitive diagnosis of the deformity. Incomplete or incorrect diagnosis will affect the final outcome of the treatment.
Among cases of unilateral CL, the most prevalent type was incomplete followed by complete, with having frequency rate of 11.5% and 8.97% respectively (Supplementary Table). Among bilateral, most of the patients had combination of different types of cleft lip contralaterally. Microform cleft lip was the least common phenotype amongst cases of CL in our case series. It was seen in 31 patients only (21 unilateral CL, 4 bilateral CL, 2 unilateral CLP and 4 bilateral CLP) with having frequency rate of 0.62% in case series. Some microform cleft lip are so small that they may go undiagnosed (Li et al., 2014). Such cases usually report in older age for the correction; therefore, careful examination should be done by the primary evaluator of the deformity because surgery performed in childhood or older age usually leave more obvious scar than the procedure performed in infancy. In our case series, we received 8 cases of bilateral cleft lip where microform cleft was present on one side along with other variant of cleft lip on contralateral side (Supplementary Figure 1). This kind of cases should be repaired as bilateral cleft lip during first surgery itself to achieve satisfactory results. Unilateral CL was more common in males whereas bilateral CL was more frequent in females. All unilateral clefts were found more on the left side. Similar results were seen by Murthy et al. (2014), Ibrahim et al. (2015) and Uppal et al. (2016). In 69.9% of cases of bilateral complete CLP and CL, premaxilla was protruded. Premaxillary protrusion can make lip repair challenging and therefore may need additional procedures like pre-surgical naso-alveolar moulding or osteotomy of the premaxilla to achieve tensionless closure [Chauhan and Sharma, 2019].
Complete cleft palate was the commonest type amongst cases of CP, followed by cleft soft palate. Their frequency in our study was found as 15.6% and 6.01% respectively (Supplementary Table). Submucous cleft palate ± bifid uvula was seen in few cases (Supplementary Figure 2). It was present in 24 patients as an isolated deformity and in other 8 cases along with cleft lip, with having frequency rate of 0.64% among all cleft cases. The bifid uvula carries possibility of getting unnoticed by the neonatologist/paediatrician during first general check-up of newborn, therefore they should be well aware of this deformity. Submucous cleft palate mostly get diagnosed when a patient with a normal palate (on gross examination) but with abnormal speech reports to the speech pathologists or otolaryngologist. Such type of patients may require nasal endoscopy for definitive diagnosis.
Rare clefts were seen in 1.62% of the patients. Most of them had Tessier 7 (Supplementary Figure 3) with a frequency rate of 0.88%, which falls within the worldwide reported incidence; 0.3–1% of the cleft spectrum (Bütow and Botha, 2010). It was followed by median maxillary cleft lip (0.4%), Tessier 3 (0.28%) and Tessier 14 (0.04%). Median mandibular cleft lip (Tessier 30) was seen in one patient only (0.02%). In literature also very few cases of Tessier 30 have been reported so far with different severity (Chauhan and Sharma, 2019). In the present study, only 1.18% of all the OFCs were noted as a part of any syndrome. Previous studies by Murthy et al. (2014) also revealed less frequency of syndromes [1.35%]. In our study, most commonly seen syndrome was Pierre Robin Sequence [PRS]. It was observed in 66.1% of all syndromic cleft cases and 0.78% of all OFC cases. PRS, characterised by the presence of micrognathia, cleft palate and glossoptosis [Supplementary Figure 4], may lead to difficulties in intubation during cleft palate repair, therefore, requires meticulous pre-anaesthetic preparations, expertise anaesthesia and post-operative care. Other syndromes which have been observed in the study were Van der Woude [0.12%], Treacher Collins [0.08%], Hemifacial Microsomia [0.06%], Hypertelorism [0.04%], Velocardiofacial [0.04%], Goldenhar [0.04%] and Apert [0.02%].
A total number of 173 patients (3.46%) were found to have associated anomalies affecting their other organs (Supplementary Figures 5 and 6). The worldwide reported prevalence ranges from 1% to 63.4%. The lowest incidence (1%) was reported by Josef et al. (1997) on Swedish population whereas the highest frequency [63.4%] of associated anomalies was seen by Shprintzen et al. (1985) at SUNY Upstate Medical University, New York. This wide variation in reports can be attributed to the clinical knowledge and experience of the evaluator as well as diagnostic methods and tools used for the same. It is possible that prevalence of associated anomalies in our study is under reported for two reasons; firstly, a part of the study is retrospective and secondly, we did not have any dysmorphologist or genetist in our team to examine the child. In the present study, most commonly affected region was craniofacial [77.5%] followed by cardiovascular [10.4%], skeletal [9.2%] and nervous system [2.9%], as shown in Figure 2. Similarly, Altunhan et al. (2012) observed dominance of craniofacial region. On the contrary, Stark (1968) and Lilius (1992) found extremities, whereas Josef et al. (1997) and Ibrahim et al. (2015) noted cardiovascular system, as the most commonly involved system in their respective studies. In our study, these associated malformations were more frequent in rare clefts [38.15%] followed by CLP [28.9%] > CP [26.01%] > CL [6.94%]. Josef et al. (1997) reported higher incidence of anomalies among patients with CLP whereas Natsume et al. (2001) and Adesina et al. (2017) observed most of the anomalies in patients with CP. It is advisable to examine the patient thoroughly before taking him/her for any primary cleft surgery to rule out any systemic anomaly because many minor procedures e.g., skin tag excision, tongue tie release, syndactyly correction etc. can be performed comfortably along with primary procedure. By this way, we can save the child from the multiple procedures involving general anaesthesia.
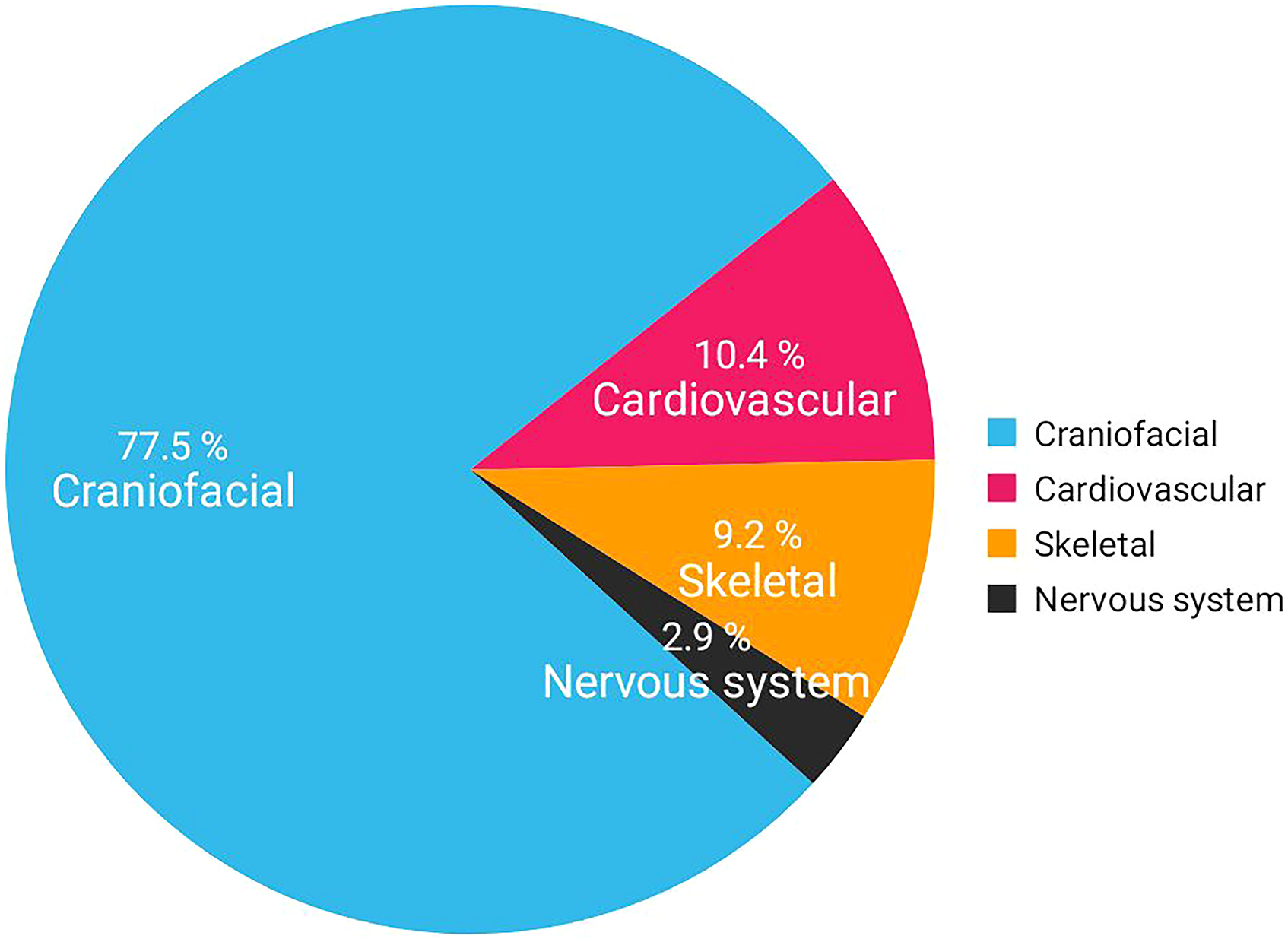
Region wise distribution of associated anomalies.
Study of this nature carries significant importance for the cleft care team especially beginners to understand the extent and severity of an OFC. This can help us to have a comprehensive assessment of the cleft deformity and treatment plan. The main limitation of our study is that it presents the data from one centre only. It is a fair possibility that the actual frequency of different phenotypes of OFC and associated malformations may be different from our figures as the present study included only those patients who were registered for the surgical care in our centre. It lacks the data of abortions, stillbirths and post-natal mortalities of children with OFC from our region.
Conclusion
An OFC may present themselves as an isolated deformity or a part of syndrome and be associated with anomalies of other organs. There can be hundreds of combinations of cleft lip and cleft palate with varying severity. In-depth knowledge of extent and severity of cleft deformities can help us to achieve satisfactory surgical outcome and prevent the patient from potential risks associated with the surgery.
Abbreviations
Orofacial cleft Cleft lip and palate Isolated cleft lip Isolated cleft palate Left side Right side Pierre Robin Sequence
Supplemental Material
sj-pdf-1-cpc-10.1177_10556656211057739 - Supplemental material for Morphological Presentation of Orofacial Clefts: An Epidemiological Study of 5004 Patients in a Tertiary Care Hospital of Central India
Supplemental material, sj-pdf-1-cpc-10.1177_10556656211057739 for Morphological Presentation of Orofacial Clefts: An Epidemiological Study of 5004 Patients in a Tertiary Care Hospital of Central India by Jaideep Singh Chauhan, MDS and Sarwpriya Sharma, MDS in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
We acknowledge Department of Paediatrics and Department of Anaesthesiology for their invaluable contribution in the presented study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.