
Abstract
Objective
This study compares patients undergoing early cleft lip repair (ECLR) (<3-months) and traditional lip repair (TLR) (3-6 months) with/without nasoalveolar molding (NAM) to evaluate the effects of surgical timing on weight gain in hopes of guiding future treatment paradigms.
Design
Retrospective review.
Setting
Children's Hospital of Los Angeles, California.
Patient, Participants
A retrospective chart review evaluated patients who underwent ECLR or TLR ± NAM from November 2009 through January 2020.
Interventions
No intervention was performed.
Main Outcome Measure(s)
Patient demographics, birth and medical history, perioperative variables, and complications were collected. Infant weights and age-based percentiles were recorded at birth, surgery, 8-weeks, 6-months, 12-months, and 24-months postoperatively. The main outcomes were weight change and weight percentile amongst ECLR and TLR ± NAM groups.
Results
107 patients met inclusion criteria: ECLR, n = 51 (47.6%); TLR + NAM, n = 35 (32.7%); and TLR-NAM, n = 21 (19.6%). ECLR patients had significantly greater changes in weight from surgery to 8-weeks and from surgery to 24-months postoperatively compared with both TLR ± NAM (P < .05). Age-matched weights in the ECLR group were significantly greater than TLR ± NAM at multiple time points postoperatively (P < .05).
Conclusions
ECLR significantly increased patient weights 24-months postoperatively when compared to TLR ± NAM. Specifically compared to TLR-NAM, ECLR weights were significantly greater at all time points past 6-months postoperatively. The results of this study demonstrate that ECLR can mitigate feeding difficulties and malnutrition traditionally seen in patients with cleft lip.
Introduction
Cleft lip and palate (CLP) is the most common congenital birth defect of the head and neck, occurring in approximately 1 in 700 live births (Parker et al., 2010; Vyas et al., 2020). Infants with CLP experience feeding difficulties secondary to poor suction, which often result in low weight gain and failure to thrive (FTT) (Beaumont, 2008; Koltz et al., 2012). Specialized feeding bottles may mitigate these issues; however, they are not permanent solutions and parents often must alternate between multiple devices to ensure adequate nutritional intake (Kumar and Khan, 2013; Goyal et al., 2014).
Traditional lip repair (TLR) follows the “Rule of 10 s,” as described by Wilhelmsen and Musgrave. As such, surgeons repair the cleft lip at 10 to 12 weeks of age, when anesthesia was perceived to be safer and most patients would have met the cut-offs of weight greater than 10 pounds, hemoglobin greater than 10 g/dL, and white blood cell count greater than 10 000 mm3 (Wilhelmsen and Musgrave, 1966). With novel anesthetic agents and improved surgical techniques, these principles must be reconsidered and the utility of early cleft lip repair (ECLR) should be revisited (Chow et al., 2016).
At this senior author's institution, a paradigm shift has occurred where many neonates and young infants undergo early primary cleft lip repair in patients with unilateral defects at 2 to 5 weeks of age rather than presurgical nasoalveolar molding (NAM) followed by a traditionally timed repair at 3 to 6 months of age (Hammoudeh et al., 2017; Wlodarczyk et al., 2021b). A novel dexmedetomidine-based neonatal anesthetic protocol (DBNAP), with perioperative equivalence to traditional anesthetics using a volatile gas-based regimen, was developed for patients undergoing ECLR (Wlodarczyk et al., 2021a).
The purpose of this study was to evaluate whether ECLR promotes infant weight gain in healthy patients with unilateral cleft lip. The primary outcomes were differences in weight changes and age-based weight percentiles between patients who underwent ECLR and those who received TLR with/without NAM (TLR ± NAM). This study will also attempt to establish a weight-based safety threshold for neonates and young infants undergoing ECLR.
Methods and Materials
Institutional Review Board (IRB ID: CCI-14-00001) approval was obtained for retrospective review of patients who underwent unilateral cleft lip repair with/without NAM between November 2009 and January 2020. Patients were separated into 3 groups: (1) patients who received primary lip repair at less than 12 weeks of age without presurgical NAM (ECLR), (2) patients who underwent presurgical NAM and TLR (TLR + NAM), and (3) patients who underwent TLR without presurgical NAM (TLR-NAM). Historically, this institution ran one of the largest NAM programs in the country; over the past 6 years, all patients with unilateral cleft lip, regardless of cleft width, who are ASA class ≤ II without major comorbidities are being offered ECLR with 98% acceptance rate by families (Figure 1). “A Novel Protocol in Early Cleft Lip Repair: Demonstrating Efficacy and Safety in the First 100 Patients,” revealed the ability of ECLR to sufficiently manage large cleft widths upon comparing cleft severity scores between patients undergoing ECLR (2015-present) versus TLR (2005-present) (Wlodarczyk et al., 2020); there were statistically significant larger cleft width ratios in the ECLR cohort versus that of the TLR + NAM cohort even after excluding incomplete clefts from the ECLR cohort.
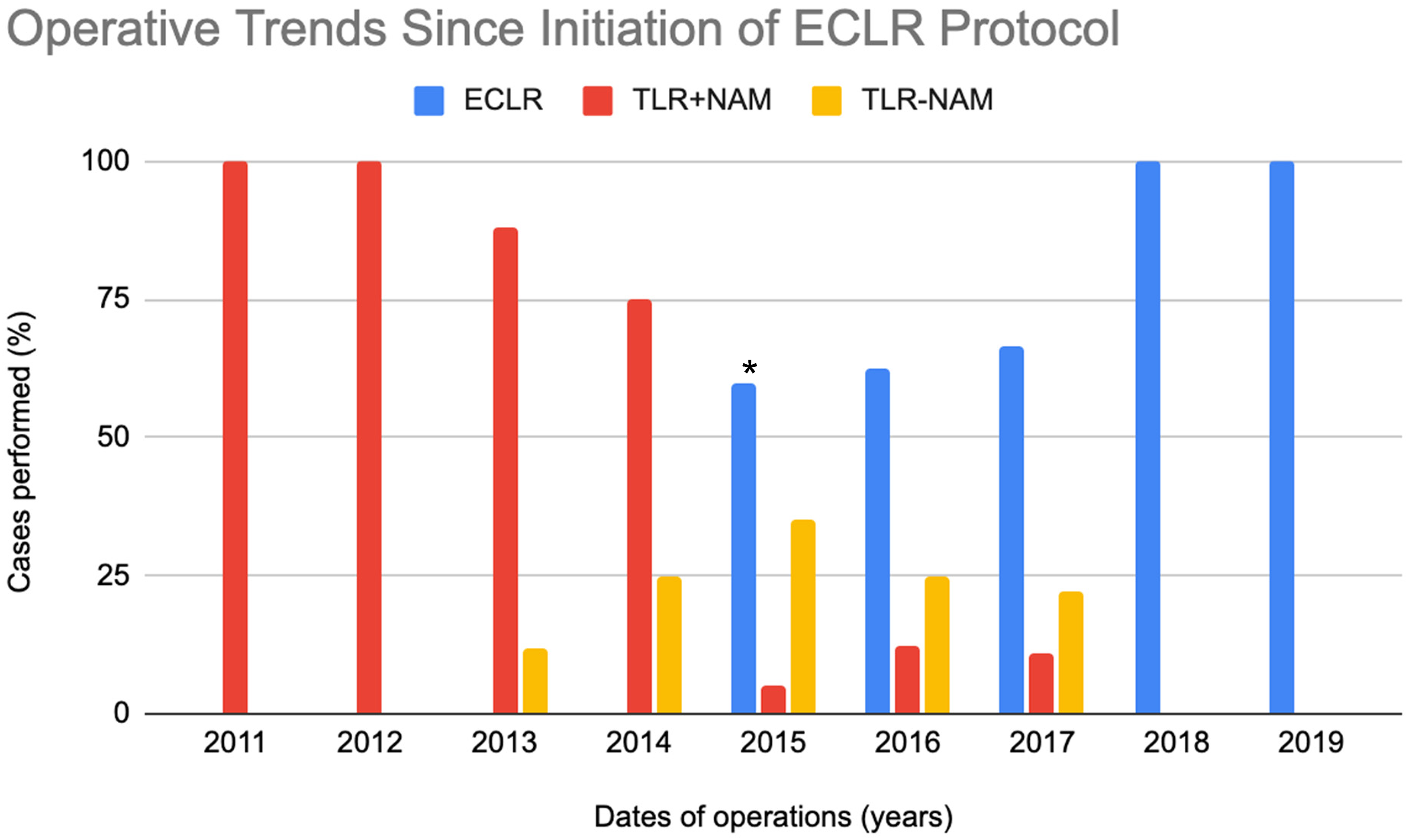
Historical trends in ECLR versus TLR ± NAM operations at our institution.
Inclusion criteria for this study were the following: (1) age less than 3 months (ECLR group) or between 3 to 6 months (TLR), (2) no major comorbidities (American Society of Anesthesiologist [ASA] class I or class II), and (3) diagnosis of non-syndromic unilateral cleft lip without palatal involvement. ASA classification was assigned preoperatively by the Anesthesia Department. ASA class I designated “normal healthy patients,” whereas ASA class II designated patients with “mild systemic disease.” It is important to note that ASA classification shows poor interrater reliability in pediatric and adult practices, alike, resulting in some patients with CLP and no comorbidities to be assigned ASA class I while others carried ASA class II (Aplin et al., 2007). Patients older than 6 months, or with bilateral cleft lip, cleft palate, clefts associated with craniofacial syndromes, or significant systemic comorbidities (ie, ASA class ≥ III) were excluded. All patients’ records were reviewed for associated major congenital anomalies and preoperative anesthesia evaluations to determine study eligibility.
Adjusted ages at time of surgery were reported for all participants to account for 6 premature patients. Patient weights (kg) were recorded at birth, time of surgery, 8-weeks, 6-months, 12-months, and 24-months postoperatively. Both changes in weight (kg) and growth chart percentiles (%) were analyzed between groups. Significant associations between variables were calculated with independent Student's t-tests, chi-square, and one-way analysis of variance. Descriptive statistics and significance testing were performed on SPSS Advanced Statistics version 28.0.
Results
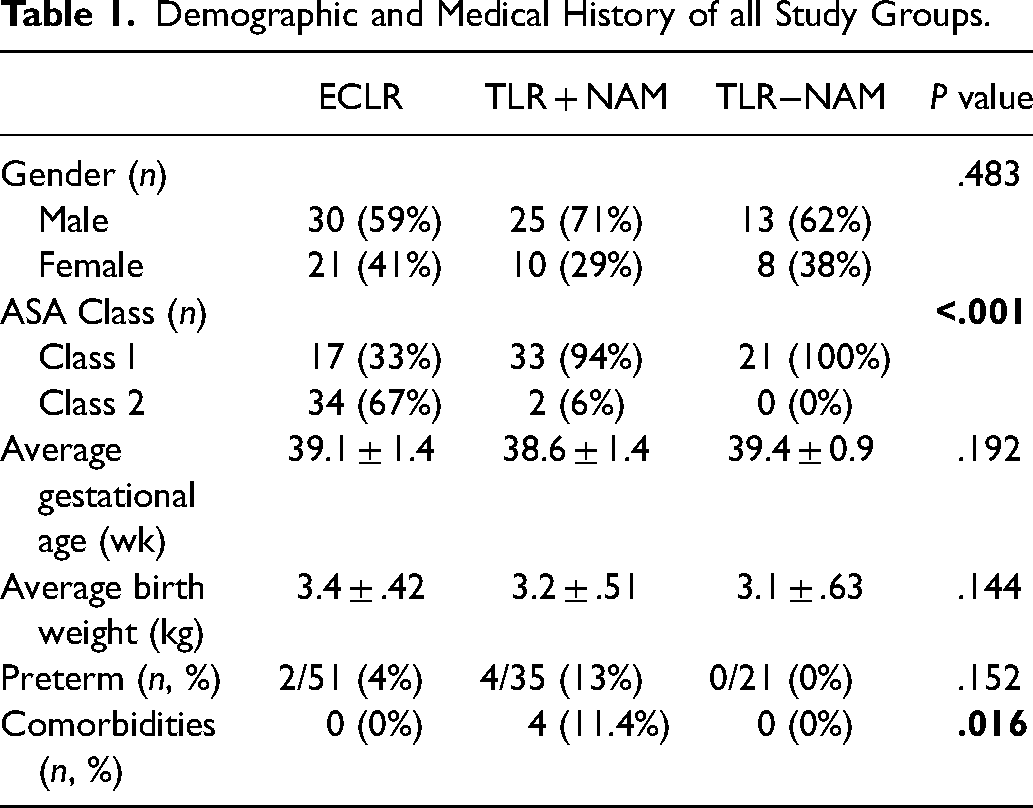
The medical records of 107 patients who underwent unilateral cleft lip repair were reviewed: ECLR n = 51 (47.6%), TLR + NAM n = 35 (32.7%), and TLR-NAM n = 21 (19.6%). ECLR, TLR + NAM, and TLR-NAM had similar average gestational ages at birth: 39.1 ± 1.4 weeks, 38.6 ± 1.4 weeks, and 39.4 ± 0.9 weeks, respectively. Six patients were preterm (2 ECLR, 4 TLR + NAM), defined as a gestational age less than 37 weeks. Mean patient birth weights were not significantly different across the 3 cohorts. Overall, there were 71 ASA class I patients (66.3%) and 36 ASA class II patients (33.6%), with a significant difference in ASA class between the 3 cohorts (P < .001, Table 1). TLR + NAM was the only group containing patients with comorbidities (n = 4, P = .016), which included: 2 patients with FTT requiring gastrostomy tubes, one of which had concurrent monosomy 18; one patient with obstructive sleep apnea; and another patient with a ventricular septal defect (Table 1). There were no major adverse events recorded with the ECLR operations. Additionally, there were no major complications reported with the DBNAP anesthesia regimen utilized during the operations.
Demographic and Medical History of all Study Groups.
ECLR patients were 31.8 ± 14.8 age-adjusted days old (mean ± SD) at time of surgery. TLR + NAM patients were 110.8 ± 27.3 days at time of surgery. Changes in weight were significantly greater in ECLR versus TLR + NAM patients between surgery and 8-weeks (0.70 ± 0.48 vs −1.07 ± 0.75, P < .001) and between surgery and 24-months postoperatively (8.77 ± 1.40 vs 6.13 ± 1.53, P < .001). Average weight percentile for ECLR was significantly greater than TLR + NAM (28.0 ± 12.6 vs 22.8 ± 26.2, P < .001) at time of surgery. At 24 months, ECLR patients had significantly greater weight percentiles than TLR + NAM (62.7 ± 30.9 vs 50.0 ± 31.8, P = .029) (Table 2). While ECLR patients demonstrated higher weight percentiles at 6- and 12-months, these differences were not statistically significant when compared to the TLR + NAM cohort (Figure 2). Although the average weight of the TLR + NAM group was greater than that of the ECLR group at 8-weeks postoperatively, there was a smaller proportion of ECLR patients in the <5th percentile weight group; this trend was consistent throughout the ECLR to TLR + NAM comparisons, with a smaller percentage of ECLR patients in the <5th percentile group at all perioperative stages.
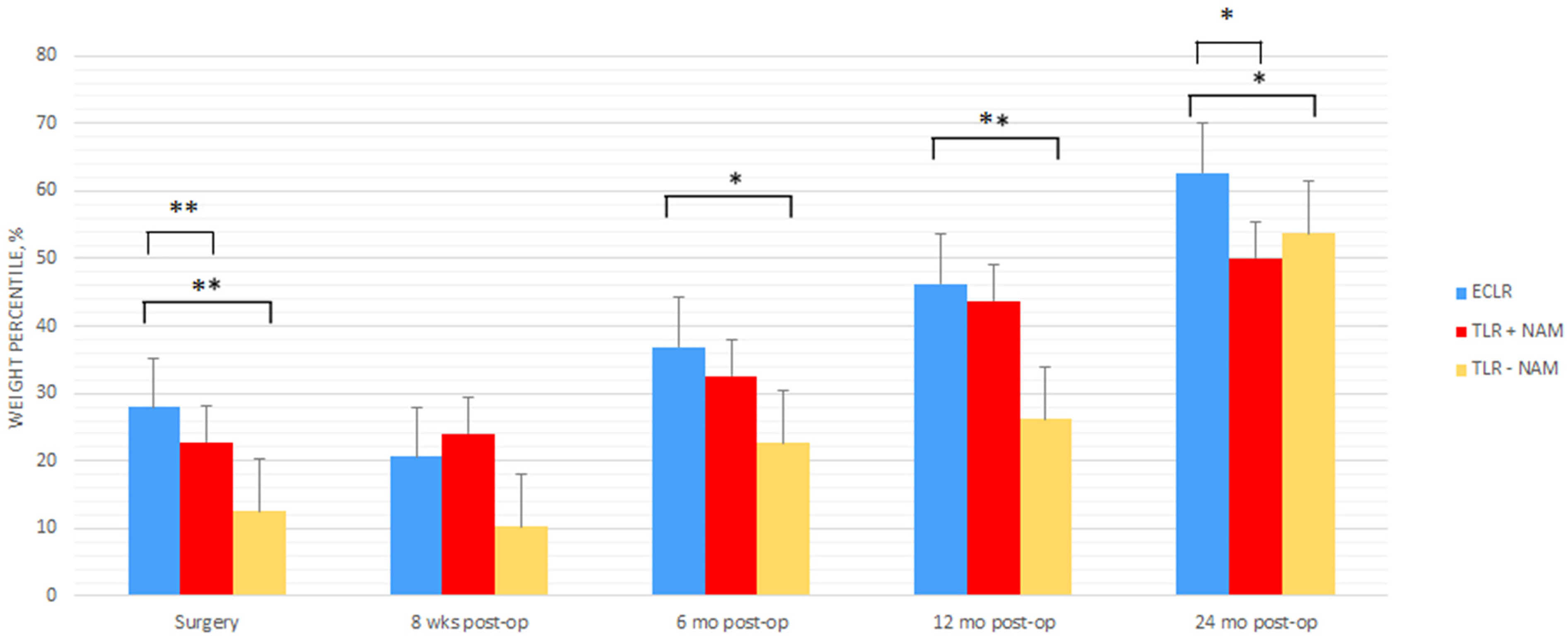
Statistical comparisons of weight percentiles across surgical groups.
Weight Outcome Comparison Between ECLR and TLR + NAM.
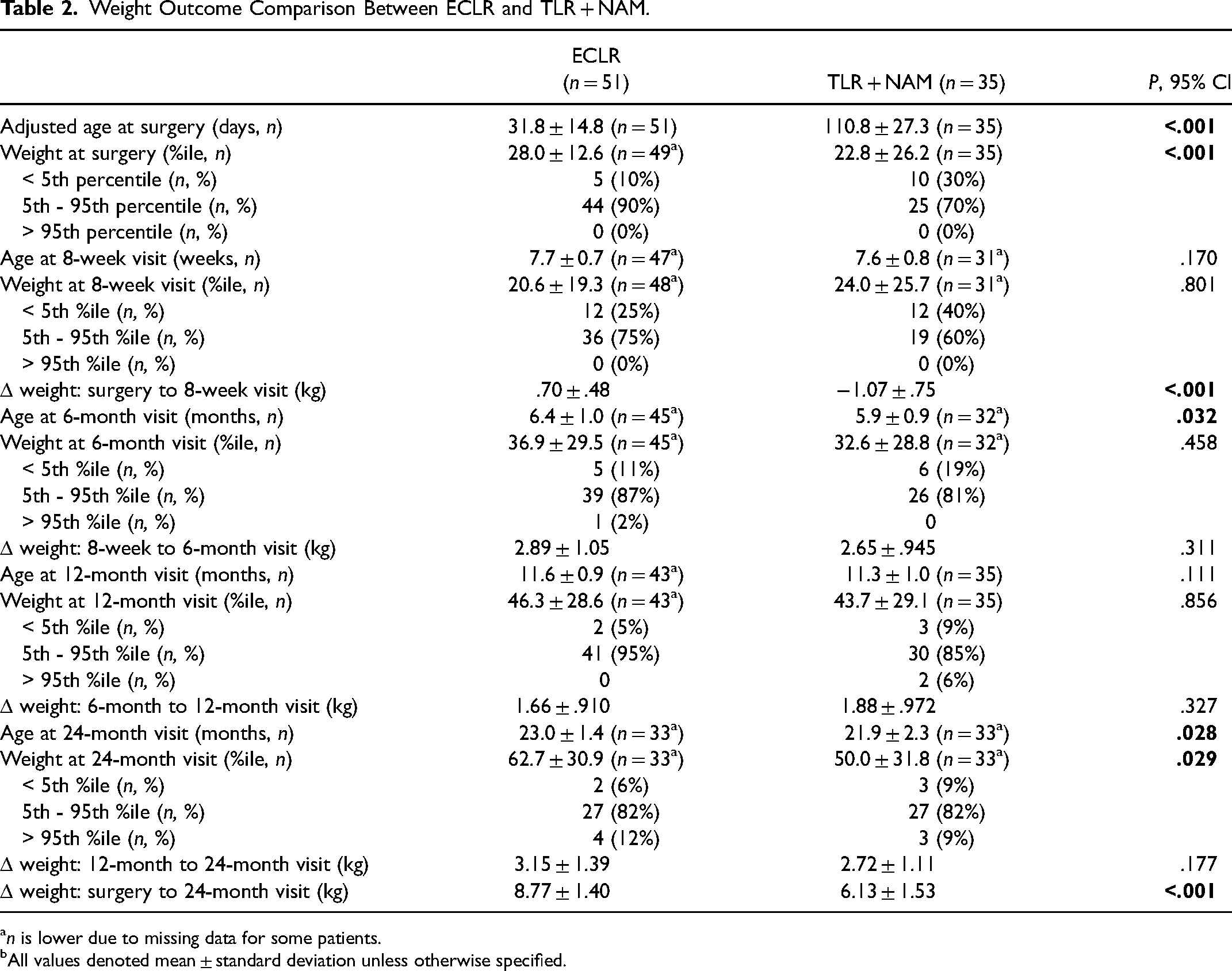
n is lower due to missing data for some patients.
All values denoted mean ± standard deviation unless otherwise specified.
TLR-NAM patients were 113.3 ± 21.6 days old at surgery. Changes in weight were significantly greater in ECLR versus TLR-NAM between surgery and 8-weeks (0.70 ± .48 vs −0.80 ± .43, P < .001) and between surgery and 24-months postoperatively (8.77 ± 1.40 vs 6.00 ± 1.15, P < .001). Average weight percentile for ECLR was significantly greater than TLR-NAM (28.0 ± 12.6 vs 12.6 ± 13.6, P < .001) at time of surgery. At 6-months postoperatively, average weight percentile for ECLR was significantly greater than TLR-NAM (36.9 ± 29.5 vs 22.7 ± 18.4, P = .034). At 12-months postoperatively, average weight percentile for ECLR was significantly greater than TLR-NAM (46.3 ± 28.6 vs 26.2 ± 18.5, P = .002). At 24-months postoperatively, average weight percentile for ECLR was significantly greater than TLR-NAM (62.7 ± 30.9 vs 53.7 ± 25.7, P = .014) (Table 3). While ECLR patients demonstrated a higher weight percentile at 8-weeks, the difference was not statistically significant when compared to the TLR-NAM cohort (Figure 2).
Weight Outcome Comparison Between ECLR and TLR–NAM.
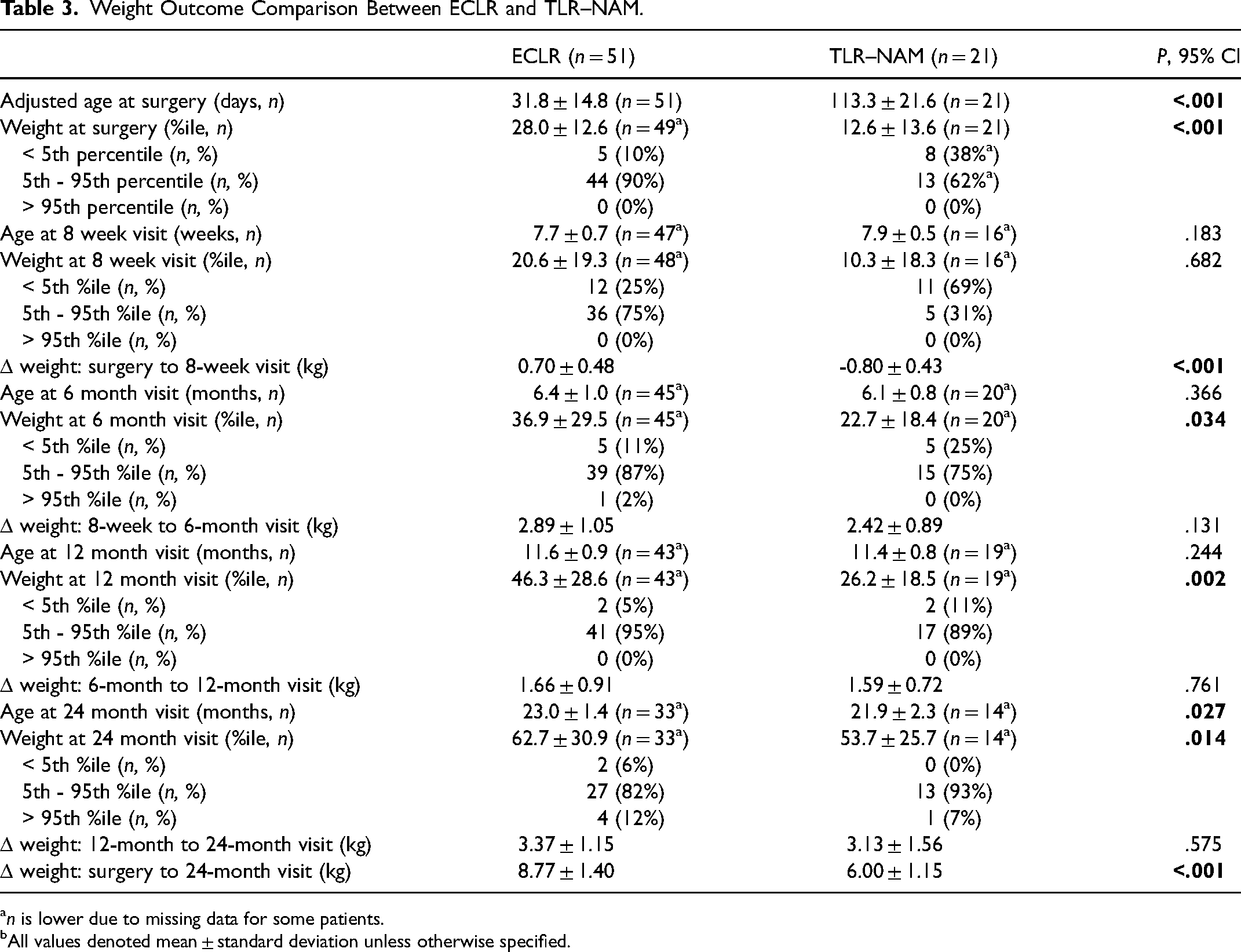
n is lower due to missing data for some patients.
All values denoted mean ± standard deviation unless otherwise specified.
Discussion
Many studies over the years have demonstrated FTT and/or poor weight in patients with cleft lip ± palate (Avedian and Ruberg,1980; Jones, 1988; Lazarus et al., 1999; Pandya and Boorman, 2001; Montagnoli et al., 2005; Miranda et al., 2016). The rate of FTT in isolated unilateral cleft lip patients alone has been reported to be over 30% (Pandya and Boorman, 2001). Further, almost a quarter of patients with cleft lip have been found to be under the 10th weight percentile during their first 2 years of life (Montagnoli et al., 2005). At the time of surgery, ECLR demonstrated a significantly greater age-matched weight percentile compared to both the TLR ± NAM groups. Thus, our results suggest that, although younger, patients undergoing ECLR may be more nutritionally replete and better suited for surgery since delaying repair for TLR leads to diminishing rates of growth during the weeks they await surgery.
Both ECLR and NAM take advantage of the neonatal tissue plasticity secondary to persisting levels of maternal estrogen that peak 72 h after birth and steadily decline over the following 3 weeks (Matsuo et al., 1984; Anstadt et al., 2016; Hammoudeh et al., 2017). This rationale is analogous to that of neonatal ear molding. Given the dropping levels of circulating maternal estrogen, surgeons should consider more aggressive treatment strategies to take advantage of tissue plasticity in neonates. ECLR patients had a significantly greater weight percentile compared to TLR + NAM at 24-months and more prevalent weight discrepancies compared to TLR-NAM throughout the postoperative period. We postulate that TLR + NAM patients were able to maintain similar weight percentiles as ECLR during the early postoperative period due to the protective effect of NAM. Studies have demonstrated that NAM can improve growth and enhance treatment outcomes in patients with cleft lip ± palate (Woods et al., 2019); accordingly, NAM may have positively influenced weight gain in our TLR + NAM cohort. The role that NAM plays in improving weight gain for patients undergoing TLR is further highlighted by the significant weight discrepancy between the ECLR and TLR-NAM cohort at even earlier postoperative time points (6-, 12-, and 24-months).
NAM, however, has several disadvantages: biweekly dental clinic visits, parental adherence to an appliance protocol, and significantly higher costs to the healthcare system and families compared to ECLR (Abbott and Meara, 2012; Esmonde et al., 2018; Wlodarczyk et al., 2021b). In one study by Wlodarczyk et al. (2021b), diverting the first 100 ECLR patients from NAM resulted in a decreased cost burden of $ 368 700 ($ 111 727 per year) on the healthcare system. Included in this cost burden is lost wages for families with a child receiving NAM, which totals $2738. Overall, our results support the use of ECLR over TLR + NAM not only by improving weight at the time of surgery and the 24-month time point, but also by reducing the financial strain and physical burden that NAM has on families and the greater medical community alike. The cost-saving results, in particular, promise for future higher grossing savings with the implementation of ECLR at other institutions.
Although ECLR patients are younger at time of surgery and require overnight observation, the cost of care for ECLR versus TLR is still comparable. Based on the current literature on national cleft care trends, most patients who undergo TLR stay overnight for inpatient observation (Hopper et al., 2009). At our institution, patients undergoing ECLR stay overnight for observation while TLR is performed on an outpatient basis; nevertheless, insurance authorization covers a 23 h observation, and thus, the cost of ECLR should equate that of TLR based on national standards.
While advantages of ECLR include improved aesthetic outcomes, wound healing, and parental mental health (Burianova et al., 2017), there is persistent concern regarding the effects of anesthetic agents on neonatal neurological development. Our institution developed a novel DBNAP for patients undergoing ECLR without any increase in adverse events compared to traditional volatile anesthetic agents (Wlodarczyk et al., 2021b). Several primate and rodent models have shown neuronal apoptosis with the use of GABA agonist and NMDA receptor antagonists (Ikonomidou et al., 1999; Jevtovic-Todorovic et al., 2003; Lee et al., 2015). However, animal models are not always representative of human biological systems (Gritli-Linde, 2008). Furthermore, the potencies of anesthetics vary within species, and age during exposure for the species studied may not correlate with the same stage of human brain development (Lin et al., 2017). To add, several large prospective studies have shown no negative long-term neurocognitive complications associated with neonatal anesthetic exposure (Cappuccio et al., 2018; McCann and Soriano, 2019), especially when novel agents, such as fentanyl-based analgesics and dexmedetomidine, are utilized (Cappuccio et al., 2018).
The results of this study suggest that performing cleft lip repair on patients as young as 13 days old is safe and improves weight gain during infancy. No patients in this study suffered major complications, so a weight-based threshold to guide ECLR eligibility was unable to be established. Other studies have similarly reported that cleft lip repair, independent of timing, results in overall better weight gain and is not associated with a significant risk of surgical wound dehiscence and resultant postoperative feeding limitations (Kaye and Che, 2019; Matsunaka et al., 2019). Our findings align with the literature and provide evidence that ECLR improves postoperative weight gain and can eliminate the need for NAM in appropriate patients.
Limitations and Bias
There are several limitations to this study. Feeding techniques, nutritional variation, and genetic factors are potential confounders that could impact feeding. Thus, we cannot assume that ease of feeding alone determines infant weight. Other study limitations include a single institution protocol and non-randomization of patients. Our study excluded patients with bilateral cleft, palatal involvement, or incomplete cleft in an effort to standardize the comparison and reduce alveolar and palatal clefting as a potential source of confounding. Future studies will be needed to further evaluate the effectiveness of ECLR on patients with these different deformities and their ability to gain weight.
Conclusion
ECLR significantly increased patient weights 24-months postoperatively when compared to TLR ± NAM. Furthermore, age-matched weights in the ECLR group were significantly greater than TLR ± NAM at multiple time points post-operatively. These results not only continue to support the novel ECLR protocol, but also suggest that ECLR is advantageous for improved patient feeding and growth, thereby mitigating malnutrition traditionally seen in patients with cleft lip.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
IRB Approval
This study was reviewed by Children's Hospital of Los Angeles’ IRB review board and approved with the identification number of