
Abstract
Pedicled buccal fat flaps have been adopted in primary Furlow double-opposing Z-plasty palatoplasty to reduce oronasal fistula formation or to attenuate maxillary growth disturbance. We combined both goals in a single intervention. This study describes a series of 33 modified Furlow small double-opposing Z-plasty palatoplasties reinforced with a middle layer of pedicled buccal fat flaps between the oral and nasal layers for full coverage of the dissected palatal surfaces, with rapid mucosalization of lateral relaxing incisions and no dehiscence or fistula formation.
Introduction
Decreasing the fistula rate (Losken et al., 2011; Tache and Mommaerts, 2019), achieving a functional muscle sling (Ha et al., 2007; Perry et al., 2018), and reducing bone exposure- and scar retraction-related maxillary growth interference (Liao and Mars, 2006) have been considered key endpoints in primary palatoplasties (Timbang et al., 2014; Pai et al., 2019).
In this setting, results have encouraged the use of pedicled buccal fat pad flaps in original and modified Furlow double-opposing Z-plasty palatoplasties (Levi et al., 2009; Yamaguchi et al., 2016; Bennett et al., 2017; Qiu et al., 2019; Jung and Lo, 2020; Thurston et al., 2020; Denadai and Lo, 2021; Lo et al., 2021; Kotlarek et al., 2021a, 2021b). Interpositional buccal fat flaps have been applied in the anterior region of the soft palate to fill the dead space between the oral and nasal flaps, alleviating possible palatal contraction during the healing process, and reducing dehiscence or fistula formation (Qiu et al., 2019; Thurston et al., 2020; Denadai and Lo, 2021; Kotlarek et al., 2021a). The lateral denuded bone surfaces were covered with pedicled buccal fat flaps to reduce healing by secondary intention and subsequent impairment of the maxillary arch development, and maxillary growth (Levi et al., 2009; Yamaguchi et al., 2016; Jung and Lo, 2020; Denadai and Lo, 2021; Khan et al., 2021; Lo et al., 2021). We combined these potential benefits in a single intervention.
This study describes the use of interpositional buccal fat flaps for full coverage of the dissected palatal surface in modified Furlow palatoplasty.
Methods
Consecutive nonsyndromic patients with cleft palate surgically treated by the first author were retrospectively included. All postoperative complications, such as donor-site hematoma, adverse airway events, reintubation, bleeding requiring operative intervention, infection, flap necrosis, hanging palate, hanging buccal fat pad, superficial dehiscence (breakdown of the partial-thickness repair that spontaneously closed), and oronasal fistula (any communication between the oral and nasal cavities due to complete, full-thickness repair breakdown) were identified based on regular palatal examinations during hospitalization and follow-ups at 1, 7, and 14 days, and 1, 3, and 6 months after palatoplasty.
Patients with submucous cleft palate, any associated syndromes (Pierre Robin sequence), and/or incomplete medical records were excluded from this study.
Surgical Description
Primary palatoplasty was routinely performed at 9 months of age; however, in some circumstances, it was delayed owing to late referral. Using a 2.5 × loupe magnification, the modified Furlow palatoplasty (Yamaguchi et al., 2016; Jung and Lo, 2020) was performed using hard palate mucoperiosteal flaps and soft palate small double-opposing Z-plasty with muscle reconstruction (
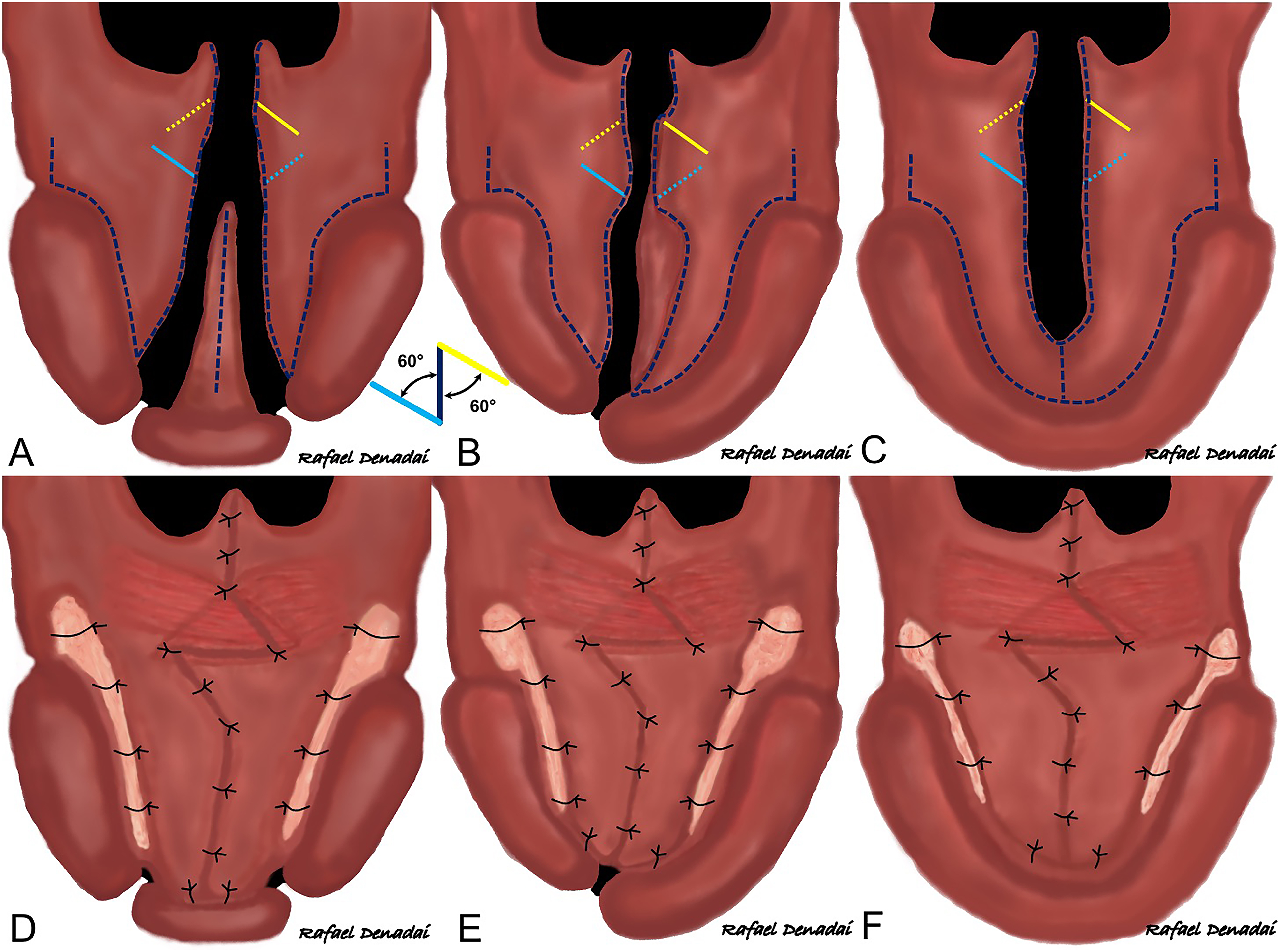
Schematic drawings of (A–C) surgical design and (D–F) final aspect of oral side of the repair in veau II, III, and IV cleft palates using the hard palatal 2-flap approach, vomer turnover flap, and modified Furlow small double-opposing Z-plasty plus interpositional pedicled buccal fat flap. Oral mucoperiosteal flaps are returned to their original anterior position with no attempt to push back. The anteriorly based oral and nasal mucosal flaps (solid and dashed yellow lines, respectively) are transposed with the posteriorly based oral and nasal musculomucosal flaps (solid and dashed blue lines, respectively). Musculomucosal flaps are overlapped with added functional tension to reconstruct the muscle sling. A middle layer of pedicled fat pad tissue is created between the oral and nasal layers (Figures 2 and 3), covering the lateral palatal incisions.

Schematic drawings of (A) veau III cleft palate repair using hard palatal 2-flap approach and modified Furlow small double-opposing Z-plasty (anteriorly based mucosal flaps and posteriorly based musculomucosal flaps are displayed in yellow and blue lines, respectively) plus interpositional pedicled buccal fat flap. (B) Nasal side of the repair with the anterior nasal layer reconstructed using vomer turnover flap sutured with the anterior nasal mucoperiosteal flap plus small Z-plasty with transposition of the right musculomucosal flap posteriorly and the left mucosal flap anteriorly. The pedicled buccal fat flaps are (C) tunneled submucosally behind the greater palatine neurovascular bundles, (D) fixed to the maxillary arch anteriorly and laterally, and (E) fixed to each other in the midline region.

(A) Intraoral images (surgeon's view) of a veau III cleft palate repair. (B, C) Retropositioning of cleft muscle (palatoglossus, palatopharyngeus, and levator veli palatine muscles) mass with transposition of the left nasal (dotted yellow line) and right oral (yellow line) mucosal flaps anteriorly and the right nasal (dotted blue line) and left oral (blue line) musculomucosal flaps posteriorly. After repair of the nasal layer and uvula, (D) the pedicled buccal fat flaps are tunneled posterior to the pedicle of the mucoperiosteal flaps to the palatal repair site. The flaps are spread to fully cover the dissected palatal surface, (E) fixed to the maxillary arch, and (F) stabilized in the midline area. (C) After repair of the oral layer, no lateral palatal region is denuded as it resurfaced with the buccal fat tissue.
Oral antibiotics were prescribed for 7 days. A liquid diet was recommended for 2 weeks, with no need for arm splints.
Results
Thirty-three patients with Veau types II, III, and IV cleft palates underwent primary modified Furlow palatoplasty using small double-opposing Z-plasty plus the newly reported pedicled fat pad flap-based surgical technique. All lateral palatal recipient areas were fully mucosalized within 3 weeks (Supplemental Figure 3), with no donor-site hematoma, bleeding, infection, flap necrosis, dehiscence, or fistula (Supplemental Table 1).
Discussion
A growing body of literature has demonstrated the value of fat tissue in enhancing the healing process, with pedicled buccal fat flaps applied to improve the outcomes of Furlow double-opposing Z-plasty palatoplasties (Levi et al., 2009; Yamaguchi et al., 2016; Bennett et al., 2017; Qiu et al., 2019; Jung and Lo, 2020; Thurston et al., 2020; Denadai and Lo, 2021; Lo et al., 2021; Kotlarek et al., 2021a, 2021b). Harvesting and placing of buccal fat flaps have increased operations by 10 to 15 min, without comprising the facial symmetry (Levi et al., 2009; Bennett et al., 2017; Qiu et al., 2019; Thurston et al., 2020; Denadai and Lo, 2021).
We described a novel technical alternative that utilized pedicled buccal fat flaps to add a middle layer of autologous vascularized tissue between the oral and nasal layers for full coverage of the repaired palatal surface (Supplemental Figure 4), filling the dead space created after palatal and muscle dissection and mobilization, avoiding bony exposure or any exposed raw areas with healing by secondary intention in the lateral portion of the hard and soft palates, and consequently, reducing scar formation and contraction. Careful dissection of the mucoperiosteal flaps with the release of tension surrounding the neurovascular pedicle cannot be overemphasized (Jung and Lo, 2020). By reinforcing the suture lines with an additional layer of fat tissue, mucosal healing was enhanced in the palatal areas (regions with a wide cleft, mucosal tears during dissection or closure, or with incomplete closure) with a high risk of postoperative dehiscence and oronasal fistula formation (Supplemental Figure 5).
Our retrospective analysis of the 6-month complication rate revealed that this modified Furlow double-opposing Z-plasty palatoplasty with the 3-layer repair of the hard and soft palates resulted in adequate cleft palate closure with rapid mucosalization of lateral relaxing incisions and no wound separation or fistula formation. This corroborates published data of satisfactory palatal healing status with reduced fistula rates following the use of pedicled buccal fat flaps in Furlow palatoplasties (Levi et al., 2009; Bennett et al., 2017; Qiu et al., 2019; Horswell and Chou, 2020; Kim et al., 2020; Thurston et al., 2020; Denadai and Lo, 2021). Interestingly, recent comparative investigations have demonstrated that adding buccal fat flaps in Furlow double-opposing Z-plasty palatoplasty improves the postoperative palatal length (Kotlarek et al., 2021a) and transverse maxillary development (Lo et al., 2021). Based on the existing objective data (Thurston et al., 2020; Lo et al., 2021; Kotlarek et al., 2021a), we hypothesized that this modified palatoplasty technique could not only reduce the wound dehiscence and fistula formation for early postoperative outcomes but also achieve a satisfactory speech outcome and reduce the probable negative influence on transverse maxillary arch development and midfacial growth. However, the potential benefit of enhanced muscle sling functioning due to less fibrotic tissue formation and prevention of maxillary growth disturbance by reducing scar contraction remains theoretical, as our 6-month follow-up interval restricts any conclusion. Further long-term outcome research is needed to show the impact of adding interpositional pedicled buccal fat flaps on modified Furlow double-opposing Z-plasty palatoplasty-related speech and midfacial growth outcomes. Future investigation should also characterize the effect of small double-opposing Z-plasty on intraoperative palatal lengthening.
In the literature, an interpositional layer has been created between the oral and nasal layers in the soft palate region using different alternatives (acellular dermal matrix, hemostatic gelatin sponge, collagen membrane, and platelet-rich plasma) to enhance mucosal healing and reduce fistula formation (Losee et al., 2008; Hudson and Pickett, 2015; El-Anwar et al., 2016; Li et al., 2017; Goh and Chia, 2019; Simpson et al., 2019; Ha et al., 2020; Tanaka et al., 2021). Modifications on palatal dissection (subperiosteal flap technique vs mucoperiosteal flap technique) (Leenstra et al., 1996; Ito et al., 2006) and lateral relaxing incision (only a small incision lateral to the hamulus or no use of lateral incision) (Karsten et al., 2003; Becker and Hansson, 2013; Parikakis et al., 2018; Seo et al., 2019) have also been proposed to attenuate bone denudation-related scar contracture and subsequent maxillary growth interference. Future fistula rate- and maxillary development-focused outcome studies could then compare the described approach based on the use of interpositional buccal fat flaps.
Conclusion
This modified Furlow double-opposing Z-plasty palatoplasty with a 3-layer soft tissue closure of the hard and soft palate regions using pedicled buccal fat pad flaps to compose the middle layer provided adequate cleft palate closure, with satisfactory mucosalization of the raw lateral palatal regions, and without fistula formation.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656211064769 - Supplemental material for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair
Supplemental material, sj-docx-1-cpc-10.1177_10556656211064769 for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair by Rafael Denadai, Pang-Yun Chou and Lun-Jou Lo in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-2-cpc-10.1177_10556656211064769 - Supplemental material for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair
Supplemental material, sj-jpg-2-cpc-10.1177_10556656211064769 for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair by Rafael Denadai, Pang-Yun Chou and Lun-Jou Lo in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-3-cpc-10.1177_10556656211064769 - Supplemental material for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair
Supplemental material, sj-jpg-3-cpc-10.1177_10556656211064769 for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair by Rafael Denadai, Pang-Yun Chou and Lun-Jou Lo in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-4-cpc-10.1177_10556656211064769 - Supplemental material for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair
Supplemental material, sj-jpg-4-cpc-10.1177_10556656211064769 for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair by Rafael Denadai, Pang-Yun Chou and Lun-Jou Lo in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-5-cpc-10.1177_10556656211064769 - Supplemental material for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair
Supplemental material, sj-docx-5-cpc-10.1177_10556656211064769 for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair by Rafael Denadai, Pang-Yun Chou and Lun-Jou Lo in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-6-cpc-10.1177_10556656211064769 - Supplemental material for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair
Supplemental material, sj-jpg-6-cpc-10.1177_10556656211064769 for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair by Rafael Denadai, Pang-Yun Chou and Lun-Jou Lo in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-7-cpc-10.1177_10556656211064769 - Supplemental material for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair
Supplemental material, sj-jpg-7-cpc-10.1177_10556656211064769 for Reinforcing the Modified Double-Opposing Z-Plasty Approach Using the Pedicled Buccal Fat Flap as an Interpositional Layer for Cleft Palate Repair by Rafael Denadai, Pang-Yun Chou and Lun-Jou Lo in The Cleft Palate Craniofacial Journal
Footnotes
Authors’ Note
R.D. and P.Y.C contributed to the acquisition, analysis, and interpretation of data. R.D., P.Y.C., and L.J.L. contributed to conceptualization and writing—original draft. All authors have read and agreed to the published version of the manuscript.
Acknowledgments
The authors would like to thank the anesthetic team for assistance during data collection of operation time and early postoperative complication. The first author would like to thank the Noordhoff Craniofacial Foundation for the provision of support during craniofacial surgical training as well as delivery of surgical cleft care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.