
Abstract
Objective
Robin Sequence (RS), characterized by micrognathia, glossoptosis, and upper airway obstruction, is an increasingly recognized diagnosis. An effective surgical intervention is mandibular distraction osteogenesis (MDO). This study analyzes published evidence regarding facial nerve dysfunction (FND) associated with MDO.
Design and Setting
According to PRISMA guidelines, a systematic review was carried out with databases queried in June 2019 using MESH terms, or equivalent terms, as follows: “distraction osteogenesis” and “Robin Sequence”. A review of original Spanish and English articles, were included. Outcome measures included the prevalence of FND; the affected branches; the rate of permanent vs. transient FND; the use of an internal vs. external device; the daily distraction rate; and finally, the overall distraction length. Subsequently, a meta-analysis was conducted to collate results regarding the prevalence of FND and the factors associated with it.
Results
Of 239 unique studies identified, 19 studies with 729 patients met inclusion criteria; 52 patients developed FND after MDO. A random-effects meta-analysis yielded a pooled prevalence of FND of 6.40%, with moderately heterogeneous studies (I2 = 41%, τ2 = 0.006). Marginal mandibular nerve involvement was most commonly noted. Nine studies reported transient FND, six permanent, one both, and two unspecified. Internal distractors were used in 8 studies and external in 3 and both in 2. Distraction rate was 1.00 to 2.00 mm/day and total distraction length ranged from 13.00 to 22.3 mm. Sample size was the only parameter inversely associated with rate of FND (p = 0.04).
Conclusion
This analysis of FND associated with MDO for patients with RS demonstrates a lack of consistent documentation. MDO-associated FND does not appear to be uncommon, and permanent dysfunction can occur. This review underscores the importance of thorough documentation to elucidate the mechanism of FND.
Introduction
The clinical triad of micrognathia, glossoptosis, and upper airway obstruction (UAO) is known as Robin sequence (RS), a diagnosis with important potential implications in the newborn period and beyond. Of particular concern is the risk for clinically significant systemic hypoxia (O2 saturation <90%) due to varying degrees of airway obstruction, as there is growing evidence that chronic disturbances in gas exchange due to apnea can result in end organ damage, as well as neurodevelopmental delays continuing into adolescence (Gangopadhyay et al., 2012). Thus, appropriate interventions that improve and normalize upper airway dynamics may be critical in avoiding these adverse effects of UAO.
Surgical airway management in patients with RS remains controversial. Indications and choice of intervention in these complex patients are often not universally accepted. Mandibular distraction osteogenesis (MDO) is a popular surgical procedure performed after subjective failure of conservative management such as prone positioning, airway support, and nasopharyngeal airway (NPA).1 Tongue lip adhesion (TLA) is another surgical option which has been shown to be successful in select patients (ie, GILLS score <3)(Rogers et al., 2011). Finally, tracheostomy is an effective surgical airway procedure that is often reserved for critically ill patients or those who have failed either TLA or MDO, due to associated potential complications, including prolonged burden of care (Han et al., 2012).
Compared to TLA and tracheostomy, MDO is a relatively new intervention for patients with RS that gradually lengthens the mandible and its surrounding soft tissues, thereby relieving tongue-based airway obstruction (Seaward and Kane, 2013). The physiological processes of distraction osteogenesis were initially described for extremity lengthening, (Ilizarov, 1989; Ilizarov, 1992, 1989) followed by landmark studies by McCarthy and colleagues documenting its successful application in mandibular lengthening in patients with craniofacial microsomia (McCarthy et al., 1992). MDO for patients with RS was first described in 1999 by Judge and colleagues (Judge et al., 1999), while Denny and associates were among the first to document its usefulness in neonates.(Bangiyev et al., 2016; Tibesar et al., 2010; Zellner et al., 2017) Although numerous reports have demonstrated improvement in UAO after MDO for patients with RS, this procedure is associated with several potential complications, including facial nerve dysfunction (FND).
FND can potentially occur during several phases of treatment including original surgical dissection and placement of distractors, active lengthening of the mandible and associated soft tissue during the activation phase, and removal of distractors after a consolidation phase of several weeks. The purpose of the current study is to systematically review the literature for studies and reports of FND associated with MDO. Our goals are to shed light on the current lack of objective data regarding this well acknowledged, but poorly characterized complication, as well as to identify potential risk factors for the development of FND.
Methods
Search Methods
A systematic review of the literature was performed per the Preferred Reporting Items for Systematic Review and Meta Analyses (PRISMA) guidelines, using the following electronic databases: PubMed, Scopus, Web of Science, and Cochrane Library. The search strategy was conducted in June 2019 using MESH terms, or equivalent terms, as follows: “Mandibular distraction,” “Robin sequence,” “Pierre Robin,” and “Pierre Robin sequence”. Our detailed search identified 475 studies, of which 239 were unique (ie, duplicates were removed).
Selection Criteria
Original articles written in English and Spanish, reporting outcomes of MDO in patients with RS, and with documentation of FND were included. Literature reviews, systematic reviews, meta-analyses, letters, book chapters, and small case series (with a sample size of 5 or less), were excluded. Additionally, articles in which the total number of patients was different from the patients with RS were excluded. The screening criteria are outlined in Figure 1.
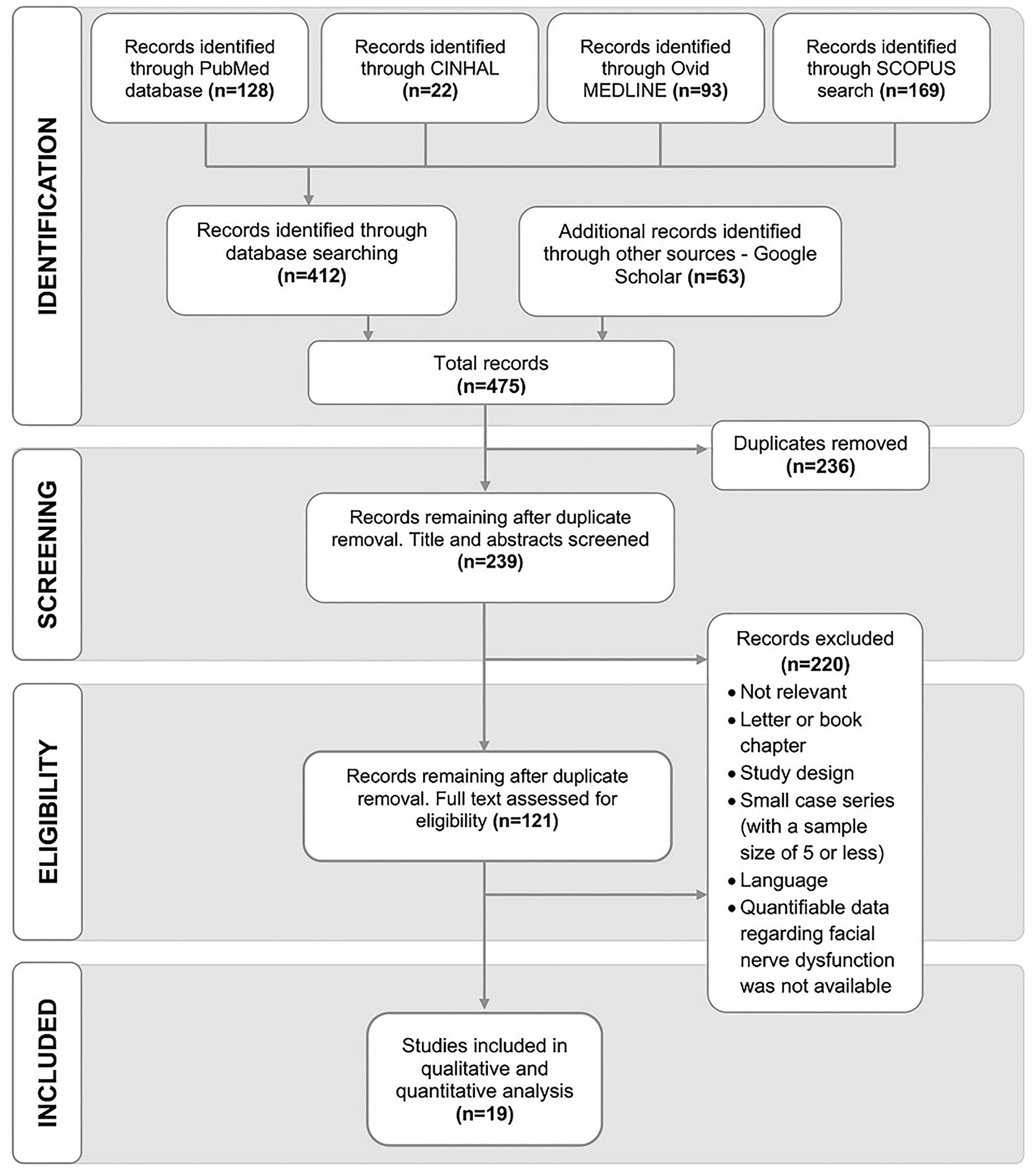
Preferred reporting items for systematic reviews and meta analyses flow diagram, literature search, and selection process.
Data Extraction
Two independent investigators (E.K and M.A) reviewed the articles in a two-step process. Articles were first screened based on abstract and titles (n = 239); second, reviewers performed a full-text evaluation using the inclusion and exclusion criteria (n = 121). All articles with a quantifiable FND (including the absence of FND) after MDO in patients with RS were included (n = 19).
The total number of patients with RS was determined by documentation of micrognathia, glossoptosis, and upper airway obstruction (UAO); alternatively, patients who underwent MDO to treat UAO were also assumed to have RS. Three authors (E.M.R, D.D.B and J.M.E) independently extracted data from each study, covering the following information: authors and year, the number of patients with RS, mean age, syndromic association, prevalence, and timing of FND, affected facial nerve branch, and mandibular distraction protocol. Inconsistencies of extracted data were checked by a fourth author (A.K.O).
Outcomes Measured
The primary variable of measurement was the prevalence of FND. The secondary variables of measurement included the facial branch affected; the rate of permanent versus transient FND, the use of an internal versus external device; the distraction rate per day; and finally, the total average distraction length.
Statistical Analysis
Prevalence of FND was expressed as percentages with 95% confidence intervals, calculated by dividing the number of FND events by the total number of study populations. In the meta-analysis, the prevalence estimates were transformed using the Freeman-Tukey double arcsine transformation to avoid overestimation of the weight of the studies with extreme prevalence (towards either 0% or 100%) (Barendregt et al., 2013). The final pooled results were then back-transformed for interpretation. To account for the between-study heterogeneity, the meta-analysis was performed using a random-effects model to calculate a pooled prevalence from the included studies. The between-study heterogeneity was assessed using the I2 statistic, with values of 25%, 50%, and 75% signifying low, moderate, and substantial heterogeneity, respectively (Higgins et al., 2003). Cochran's Q statistic was used to assess the statistical significance of heterogeneity. The between-study variance was examined using Tau-squared (τ2) which was calculated using the Sidik-Jonkman estimator (Sidik and Jonkman, 2007). Finally, a 95% prediction interval for the pooled prevalence was calculated and plotted. The prediction interval provides an appropriate range in which the prevalence of future studies is expected to fall based on our present evidence in the meta-analysis.
To detect studies that may be overly influential and distort the pooled prevalence estimate, we performed influential analyses using the Leave-One-Out-method, plotting different influence measures (DIFFITS value, Cook's distance, and covariance ratio), and visually inspecting the Baujat diagnostic and plot (Viechtbauer and Cheung, 2010). The Baujat Plot detects studies that contribute excessively to the overall heterogeneity of a meta-analysis (Baujat et al., 2002). Studies were considered outliers if their 95% confidence interval did not overlap with the 95% confidence interval of the pooled estimate. To evaluate the robustness of the result, we conducted sensitivity analyses by excluding studies that were influential and outliers.
Prespecified subgroup analyses were done to investigate whether age category (<6 months vs ≥ 6 months), type of FND (transient vs permanent), type of device (internal vs external vs both), distraction rate (<1.5 mm/day vs ≥1.5 mm/day), and total distraction length (<20 mm vs ≥20 mm) influenced the prevalence estimates. The prevalence estimates of subgroups were compared using a mixed-effects model. Specifically, the random-effects model was implemented within subgroups, and the fixed-effects model between subgroups. Then, the statistical significance of subgroup differences was assessed using the Q statistic. A mixed-effects meta-regression was performed to examine the potential influence of continuous predictors (mean age, distraction rate in mm/day, total distraction length in mm, and sample size of the studies) on the prevalence estimates. We plotted our meta-regression output using bubble plots.
We generated both regular and contour-enhanced funnel plots to investigate small study effects or publication bias. In the presence of publication bias, the funnel would look asymmetrical because small studies with small effect sizes are missing. Furthermore, contour-enhanced funnels contain color coding for the significance level of the effect size of each study and help to distinguish publication bias from other forms of asymmetry (Peters et al., 2008). Egger's test was used to perform a statistical test to quantify the funnel plot asymmetry (Egger et al., 1997). When Egger's test was significant, we used the Trim-and-Fill procedure to estimate the actual prevalence by imputing missing studies into the funnel plot (Duval and Tweedie, 2000). A P-curve analysis was also performed as an alternative way to assess publication bias and estimate the true prevalence (Simonsohn et al., 2014).
All statistical tests were two-sided and performed at 0.05 level of significance. All data was represented graphically with forest plots. Statistical analyses were performed using meta (Balduzzi et al., 2019), metaphor (Viechtbauer and Cheung, 2010), and dmetar (Companion R Package for the Guide Doing Meta-Analysis in R • Dmetar, 2021) packages in R statistical software, version 4.0.0 (R: The R Project for Statistical Computing, 2021).
Results
Search Results
475 studies were returned after the initial search, and 239 studies remained after the removal of duplicate studies. Ultimately, after applying selection criteria, a total of 19 studies were included in the final meta-analysis. A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) screening process flow diagram is documented in Figure 1.
Study Characteristics
Across all 19 studies, 729 patients with RS were enrolled, among whom FND was documented in 52 patients. The number of patients per study ranged from 9 to 123 (median: 22 [IQR: 14, 51]; mean: 38.4). The prevalence of FND ranged from 0% to 22.22%. Mean study population ages ranged from 1.1 months to 30 months (median of mean age: 3.1 months [IQR: 2.0, 11.4]). Mean follow-up for the studies that documented this data was 48.76 months (range 1−192 months). Nine studies reported transient FND (Frawley et al., 2013; Goldstein et al., 2015; Lam et al., 2014; Lin et al., 2007; Mahrous Mohamed et al., 2011; Murage et al., 2014; Zellner et al., 2017) and 6 studies reported permanent FND (Konaş et al., 2016; Scott et al., 2011; Senders et al., 2010; Steinberg et al., 2016; Tahiri et al., 2015; Tibesar et al., 2010) while 1 study had both types of FND (Mudd et al., 2012); 1 study explicitly reported no FND in their cohort of patients (Martín-Masot et al., 2018); and 2 studies documented FND without noting the duration of palsy (Allam et al., 2011; Mao et al., 2019). Ten of 19 publications (47.4%) documented marginal mandibular branch (MMB) dysfunction (Allam et al., 2011; Frawley et al., 2013; Konaş et al., 2016; Lin et al., 2007; Mahrous Mohamed et al., 2011; Scott et al., 2011; Senders et al., 2010; Steinberg et al., 2016; Tibesar et al., 2010; Zellner et al., 2017), and 9 studies did not document which branch of the facial nerve was injured.
Eight studies used internal devices (Allam et al., 2011; Frawley et al., 2013; Goldstein et al., 2015; Hammoudeh et al., 2012; Mahrous Mohamed et al., 2011; Murage et al., 2014; Steinberg et al., 2016), 3 used external devices (Scott et al., 2011; Senders et al., 2010; Tibesar et al., 2010), and 2 studies used both types of device (Lin et al., 2007; Martín-Masot et al., 2018); 6 studies did not document the type of device (Hu et al., 2001; Lam et al., 2014; Mao et al., 2019; Murage et al., 2014; Zellner et al., 2017). Distraction rate ranged from 1.00 mm/day to 2.00 mm/day (median: 1.00 mm/day, mean 1.37 mm/day) and the total distraction length ranged from 13.00 mm to 22.3 mm (median: 18.1 mm, mean 18.5 mm). Furthermore, study designs varied. Eight studies were retrospective (Frawley et al., 2013; Goldstein et al., 2015; Hammoudeh et al., 2012; Hu et al., 2001; Lam et al., 2014; Mahrous Mohamed et al., 2011; Mao et al., 2019; Murage et al., 2014), 5 were cohort retrospective (Konaş et al., 2016; Scott et al., 2011; Senders et al., 2010; Steinberg et al., 2016; Tibesar et al., 2010), 2 were case series (Lin et al., 2007; Mudd et al., 2012), and the remaining 4 studies were case control (Tahiri et al., 2015), retrospective case control (Zellner et al., 2017), observational descriptive (Martín-Masot et al., 2018), and combined retrospective and prospective (Allam et al., 2011).
Meta-Analysis of Prevalence
A random-effects meta-analysis of the results revealed an overall pooled prevalence of FND of 6.40% (95% CI: 3.76%, 9.53%; 19 studies, 729 participants). Moderate heterogeneity existed between studies (I2 = 41%, τ2 = 0.006) which was significant by Cochran's Q statistic (Q = 30.67; P = 0.03). The overall 95% prediction interval of the pooled prevalence was 0.06% to 18.46% (Figure 2a). No outlier study was detected whose 95% confidence interval range fell outside of the 95% confidence interval range of the pooled estimate. However, in the influential analyses, a single study by Tahiri and colleagues was found to be overly influential (Supplemental Figure 1), and this study accounted for almost all of the between-study heterogeneity (Tahiri et al., 2015). We performed a sensitivity analysis after removing this study. After excluding the Tahiri et al., 2015 study from the meta-analysis, the overall pooled prevalence estimate was 7.36% (95% CI: 4.88%, 10.20%; 18 studies, 608 participants). Between-study heterogeneity (I2) decreased from 41% to 0% and the P value of Cochran's Q statistic became non-significant (from 0.03 to 0.57) (Figure 2b).
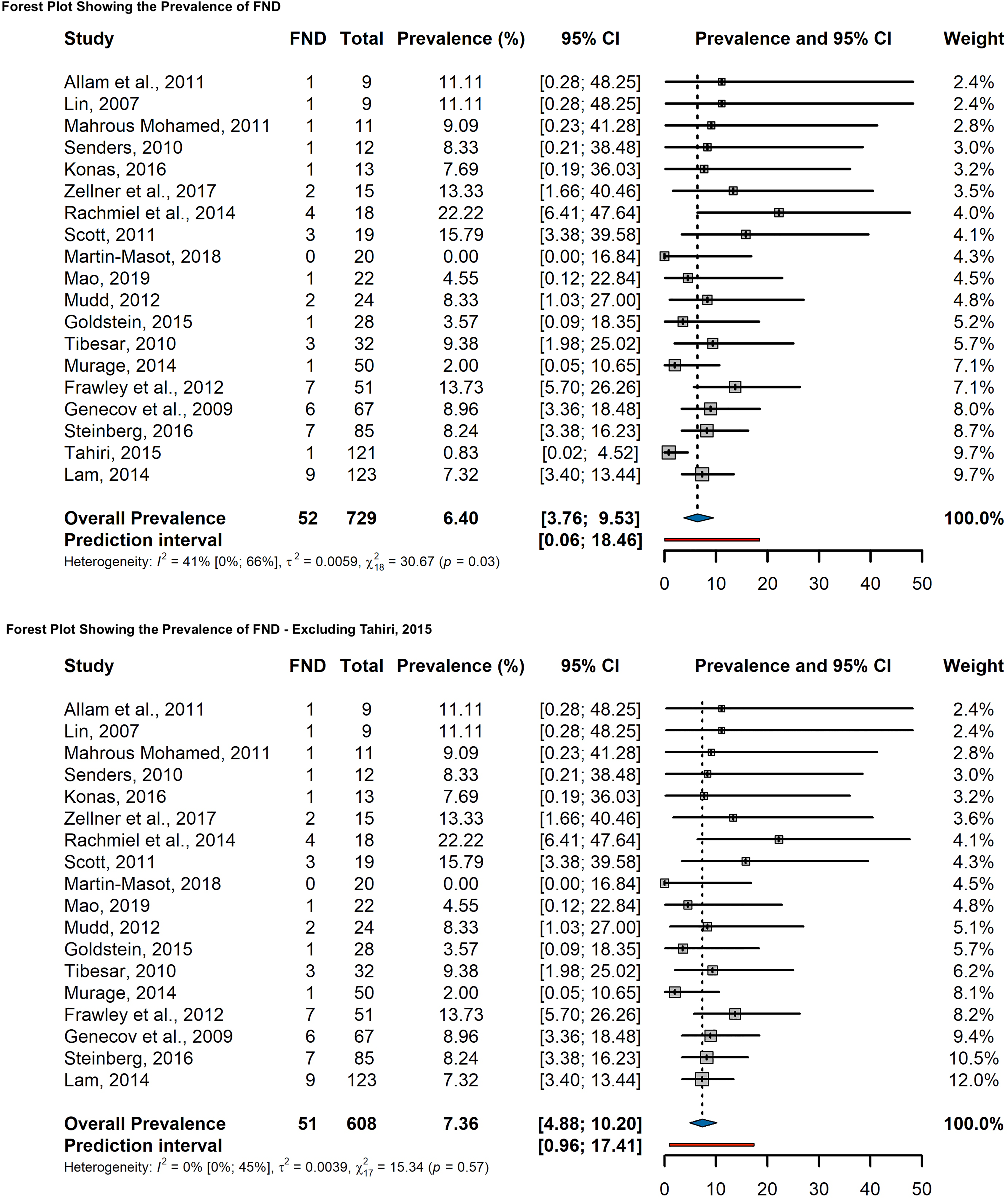
A) random effects model forest plot showing the prevalence (%) of FND with 95% confidence interval. B) Random effects model forest plot showing the prevalence (%) of FND with 95% confidence interval excluding the overly influential study (Tahiri et al., 2015).
Subgroup Analysis and Meta-Regression
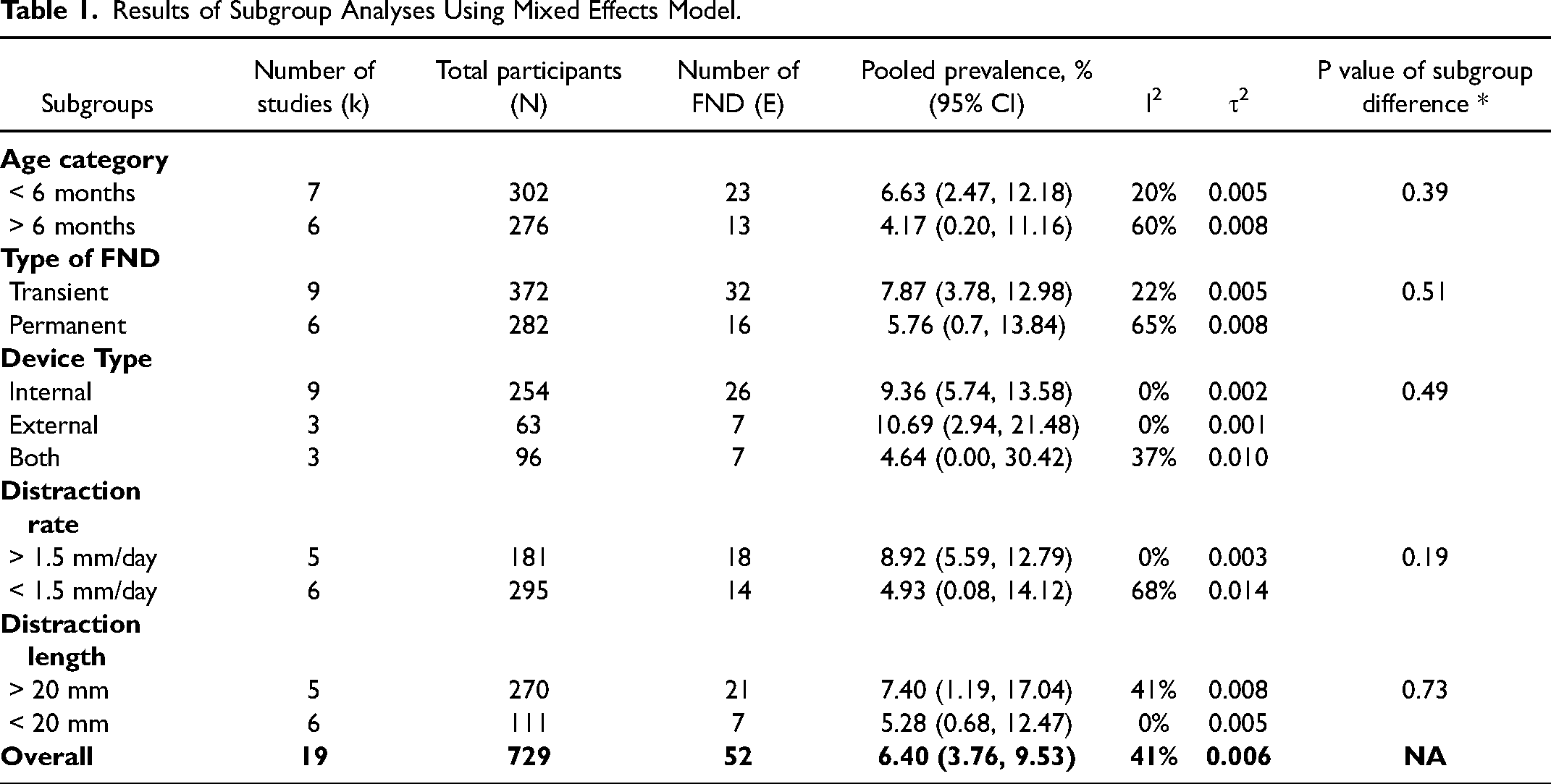
We conducted several prespecified subgroup analyses based on age category (<6 months vs ≥6 months), type of FND (transient vs permanent), type of device (internal vs external vs both), distraction rate (<1.5 mm/day vs ≥1.5 mm/day), and total distraction length (<20 mm vs ≥20 mm). However, the pooled prevalence of FND did not differ significantly across subgroups. A detailed comparison of various subgroups is in Table 1. Forest plots of these subgroup analyses were provided in the supplemental Figures 2 to 6.
Results of Subgroup Analyses Using Mixed Effects Model.
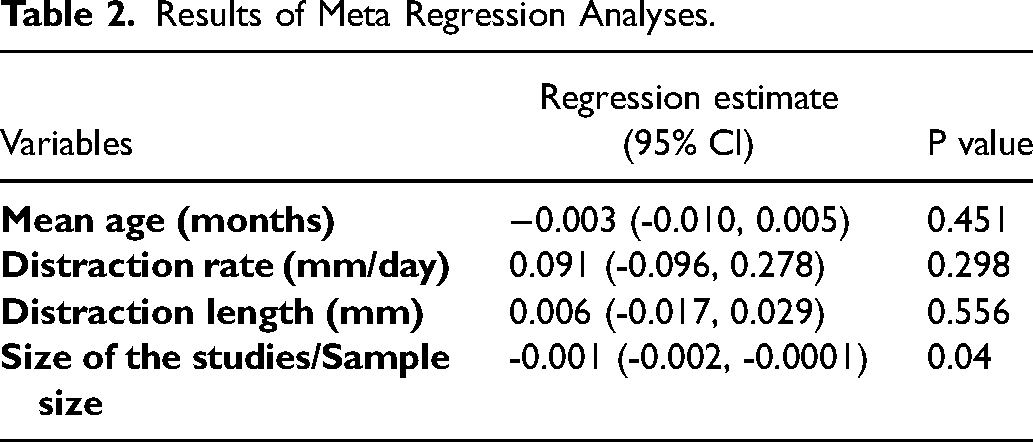
We also performed mixed-effects meta-regression analyses to examine the potential influence of continuous predictors (mean age, distraction rate, total distraction length, and study sample size) on prevalence estimates. However, none of these variables were associated with the increased prevalence of FND except for the size of the studies. The size of the study (sample size) was inversely associated with the prevalence of FND (P = 0.040). The results of meta-regression analysis were presented in Table 2 and shown in Figure 3 using bubble plots.
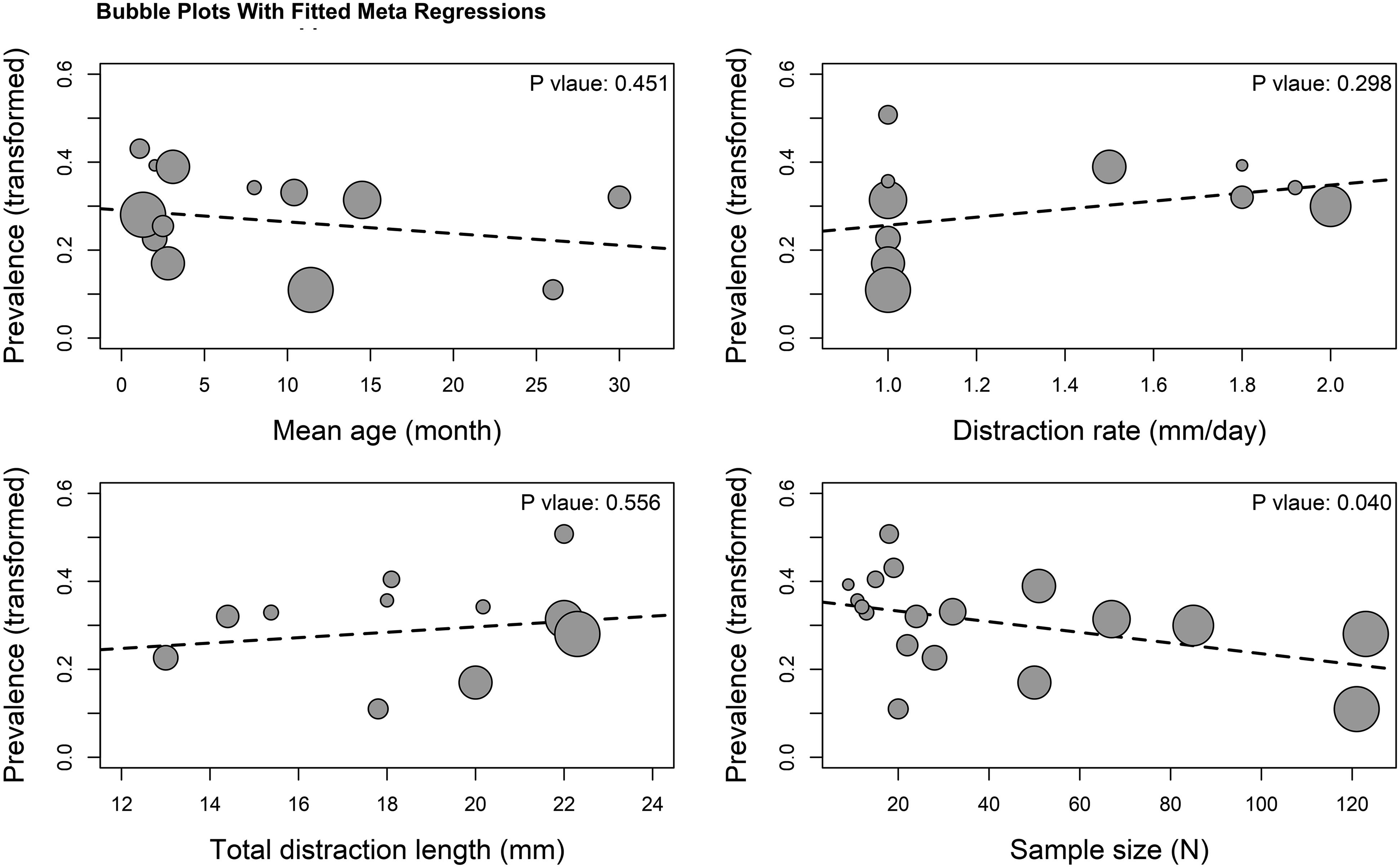
Bubble plots with fitted meta regressions line of the double arcsine transformed prevalence of FND on mean age, distraction rate, total distraction length, and size of the studies.
Results of Meta Regression Analyses.
Publication Bias
No substantial funnel plot asymmetry was observed (Figure 4). Although some studies appeared to be missing in the lower left quadrant of the funnel plot, the asymmetry was not conspicuous enough to be suggestive of publication bias or small study effect. The Egger's test also indicated that there was no significant publication bias (intercept: 0.73, 95% CI: −0.40 to 1.87, P = 0.22). From the counter-enhanced funnel plot, only Martin-Masot 2018 (Martín-Masot et al., 2018), had a non-significant prevalence estimate (white background) while the remaining 18 studies had a statistically significant (P < 0.05) prevalence estimate of FND (grey background). No trend was observed between study size and statistical significance. A P-curve analysis was also performed to investigate the possible bias arising from P-hacking (ie, manipulation of data and analysis to achieve a statistically significant result). Our analysis did not find any evidence of such bias. The curve analysis estimated that the power of our meta-analysis was 90% (78.9% to 96.0%).
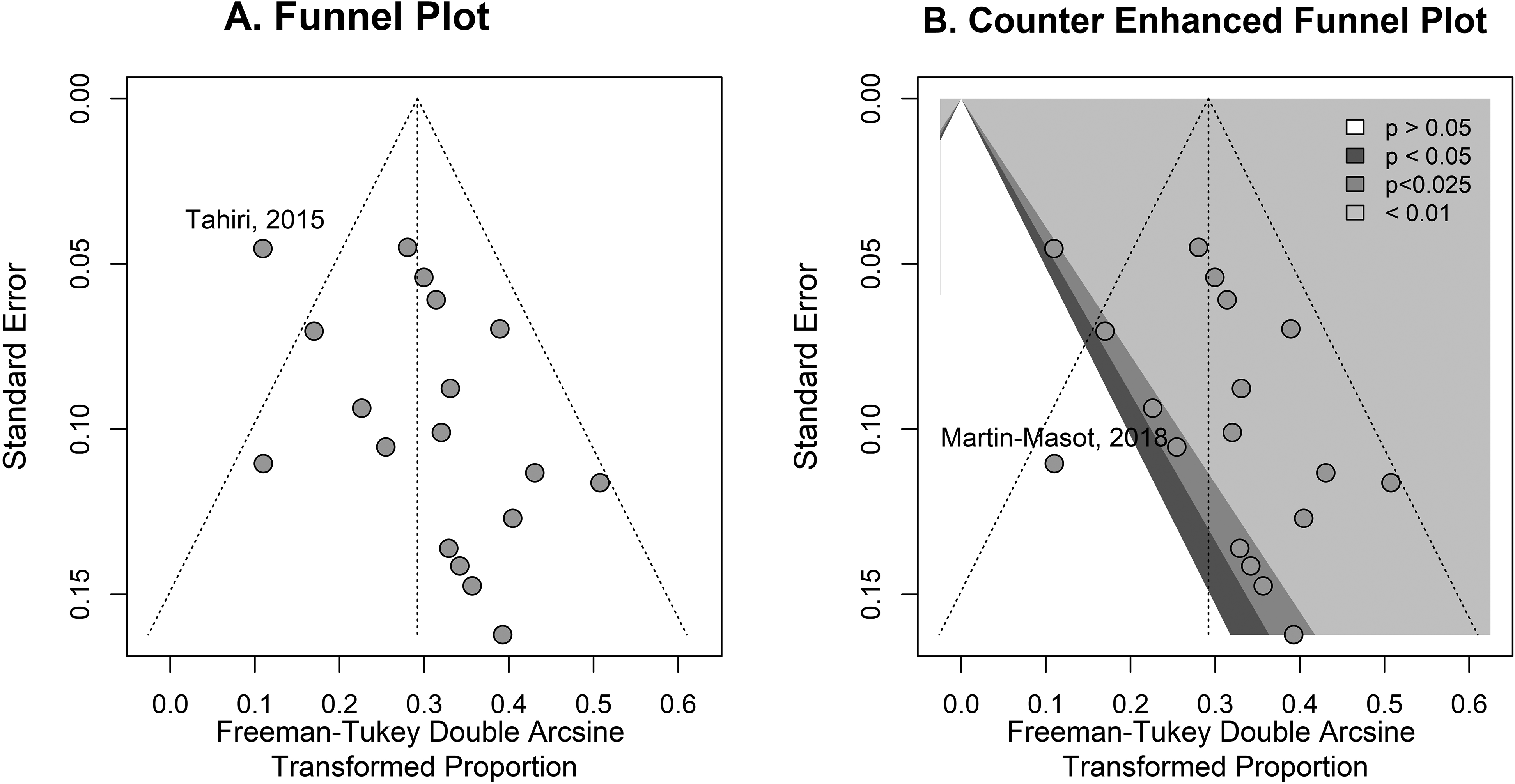
Funnel plot (A) and contour enhanced funnel plot (B) to examine publication bias.
Discussion
Facial neuropraxia has been a recognized complication of mandibular distraction since McCarthy’s landmark studies over 40 years ago (McCarthy et al., 1992). As MDO has become an integral part of the surgical algorithm for Robin sequence, the potential long-term complications for these neonates should be elucidated to adequately counsel families. While large-scale studies on MDO outcomes have been reported, there is marked variation in the methodology and documentation, particularly in regards to FND.
Prevalence of FND after MDO has varied in numerous studies, due, in part, to inconsistent reporting. In 2016, Breik et al., conducted a systematic review of 124 studies and reported FND incidence rate as 4.7%, but long-term follow-up was not done and the injured FN branch was not specifically reported (Breik et al., 2016). Kapadia and colleagues presented a pediatric case of nerve paralysis after MDO, as well as a review of similar cases in the literature, but only 6 studies were reported (Kapadia et al., 2013). Mao and associates reported complications for two groups undergoing MDO, one control group and one group with 3D remodeling guidance; “nerve injury” and “facial asymmetric deformities” were both listed as complications; the authors did not specify a difference, nor did they provide information on the temporality or locality of nerve damage (Mao et al., 2019).
Clarifying the type of nerve dysfunction is important in accurately documenting surgical outcomes. “Nerve injury” may refer to direct nerve trauma, stretch secondary to surgical retraction, or intraoperative edema secondary to nerve manipulation. Damage appears to commonly involve either the marginal mandibular branch of the facial nerve. Furthermore, lack of specific information regarding the timing of FND introduces the question of whether the surgical procedure itself or postoperative distraction resulted in nerve dysfunction, and if any predisposing factors, such as congenital subclinical weakness of the FN (eg, craniofacial macrosomia or Moebius syndrome), are potential confounding variables (Mandell et al., 2004).
If traction is indeed the injurious action, then it may logically follow that the severity of micrognathia and the length of necessary distraction would also be predisposing factors for FND. In fact, encouraging adequate axonal growth along extensive distances can be quite difficult, particularly in instances of high nerve tension (ie, active stretch). The pathologic changes include demyelination, axonal swelling, axoplasmic darkening, and axonal density reduction (Hu et al., 2001; Smith, 2009). These nerve microenvironments may be “non-permissive” for axonal growth. Our meta-analysis did not identify an association between length of distraction and risk of FND, although the nonspecific and incomplete documentation of these data may be perhaps to blame.
Palsy duration may also provide insight into the mechanism of MDO-associated FND. Scott and colleagues documented the temporality of the FND observed among their patients, hypothesizing that transient FND is more likely to be from stretch injury during distraction, while permanent FND may be due to direct nerve trauma during surgery or from external device pin placement (Scott et al., 2011). The current meta-analysis was unable to find any correlation between the duration of FND and time of diagnosis (eg, FND documented immediately following device placement/osteotomies vs during active distraction). Future studies that record temporality of the nerve dysfunction along with surgical technique and device type may aid in elucidating the mechanism of temporary versus long-term FND. Such data is potentially critical, as some authors have commented that FND was not likely to decrease patients’ quality of life, most likely due to its transient nature (Scott et al., 2011). While we found a majority of cases in the literature to indeed be cases of transient FND, there are documented cases of permanent FND, which can have profound clinical consequences.
Ultimately, very few studies utilize uniform screening and clinical assessment tools to identify and document FND. Only one study by Steinberg and colleagues commented on a specific modality used to detect FND (1,1,1,2-tetrafluoroethane cold stimulation and photography and videography) which assessed the function of the inferior alveolar nerve and marginal mandibular branch of the facial nerve, respectively (Steinberg et al., 2016). Our analysis underscores the need for more systematic and complete descriptions in studies of MDO for patients with RS to identify the etiology of FND.
Limitations
Systematic reviews rely on data reporting of other researchers and thus have the potential to replicate biased results from flawed studies. Furthermore, no randomized control trials with control groups were found, which generally have less bias, unlike smaller clinical case series and case reports which often contain publication bias. Although no statistical evidence of publication bias was found in our analysis, there are certainly biases against reporting of any surgical complications that occur in clinical practice. Intuitively, therefore, the incidence of FND associated with MDO is likely higher than rates reported in the literature.
Conclusions
Facial nerve dysfunction following neonatal MDO for RS occurs with notable frequency and is occasionally permanent. Though the marginal mandibular branch of the facial nerve is at highest risk due to its location within the surgical field and proximity to the distraction hardware, other branches, as well as the main facial nerve trunk are also at risk for both transient as well as permanent dysfunction. A lack of details regarding such important complications limits our ability to report a true incidence or identify risk factors for FND, and more granular details of these complications should be included in future investigations.
Financial Disclosure:
The authors have nothing to disclose.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656211070728 - Supplemental material for Facial Nerve Dysfunction After Mandibular Distraction Osteogenesis in Patients with Robin Sequence: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-cpc-10.1177_10556656211070728 for Facial Nerve Dysfunction After Mandibular Distraction Osteogenesis in Patients with Robin Sequence: A Systematic Review and Meta-Analysis by Elina Kapoor, Esperanza Mantilla-Rivas, Md Sohel Rana, Marudeen Aivaz, Daniela Duarte-Bateman, Joseph M. Escandón, Hannah R. Crowder, Monica Manrique, Gary F. Rogers and Albert K. Oh in The Cleft Palate-Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.