
Abstract
Objective:
To determine whether orthodontically treated patients with cleft lip and palate (CLP) possess a different masticatory function than those of untreated patients with normal occlusion.
Design:
Occlusal contact area, occlusal force, as well as masseter and anterior temporal muscular activity were measured during maximum voluntary clenching (MVC) tests. Mandibular left and right lateral movements during mastication were also assessed. To further elucidate the nature of masticatory function, especially to determine the rate of abnormal jaw movement patterns, a parametric error index (EI) was set. Finally, masticatory efficiency was evaluated with a glucose sensitive measuring device.
Participants:
Fifteen patients with CLP who had previously completed the orthodontic treatments required to achieve an acceptable and more harmonious occlusion accepted to volunteer in this study along with 21 untreated patients who already possessed a normal occlusion.
Results:
Patients with CLP showed a significantly lower occlusal force, reduced occlusal contact area, and decreased masticatory efficiency as well as significantly higher EI value when compared with controls. However, there was no significant difference when analyzing muscle activity, although masticatory efficiency was significantly different between the 2 groups. Despite this result, the scores obtained by the patients with CLP in the masticatory efficiency tests were still in the normal range.
Conclusions:
Orthodontic treatment for adult patients with CLP provides a satisfactory result for the patients’ masticatory ability albeit significantly less ideal compared with untreated patients with normal occlusion.
Introduction
Patients with cleft lip and palate (CLP) show several congenital morphological and functional disorders (Proffit et al., 1986; Trindade-Suedam et al., 2012). They also exhibit various disorders of stomatognathic function, such as masticatory dysfunction, breathing disorders, and speech problems (Sipert et al., 2008; Hortis-Dzierzbicka et al., 2014; Tan et al., 2016). Therefore, patients with CLP who undergo orthodontic treatment may have divergent expectations about both morphological and functional improvement (Ireland et al., 2014). The characteristics of masticatory function, in terms of muscle activity, bite force, mandibular movement, and occlusal contacts, have been well-documented to allow for examination of the related functional problems (Dean et al., 1992; Tate et al., 1994; Throckmorton et al., 1996; de Abreu et al., 2014; Takeshima et al., 2019). In these studies, various methods were used to evaluate masticatory function because there is no single method that can provide an optimal assessment. The stomatognathic system is a physiological and functional entity consisting of a set of organs and tissues, of which the biology and physiopathology are completely interdependent. Thus, masticatory function is primarily dependent on the temporomandibular joint, masticatory muscles, and dentofacial structures (Bakke, 1993; Hatch et al., 2001).
Several previous studies have attempted to assess the masticatory function in children with CLP by comparing it with that in children with normal dentition (Garcia et al., 2016; Szyszka-Sommerfeld et al., 2018). Since scar formation after surgery on the upper lip and palate may cause anterior/posterior crossbite, children with CLP fail to achieve sufficiently satisfactory masticatory function (Montes et al., 2018). On the other hand, very limited information is available for the functional status in adult patients with CLP, as stated in a study by Sipert et al. (2008), which was performed during and after orthodontic treatment, and even in patients with no previous orthodontic treatment. A thorough understanding of the direct association of CLP with the functioning of the stomatognathic system is essential to estimate the appropriate orthodontic treatment plan for each affected individual. The aim of this study was to confirm the hypothesis that patients with CLP, after orthodontic malocclusion correction, would possess a masticatory function similar to untreated control participants without CLP by recording several aspects of masticatory function, including occlusal force, occlusal contact area, muscle activities, jaw movement, and masticatory efficiency in patients with CLP and those with normal occlusion, and comparing said findings.
Material and Methods
Patients
This study included 15 adult patients (7 males and 8 females; mean age, 29.3 ± 8.4 years) who were diagnosed with CLP (12 unilateral [7 on the right side, 5 left side] and 3 bilateral) at Hiroshima University Hospital, these patients underwent orthodontic treatment with multibracket appliance and had to have finished said treatment and already in the retention stage to be included in this study. After careful assessment of post-orthodontic treatment and/or prosthodontic treatment on both unilateral and bilateral patients with CLP, taking into consideration treatment outcomes including final dentition and occlusion, it was deemed that the differences were not as big as to merit excluding patients with bilateral CLP from this study. The orthodontic treatments for patients with CLP were performed by veteran orthodontists who all have been well trained at the institution. Patients who were scheduled to undergo orthognathic surgery, had temporomandibular joint disorders, experienced pain or discomfort during the examination, or had complications from serious systemic disease were excluded.
The control group consisted of 21 healthy adults (12 males and 9 females; mean age, 25.5 ± 2.1 years). Participants in the control group had Angle Class I molar relationship, no severe malocclusion, no complaints of temporomandibular joint disorders, no history of bruxism, and no previous experience of orthodontic treatment. Information regarding the number of teeth and the dentoskeletal relationships of the patients in this study is summarized in Table 1. This study was conducted from March 2018 to April 2020, with data from patients with CLP already in the orthodontic retention period (mean retention period 8.3 ± 6.3years).
Comparison of CLP Group and Control Group.

Abbreviation: CLP, cleft lip and palate.
Assessment of Orthodontic Treatment
Study casts obtained during the post-orthodontic retention period were quantitatively scored by using the objective grading system (OGS) of The American Board of Orthodontics (ABO). Eight measurements (alignment, marginal ridges, buccolingual inclination, occlusal relationships, occlusal contacts, overjet, interproximal contacts, and root angulation) were obtained for each patient with the ABO gauge, and points were deducted for any discrepancy from the ideal as described by the ABO guidelines (Casko et al., 1998). The number of points lost was totaled to obtain the OGS score. Loss of 30 or fewer points was generally considered to indicate a successful treatment. All study casts were assessed with measurements taken twice with at least 2 weeks in between to check for inconsistencies and evaluator errors by the first author. Besides this, intraclass correlation coefficient reliability test was performed with a result of 0.86, meaning a good reliability has been achieved when measuring the dental casts.
Occlusal Contact Area and Occlusal Force
Maximum occlusal contact area and occlusal force were measured using a pressure-sensitive occlusal force measurement film (Dental Prescale II System [GC]) consisting of pressure-sensitive sheets and analyzed with its proprietary software (Bite Force Analyzer ver. 1.0.1, 2018, GC; Figure 1A). The Dental Prescale II responds to pressure with a color-developing chemical reaction. The amount of occlusal pressure and the size of the occlusal contact can be estimated by measuring the density and area with a color image scanner. The occlusal force can be calculated from the occlusal pressure and the size of the occlusal contact area. Before recording, each patient was seated in the upright position and instructed to bite properly to exert and produce the maximum voluntary clenching (MVC). The Dental Prescale II measurement sheet was placed between the upper and lower dentitions, and patients were instructed to bite the sheet in the intercuspal position for 3 seconds.
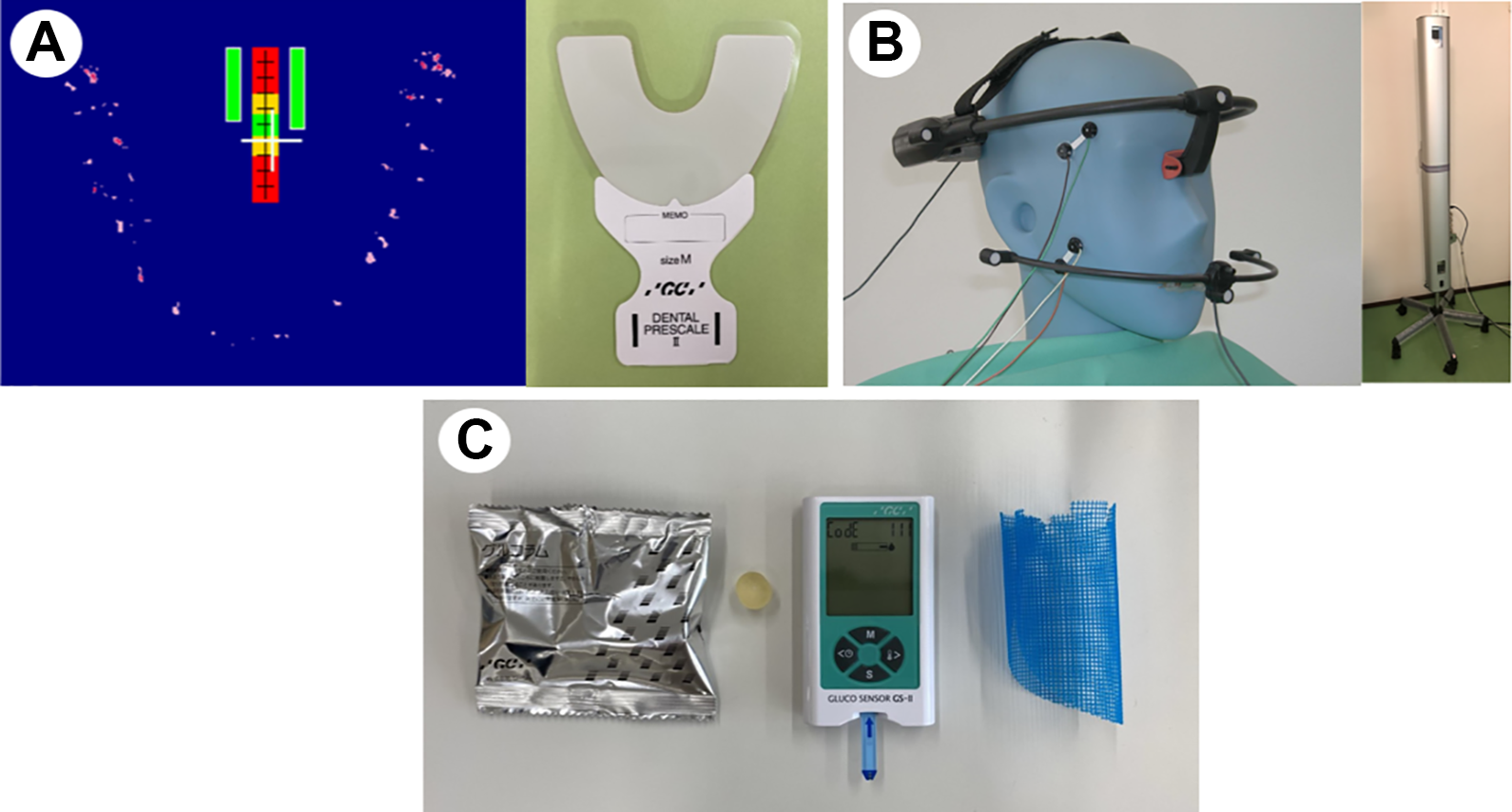
A, An occlusal force measurement system (dental prescale II). B, A 6-degree-of-freedom optoelectric mandibular motion recording system (GNATHO-HEXAGRAPH III) and electromyography (EMG) electrodes. C, A masticatory efficiency measurement system (gluco sensor set).
Measurements of Muscle Activity and Jaw Movement
Muscle activity and jaw movement were recorded simultaneously in all tasks. Both masseter and anterior temporal muscle activities were recorded bilaterally using a silver/silver chloride surface electrode (Figure 1B).
The maximum size of the muscle bellies was determined by palpation, and the electrodes were applied parallel to the muscle fibers. Before placing the electrodes, the skin was scrubbed with an alcohol-soaked gauze pad to reduce the impedance between skin and electrodes. The electromyography (EMG) signals were amplified and recorded by electrical pulses. The parameters at this time were 2 KHz or higher for the high-cut filter and 20 Hz or lower for the low-cut filter. Averages of EMG data were stored in a data recorder (Neuropack S1; Nihon Kohden).
Electromyography was recorded during the 5-s MVC with the teeth in the maximum intercuspal position. The patients were instructed to clench with maximum effort 3 times with an interval of 10 s. The integrated value of muscle activity was calculated during the median 3 seconds of the 5-s MVC.
Jaw movement was analyzed using a 6-degree-of-freedom optoelectric mandibular motion recording system, which consists of a headframe, a facebow, light emitting diodes (LEDs; Gnatho-Hexagraph III, JM-3000; GC), charge-coupled device (CCD) cameras, and a personal computer (Nakata et al., 2007; Sato et al., 2007; Komori et al., 2013; Figure 1B). A headframe with 3 LEDs was placed on the head parallel to the Frankfort horizontal plane of the patient, and a facebow was set to the mandible using a dental clutch. The dental clutch was attached to the labial surface of the lower anterior teeth by means of cyanoacrylate adhesive. Each patient was seated on a chair in an upright but relaxed position without a head support. Two CCD cameras were placed in front of the patient. The position of each LED was determined 3-dimensionally according to the parallax principle. The center point between the right and left lower central incisors was recorded using a pointer with 2 LEDs and calculated based on the respective 3-dimensional positions of 6 LEDs attached to the headframe and facebow recorded by the pointer.
Movement of the incisal point was recorded over 50 seconds of chewing gum with natural mastication movements. All the chewing strokes on the working side during unilateral gum chewing were classified into several specific patterns: normal chewing pattern, crossover type, and reverse type. The latter 2 types are regarded as abnormal chewing patterns.
The error index (EI) was used to investigate the patients’ patterns of jaw movement (Nakata et al., 2007). During unilateral gum chewing, the total number of abnormal chewing patterns on the working side was calculated. Subsequently, EI was calculated as the ratio of the number of strokes showing an abnormal chewing trajectory to the total chewing strokes, as shown in the following equation:

Here, EI indicates the rate of the abnormal jaw movement pattern.
Evaluation of Masticatory Efficiency
Masticatory efficiency was assessed on the basis of the concentration of dissolved glucose after chewing a ready-made gummy jelly. After rinsing the patient’s mouth with water, a gummy jelly containing 5% glucose (diameter, 15 mm; height, 8 mm) was placed on the tongue. The participants were instructed to chew the gummy jelly on their habitual chewing side for 20 seconds without swallowing. After chewing, the participants were asked to take 10 mL of distilled water in their mouth and to spit out the gummy jelly, distilled water, and saliva into a filter cup. The glucose concentration (mg/dL) in the filter cup was measured using the Glucose Sensor Set (Gluco Sensor GS-II, GC; Figure 1C). The measured concentration of glucose was used as an indicator of masticatory efficiency (Takeshima et al., 2019).
Statistical Analysis
The collected research data consisted of data from 12 patients with unilateral CLP for analysis of muscle activity during MVC with comparison between the cleft and noncleft sides. For evaluation of occlusal contact area and force by the Dental Prescale II System, the data for all patients with unilateral and bilateral CLP were analyzed separately for males and females. When no significant differences were observed between cleft and noncleft sides, we calculated the total occlusal contact area and force on the dentition to compare patients with CLP and controls. For evaluation of jaw movement and masticatory efficiency, since no sex-related differences were found, the data for all 15 male and female participants with both unilateral and bilateral CLP were statistically analyzed. To examine the correlation between masticatory efficiency and other masticatory functions, Pearson correlation test was employed. All masticatory function tests were performed 3 times each, and the average value of these 3 times was used as the measured value. All tests, measurements, and all data were performed, collected, and analyzed by the first author.
All statistical analyses were performed with the Statcel 3 software (OMS Publisher, 2011). The Kruskal-Wallis test was used to determine significant differences among 3 groups (cleft side, noncleft side, and control), whereas the Mann-Whitney U test was used for comparisons of 2 groups (CLP and control groups).
Results
Outcomes of the Orthodontic Treatment
The mean OGS score after orthodontic treatment for the patients with CLP was 25.5 ± 6.2. According to the ABO, a case can lose only 30 or fewer points to receive a passing grade.
Examiner reliability was analyzed by obtaining repeated measurements in all cases after data collection. No statistically significant differences (P < .05) were found between any of the initial measurements and the second measurements of the OGS categories.
Assessment of Masticatory Function
The patients with CLP demonstrated no major differences in the occlusal contact and occlusal force between the cleft and noncleft sides (Figure 2A and C). In addition to this, the total occlusal contact area in males and females was significantly (P < .05) smaller in the patients with CLP than in the controls (Figure 2B). Similarly, the total occlusal force during MVC was significantly (P < .05) smaller in the patients with CLP than in controls in males (Figure 2D).
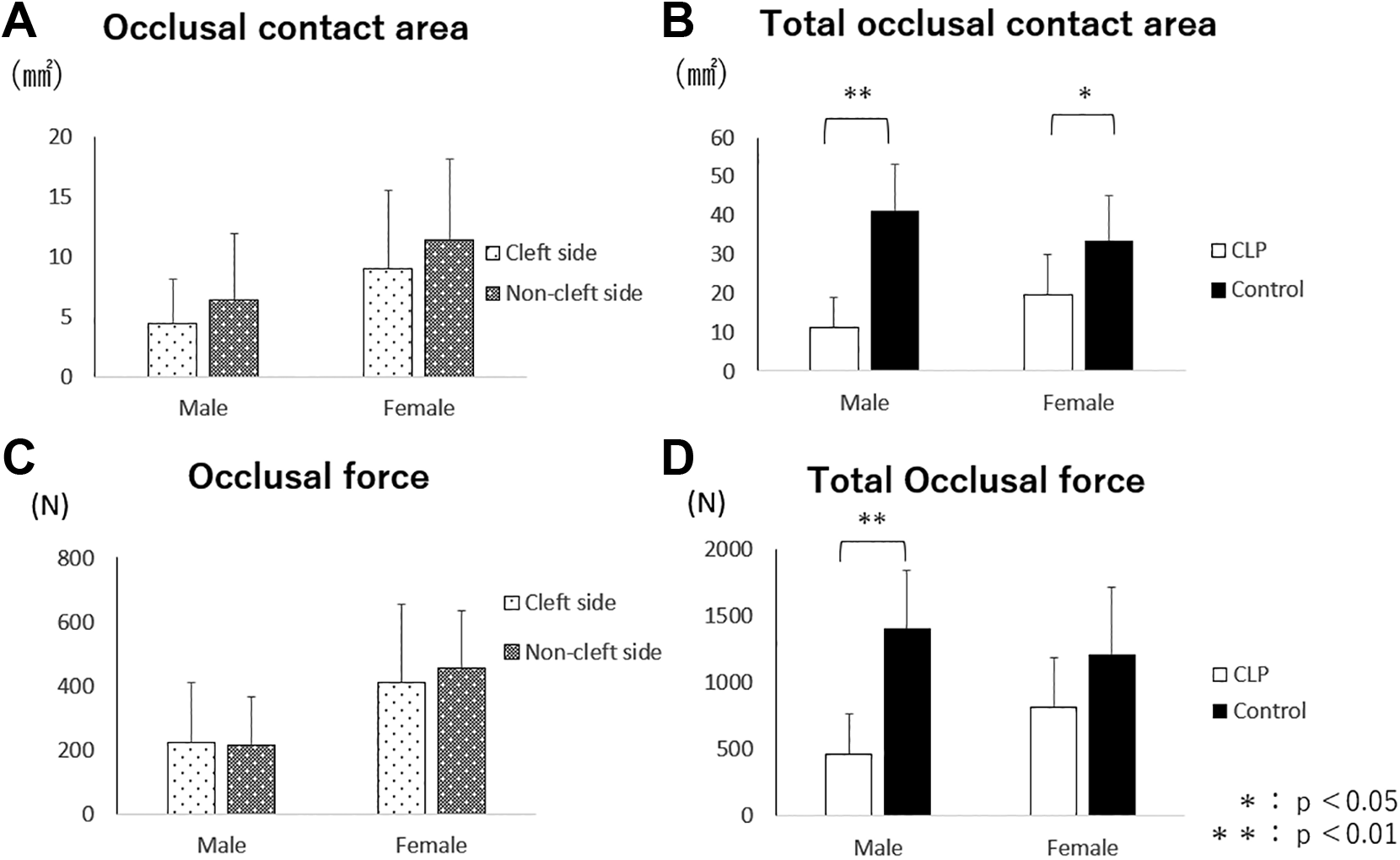
A, Comparison of the occlusal contact area between cleft and noncleft sides in males and females. B, Comparison of total occlusal contact area between patients with cleft lip and palate (CLP) and controls. C, Comparison of occlusal force between cleft and noncleft sides in males and females. D, Comparison of total occlusal force between patients with CLP and controls.
When evaluating the masseter muscle, muscle activity during MVC on the cleft side was lower than that on the noncleft side in males and females. In comparison with the controls, masseter muscle activity on the cleft side in males and females was lower than the average value of the right and left sides in the controls (Figure 3).
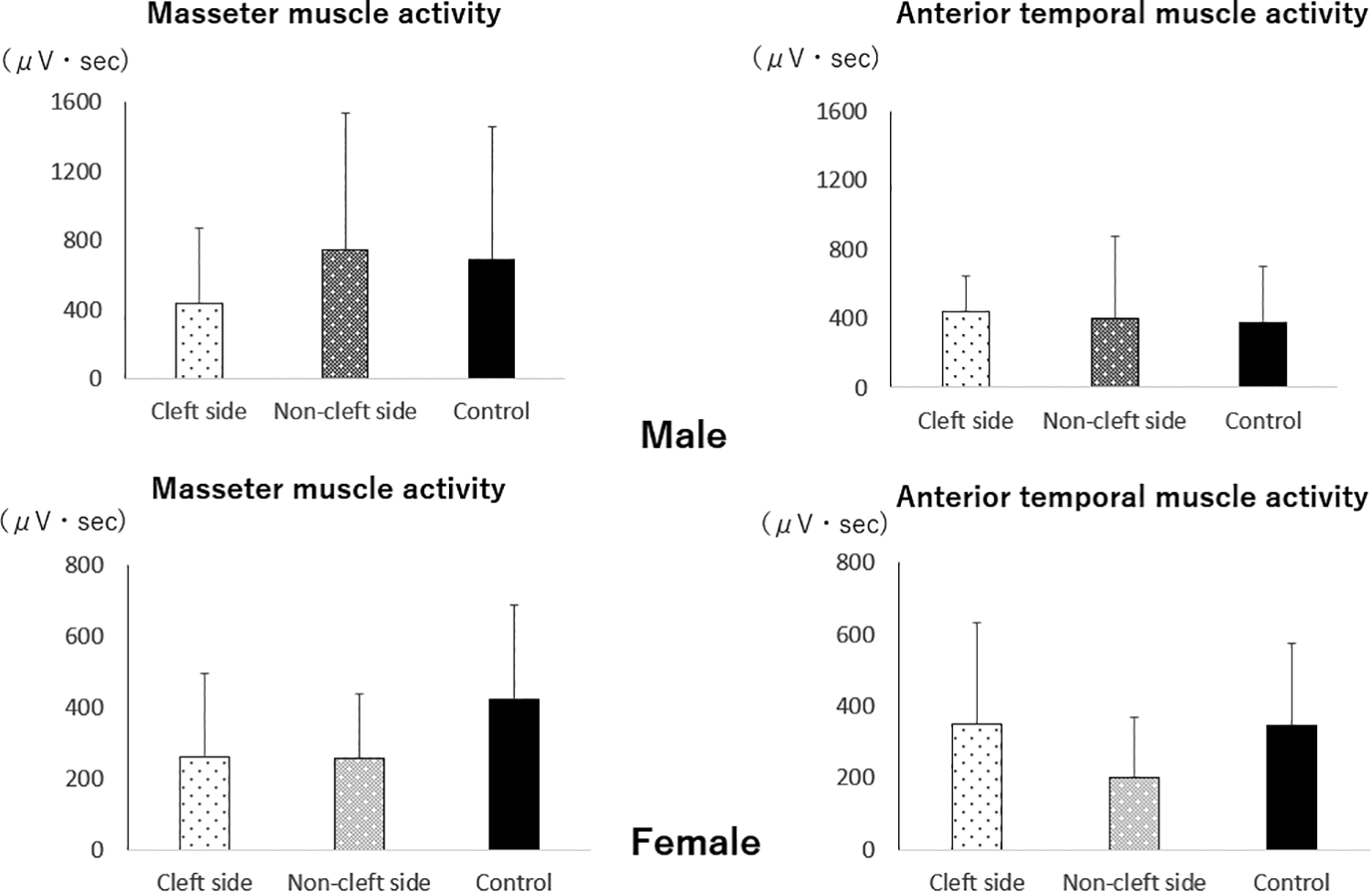
Comparison of masseter and anterior temporal muscle activity during MVC in the cleft and noncleft sides and average of right and left sides in controls in males and females.
However, no significant differences were found, although both values on the cleft side were approximately 60% of that in the controls. On the other hand, anterior temporal muscle activity showed no considerable difference between the cleft and noncleft sides in males and females, and no significant difference in comparison with the controls in both sexes (Figure 3).
The EI value was 0.61 ± 0.24 and 0.51 ± 0.27 while chewing on the right and left sides in the patients with CLP, respectively. In contrast, the EI value was 0.24 ± 0.27 (right side chewing) and 0.20 ± 0.23 (left side chewing) in the controls. The EI values were significantly (P < .01) larger in the patients with CLP than in the controls (Figure 4A).
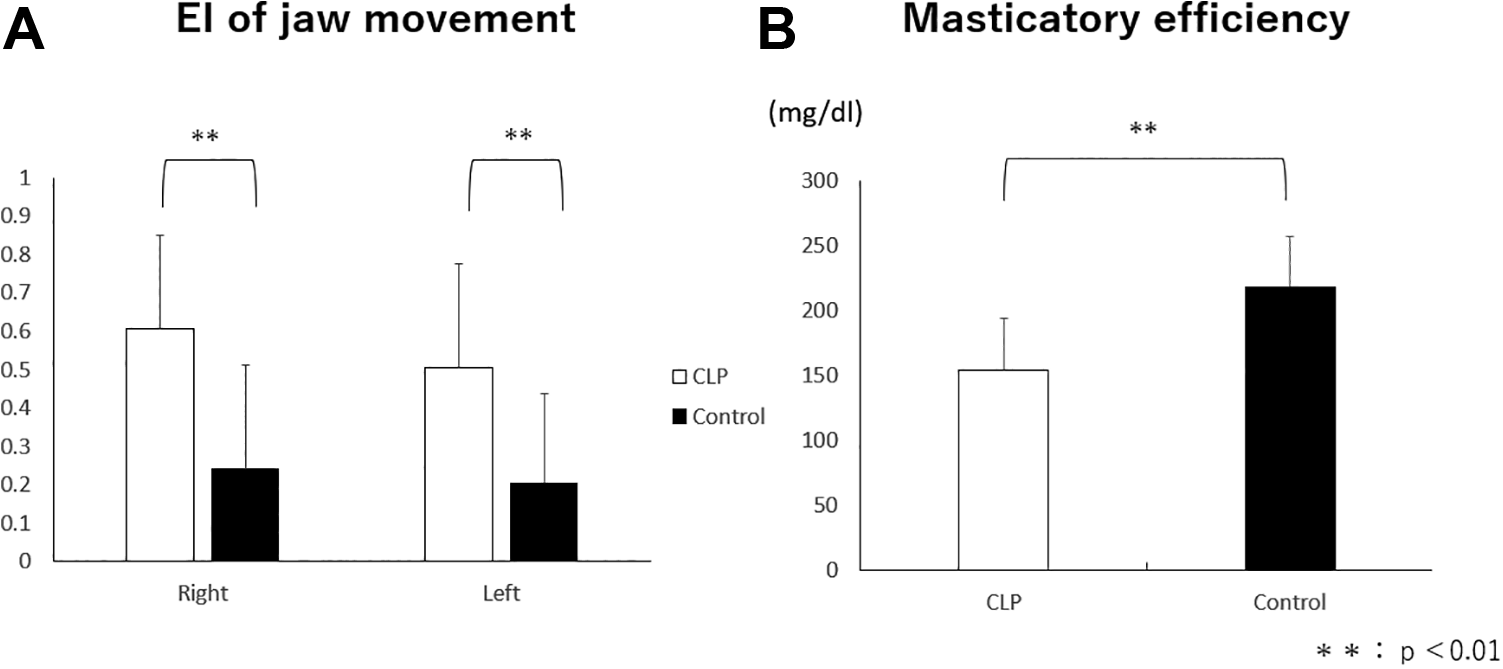
A, Comparison of error index (EI) of jaw movement between cleft lip and palate (CLP) and controls. B, Comparison of masticatory efficiency between CLP and controls.
The mean scores for masticatory performance are shown in Figure 4B. Although the controls showed significantly (P < .01) higher scores than patients with CLP, the score in patients with CLP was indicated to be within the normal range (over 150 mg/dL). As shown in Table 2, statistically significant correlations were found between masticatory efficiency and other masticatory functions. The total occlusal contact area, occlusal force, and EI of jaw movement were significantly correlated with masticatory efficiency; however, no significance was observed for muscle activity during maximum clenching and masticatory efficiency. All significant correlations between masticatory efficiency and occlusal contact area and force were positive, whereas the correlations with EI were negative.
The Correlation Coefficients Between Masticatory Efficiency and Other Masticatory Function.a

aP<0.05.
Discussion
In this study, we evaluated the masticatory function of orthodontically treated patients with CLP and compared the results to those of untreated Angle Class I controls, with the aim to clarify the differences, if any, between these 2 groups. Generally speaking, patients with CLP are more likely to exhibit poor masticatory functions, because of the present malocclusion in the vertical, anteroposterior, and transversal relationships in their dentition (Sipert et al., 2008; Altalibi et al., 2013; Paradowska-Stolarz et al., 2014; Montes et al., 2018). A frequent motivation to perform occlusal corrections in orthodontic treatment are not only esthetic issues but also functional disorders. Therefore, a comprehensive evaluation of the outcomes of orthodontic treatment related to masticatory function is essential.
Several factors are involved in determining masticatory muscle function. Optimal masticatory efficiency is a complex phenomenon affected by a number of major aspects, including a healthy temporomandibular joint, strong muscle force, and normal dentofacial relationships, including normal occlusion (Bakke, 1993; Hatch et al., 2001). For the present study, orthodontically treated patients with CLP with no symptoms of temporomandibular joint disorders were selected; the influence of occlusion on the complicated multifactor masticatory system would be limited as orthodontic treatment had been completed to reduce malocclusion. Therefore, in the present study, muscle function may be a primary factor in determining the optimal masticatory efficiency.
It must be noted though, that due to the nature of clefts in the oral cavity, patients with CLP are often missing permanent lateral incisors which are usually replaced with the canine of the same side or with prosthodontic crowns, and this factor may induce a concern on the outcomes of the tests performed in this study. For this study, 12 of 15 patients were reported to have missing permanent lateral incisors and 10 patients received prosthodontic replacement treatment, from within this group 5 patients with missing lateral incisors whether due to clefts on the upper jaw or dental agenesis in the lower jaw had these replaced with the canine of the same side; however, a previous report states that the occlusal force of the anterior dentition counts for less than 10% of the total dentition (Kumagai et al., 1999), because of this reason we consider that prosthodontic replacement of the missing lateral incisors would not represent a considerable impact in the results from this study.
We found that the total occlusal contact area during MVC was significantly smaller in the patients with CLP than in the controls. Moreover, no difference was found between the cleft and noncleft sides. However, the selected patients with CLP already showed satisfactory occlusion after orthodontic treatment, based on the OGS score of the ABO. This contradiction might be explained by the following reasons: (1) the static occlusal contacts assessed by model casts are fundamentally different from the occlusal contacts during MVC, and (2) patients with CLP may have substantially fewer occlusal contacts and near contacts because of the malocclusion involved in the vertical relationships of the upper and lower dentitions, especially after orthodontic treatment. With respect to the total occlusal force, significant differences were found between male patients with CLP and the controls, due to this force being strongly related to the occlusal contact area in the algorithm used by the Dental Prescale II System. Thus, the null hypothesis was rejected.
Despite this, muscle activity affected by the occlusal force did not show similar results. For the masseter muscle, muscle activity on the noncleft side in the patients with CLP and on the bilateral average in controls was larger than that on cleft side, although no significant differences were found in both males and females. This result suggested that the masseter muscle in patients with CLP works on the same levels as the masseter muscle in patients in the control group. On the other hand, the anterior temporal muscle activity in patients with CLP and controls did not seem to show a constant tendency. This can be attributed to the different roles of the temporal and masseter muscles. The temporal muscle stabilizes the mandibular position, while the masseter muscle mainly works during biting and clenching (Ueda et al., 1998; Szyszka-Sommerfeld et al., 2018).
With respect to jaw movement, the prevalence of abnormal chewing patterns, such as the reverse and crossover types, is reported to be higher in patients with skeletal Class III malocclusion, including anterior and/or posterior crossbite, than in the control group; Ben-Bassat et al. found that a very high prevalence of the reverse type and irregular masticatory strokes in patients with posterior crossbite became significantly lower after the correction of posterior crossbite (Ben-Bassat et al., 1993; Youssef et al., 1997; Ueki et al., 2005). In this study, we used EI to evaluate jaw movement more concretely by assessing the rate of abnormal mastication patterns (Nakata et al., 2007). Error index is the ratio of the number of strokes showing an abnormal chewing trajectory to the total number of chewing strokes. Patients with posterior malocclusion have also been reported to acquire normal jaw movement after establishment of a good occlusion (Miyawaki and Takada, 1997; Yashiro and Takada, 2004). However, in the present study, the EI values in the patients with CLP were significantly larger than those in the controls, even though anterior and/or posterior crossbite of the patients with CLP was corrected after orthodontic treatment. Meanwhile, in patients with normal occlusion, the masticatory movements of the mandible were more regular and consistent in form. Since jaw movement is a developmental function that matures as a result of learning experience, inadequate learning of mastication patterns and movements, which resulted in improper function before and during orthodontic treatment, may cause difficulties in obtaining a normal chewing cycle, even after optimal dental occlusion is established (Stevenson and Allaire, 1991). In future studies, it will be necessary to examine how patients with CLP adapt to and achieve normal chewing cycles, while determining if this process is associated with an improvement in jaw motor function. Neural control patterning might be another variable associated with this process. Therefore, the rehabilitation process should be considered carefully.
The most important measure of masticatory function is the efficiency in grinding food, since this factor has been recognized as having a direct impact on the patients’ quality of life. Therefore, masticatory efficiency or chewing performance in triturating food has major significance as the most important indicator of comprehensive and harmonious functioning of the stomatognathic system. Measurement of the amount of glucose extracted from chewing the gummy jelly has proven to be a reliable method for quantifying masticatory performance (Wilding and Lewin, 1994; Kobayashi et al., 2006; Shiga et al., 2006). The method used in the present study is simple and acceptable for use in both patients with CLP and patients in the control group.
In this study, after assessing the results from the used glucose sensor, patients with CLP demonstrated satisfactory masticatory efficiency in the normal range, although they showed significant differences in comparison with control data. Furthermore, we also found significant positive and negative correlations between masticatory efficiency and the total occlusal contact area/force and EI, respectively. Occlusal force has been recognized as a mechanical advantageous factor that plays an important role in determining masticatory efficiency, a quantitative indicator of masticatory function (Tate et al., 1994). Lower occlusal forces have been reported in patients with many kinds of malocclusions, and in those with incomplete dentitions, such as less occlusal contact area. In addition, masticatory efficiency is related to a widely excursed jaw-closing movement (Wilding and Lewin, 1994). Based on these findings, low occlusal force and abnormal jaw movement would be considered important functional deficits if these factors reduce the patient’s efficacy in breaking down a bolus. On the other hand, the significant difference in masticatory efficiency in the patients with CLP might be explained by the significant difference in occlusal contact area during MVC, as the dynamic occlusal contact status can substantially contribute to the chewing performance (Owens et al., 2002). Based on these findings, it seems reasonable to speculate that masticatory efficiency is correlated with the occlusal contact area/force and jaw movement. The direction and magnitude of the occlusal force vector during jaw-closing plays an important role as the major contributing factor for masticatory efficiency, and it might be independent of static occlusal assessment by the cast model and muscle activity during MVC in patients with CLP.
A limitation encountered while producing this study include the reduced number of patients. A future study which could include a larger cohort would certainly prove to be of greater statistical importance.
Finally, orthodontists treating patients with CLP in their practices, should strive to obtain optimum occlusal contacts on both cleft and noncleft sides, also adequate patient training aiming to correct any improper chewing movements that may have arisen due to the previously untreated clefts may also provide with more satisfactory end results for both the treating doctor and the patient.
Conclusion
This study confirms important masticatory functional differences between untreated controls and patients with CLP who underwent orthodontic treatment. These results suggest that orthodontic treatment for adult patients with CLP could result in satisfactory masticatory efficiency generated by the temporomandibular joint, muscles, and orthodontically achieved normal occlusion, although a significant difference was still found compared to the controls.
Footnotes
Authors’ Note
The Ethics Committee of Hiroshima University Hospital approved this cross-sectional study’s protocol, and informed consent was obtained from each patient after provision of sufficient explanation about the whole experiment (E-1221). This study adhered to the guidelines stated in the Declaration of Helsinki.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.