
Abstract
Objective
To describe trends, age, and sex-specific patterns of population hospital admissions with a diagnosis of craniosynostosis (CS) in Australia.
Data Source
Population data for hospital separations (in-patient) from public and private hospitals (July 1996-June 2018) were obtained from the publicly available Australian Institute of Health and Welfare (AIHW) National Hospital Morbidity Database.
Main outcome measures
The outcome variables were hospital separation rates (HSR) (number of hospital separations divided by the estimated resident population [ERP] per year) and average length of stay (aLOS) (patient days divided by the number of hospital separations) with a diagnosis of CS. Trends in HSR and aLOS adjusted for age, sex, and type of CS were investigated by negative binomial regression presented as annual percent change (APC).
Results
In 8057 admissions identified, we observed no significant change in the annual trend for HSR for the 22-year period. However, a marginal annual decrease of 1.6% (95% CI: -0.7, -2.4) in the aLOS was identified for the same time period. HSR were higher for males, infants, and single suture synostosis. aLOS was 3.8 days (95% CI: 3.8, 3.9) per visit, longer for syndromic conditions.
Conclusion
There was a minor reduction in the average length of hospital stay for CS over the 22-year period potentially indicative of improved care. Population-level information on hospitalisations for rare craniofacial conditions can inform research, clinical, and surgical practice.
Keywords
Background
Craniosynostosis (CS) (primary) refers to a developmental condition that results from premature fusion of cranial suture/s prior to completion of brain growth leading to deformation of the cranium and alterations in craniofacial morphology. 1 In Australia, CS occurs in approximately 1 in every 1900 births with the single suture synostosis form being the most common (0.08-0.4 in 1000 births and 80% of cases).2,3 Syndromic presentations are much less prevalent ranging from 1 in 35 000 (Crouzon syndrome) to 1 in 170 000 (Pfeiffer syndrome) births. 3 Among single suture synostosis, the sagittal suture (48.5%) is most frequently affected, followed by coronal (17.7%), metopic (17.0%), and lambdoid (16.7%) sutures, respectively. 3 All, except coronal synostosis, are more common in males when compared to females. 3
These disorders are treated by early craniofacial intervention, ideally at 4 to 13 months of age, to optimize opportunity for re-ossification of surgical cranial defects, allow skull growth, reduce risk of increasing intracranial pressure, and improve head shape. 4 Over time, surgical treatment for CS per se, has evolved from strip craniotomies to minimally invasive procedures (endoscopic suture release with helmet modeling) with the latter exhibiting minimal postoperative complications. 5 However, surgical management of CS incurs high costs and lengthy hospital visits which are often exacerbated by the presence of associated anomalies. 6
Although there have been a number of studies evaluating surgical management techniques and complications of CS, little is known about population-level patterns of hospital admissions for CS (especially the rare syndromic CS). 7
Hospitals in Australia are public and private, broadly funded by state and territorial governments and underpinned by a universal health insurance scheme (Medicare).8,9 The Australian Institute of Health and Welfare (AIHW) National Hospital Morbidity Database is a unique publicly available dataset that provides collated national data (from public and private hospitals) that can be used to assess trends of hospital admissions for various conditions, including dental and craniofacial.10,11, 12 However, use of population administrative data in craniofacial research has been largely limited to the reporting of hospitalisations related to oral clefts leaving little known about the hospital burden of rarer craniofacial anomalies including CS.10,13
Hence, the aim of this study was to describe trends, age, and sex-specific patterns of population hospital admissions with a diagnosis of CS, in Australia using population data from the AIHW National Hospital Morbidity Database over a 22-year period.
Methods
Study Design and Data Sources
This cross-sectional study used population hospital separation data for Australia made available by the AIHW. A compilation of episode-level records on CS-related admissions to public and private hospitals across all Australian states and territories were accessed online from the AIHW National Hospital Morbidity database. 11 These data are deidentified and not linkable to a specific individual such that the number of separations may include repeat admissions for the same individual.
The term CS used in this study refers to all separations with a principal diagnosis of craniosynostosis, craniofacial dysostosis, or acrocephalosyndactyly. Data for hospitalisations with the principal diagnosis of CS or craniofacial dysostosis (Crouzon syndrome) during the period between July 1, 1996 and June 30, 2018 were accessed. Data for hospitalisations related to constituent types of CS were available as subcategories from July 1, 2002 onwards. Data for hospitalisations associated with acrocephalosyndactyly (Apert syndrome) only during the periods from July 1, 2002 to June 30, 2015 and July 1, 2017 to June 30, 2018 were also accessed. Hospital separation data for acrocephalosyndactyly (Apert syndrome) was unavailable for years between 2015 to 2016 and 2016 to 2017 for reasons related to confidentiality, either of the patient or the health care provider especially if there were only one or two treating hospitals for the respective year.
The recent data (from July 1, 1998 onwards) in the AIHW are typically recorded according to the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM) diagnosis codes. Older data (July 1, 1996-June 30, 1998) was recorded according to ICD 9th revision, Clinical Modification (ICD-9-CM) diagnosis codes. The codes of interest in this study were CS [Q756.0 (ICD-9-CM) and Q75.0 (ICD-10-AM)]; types subcategorized: coronal synostosis (Q75.01), sagittal synostosis (Q75.02), trigonocephaly (Q75.03), CS of other multiple sutures (Q75.04), Pfeiffer syndrome (Q 75.05), cloverleaf skull (Q75.06), other and unspecified CS (Q75.09), and craniofacial dysostosis (Crouzon syndrome) [756.1 and Q75.1], and acrocephalosyndactyly (Apert syndrome) [Q87.02] (Supplementary Table 1). 14
Total estimated resident population (ERP) counts for different geographical regions of the country stratified on basis of age and sex for the financial years 1996 to 2018 were retrieved from an online tool (ABS.Stat Beta) maintained by the Australian Bureau of Statistics. 15
Study Outcome
Information collected in the study included the total number of separations per year with a principal diagnosis of craniosynostosis, craniofacial dysostosis, or acrocephalosyndactyly, patient days, sex, and age. 11 Outcomes were hospital separation rate (HSR) and average length of stay (aLOS). HSR was calculated by dividing the number of hospital separations by the ERP over the given time period. Separation from hospital refers to every episode of care for the admitted patient including total hospital stay (from admission to discharge, transfer, or death) or a portion of hospital stay beginning or ending in a change of type of care (ie acute care to rehabilitation).11,16 AIHW considers number of hospital separations as the number of hospital admissions and hence HSR is equivalent to the hospital admission rate. 17 aLoS refers to average number of patient days for admitted patient episodes. 16
Additionally, we recorded the total number of separations related to all congenital anomalies to allow comparison with CS separation data by age [Older data (July 1996-June1998) ICD-9-CM 740-759; recent data (July 1998 onwards) ICD-10-AM: Q00-Q99)].
Explanatory Variables
We described associations of HSR and aLoS with age groups, sex, and type of CS. We categorized age at separation as “<1 year”, “1-4 years”, “5-14 years”, and “15-79 years” based on reported guidelines for the treatment of CS. 6
For analysis purposes, types of CS (data available from July 2002 onwards) in our study were broadly divided into single suture synostosis (includes principal diagnosis of sagittal, coronal, and metopic synostosis), multiple suture synostosis, and syndromic synostosis [includes principal diagnosis of craniofacial dysostosis (Crouzon syndrome), acrocephalosyndactyly (Apert syndrome), Pfieffer syndrome, and cloverleaf skull].
Statistical Analysis
Descriptive statistics were used to summarize the admission patterns for the observed time period. Linear trends in the overall rates of HSR and aLoS for CS (1996-2018) adjusted for age and sex were investigated using the negative binomial regression and the annual percent change (APC) of incidence rate was reported. The APC was calculated by exponentiating the beta coefficient of the time variable (ie year group) and subtracting 1. 18 The association of separation rates and aLOS with age (data available: 1996-2018), sex (data available: 1996-2018), and type of CS (data available: 2002-2018) was assessed using the same modeling approach with the estimates shown as incidence rate ratio (IRR). All estimates and their 95% confidence intervals were reported. Statistical significance was defined at the 5% level. All analyses were carried out using Stata 16.0 (StataCorp). As this project used publicly available data and not individual data, an exemption from the review was obtained from the Human Research Ethics Committee of the University of Western Australia (RA/4/1/7865).
Results
We identified a total of 8057 separations for the principal diagnosis of CS, craniofacial dysostosis, and acrocephalosyndactyly between 1996 and 2018 and the HSR was calculated to be 0.16 per 10 000 ERP. These rates showed no significant change in annual trend over the observed time period (APC −0.2% [95% CI: −1.5, 1.1]) (Figure 1). However, we observed a marginal decrease in aLOS (APC: −1.6% [95% CI: −0.7, −2.4]) over the same time period (Figure 2). Additionally, HSR and aLOS showed variable differences within different age groups, sex, and CS types as described below.
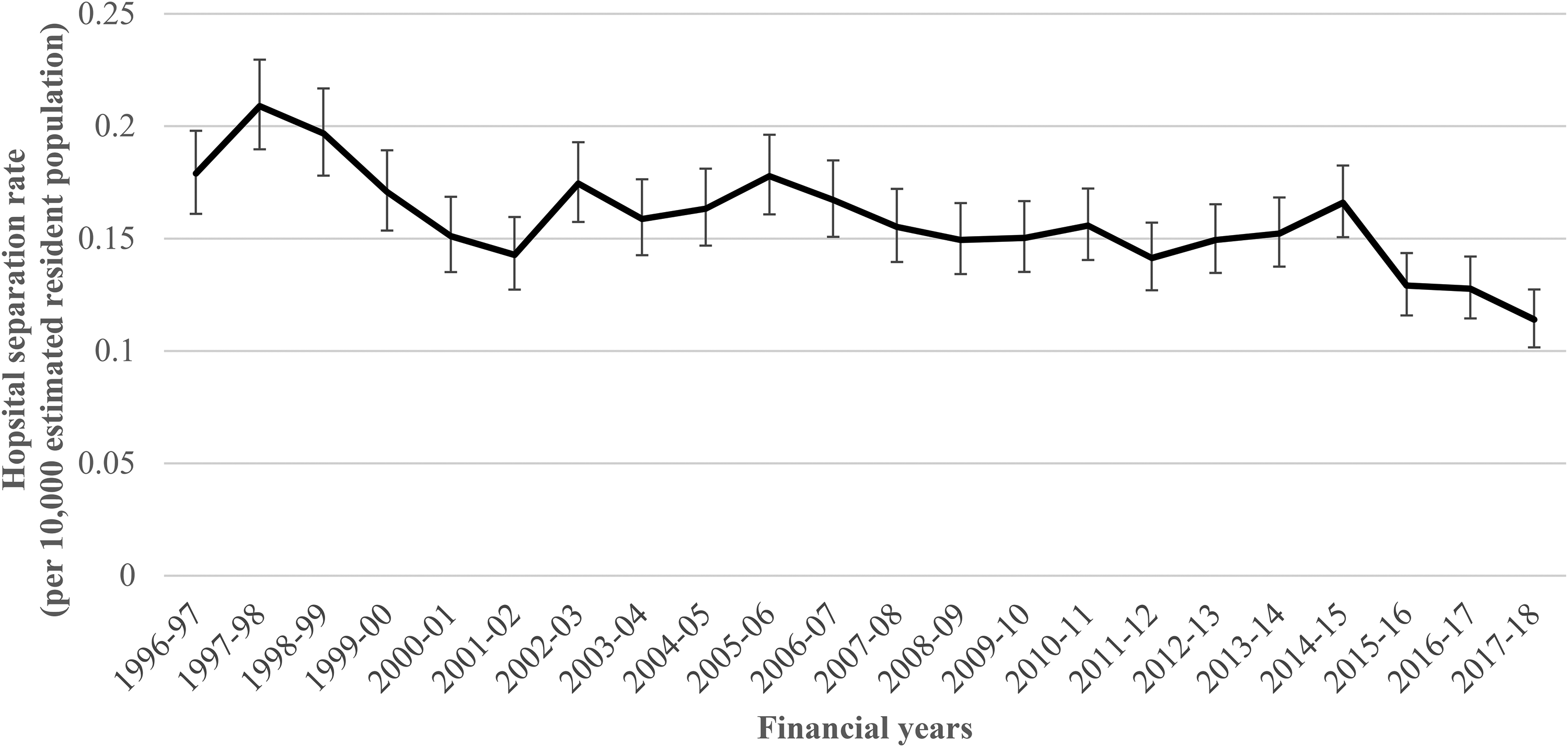
Description and trends of hospital separation rates (HSR) for the principal diagnosis of either craniosynostosis , craniofacial dysostosis, and acrocephalosyndactyly between July 1996 and June 2018.
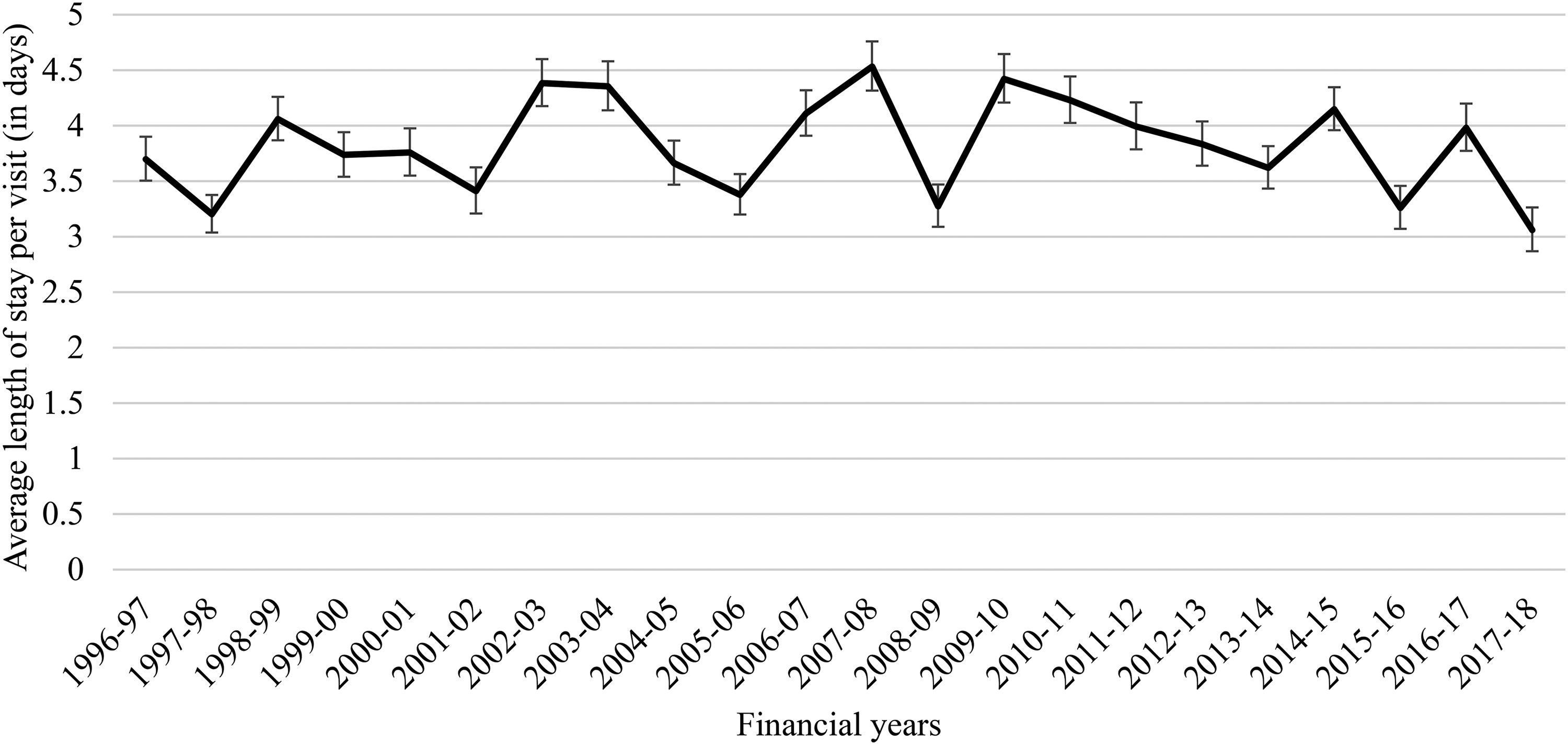
Description and trends of average length of stay (aLOS) per visit for the principal diagnosis of either craniosynostosis, craniofacial dysostosis, and acrocephalosyndactyly between July 1996 and June 2018.
Hospital Separation Rate
Age
We identified separations with the diagnosis of CS which occurred across all ages up to 79 years. A sharp decline in HSR for CS was observed with increasing age [IRR 0.21 (95% CI: 0.20, 0.22)]; (Table 1 and Supplementary Table 2). The proportion of admissions for CS was also higher (88.4%) when compared to the proportion of admissions of every other congenital anomaly combined (48.6%) in those under 5 years (P = .001).
Descriptive Statistics of Hospital Separations, Hospital Separation Rates, and Average Length of Stay, by Age, Sex, and Type of Craniosynostosis.
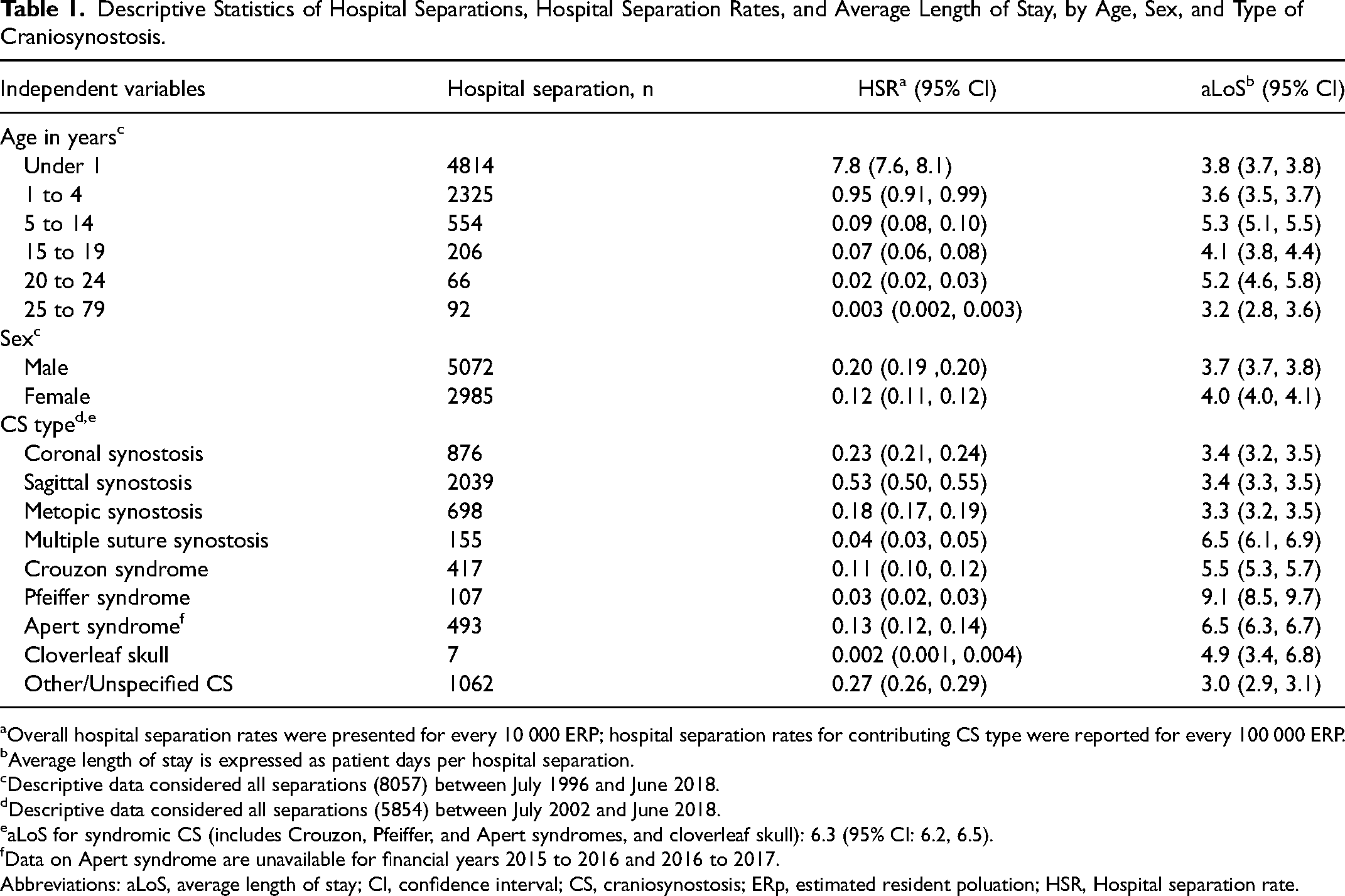
Overall hospital separation rates were presented for every 10 000 ERP; hospital separation rates for contributing CS type were reported for every 100 000 ERP.
Average length of stay is expressed as patient days per hospital separation.
Descriptive data considered all separations (8057) between July 1996 and June 2018.
Descriptive data considered all separations (5854) between July 2002 and June 2018.
aLoS for syndromic CS (includes Crouzon, Pfeiffer, and Apert syndromes, and cloverleaf skull): 6.3 (95% CI: 6.2, 6.5).
Data on Apert syndrome are unavailable for financial years 2015 to 2016 and 2016 to 2017.
Abbreviations: aLoS, average length of stay; CI, confidence interval; CS, craniosynostosis; ERp, estimated resident poluation; HSR, Hospital separation rate.
Sex
Overall, there were more male separations with CS (5072 separations) [IRR 1.4 (95% CI: 1.1, 1.6)] than female (2985 separations) (Figure 3, Table 1 and Supplementary Table 3).
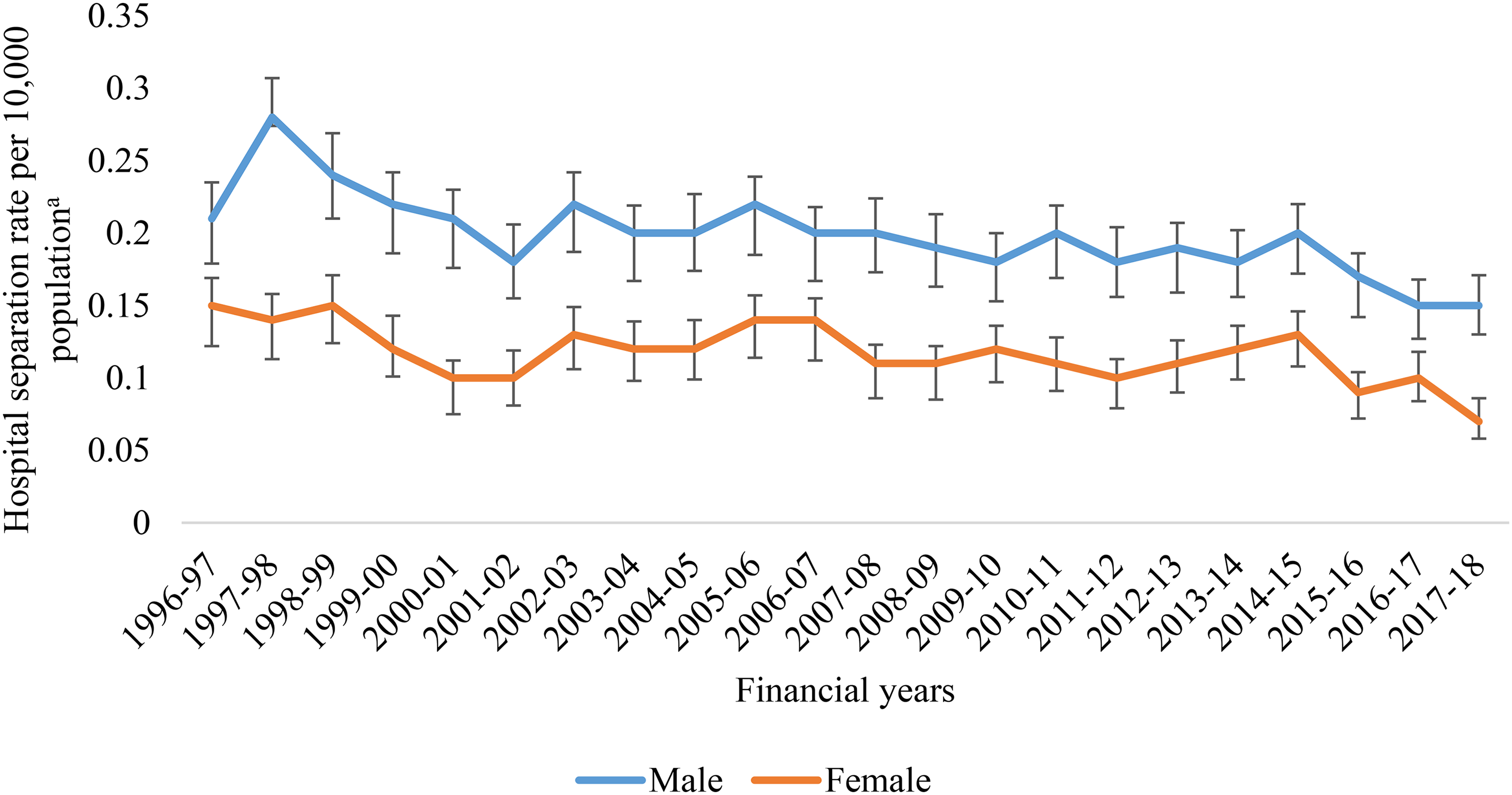
Differences in sex for hospital separation rates (HSR) with the principal diagnosis of either craniosynostosis, craniofacial dysostosis, and acrocephalosyndactyly observed between July 1996 and June 2018.
CS Type
Of the total separations identified (5854) between 2002 and 2018, more than one-third had a diagnosis of sagittal synostosis (34.8%) followed by other and unspecified CS (18.1%), coronal synostosis (15%), trigonocephaly (metopic synostosis) (11.9%), Apert syndrome (8.4%), Crouzon syndrome (7.1%), multiple suture synostosis (2.6%), Pfeiffer syndrome (1.8%), and cloverleaf skull (0.1%) (Table 1).
Almost three-fifths of admissions with a diagnosis of coronal synostosis were females (59.7%) and there were more male admissions for diagnosis of sagittal synostosis and metopic synostosis (72.2% and 73.9%, respectively). Most admissions related to syndromic CS were males but for Pfeiffer syndrome, there was a marked female preponderance (66.4%) (Figure 4).
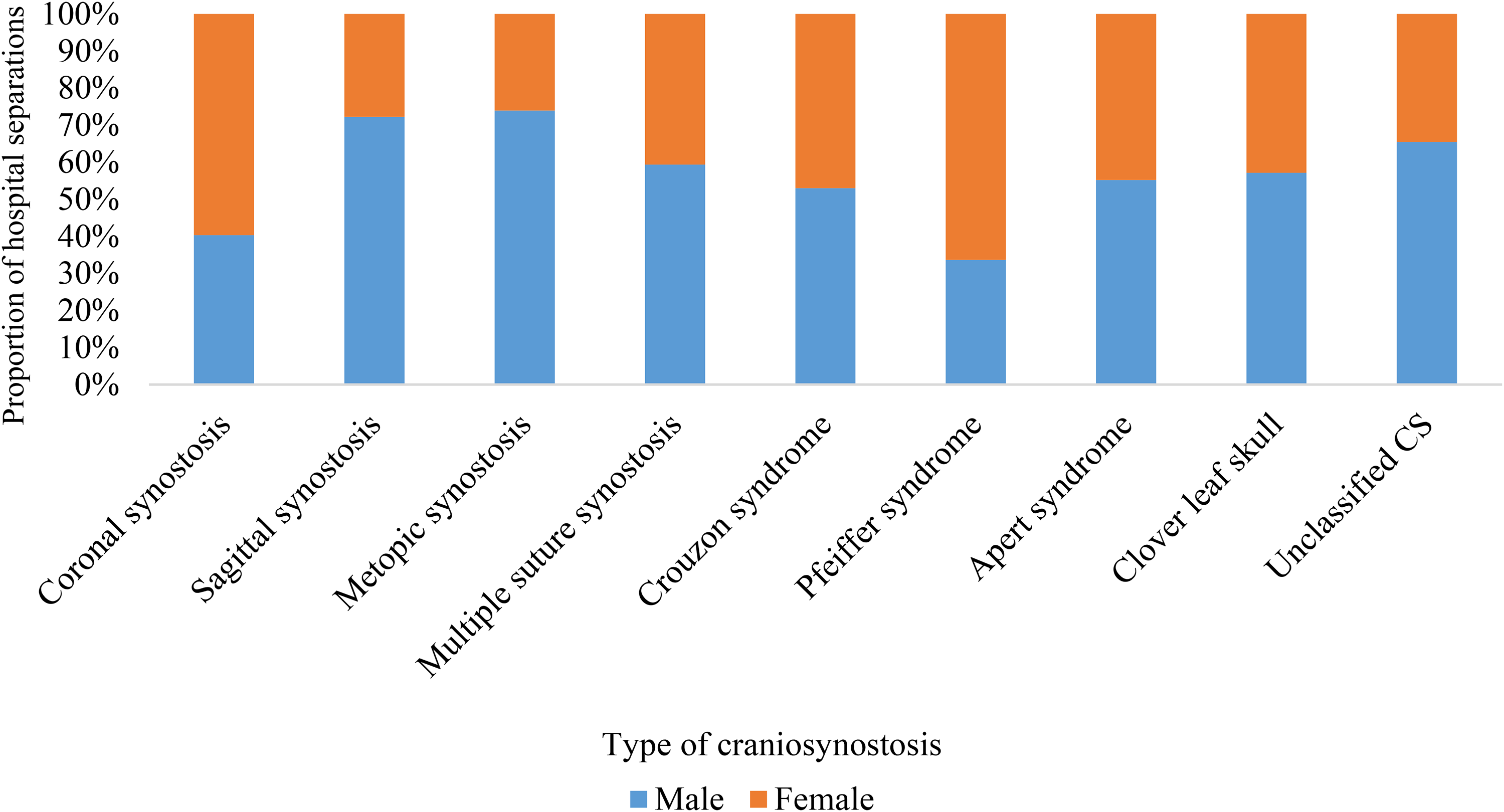
Proportion of hospital separations (%) for different types of craniosynostosis (CS) according to sex.
The incidence of hospital admissions related to single suture synostosis (eg sagittal, coronal, and metopic synostosis) declined with increasing age (Table 2 and Supplementary Table 4). However, the incidence of hospital admissions for the diagnosis of syndromic CS among the 15 to 79 age group was almost five times that of single suture synostosis [IRR: 4.50 (95% CI: 2.55, 7.94)] (Table 2).
Adjusted Associations of Craniosynostosis Type with Hospital Separation Rates (HSR) and Average Length of Stay (aLOS) According to Different age Categories Calculated Using Negative Binomial Regression (July 2002-June 2018).
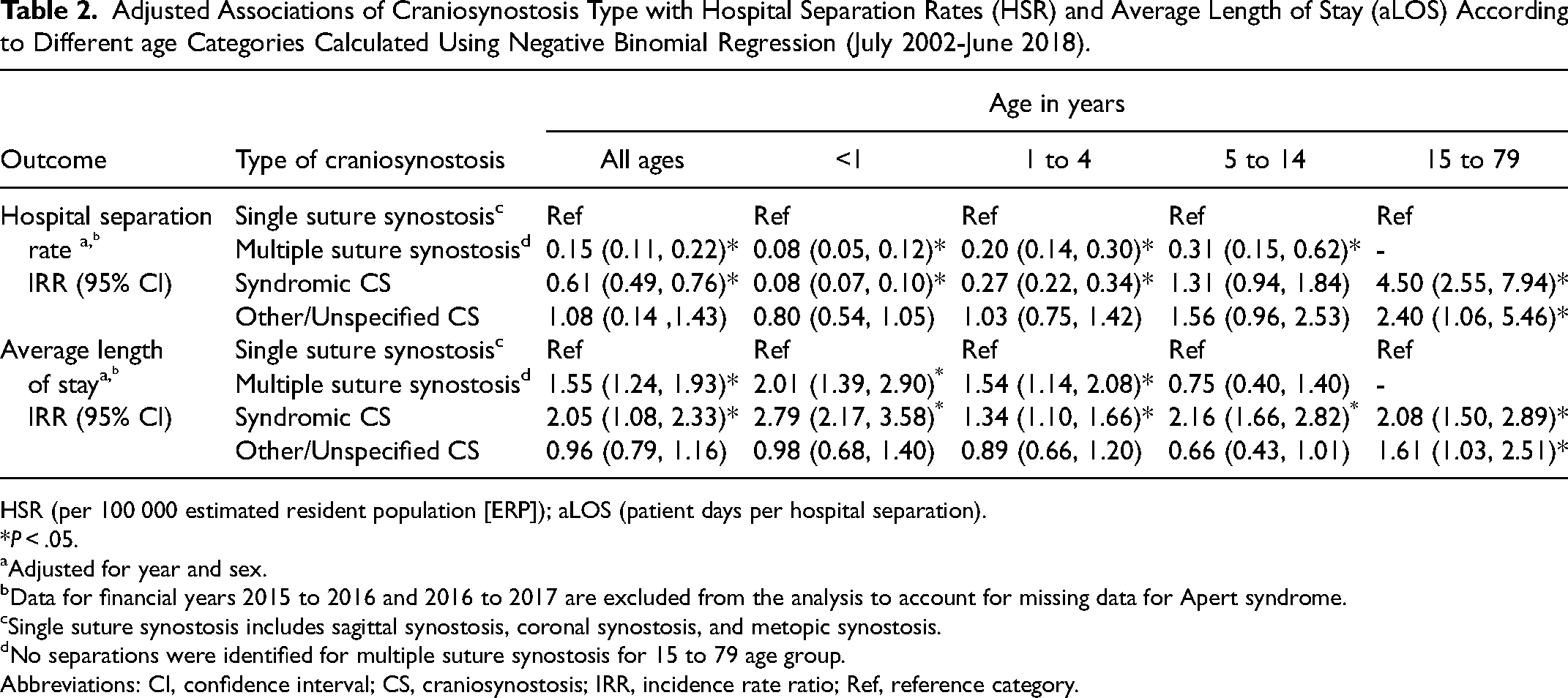
HSR (per 100 000 estimated resident population [ERP]); aLOS (patient days per hospital separation).
*P < .05.
Adjusted for year and sex.
Data for financial years 2015 to 2016 and 2016 to 2017 are excluded from the analysis to account for missing data for Apert syndrome.
Single suture synostosis includes sagittal synostosis, coronal synostosis, and metopic synostosis.
No separations were identified for multiple suture synostosis for 15 to 79 age group.
Abbreviations: CI, confidence interval; CS, craniosynostosis; IRR, incidence rate ratio; Ref, reference category.
Average Length of Stay
CS admissions had an average hospital stay of almost 4 days [3.8 (95% CI: 3.78, 3.87)]. Based on age, aLoS was the highest for children aged between 5 and 14 years [5.3 (95% CI: 5.1, 5.5)], despite this group having much lower hospitalization rates than those under the age of 1 year [IRR: 1.4 (95% CI: 1.1, 1.7)] (Tables 1 and 2). Males had a slightly shorter average hospital stay when compared to females [IRR: 0.9 (95% CI: 0.8, 1.1)) (Supplementary Table 3).
Based on CS types, admissions related to Pfeiffer syndrome had an extended average hospital stay of about 9 days [9.1 (95% CI: 8.5, 9.7)] per visit and those with coronal synostosis had the shortest mean stay of around three and a half days [3.4 (95% CI: 3.2, 3.5)] per visit (Table 1). Syndromic CS (includes principal diagnosis of Crouzon, Apert, Pfeiffer syndrome, and cloverleaf skull) patients stayed twice as long in the hospital during each visit than those with single suture synostosis [IRR: 2.05 (95% CI: 1.08, 2.33)] (Table 2).
Discussion
Our study findings indicate no significant change in trend in the HSR for CS over 22 years; however, we observed a marginal annual reduction in aLOS over the same period. The proportion of admissions for syndromic CS was higher for age groups 1 to 5, 5 to 15, and 15 to 19 years than single suture synostosis. Overall HSR for sagittal synostosis were highest followed by the other single suture synostosis and syndromic CS, respectively. These rates showed additional differences related to sex which varied according to the specific type of CS. Additionally, we identified lengthier hospital stay for syndromic CS across all age groups than single suture synostosis.
The considerable strength of this study was that it explored trends in hospital admissions of CS using administrative data over a time span of two decades. However, a sizeable group of CS was coded as unspecified (18.1%) in the dataset which reduced our ability to draw inferences or conclusions. The use of different classifications (ICD-CM-9 and ICD-AM-10) in the data collected from 1998 to 1999 may confound analyses. 19 Details related to non-CS admissions (eg upper respiratory tract infections, ear infections, or other potential conditions) in this data collection are unavailable as non-CS admissions are coded with different distinct principal diagnostic codes which are not linkable with CS. Although the publicly available AIHW National Hospital Morbidity Database provides procedure information for all separations excluding neonates, 20 the procedure codes are not linked to principal diagnosis codes which limits our understanding of the exact treatment changes with time.
The stable trend in hospitalization rates which we observed could potentially relate to the continued use of traditional surgical techniques in preference to minimal invasive surgery for managing CS by the majority of craniofacial units in Australia in spite of the growing popularity of the latter in other developed countries.21,22 However, the reduction in aLOS in our data could also indicate efficiency and improved quality of hospital care. 17 These findings are likely a consequence of refined surgical protocols, better anesthetic techniques, improved perioperative management, and surgical planning (to a lesser extent) through the use of enhanced diagnostic techniques (computed tomographic [CT] scans, three-dimensional craniofacial analysis).23,24,22
A large proportion of admissions took place during infancy which is in line with the ideal age for craniofacial interventions for CS. 4 We also observed a large number of CS-related admissions for children aged between 1 and 5 years. These might reflect those admissions related to patterns of diagnosis (delayed diagnosis), increased waiting times between specialist diagnosis and elective surgery, surgical timing of cases (delayed especially for syndromic CS), postsurgical complications, major revision procedures, and/or continued treatment for specific syndromic conditions.6,25,26 There was a substantial decline in the number of separations for children over the age of 5, however, differences were observed based on types of CS. The majority of admissions relating to single suture synostosis (eg coronal, sagittal, or metopic) occurred under 1 year of age with fewer admissions with increasing age. These children usually have lower rates of postoperative complications, better surgical outcomes as well as fewer CS-related service contacts in later life. 27 Individuals born with syndromic CS, however, have prolonged service contacts when compared to those born with single suture synostosis.27,6 As most syndromic CS has an underlying genetic cause, better access to genetic diagnostic testing may provide an opportunity for increasing the precision of service planning.
The need for extensive surgical corrections to manage the additional complexity and complications ensuing from surgical procedures could contribute to the lengthier hospital visits for syndromic CS. However, the length of hospital stay for syndromic CS could also be influenced by underlying non-craniofacial structural or functional comorbidities.28,6 We observed a similar length of hospital stay for infants (under 1 year of age) with single suture synostosis in Australia to those undergoing management for non-syndromic CS in the United States of America, reflecting similar treatment practices. 29
These differences in overall HSR could likely be explained by different population prevalence rates for individual CS types. However, we observed higher rates of hospitalisation for Apert's syndrome between 2005 to 2006 and 2009 to 2010, rates which would be at variance with the prevalence rates for this clinical condition. This finding reflects repeated hospital service use which could be an outcome of varying protocols followed by different craniofacial units across Australia with a few units serving as referral centers for overseas syndromic CS patients. 30 The subsequent decline in the HSR after 2010 could indicate either reduced prevalence of disease over time, improved case management, and/or reduced overseas admissions which requires further investigation beyond the scope of this data.
The findings of this study could serve as baseline information for future population data linkage studies which can evaluate individual-level patient data. Furthermore, it will be critical that health system coding (Orphacodes) is granular and can accommodate for clinical grouping that can accommodate meaningful and accurate classification including for syndromic and rare causes of CS. 31
Conclusions
This study provides unique population data indicating a marginal reduction in the overall aLOS of CS potentially suggestive of improved care services. We observed a greater incidence of syndromic CS admissions with increasing age relative to single suture synostosis which indicates the prolonged hospital service use of these rare conditions. We also identified lengthy hospital stays for syndromic CS which could potentially relate to the severity of phenotype, surgical complications, and requires further exploration. Such population-based studies in addition to genetic diagnosis are imperative to improve our understanding of rare craniofacial conditions that would provide an opportunity to advance system efficiency and value.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656221074215 - Supplemental material for Epidemiology of Hospital Admissions for Craniosynostosis in Australia: A Population-Based Study
Supplemental material, sj-docx-1-cpc-10.1177_10556656221074215 for Epidemiology of Hospital Admissions for Craniosynostosis in Australia: A Population-Based Study by Mohammed Junaid, Linda Slack-Smith, Kingsley Wong, Gareth Baynam, Hanny Calache, Timothy Hewitt and Helen Leonard in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656221074215 - Supplemental material for Epidemiology of Hospital Admissions for Craniosynostosis in Australia: A Population-Based Study
Supplemental material, sj-docx-2-cpc-10.1177_10556656221074215 for Epidemiology of Hospital Admissions for Craniosynostosis in Australia: A Population-Based Study by Mohammed Junaid, Linda Slack-Smith, Kingsley Wong, Gareth Baynam, Hanny Calache, Timothy Hewitt and Helen Leonard in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656221074215 - Supplemental material for Epidemiology of Hospital Admissions for Craniosynostosis in Australia: A Population-Based Study
Supplemental material, sj-docx-3-cpc-10.1177_10556656221074215 for Epidemiology of Hospital Admissions for Craniosynostosis in Australia: A Population-Based Study by Mohammed Junaid, Linda Slack-Smith, Kingsley Wong, Gareth Baynam, Hanny Calache, Timothy Hewitt and Helen Leonard in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-4-cpc-10.1177_10556656221074215 - Supplemental material for Epidemiology of Hospital Admissions for Craniosynostosis in Australia: A Population-Based Study
Supplemental material, sj-docx-4-cpc-10.1177_10556656221074215 for Epidemiology of Hospital Admissions for Craniosynostosis in Australia: A Population-Based Study by Mohammed Junaid, Linda Slack-Smith, Kingsley Wong, Gareth Baynam, Hanny Calache, Timothy Hewitt and Helen Leonard in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
The authors are grateful to the Australian Institute of Health and Welfare and Australian Bureau of Statistics for providing the data; however, the authors are responsible for the subsequent data extraction and analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Mohammed Junaid is being supported by the Australian Government International Research Training Program Scholarship and the Stan and Jean Perron Top-Up Scholarship.
Author Contribution
The study was conceptualized by MJ, LSS, and HL. MJ, LSS, and HL participated in the organization and execution of the study including planning the analysis, drafting, and reviewing the manuscript. MJ and KW designed and executed the statistical analysis, in discussion with other authors. All authors were actively involved in interpreting data, drafting, reviewing, and revising the manuscript and have read and approved the final manuscript.
Availability of Data and Materials
The raw data on separation statistics collected for this paper can be accessed online through the website of the Australian Institute of Health and Welfare (![]() ). Separation statistics for years 1993 to 2018 are available with the National Hospital Morbidity database which can be accessed through a SAS Web report studio which allows filtering and export of data.
). Separation statistics for years 1993 to 2018 are available with the National Hospital Morbidity database which can be accessed through a SAS Web report studio which allows filtering and export of data.
Ethics Approval
As this project used publicly available data and not individual data, an exemption from review was obtained from the Human Research Ethics Committee of the University of Western Australia (RA/4/1/7865).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.