
Abstract
Objective
Assess cephalometric parameters and the need for orthognathic surgery (OS) and its relationship with compliance in protraction headgear (PHG).
Design
Retrospective case series.
Setting
Hospital cleft-craniofacial center.
Patients
23 patients with nonsyndromic cleft lip and palate and history of lip and palate repair.
Interventions:
Patients received PHG and orthodontic treatment. Compliant patients were compared to patients that were not. Protraction was applied with 170-gram elastics and patients were instructed to wear for at least 12 hours daily.
Main outcome measures
Cephalometric measurements at initial (T1), post-PHG (T2), and pre-surgical or post-orthodontic treatment (T3) of at least age 15 for females and 17 for males and the presence of OS were compared.
Results
83% (19) of patients reported compliance with therapy. Of those compliant, 68% (13) had OS and 32% (6) did not (P = .99). Inter-group comparisons at T1 between compliant and noncompliant showed no significant differences and the non-OS patients started with larger nasolabial angles (P < .05). At T2, there were no significant cephalometric differences between groups. At T3, compliant patients showed significantly more upper incisor proclination than noncompliant patients. Between OS and non-OS, OS patients had significantly decreased ANB, Wits, convexity, overjet, and FMA and larger nasolabial angles (P < .05).
Conclusions
Patients compliant with PHG showed no difference in the need for OS. However, after orthodontic treatment, compliant patients showed more upper incisor proclination and OS patients with decreased ANB, Wits, convexity, overjet, FMA, and larger nasolabial angles.
Introduction
It is common for patients with cleft lip and palate (CLP) to develop maxillary hypoplasia, resulting in a class III skeletal relationship and negative overjet. The etiology may be associated with intrinsic deficiencies, functional muscle distortions, and iatrogenic factors. 1 Numerous studies on adults with unoperated clefts have shown minimal deviations from adults without clefts implicating iatrogenic factors introduced during treatment may be a significant source of midface deficiency in patients with CLP.1,2,3 For patients with unilateral cleft lip and palate (UCLP), surgical lip repair within the first 6 months of life has no appreciable adverse effects on growth of the maxillary size and position.2,4,5 However, surgical palate repair has been suggested to have inhibitory effects on the growing maxilla. This intervention creates scar formation that inhibits maxillary growth.2,4,6,7,8 The scar tissue may inhibit separation of the maxilla, palatine, and pterygoid plates, thereby creating a form of maxillary ankylosis. 2 Additionally, aggressive palatoplasty may leave an area of denuded bone adjacent to the alveolus upon which periodontal fibers may become embedded, contracting and collapsing the arches as well as possibly disrupting vertical eruption of the dentition.1,2 Palatoplasties for UCLP repair have been associated with an increased rate of midfacial retrusion observed between ages 8 and 15, especially if the surgery was completed prior to the first year of life.8,9 Impaired maxillary growth subsequently leads to a retrognathic maxilla, flatter midface, more concave profile, distortion of dentoalveolar structures, and difference in posture and shape of the mandible that may increase the mandibular plane angle and decrease protrusion of the chin as the child ages.2,7,10 This is in contrast to those with unoperated UCLP showing SNA to be normal or prognathic compared to patients without clefts; specifically, those without surgical palate repair had the potential for adequate maxillary growth and occlusion capable of compensating for the skeletal discrepancy.2,4,11,12
There are several treatment options to address midfacial retrusion that are often dependent upon the severity and physical maturity of the patient. Orthopedic appliances such as the chin cup, Frankel III, and protraction headgear (PHG) or procedures such as maxillary distraction osteogenesis or bone-anchored protraction may be used to alleviate skeletal Class III discrepancies.13,14
PHG is a functional orthodontic appliance often used in prepubertal children in early to late mixed dentition, particularly before age 10, to treat maxillary deficiency in skeletal Class III discrepancies. 15 This treatment aims to displace the maxilla forward into a skeletal and dental Class I relationship with positive overjet. Mandibular downward and backward rotation also occurs. Cephalometric changes that have been observed with PHG in patients without CLP are increases in SNA, Wits, ANB, mandibular plane, and upper incisor angulation, decreases in SNB, IMPA, and palatal plane values, and forward movement of Point A.15–17 Long-term follow-up studies reassessing patients after their pubertal growth spurt, however, suggested that treatment effects in SNA, SNB, ANB, and skeletal effects were not maintained. 18 PHG may have a better prognosis to reach Class I relationships with positive overjet in patients that are younger than age 10 years with shorter ramus, obtuse cranial base angle, and lower mandibular plane angle or to overcorrect until overjet is 5 to 8 mm and the molars are in Class II.14,19,20 PHG in patients with CLP has demonstrated maxillary protraction and clockwise mandibular rotation in prepubertal patients and improves both cephalometric hard and soft tissue values.8,13,21,22,23 Long-term prognosis, however, showed a large variation of relapse. 8 Treating Class III discrepancies in patients with CLP is difficult because results may depend more on surgical history than the orthopedic appliance; specifically, effects of protraction may vary cleft to cleft, especially the amount and condition of the palatal scar tissue.8,24,25,26 In patients without CLP, relapse rates range from approximately 12% to 33% where negative overjet has been observed in patients that have completed growth with a history of PHG.18,19,21,27 PHG starting between the ages of 7 to 9 yielded patients that maintained positive overjet by age 15, thus odds of needing orthognathic surgery were 3.5 times more likely when PHG was not used compared to those with early PHG. 18 There is little evidence suggesting the long-term prognosis of PHG in patients with CLP and its prognostic factor in predicting whether early measures of successful PHG correlate with a decreased incidence of orthognathic surgery. The aim of this study is to assess the need for orthognathic surgery (OS) and the relationship with compliance in PHG. The secondary aim is to evaluate cephalometric characteristics of patients that did not need OS and to increase the available long-term data on the use of PHG in patients with CLP.
Methods
23 participants for this study were selected from the craniofacial center with the following inclusion criteria: (1) Patients with nonsyndromic (2) unilateral or bilateral cleft lip and palate treated with (3) PHG with or without expansion followed by (4) completion of Phase II orthodontics. Patients also have a history of (5) cleft lip and (6) cleft palate repairs. Additionally, patients selected have (7) a minimum of 3 lateral cephalograms at pre-PHG (T1), post-PHG (T2), and pre-surgical or post-orthodontic treatment (T3) of at least age 15 for females and 17 for males. The exclusion criteria were patients that had (1) syndromic clefts, (2) did not receive PHG, (3) or lacking lateral cephalograms at designated timepoints.
Variations of bonded, banded, or quad-helix palatal expanders were used if arch form coordination was needed prior to protraction. Buccal arms from the permanent first molars were extended to the canine area. Protraction was applied with PHG and 170-gramelastics were connected to each buccal hook and directed slightly downward in relation to the occlusal plane. Patients were instructed to wear the headgear for at least 12 hours daily until at least 3 mm of positive overjet was achieved. Comprehensive orthodontic treatment was completed after protraction.
Cephalograms were produced before and after PHG and another representing completion of growth at age 15 for females and 17 for females or as a part of the patient's pre-surgical records. Patients’ records were reviewed for the presence or absence of an expander, comments on PHG therapy compliance, and the presence, absence, or recommendation for orthognathic surgery. Cephalograms were digitized and traced using Dolphin Imaging and Management Solutions to assess the cephalometric variables (Figure 1).
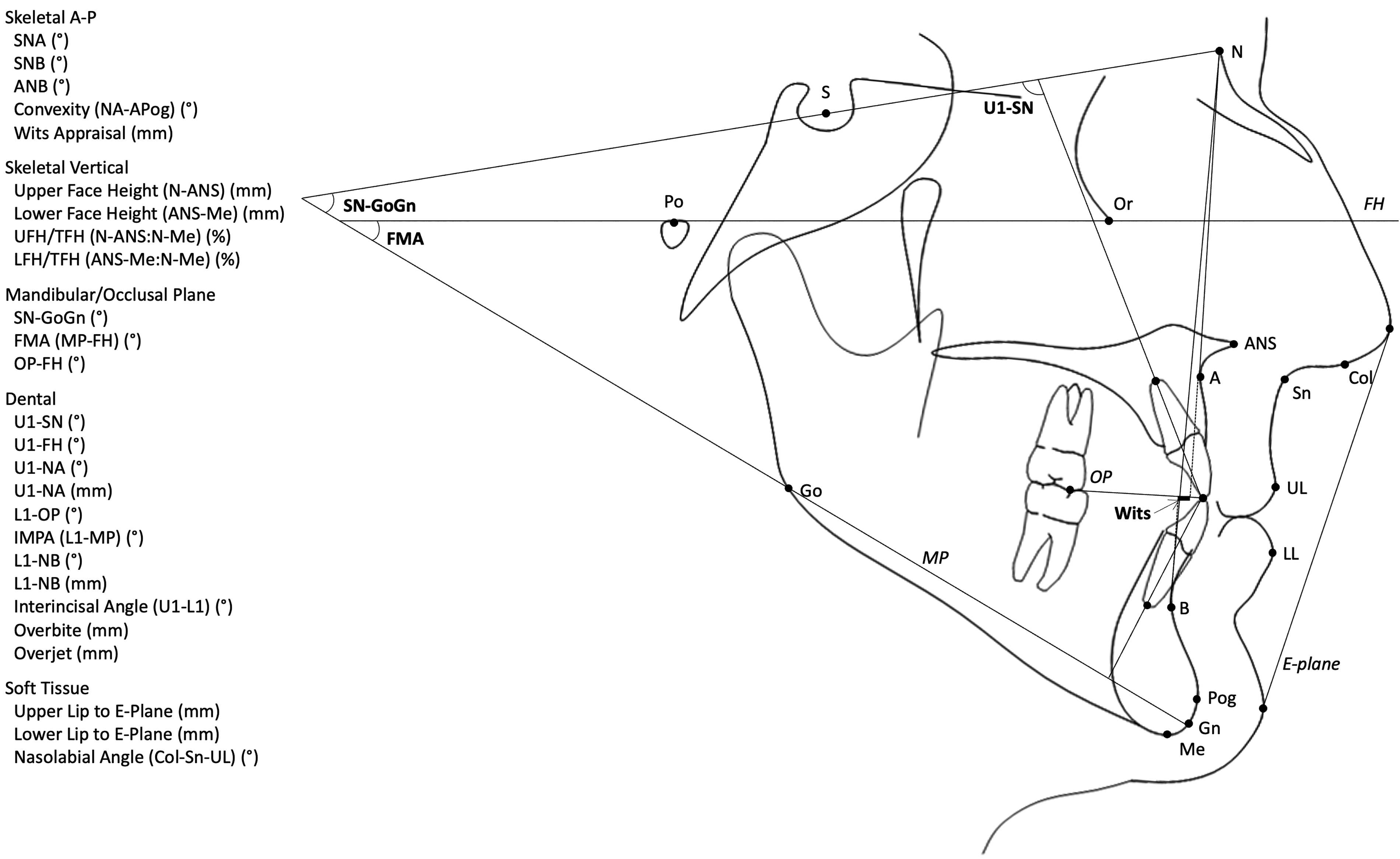
Cephalometric tracing.
Statistical Analyses
Fisher's exact test was used to evaluate the association between compliance in PHG therapy and the presence or recommendation for OS. Two-sample independent t-tests were used to evaluate significant differences between compliant and noncompliant groups and OS and non-OS groups at T1, T2, and T3. Two-sample paired t-tests were used to evaluate significant changes among patients in the compliant, noncompliant, OS, and non-OS groups.
Results
A total of 23 patients matched the inclusion criteria for this study. 10 females (43%) and 13 males (57%) and 18 with UCLP (78%) and 5 with BCLP (22%). The average ages at T1, T2, and T3 were 8.3, 9.5 years, and 16.7 years, respectively, and the average PHG treatment duration was 7.4 months.
19 (83%) of 23 patients reported compliance with PHG therapy. Among those that were compliant, 68% had OS and 32% did not. 4 (17%) patients were not compliant with PHG and 75% needed OS. There was no significant association between PHG compliance and OS (Table 1).
Fisher's Exact Test for Association Between PHG Compliance and OS.
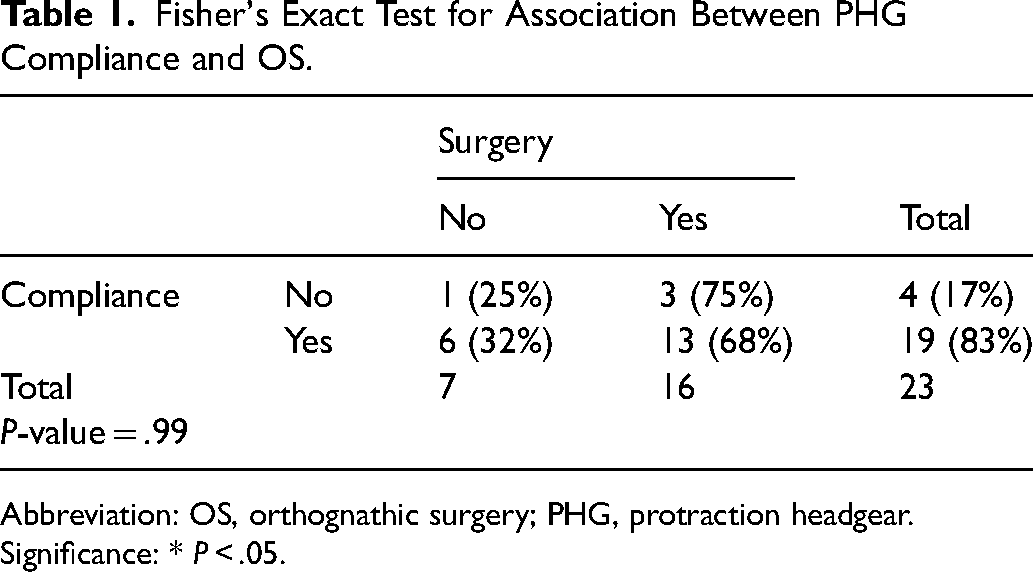
Abbreviation: OS, orthognathic surgery; PHG, protraction headgear.
Significance: * P < .05.
At T1, the only significant difference was that the OS group had a nasolabial angle 18° smaller than the non-OS group; the remainder showed no significant cephalometric differences.
At T2, there were no significant cephalometric differences between patient groups. However, compliant patients achieved positive overjet of 2 mm with approximately 11° and 4 mm more upper incisor proclination and protrusion, respectively, 4 mm more overjet, and 2 mm more upper lip protrusion compared to noncompliant patients (Table 2).
Average Cephalometric Differences at T2.
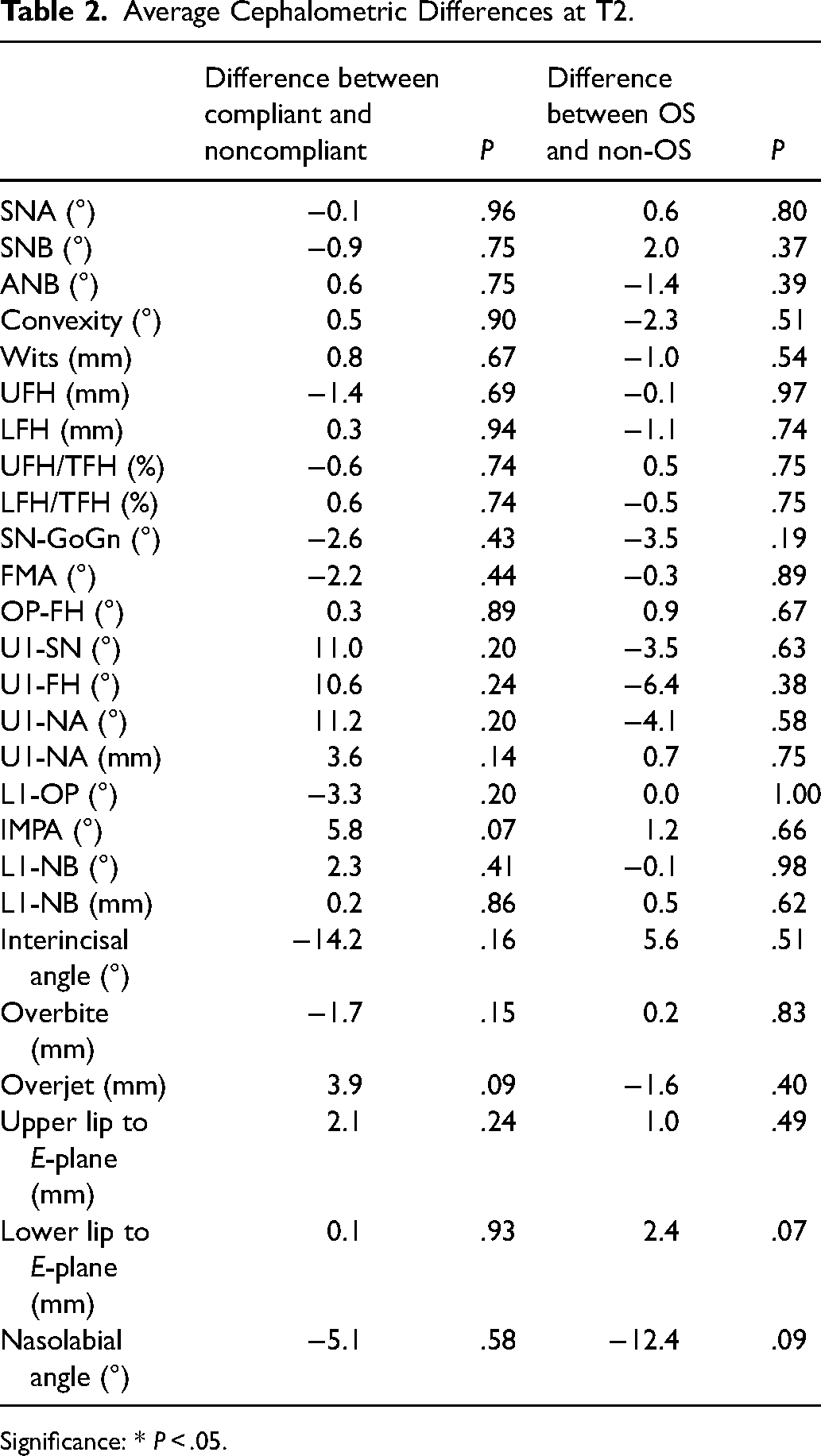
Significance: * P < .05.
At T3, upper incisors are significantly more proclined in the compliant group; specifically, compliant patients had approximately 19° more proclination than noncompliant patients. Patients that needed OS presented significantly more Class III with a deep vertical pattern compared to non-OS patients (Table 3).
Average Cephalometric Values at T3.
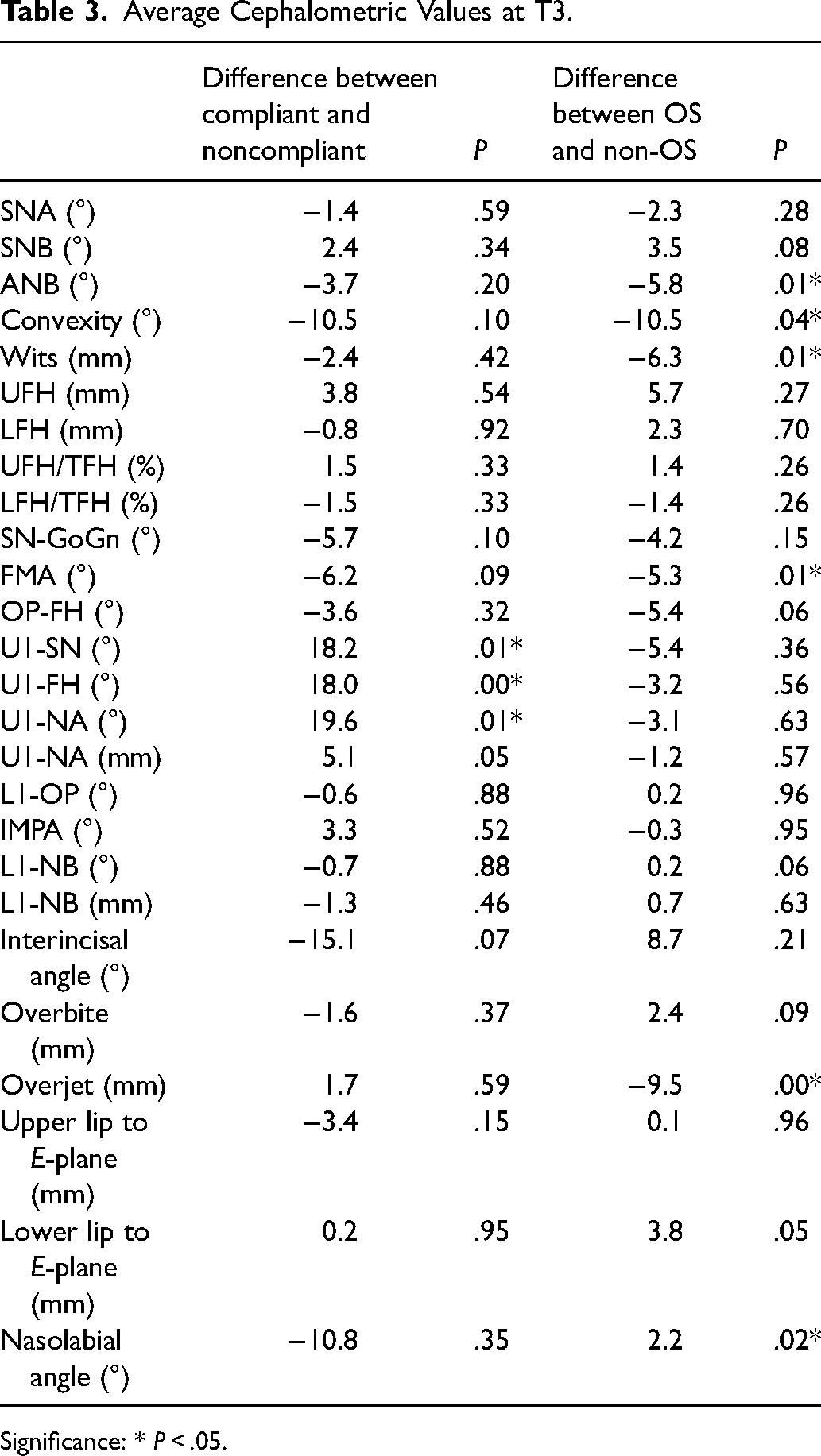
Significance: * P < .05.
Compliant patients showed favorable changes in anteroposterior (AP), proclined upper and retroclined lower incisors, opening of MPA, and retrusion of lower incisors with PHG. During fixed appliances, there was an unfavorable relapse in ANB, convexity, Wits, and overjet, anterior facial heights increased, MPA deepened, and upper incisors proclined and protruded further. Overall, compliant patients became more Class III attributable to the combination of maxillary retrusion and mandibular prognathism, MPA deepened, upper incisors proclined, lowers incisors retroclined, and upper lip further retruded (Table 4).
Changes in Patients Compliant and Noncompliant with PHG Therapy.
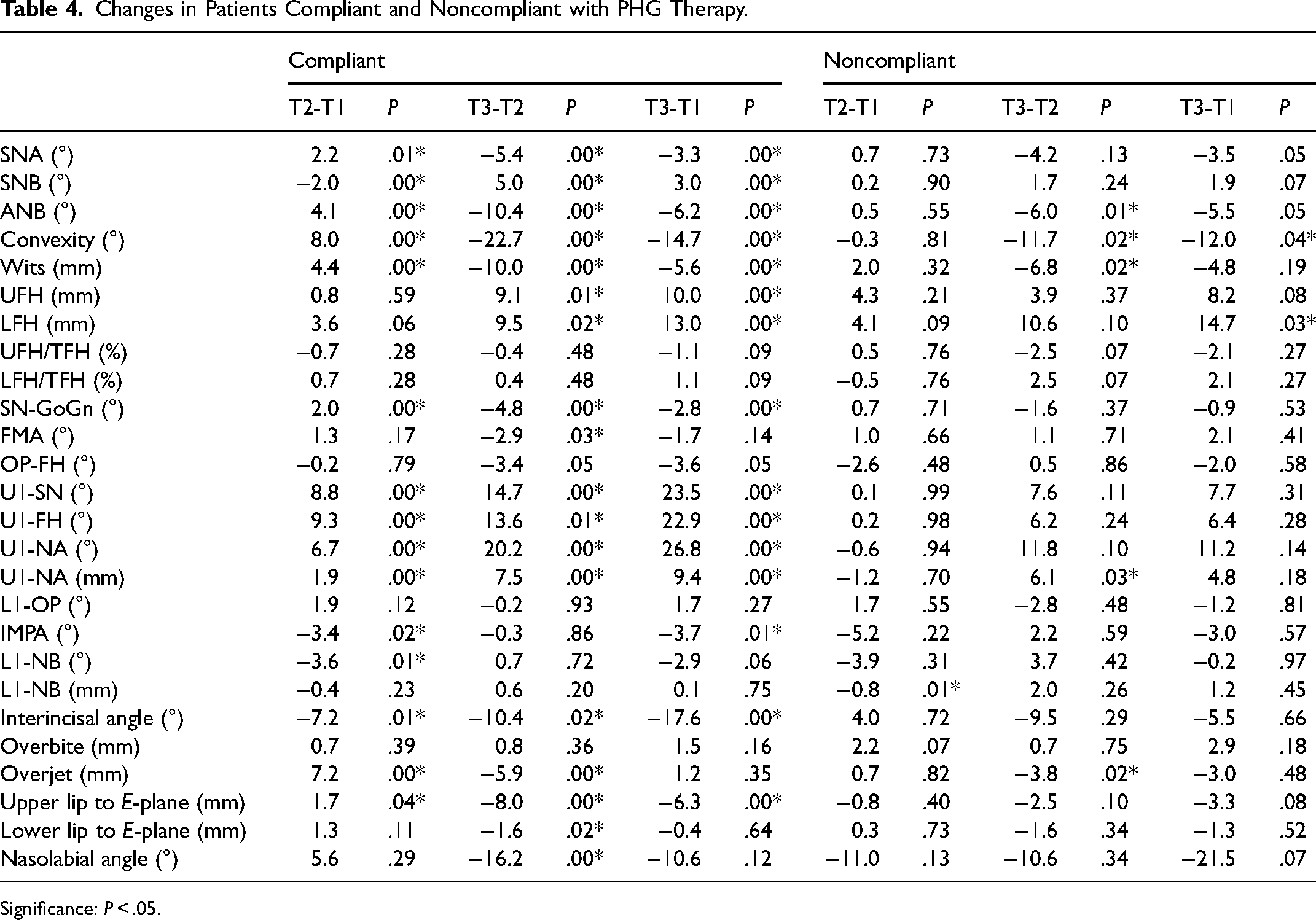
Significance: P < .05.
For noncompliant patients, PHG retruded lower incisors. During fixed appliances, unfavorable changes were observed in ANB, convexity, Wits, and overjet and upper incisor protruded. Overall, noncompliant patients had decreased convexity and increased lower facial heights (Table 4).
OS patients showed favorable changes in AP, proclined upper and retroclined lower incisors, slight opening of MPA, and retrusion of lower incisors with PHG. During fixed appliances, there was unfavorable relapse in AP measurements, anterior facial heights increased, MPA deepened, and upper incisors proclined and protruded further. Overall, OS patients became more Class III attributable to the combination of maxillary retrusion and mandibular prognathism, MPA deepened, upper incisors proclined and lowers retroclined, and upper lip further retruded (Table 5).
Changes in Patients That Did and Did Not Need OS.
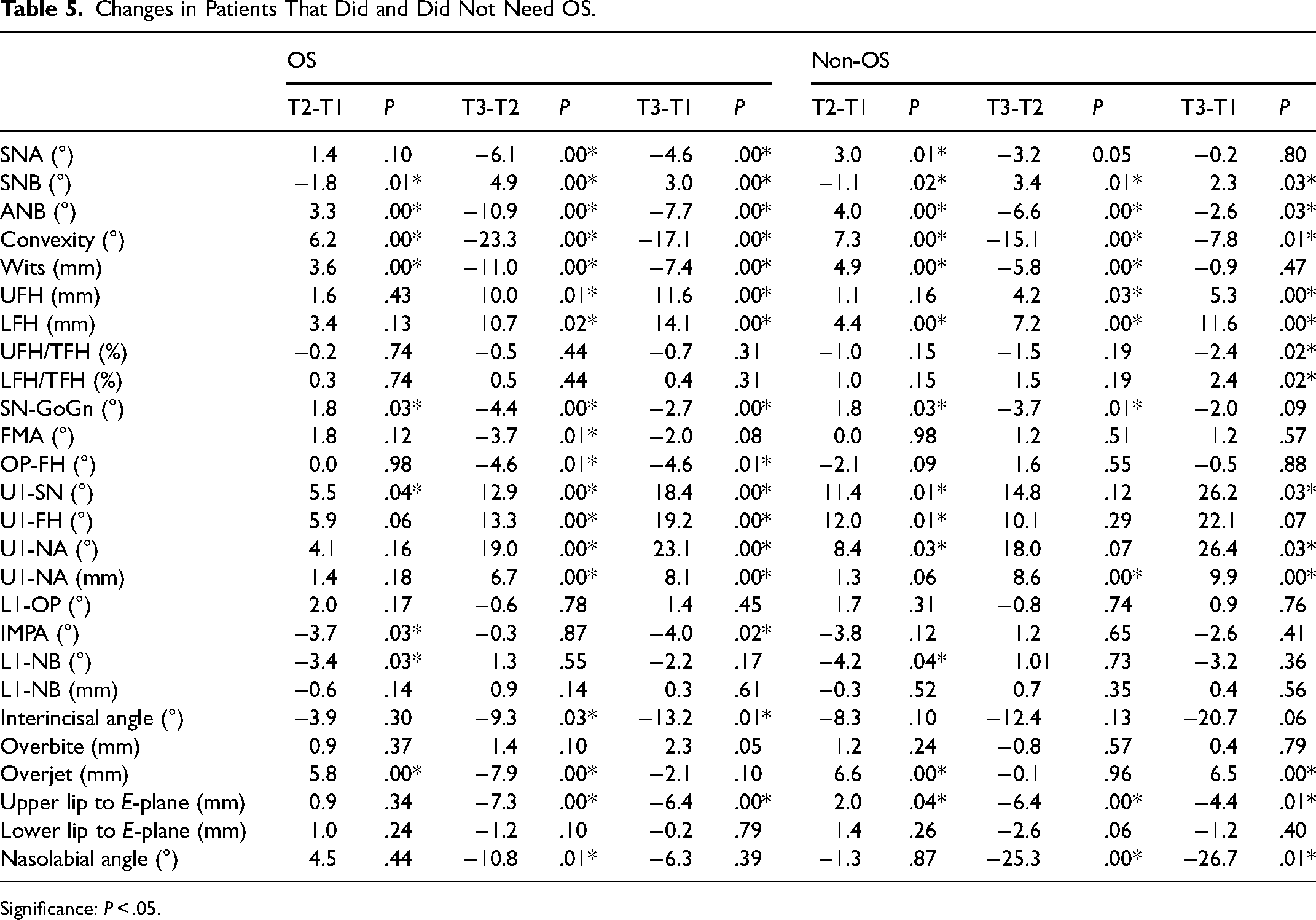
Significance: P < .05.
Non-OS patients showed favorable changes in AP, proclined upper incisors, slight opening of MPA, and retrusion of lower incisors with PHG. During fixed appliances, unfavorable relapse occurred in AP measurements, anterior facial heights increased, SN-GoGn deepened, upper incisors protruded, and nasolabial angle became more acute. Overall, despite measurements indicating increased mandibular prognathism, upper incisors proclined and protruded with a 6.5 mm increase in overjet, and the upper lip became more acute. Additionally, the lower facial height ratio significantly increased without significant mandibular rotation (Table 5).
Discussion
Our results demonstrate favorable responses in the maxilla and mandible to PHG to improve the Class III skeletal relationship as well as upper incisor proclination and clockwise mandibular rotation. Palikaraki et al reports similar skeletal responses to PHG among patients with UCLP with or without expansion and showed approximately 2° improvements in SNA and SNB, 4° change in ANB, and 2° increase in MPA. 28 These changes are in concordance with short-term effects of PHG in young patients without CLP. 16 Proclination of the upper incisors is also significant post-PHG in both our sample and in the literature for patients with and without CLP.15,17,20,21 Upper incisors that are excessively proclined may compensate and camouflage maxillary retrognathia and may not be the desired treatment goal for PHG. However, patients with CLP often present with retroclined upper incisors partly attributable to surgical lip repair. Our patients experienced an average of 11° of proclination with PHG and this helped to improve the upper incisor relationship relative to the maxilla.
Despite improvements with PHG, significant relapse and unfavorable changes were observed. Regardless of compliance, 70% of our patients were treated with OS. There are few studies on the long-term effects of PHG and its correlation with OS. Susami et al observed a large variation in the long-term response of PHG in patients with UCLP; 5 out of 11 patients needed OS. 8 In comparison to those without CLP, post-pubertal treatment effects of PHG in patients without CLP reported 68% to 76% maintaining positive overjet 5.5 to 6 years post-treatment.14,18,20 25% to 33% relapse into negative overjet with exceeding pubertal mandibular growth. 20 Westwood et al suggest that though Class III characteristics may relapse post-treatment, 93% of skeletal changes that occurred prior to the pubertal growth spurt are maintained through skeletal maturity with no significant cephalometric changes. 14 The prognosis of PHG appears favorable for those without CLP, however, more studies are needed to assess the long-term prognosis of PHG among patients with CLP.
Compliance with PHG among our patients did not have a significant impact on the likelihood of OS. Patients experienced a relapse in ANB, convexity, Wits, and overjet. Compliant patients appear to have more relapse and overall unfavorable changes in AP and vertical dimensions with increased incisor proclination that are clinically relevant despite lack of statistical significance. The vector of pull with PHG often encourages both forward and downward movement of the maxilla; however, Wells et al suggested that the subsequent mandibular rotation from downward movement of the posterior maxilla may be associated with increased late horizontal mandibular growth that would worsen the Class III relationships. 21 This suggests for increased focus on vertical control during PHG. OS patients experienced significant counterclockwise rotation of the mandible from T1 to T3 and more forward growth at the condyle with a horizontal projection of the mandible. Non-OS patients showed a significant increase in LFH/TFH ratio and more backward growth at the condyle with backward rotation of the mandible (Figure 2). 29 These observations suggest that the mandibular growth pattern contributes a role in the prognosis of PHG. Patients with vertical growth patterns may observe less relapse and better prognosis with PHG.
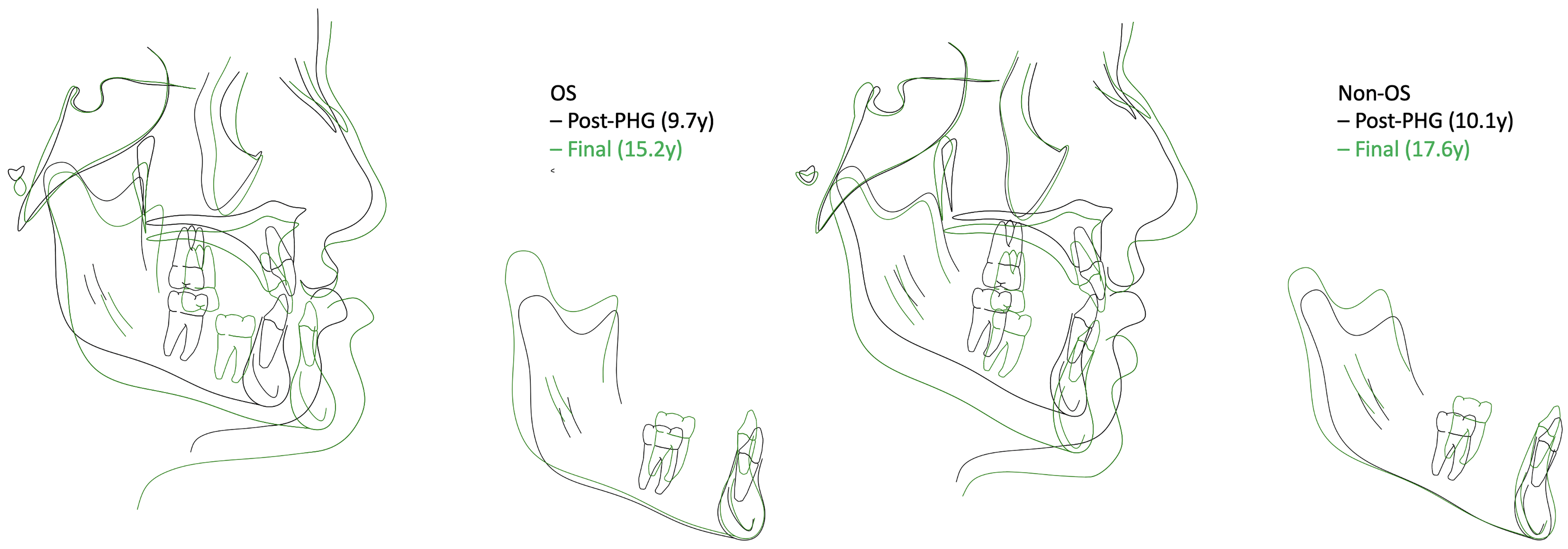
Cranial base and mandibular superimpositions of a representative OS and non-OS patients from T2 to T3. Representative patients demonstrating Class I skeletal and dental relationships with positive overjet post-PHG. Significant horizontal mandibular growth with counterclockwise rotation contributing to relapse of overjet and worsening of Class III relationships. Non-OS patients experienced more vertical mandibular growth with less counterclockwise rotation. Though non-OS patients experienced unfavorable AP changes during fixed appliances, vertical growth patterns helped to increase LFH/TFH and insignificant mandibular rotation was observed overall.
In addition to compliance, there are other considerations in the success of PHG for patients with CLP. Our patients used PHG until 3 mm of OJ was achieved, however, others incorporated overcorrection of 5 to 8 mm OJ with Class II molar relationship. 14 This amount of overcorrection may account for anticipated relapse that occurs with PHG. Class III elastics may be used when PHG is not worn as well as using Class III elastics post-PHG and throughout fixed appliances for retention. 30 Bone-anchored maxillary protraction (BAMP) is an alternate option for patients with maxillary retrognathia older than 10 years of age. Studies suggest that BAMP among patients with UCLP offers more skeletal effects, including forward movement at the zygomatic arches, minimal to no mandibular clockwise rotation, treatment starting closer to pubertal age, and method for retention with Class III elastics without adverse dental effects.31,32 Moving forward, modifying our protocol to incorporate overcorrection, retention, or surgical intervention with BAMP may be considered.
Limitations
This study included male and female patients starting PHG at age 10.5 and under with either UCLP or BCLP indicating that these results may be representative, however, the results should be applied with caution given the study's limitations. Patients with different expansion appliances and protocols and 26% of patients with no expansion were included in this study due to difficulties in obtaining a large sample. This may introduce confounding factors. Studies have shown that rapid palatal expansion disrupts circumaxillary sutures and its use prior to PHG may facilitate maxillary protraction.15,33 However, recent data suggests that there are no significant improvements of maxillary protraction with additional expansion.16,17 Alternating rapid maxillary expansion and constriction with a palatal expander has been used in patients with CLP prior to maxillary protraction with stable results.30,34 There was no clinically significant difference in maxillary protraction and rotations of the palatal and mandibular planes when compared to standard expansion protocols. 35 Another limitation is the lack of a control group with no treatment and another cohort of patients that did not receive PHG. This would have provided data representing skeletal measures that occur with and without fixed appliances prior to orthognathic surgery and further clarify the effects of PHG. Additionally, cephalometry presents limitations such as magnification, distortion, and proper patient positioning that could alter the data as not every patient was not standardized into centric relation prior to creating the cephalometric images. 36 Furthermore, the sample is limited in size and documented from a single center. Given proper standardization of protocols and outcomes, data from other centers that provide similar treatments would have strengthened the study.
Conclusion
Compliance with PHG was not associated with a decreased need for OS. However, it improved upper incisor proclination and protrusion for patients with CLP. Non-OS patients demonstrated a vertical pattern of growth that was not associated with OS. Future studies will be directed at recruiting a larger study population and identifying primary predictor variables for decreasing the need for OS among patients with CLP.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.