
Abstract
Objective
To investigate the craniofacial growth outcomes of early secondary alveolar bone grafting(ABG) around 6 years of age.
Design
Retrospective cohort study
Setting
1 North-American and 5 Northern-European cleft centers.
Subjects
33 subjects with CUCLP consecutively treated with secondary ABG around 6 years of age were compared to 105 subjects from 4 centers treated with late secondary ABG and 19 subjects from 1 center with primary ABG.
Methods
Preorthodontic standardized lateral cephalometric radiographs taken after 12 years of age were traced and analyzed according to the Eurocleft Study protocol. Fourteen angular and two proportional measurements were performed. Measurement means from the Study Center(SC) were compared to 5 Northern-European centers using analysis of variance and Welch's modified t-tests, and P < .05 was considered statistically significant.
Results
For the SC, the mean age ± SD at the time of bone graft was 5.85 ± 0.71 years and the mean age at the time of the lateral cephalogram was 13.4 ± 1.8 years. The sagittal maxillary prominence of the SC was favorably comparable to the 5 Northern-European centers. The mean SNA (78.1 ± 4.3) for the SC was significantly higher compared to 4 of the 5 Northern-European centers(all P < .05), and the mean ANB angle was comparable to 4 of the 5 centers. Similarly, the mean soft tissue ANB angle was not significantly different to the 5 centers. The soft tissue vertical proportions compared favorably to all 5 Northern-European centers(all P < .01).
Conclusions
Craniofacial growth outcomes of early secondary ABG around 6 years compare favorably to the outcomes of late secondary ABG.
Introduction
Reconstruction of the alveolar cleft is a requirement for patients with congenital complete unilateral cleft lip and palate (CUCLP). Alveolar bone grafting (ABG) also is necessary to provide sufficient bone stock for eruption and periodontal support of the cleft-adjacent teeth; achieve closure of any vestibular and palatal oral nasal fistulae; establish nasal skeletal base, floor of the nose and functional nasal airway; and provide adequate bone stock for the future placement of an osseointegrated dental implant in cases where the permanent lateral incisor is missing and replacement is needed. 1
Primary ABG is defined as a graft placed before 2 years of age. Most cleft centers have abandoned primary ABG due to its association with restricted anterior-posterior (A-P) maxillary growth.2–4 Secondary ABG has traditionally been timed prior to the eruption of the cleft-adjacent canine. 5 These secondary grafts occurring between the ages of 9 and 11 years of age have been shown to minimally impact maxillary growth.6–8 Delaying the ABG until 9 years of age however ignores both the eruption and prognosis of the cleft-adjacent incisors. This delay can compromise the periodontal status and lead to poor balance of clinical crown height and poor crown-to-root ratio for the maxillary central incisor. 1
Timing the secondary ABG prior to eruption of the cleft-adjacent maxillary central incisor can prevent the compromised bony and periodontal status of the incisor. This early secondary ABG occurring closer to 6 years of age has been shown to optimize the soft and hard tissue periodontal health and support of all cleft-adjacent permanent teeth 1 while also providing adequate bone stock. 9 The main concerns and criticisms associated with early secondary ABG around 6 years of age have been related to maxillary growth. Some authors have reported potential maxillary growth restriction similar to primary ABG, 10 while others have reported that it does not compromise anterior maxillary growth. 11
The purpose of this study was to compare the craniofacial growth following early secondary ABG around 6 years of age to the craniofacial growth outcomes from the Eurocleft data where the ABGs were performed around 9 years of age in 4 centers and at 5 months of age in 1 center. Our hypothesis is that the maxillary growth for patients with CUCLP will be similar for early secondary ABG versus late secondary ABG.
Methods
This retrospective cohort study reviewed available clinical records for subjects with CUCLP who were consecutively treated with secondary ABG around 6 years of age at the Cleft and Craniofacial unit of the Study Center (SC) between January 1996 and January 2008. The study was approved by the IWK Health Center Research Ethics Board.
The inclusion criteria of the SC were: Caucasian, non-syndromic CUCLP, longitudinal follow-up of a minimum of 12 years of age, secondary ABG around 6 years of age, and all ABG performed sequentially, by the same surgeon, using the same surgical technique. 1
The exclusion criteria of the SC included: syndromic clefts, incomplete clefts, bilateral cleft lip and palate, primary alveolar bone grafting, incomplete records, and patients lost to follow-up. None of the subjects in the SC had any pre-grafting orthodontic expansion or other orthodontic treatment.
The craniofacial growth of subjects in the SC was compared to that of the 5 other Northern European cleft centers from the Eurocleft Study.12,13 The inclusion and exclusion criteria for the Eurocleft Centers are described in. 13 The treatment protocol for each center is summarized in Table 1.
Treatment Protocols for the Study Center and Eurocleft Centers a .
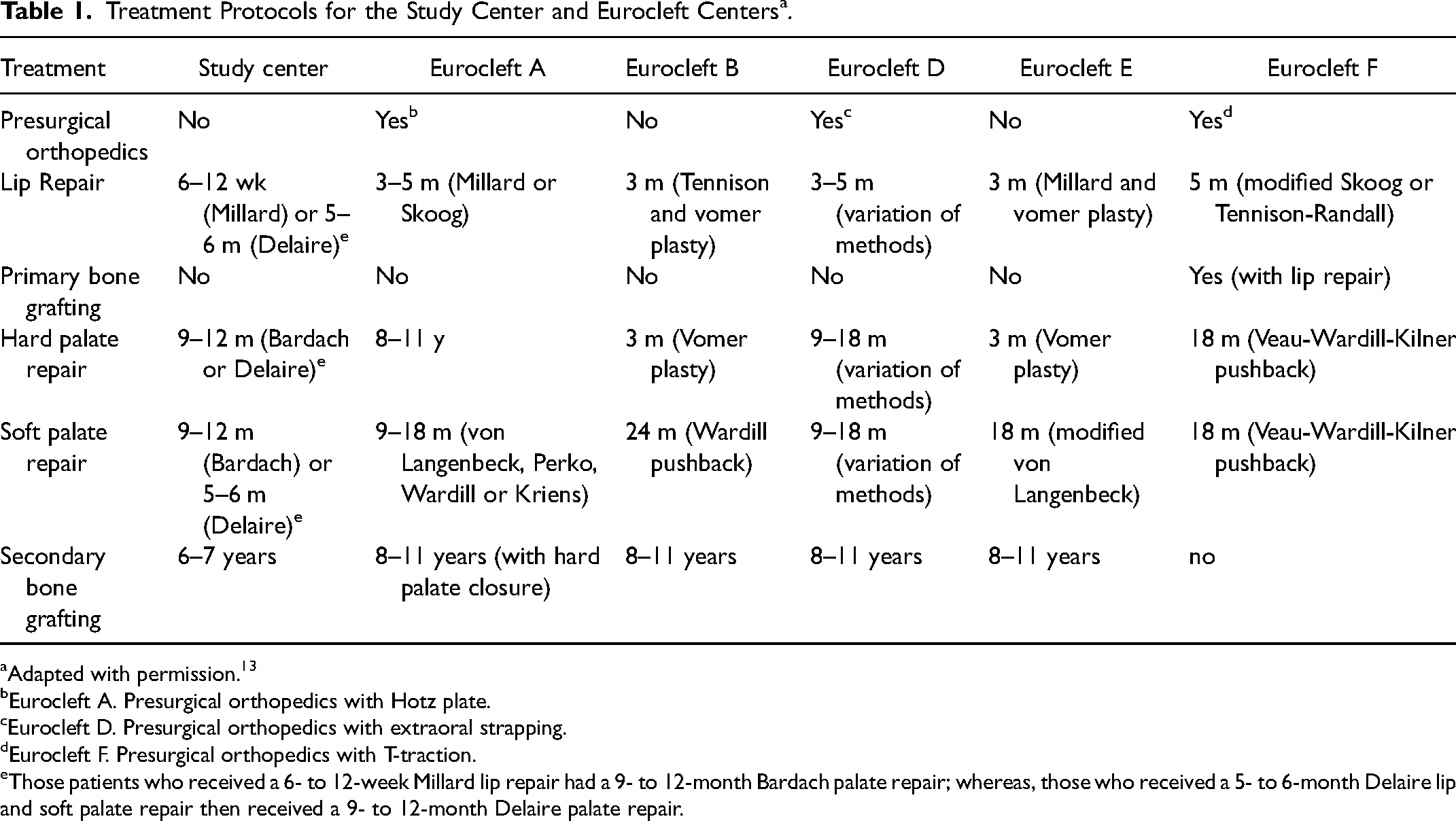
Adapted with permission. 13
Eurocleft A. Presurgical orthopedics with Hotz plate.
Eurocleft D. Presurgical orthopedics with extraoral strapping.
Eurocleft F. Presurgical orthopedics with T-traction.
Those patients who received a 6- to 12-week Millard lip repair had a 9- to 12-month Bardach palate repair; whereas, those who received a 5- to 6-month Delaire lip and soft palate repair then received a 9- to 12-month Delaire palate repair.
Cephalometric Analysis
Preorthodontic standardized lateral cephalometric radiographs taken with the teeth in occlusion were traced and analyzed according to the Eurocleft Study protocol 12 using the Dolphin© Software (Version 1.6.3861.20105). All radiographs were analyzed and interpreted by two professionals with over two decades of experience in tracing cephalograms of patients with CLP.
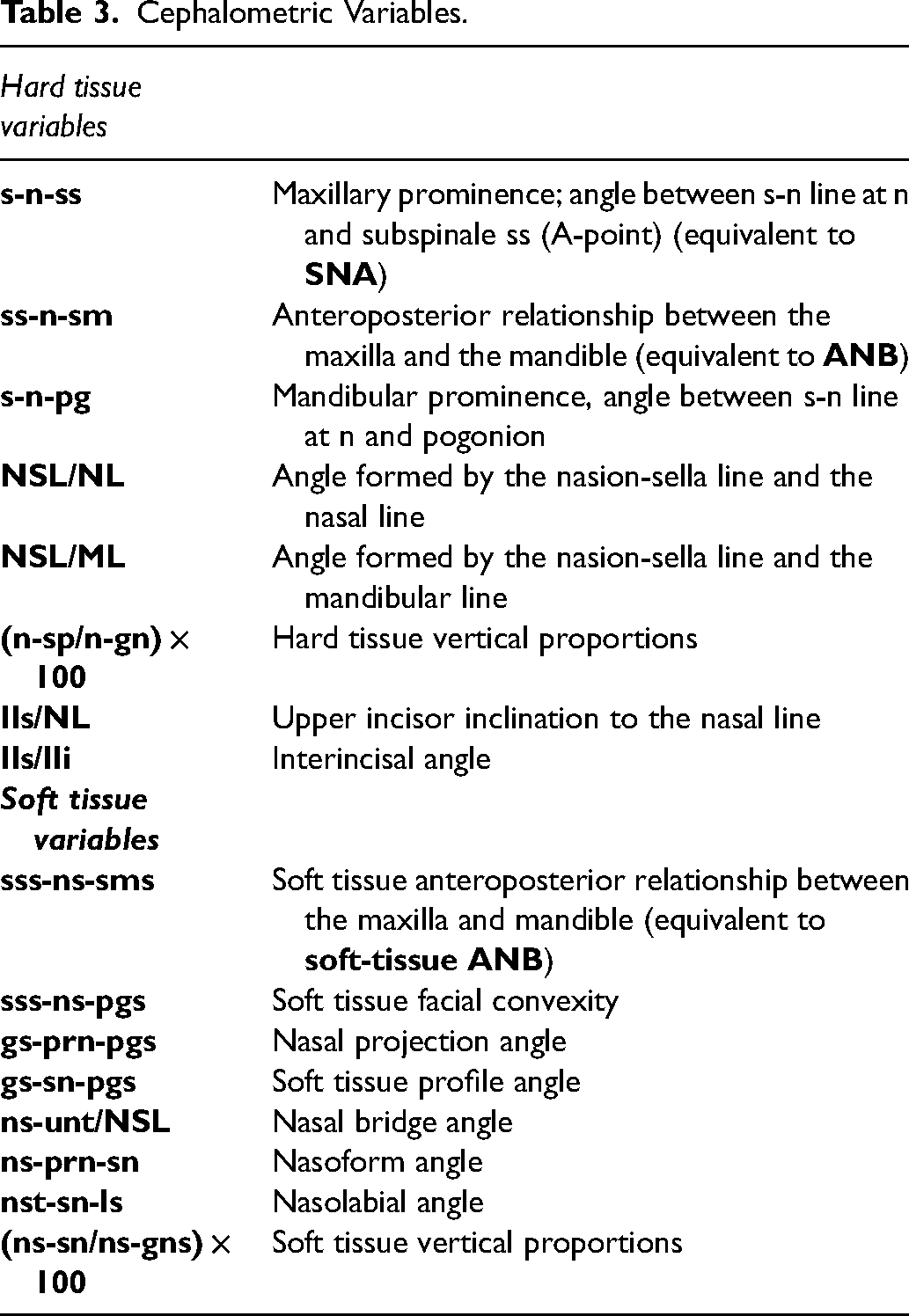
Fifteen hard tissue and 12 soft tissue landmarks and 5 skeletal reference lines based on the original Eurocleft study were identified on each lateral cephalometric radiograph (Figure 1 and Table 2). 12 From these landmarks, 14 angles and 2 proportions were analyzed and compared to those from the 5 Eurocleft centers (Table 3). Only angular and ratio measurements were used to minimize errors related to the radiographic equipment and differential magnification.
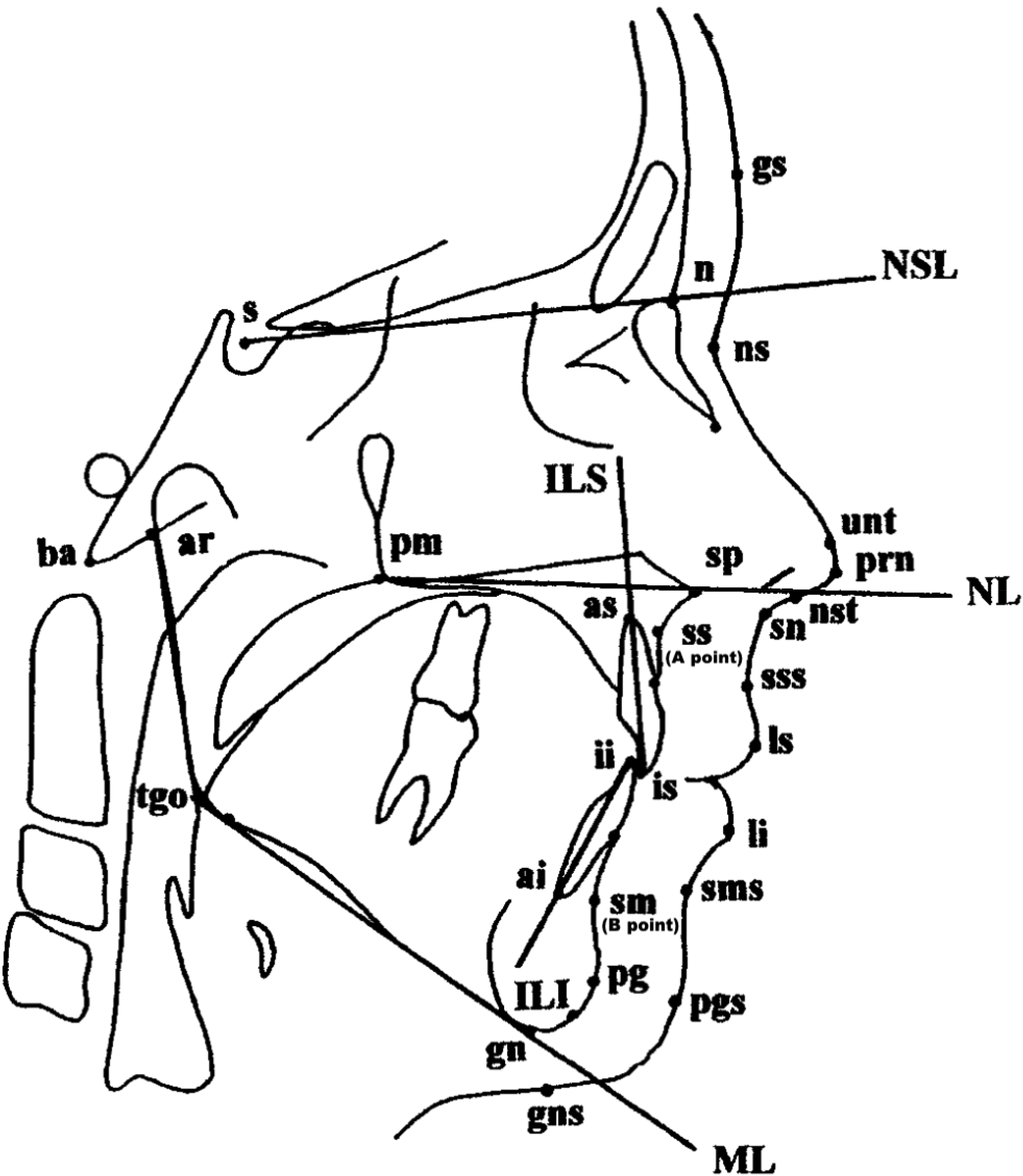
Lateral cephalometric landmarks*. *Adapted with permission. 12
Cephalometric Landmark Definition a .
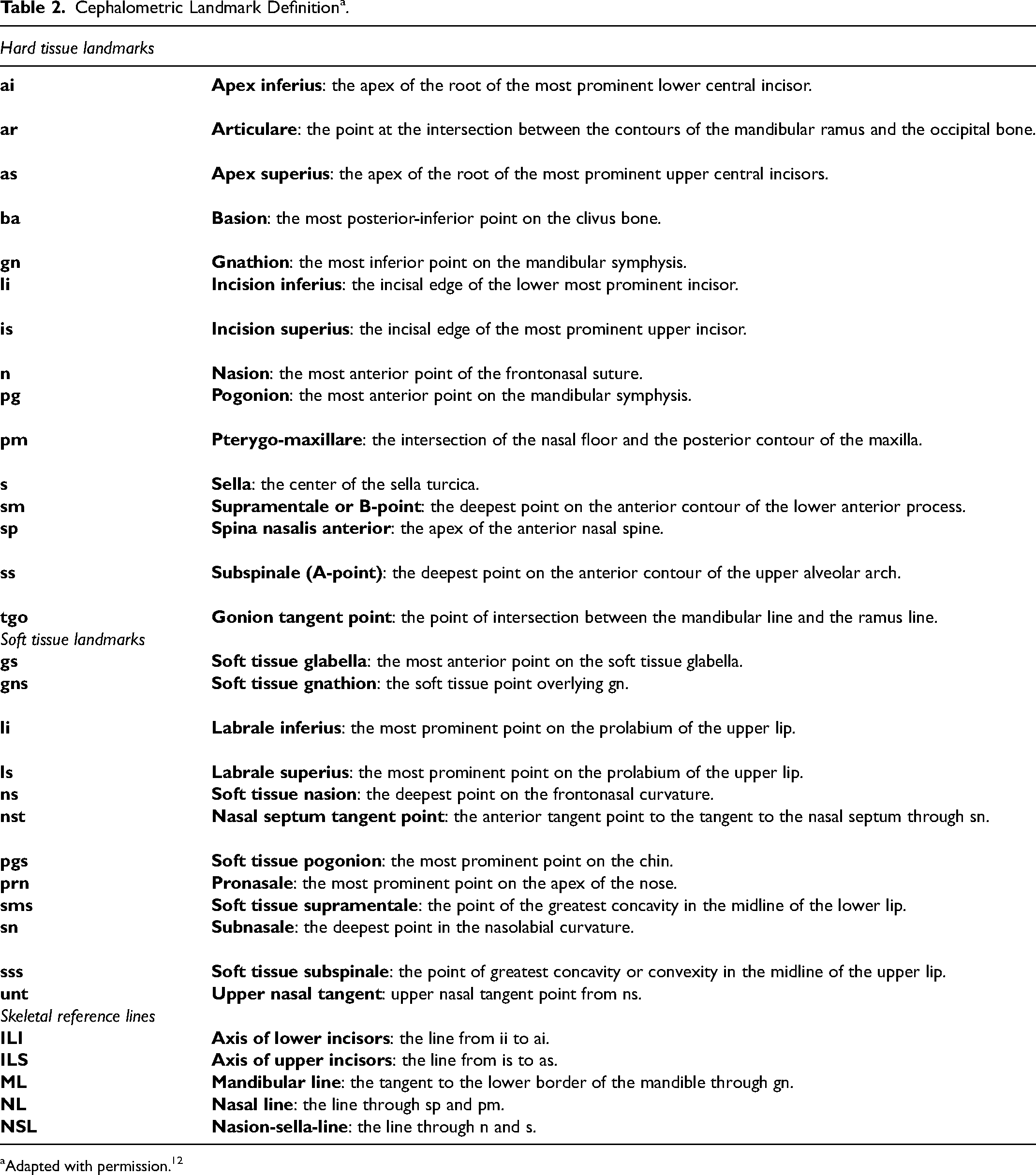
Adapted with permission. 12
Cephalometric Variables.
Statistics
Sample sizes in the range of 30 to 40 were sought according to the findings of the original Eurocleft Study, 14 and Americleft Study15,16 for retrospective cohort studies of this type.
Statistical analysis was performed using the Statistical Package for Social Sciences software (SPSS.22.0, Chicago, IL). Intrarater and interrater reliability for the cephalometric analysis were determined using Intraclass Correlation Coefficient (ICC) statistics. For the intra-rater reliability, 10 cephalograms from the SC were randomly selected and retraced after the original tracing after a 1 week time period. Measurement means of each center were compared using analysis of variance (ANOVA) and Welch's modified t-tests. For all statistical tests, a 95% confidence interval (CI) was used, and P < .05 was considered statistically significant.
Results
Thirty-nine patients with CUCLP were identified at the SC. Six patients were excluded due to incomplete records or loss to follow-up, leaving 33 patients that met the inclusion criteria. The demographics of the Study center (SC) and the 5 Eurocleft centers are presented in Table 4.
Demographics of the Study Center and Eurocleft Centers.
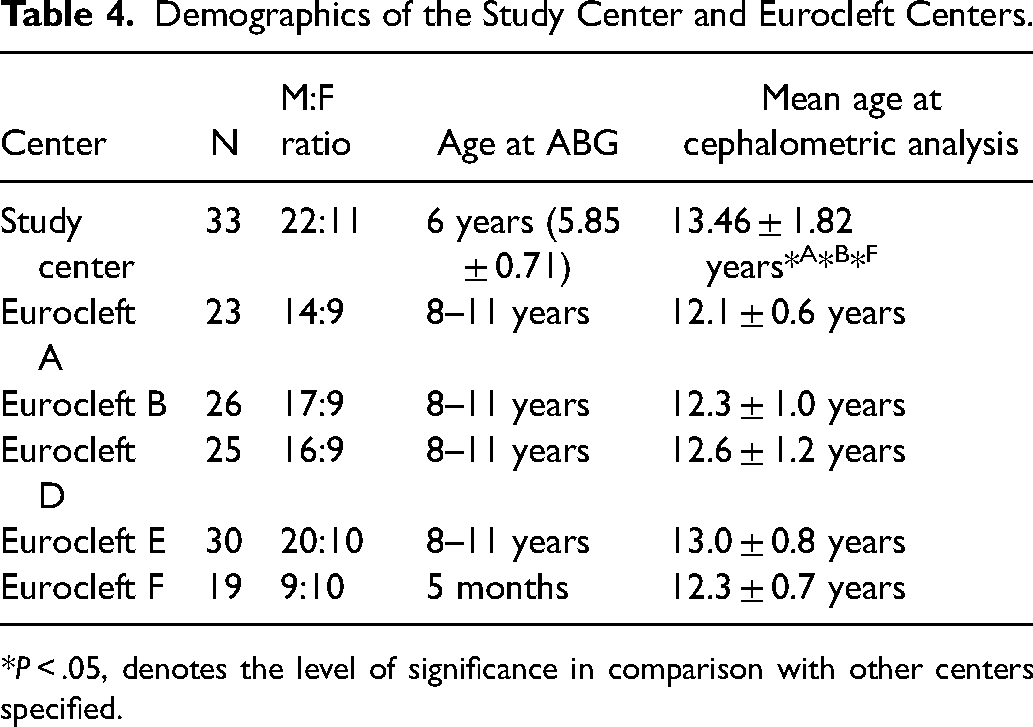
*P < .05, denotes the level of significance in comparison with other centers specified.
Intrarater and interrater reliabilities for the cephalometric analysis were very good to excellent with ICCs ranging from 0.943 to 0.996 and 0.839 to 0.980 respectively.
The results of the cephalometric comparisons between the six centers is shown in Table 5.
Mean Values ± SD for the Hard and Soft Tissue Measurements.
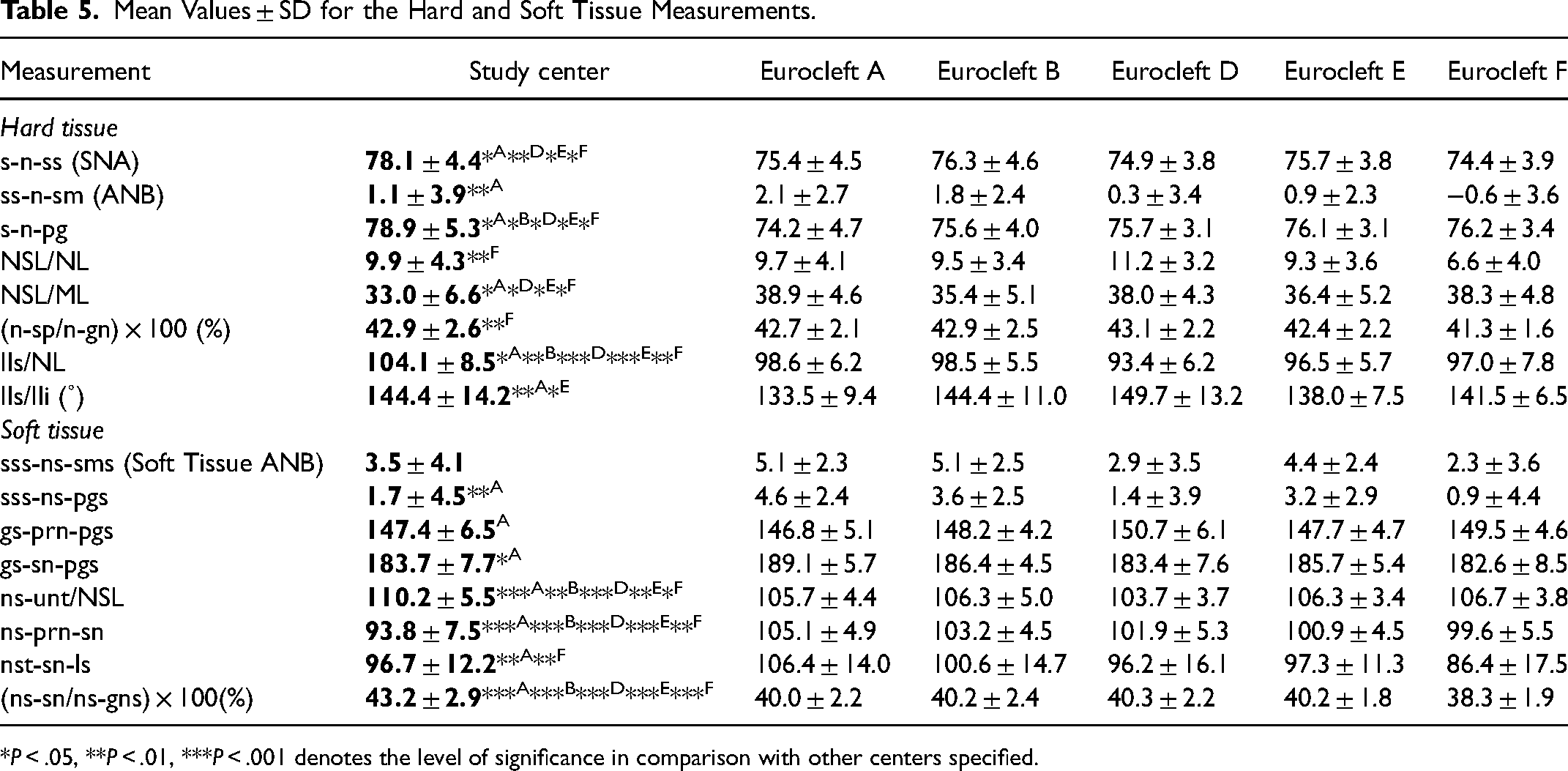
*P < .05, **P < .01, ***P < .001 denotes the level of significance in comparison with other centers specified.
Hard Tissue Variables
Sagittal dimensions
The sagittal maxillary prominence (s-n-ss or SNA) of the SC was significantly greater than in the Eurocleft centers (all P < .05) except for Center B (Table 5). The sagittal jaw relationship (ss-n-sm or ANB) was comparable to all Eurocleft centers except for Center A which had a significantly higher angle (Table 5).
Vertical dimensions
The maxillary inclination (NSL/NL) of the SC was similar to the other Centers, except for Center F that showed a significantly lower maxillary inclination (P < .01). Similarly, the facial proportions ([n-sp/n-gn] × 100) were comparable between the SC and Eurocleft centers, except for Center F that showed significantly less harmonious proportions (P < .01). Otherwise, the overall vertical growth of the SC, when evaluated by the NSL/ML angle, was significantly different than the Eurocleft centers (P's < .05), except for Center B.
Dentoalveolar variables
The maxillary incisor inclination (ILs/NL) for the SC was significantly greater than for the Eurocleft Centers (all P's < .05) The interincisor angle (Ils/Ili) was significantly more obtuse in the SC compared with Centers A and E (both P's < .05), but comparable to Centers B, D and F.
Soft Tissue Variables
Sagittal dimensions
The sagittal relationship (sss-ns-sms or soft tissue ANB) were similar between the SC and Eurocleft Centers. The soft tissue facial convexity and profile angle were also comparable between the SC and the Eurocleft centers, except for Center A that showed higher sss-ns-pgs and gs-sn-pgs values (both P's < .05).
Vertical dimensions
The soft tissue vertical proportions ([ns-sn/ns-gns] × 100) was significantly more favorable for the SC compared to the Eurocleft centers (all P's < .001).
Nasal dimensions
The nasal projection angle (gs-prn-pgs) was comparable between the SC and Eurocleft Centers. The nasal bridge angle (ns-unt/NSL) was significantly flatter for the Eurocleft Centers compared to the SC (all P's < .05). The nasoform angle (ns-prn-sn) of the SC was significantly lower than the Eurocleft Centers (all P's < .01). The nasolabial angle (nst-sn-ls) of the SC was significantly lower than Center A (P < .01), significantly higher than Center F (P < .01), and similar to Centers B, D and E.
Discussion
Early secondary ABG around 6 years of age, prior to the eruption of the cleft-adjacent maxillary central incisor, has been advocated to promote the periodontal health of all cleft-adjacent permanent teeth. 1 The main concern with early secondary ABG has been linked to a potential compromised maxillary growth, 10 with effects that may be similar to those associated with primary ABG.2–4 The present study did not confirm this association. On the contrary, this study showed that maxillary growth of patients with CUCLP treated with early secondary ABG around 6 years compared favorably with maxillary growth of patients from centers where grafting occurred after 8 years of age.
The sagittal maxillary growth of patients with CUCLP grafted around 6 years of was not compromised compared with the other cleft centers. The maxillary prominence of the SC, when measured with the s-n-ss (SNA) angle was significantly greater than all other Eurocleft Centers, except for Center B. The sagittal jaw relationship of the SC, when measured with the ss-n-sm (ANB) angle or the sss-ns-sms (soft tissue ANB) angle was similar to the other Eurocleft Centers, except for Center A that also had a significantly higher ss-n-sm angle. These findings have also been supported by previous studies.11,17,18 Siegenthaler et al. in 2018 compared patients with CUCLP (36 early ABG to 56 late ABG) and showed that ABG carried out between 2 and 4 years of age showed no significant negative impact on the dental arch relationship at age 10 years. Doucet et al. in 2019 showed that the antero-posterior maxillary growth of patients with CUCLP who received early secondary ABG was not compromised compared to 4 Americleft Centers that used late secondary ABG. Similarly, Brudnicki et al. in 2020 retrospectively reviewed 128 consecutively treated patients with nonsyndromic CUCLP who received secondary ABG between 1.4 to 11.5 years of age, and demonstrated no association between the timing of the ABG and the SNA at 10 years of age.
Early secondary ABG around 6 years of age did not negatively influence vertical maxillary growth in this study. The maxillary inclination and vertical proportions of the SC were comparable to the Eurocleft Centers, except for Center F that showed less favorable vertical growth. The soft tissue vertical proportions of the SC were also found to be more favorable than all of the Eurocleft centers. Brudnicki et al. in 2017 also showed that the upper anterior facial height and vertical dimensions were comparable between patients with CUCLP grafted at 2.5 years and 9.8 years of age. 19 Similarly, Doucet et al. in 2019 showed that the vertical maxillary growth of patients with CUCLP treated with ABG at 6 years was comparable to 4 Americleft centers that performed late secondary ABG. 11
The deleterious effect of primary bone grafting on maxillary growth was again highlighted in this study. Center F, that performed primary ABG, showed the least favorable sagittal and vertical proportions compared to all other centers. These results reinforce the findings of previous studies2–4,12,20 confirming that the negative impact of primary ABG on maxillary growth is not seen with early secondary ABG.
Early secondary ABG has numerous other advantages. It provides better periodontal support to the cleft side central and lateral incisor (if present).1,21 Precious in 2009 showed that early secondary ABG provided almost normal symmetry of clinical crown length of the cleft and non-cleft erupted permanent maxillary central incisors, while the cleft side central incisor clinical crown height was 25% longer with late secondary ABG. Early secondary ABG also provides reliable bone stock as shown with SWAG (Standardized Way to Assess Grafts) scores comparing favorably with centers performing late secondary ABG.9,11,22,23 Early secondary ABG has also been associated with decreased operative times and decreased burden of treatment for the patients.18,21,24 Furthermore, the procedure is typically carried out before / without prior arch expansion shortening the amount and duration of orthodontic treatment. 1
The main limitation of our study was its retrospective nature and associated biases. To diminish these, a sample of consecutively treated patients with CUCLP was used minimizing selection biases. The inclusion criteria and sample size were comparable with the Eurocleft and Americleft studies. The sample size also was within the recommended range of 30 to 40 based on the findings of the Eurocleft 14 and Americleft studies.15,16 The mean age of the Study Centre was also higher than Eurocleft Centers A, B and F which could have potentially influenced the results. To minimize this effect, we used angular measurements and ratios in our analysis. Furthermore, the intrinsically different and varied underlying skeletal facial growth pattern of the samples was not accounted for in this study. The study also did not control for other protocol-related differences among the centers, such as the surgical techniques and timing, the number of surgeons, and the use of presurgical orthopedics that can all potentially influence maxillary growth. Of note is that the SC only had one surgeon, utilizing one surgical technique, and no presurgical orthopedics. Additionally, the present study did not evaluate transverse maxillary growth.
Conclusions
Early secondary alveolar bone grafting around 6 years does not negatively influence maxillary growth. The craniofacial growth outcomes at the mean age of 13.5 years compare favorably to or better than the outcomes of late secondary ABG performed around 9 years of age. Further controlled prospective studies evaluating transverse maxillary growth as well as the sagittal and vertical maxillary position at completion of facial growth are warranted.
Footnotes
Acknowledgments
The authors would like to acknowledge Nicholas Emanuele, DDS, BSc; Lindsay James, BSc, and Jennifer Fessler, MSW for their contribution.
Author Note
This article was presented, in part, at the American Cleft Palate– Craniofacial Association meeting in Atlanta, GA, April 2016.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Faculty Research Grant Dalhousie Dentistry, Subtelny Orthodontic Clinical Research Grant. This study was funded in part by the 2014 Subtelny Orthodontic Clinical Research Grant from the Cleft Palate Foundation and by a Faculty Research Grant from the Faculty of Dentistry, Dalhousie University, Halifax, Canada.