
Abstract
Objective
While knowledge of the psychosocial impact of craniofacial conditions is growing, literature regarding the impact on parents remains limited. Parents of children born with a health condition may be at risk of experiencing a range of psychosocial challenges. This study conducted an initial investigation of psychosocial adjustment of parents of individuals with craniosynostosis to inform support provision for families.
Setting
An online UK-wide mixed-methods survey was distributed to members of Headlines Craniofacial Support.
Design
Quantitative data including standardized measures were analysed using descriptive statistics and independent samples t-tests, and inductive content analysis was used for open-ended questions.
Participants
Mothers (n = 109) and fathers (n = 9) of individuals ages 3 months to 49 years with single suture (63%) or syndromic (33%) craniosynostosis participated.
Results
Compared to the general population, parents of individuals with craniosynostosis reported higher levels of stress, anxiety, and depression; lower levels of resilience and optimism. Qualitative responses provided insight into parents’ experiences of birth, diagnosis, healthcare provision, familial wellbeing, and relationships. Parents reported several unmet information and support needs, alongside a range of positive outcomes.
Conclusions
This study illustrates the potential long-term psychosocial implications for parents raising children with craniosynostosis. There is a need for routine psychological screening for family members and provision of appropriate psychological support for those at risk for distress. Non-specialist health professionals may benefit from additional training about craniofacial conditions so they are better equipped to support and refer families.
Introduction
Craniosynostosis is a craniofacial condition, affecting approximately one in every 2000 live births and occurring when two or more of the cranial plates fuse prematurely (Mathijssen, 2021). This condition presents in various ways and can be isolated, or can be more complex to manage when presenting as part of a broader syndrome, such as, Apert, Pfeiffer, Muenke, Sathre-Chotzen, and Crouzon syndromes (Kajdic et al., 2018). Early surgery is often recommended, and ongoing multidisciplinary treatment may also be indicated, dependent upon the needs of the child.
Having a child with a health condition can have a considerable impact on parents’ mental health and relationships (Cousino and Hazen, 2013). Importantly, research finds that parental psychological distress is a key risk factor for poor medical and psychosocial outcomes in their children (Sanger et al., 2015). Within the craniofacial literature specifically, the possible psychological impact of craniofacial conditions on both affected individuals and their families is becoming increasingly recognized (Nelson et al., 2012; Feragen and Stock, 2017). Whilst the broad evidence base for craniofacial conditions is growing, such as in the case of cleft lip and/or palate (CL/P), the most common craniofacial condition, research specifically related to craniosynostosis remains sparse (Feragen and Stock, 2017). This is particularly notable in the case of the psychosocial wellbeing of parents and the wider family (Feragen and Stock, 2017). The research that is available indicates that parents of children with craniosynostosis may experience a range of challenges and be at risk of adverse outcomes (Feragen and Stock, 2017). For example, in a Swedish qualitative study with 20 parents about their experiences of diagnosis and early care, Zerpe and colleagues (2020) found that most parents had little knowledge about craniosynostosis prior to their child’s diagnosis, and reported many concerns about their child’s treatment and prognosis. Zerpe and colleagues (2020) also reported that parents were disappointed with the care available, particularly in regard to health professionals providing missed/incorrect diagnoses, and the (poor) quality of information the parents had received. In contrast, researchers in the US and Germany have found parents of children with craniosynostosis to be satisfied with the healthcare they had received (Wong-Gibbons et al., 2009; Kluba et al., 2016). While some studies have identified elevated parenting stress in the preoperative period in specific domains of adjustment, including child health and appearance (Rosenberg et al., 2011), a more recent study indicates that parents of children with craniosynostosis are not adversely affected by increased stress over time (Gray et al., 2015). Last, in a Turkish qualitative study by Zeytinoǧlu and colleagues (2021), parents of children with Apert syndrome highlighted experiences of perceived social stigma and negative reactions from others, including members of the public. In their review of the craniofacial literature, Feragen and Stock (2017) concluded that the psychosocial impacts of relatively rare craniofacial conditions, like craniosynostosis, require further investigation, in order to improve information and support.
In the United Kingdom (UK), multidisciplinary, long-term care for those affected by craniosynostosis is delivered by five supra-regional specialist units. Additional community-based support is offered by leading charity, Headlines Craniofacial Support, a UK-wide organisation that became a registered charity in 1996. Over the years, Headlines Craniofacial Support has developed a range of services, including a helpline, a welfare fund, information leaflets, family events, fundraising activities, e-newsletters, and a biennial conference. In 2017, Headlines Craniofacial Support developed a new five-year strategy, of which research is a key component, to ensure the support the charity offers is evidence-based. As part of this review, they also conducted a priority-setting exercise to identify their top 10 questions for future research. Two of these priorities related to psychosocial outcomes: 1) What are the long-term physical and psychological effects for individuals with syndromic and non-syndromic craniosynostosis? and 2) Are individuals with craniosynostosis likely to suffer from mental health difficulties, or are they more resilient (as compared to the general population)?
Given the potential impact of raising a child with a craniofacial condition such as craniosynostosis, it is important to consider not only the wellbeing of the parents themselves, but parental adjustment as an important factor in the long-term development of the child. A better understanding of the challenges that families affected by craniosynostosis experience, in addition to a greater awareness of the information and support that is needed at different time points, would provide stakeholders with directions for future research, as well as service/intervention development and delivery.
The current study aimed to conduct an initial investigation of psychosocial adjustment among parents of individuals with craniosynostosis, via a UK-wide online, mixed-methods survey, with a view to informing psychosocial care provision for the family as a whole.
Method
Design
Ethical approval to conduct the study was obtained from the Faculty Research Committee at The University of the West of England. An online survey (see Table 1), using Qualtrics as a hosting platform, was designed drawing upon current craniofacial literature (e.g Feragen and Stock, 2017). Clinical psychologists from the four specialist units in England, ten adults with craniosynostosis, and eight family members of individuals with craniosynostosis provided feedback on the study design and draft materials at a dedicated research workshop in September 2019.
Full Survey Overview.
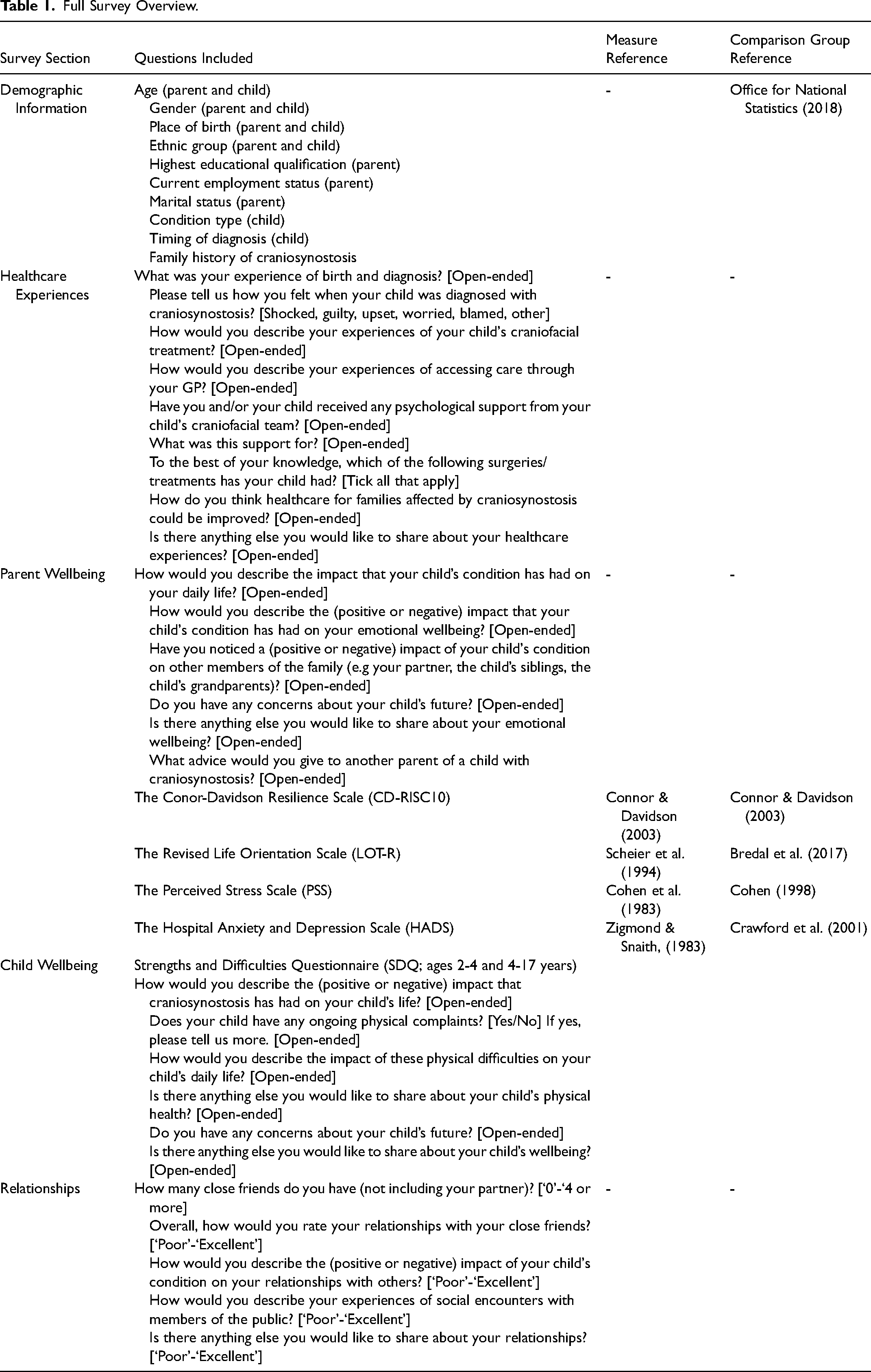
The survey consisted of five standardised parent-reported outcome measures, chosen for their psychometric properties, clinical utility, the availability of general population norms, and for consistency with related studies to allow for comparisons among similar populations (see Stock et al., 2016 for a review). Additional single item questions were included where issues of interest were not captured by standardized measures (see Table 1). Demographic data were also collected (Table 2), alongside open-ended questions for participants to provide more detail if they wished (see Table 1). As part of the survey, parents were asked about their own and their child’s wellbeing. A version of the survey was also administered to adults with craniosynostosis. The current paper presents the findings on parents’ wellbeing only. Other results are presented in separate papers (Stock et al., 2021).
Demographic Information.
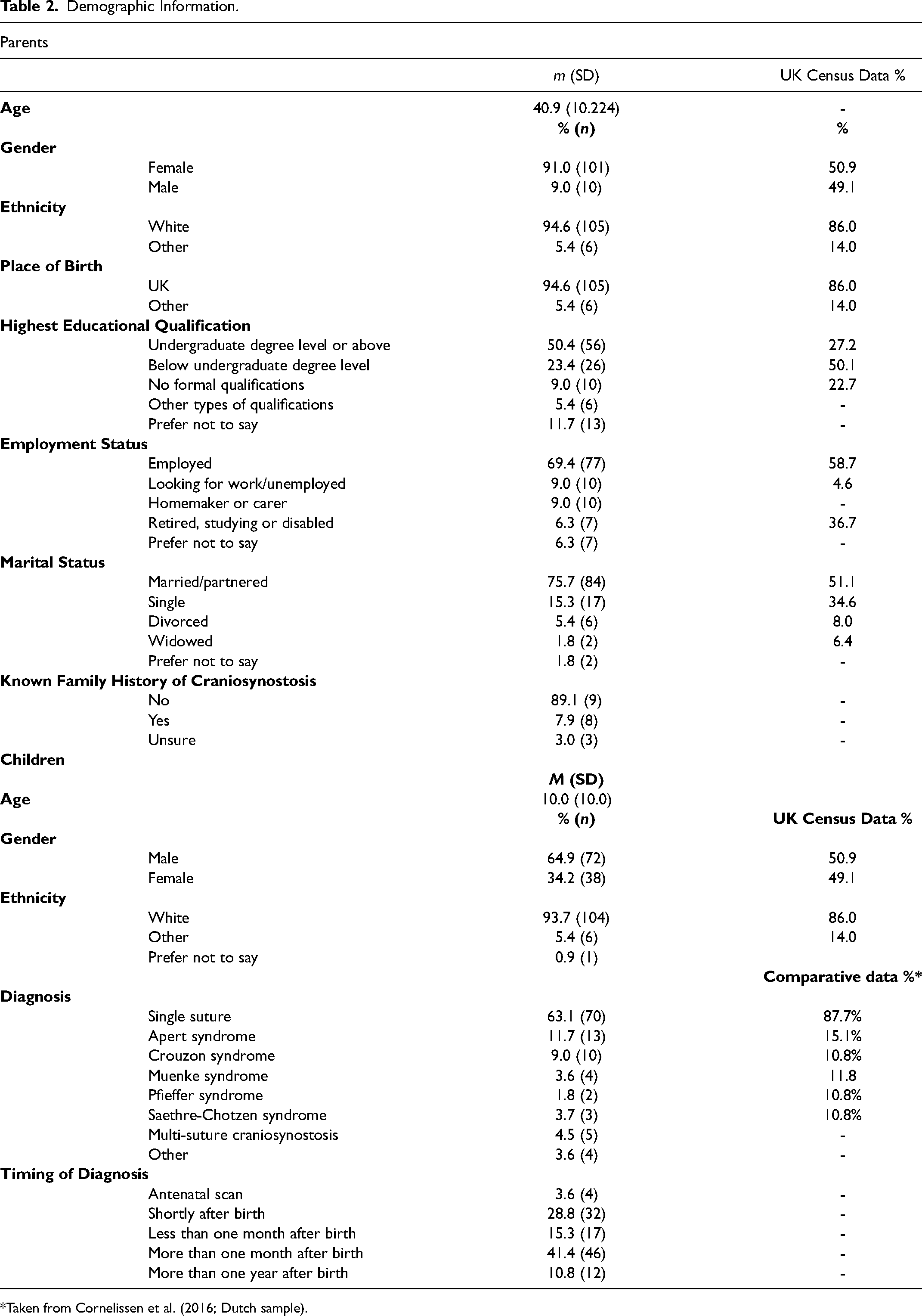
*Taken from Cornelissen et al. (2016; Dutch sample).
Procedure
An advert containing a link to the online survey was distributed on relevant Headlines Craniofacial Support websites, social media, and e-newsletters. Before proceeding to the survey itself, participants were asked to read the Participant Information and Privacy Notice, and to indicate their consent to participate. Participants were eligible if a) their child had been diagnosed with syndromic or non-syndromic craniosynostosis, b) their child had been born in the UK (due to likely variations in healthcare between countries), c) parents were aged 16 years or older, d) the family was currently living in the UK, and e) the parent was proficient enough in written English to provide informed consent and complete the online survey. The survey was launched in October 2019 and remained open to responses until April 2020.
Standardized Outcome Measures
The Hospital Anxiety and Depression Scale (HADS; Zigmond and Snaith, 1983) is a 14-item self-reported measure of common ‘symptoms’ related to anxiety and depression during the past month. The measure consists of seven questions associated with anxiety (HADS-A) and seven questions associated with depression (HADS-D). Items are rated on a 4-point Likert scale (eg, 0 = Not at All; 3 = Most of the Time) and higher scores indicate a higher level of emotional distress. Results can be interpreted as follows: a score of 0–7 is considered Normal, 8–10 is considered Borderline, and 11+ is considered to be Clinically Concerning.
The Perceived Stress Scale (PSS; Cohen et al., 1983) is a 10-item self-report measure of perceived stress during the past month. The measure reflects the degree to which situations in the person’s life are appraised as stressful. Items are rated on a 5-point Likert scale (0 = Never; 4 = Very Often) and a higher score indicates a higher level of perceived stress and can be interpreted as follows: 0–13 (Low Stress), 14–26 (Moderate Stress), 27–40 (High Stress).
The Revised Life Orientation Scale (LOT-R; Scheier et al., 1994) is a 10-item measure of optimism and pessimism. Items are rated on a 5-point Likert scale (0 = Strongly Disagree; 4 = Strongly Agree) and 6 items are used to calculate a total score. A higher score indicates a more positive life orientation. Results can also be interpreted as follows: 19–24 High Optimism; 14–18 Moderate Optimism; 0–13 Low Optimism.
The Conor-Davidson Resilience Scale (CD-RISC10; Connor and Davidson, 2003) is a 10-item measure of an individual’s level of resilience. Items are rated on a 5-point Likert scale (0 = Not True at All; 4 = True Nearly all the Time) and a higher score indicates greater resilience.
Analysis
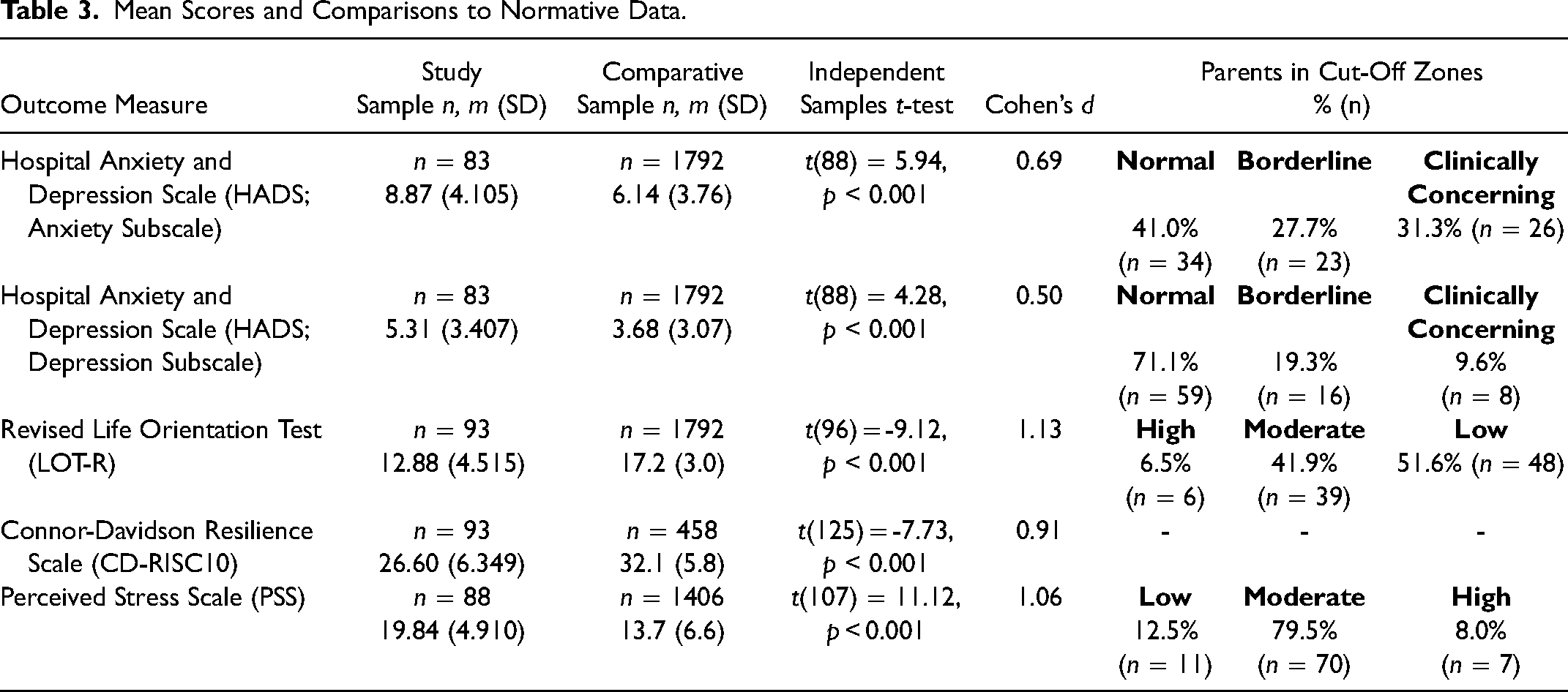
Data were analysed using SPSS. A review, verification, and validation of standardised quantitative data was undertaken prior to analysis. Sample means were generated and compared to published general population data obtained from Europe and the United States (Table 3) using independent samples t-tests. Cohen’s d was also calculated, whereby a value of 0.2–0.5 represents a small effect, 0.5–0.8 represents a medium effect, and 0.8 or more represents a large effect (Cohen, 1998). Pearson’s Correlation was used to assess the relationship between outcome measures. For statistically significant correlations, r values of approximately 0.1 in magnitude are considered to represent a small effect, 0.3 to represent a medium effect, and 0.5 to represent a large effect (Cohen, 1998). Single item questions were analysed using descriptive statistics.
Mean Scores and Comparisons to Normative Data.
Qualitative data were analysed independently using inductive content analysis (Hsieh and Shannon, 2005) by the first and second authors. First, qualitative data were read and re-read, to establish an overall picture of the data. Common codes were then inductively grouped together in an iterative process and discussed until full agreement was reached. Finally, frequency counts were calculated.
Preliminary findings were shared with parent representatives and clinical psychologists, and their feedback was integrated into the final paper.
Results
Participant Demographics
A total of 111 eligible parents of individuals with craniosynostosis took part in the study, and on average, participants took approximately 45-min to complete the survey. Table 2 provides for full demographic information on participating parents and their children, as well as comparisons to national census data where available. Very rare conditions have been grouped together under ‘Other’ to preserve participant anonymity.
Participating parents had a mean age of 41 years and were mostly female and married. Most of the parents were White and had been born in the UK. More than half of parents were employed at the time of completing the survey. As a whole, the current sample were educated to a higher level compared to the national census. A large proportion of the sample did not report a known family history of craniosynostosis. The majority of the children were male and White. Children had a mean age of 10 years (standard deviation = 10), despite 22 children being aged 18 + years at the time of the study (minimum = 3 months, maximum = 49 years). There were similar proportions of participants with children ages 4–17 between the syndromic and nonsyndromic groups. However, there were more parents of children ages 0–3 without a syndrome (n = 31; 44%) than those with a syndrome (n = 4; 11%) and conversely there were more parents of individuals ages 18 and older that had a syndrome (n = 16; 43%) relative to individuals without a syndrome (n = 5; 7%). The most common diagnosis was single suture craniosynostosis, and most parents had waited more than one month after their child’s birth to receive a diagnosis.
Within Group Analyses
To examine possible differences across the sample according to the age of the child, a one-way ANOVA was carried out (see Supplemental Table 1). The ANOVA did not identify any significant differences in outcomes across attributed developmental age groups (0–3 years, 4–11 years, 12–17 years, 18 + years). Similarly, no statistically significant differences in outcomes between parents of children with syndromic (n = 37) and non-syndromic (n = 70) craniosynostosis were identified using independent samples t-tests (see Supplemental Table 2). In four cases, the syndromic status of the condition could not be determined and these data were excluded from the exploratory analysis. The sample was therefore subsequently analysed as a whole.
Comparisons to General Population Data
In comparison to the general population (Table 3), parents of individuals with craniosynostosis reported significantly lower levels of resilience (large effect), significantly lower levels of optimism (large effect), significantly higher levels of stress (large effect), significantly more symptoms of anxiety (medium effect), and significantly more symptoms of depression (medium effect). Overall, and according to clinical cut-off points (Table 3), parents’ optimism scores were found to be ‘low’, levels of stress were found to be ‘moderate’, anxiety symptom severity was found to be ‘moderate’, and symptoms of depression were found to be in the ‘normal’ range.
Single-Item Data
A large proportion of participating parents reported feeling upset (92.8%, n = 103) when their child was diagnosed with craniosynostosis, in addition to feelings of shock (73.9%, n = 82) and worry for the future (99.1%, n = 110). Seventy-six parents reported feeling guilty (68.4%) at the time of diagnosis and a small proportion (10.8%, n = 12) reported feeling blamed by others. Despite these challenges, only 27 percent (n = 30) of parents reported having accessed psychological support (for them or their child).
Associations between Outcomes
Pearson’s correlation analyses found that all outcome variables were correlated to varying degrees, displaying small to large coefficient (r) values. Anxiety was positively associated with depression (r(83) = .64, p < .01) and perceived stress (r(83) = .59, p < .01). Anxiety was negatively associated with optimism (r(83) = -.54, p < .01) and resilience (r(83) = -.41, p < .01). Depression was positively associated with perceived stress (r(83) = .59, p < .01). Depression was negatively associated with optimism (r(82) = -.54, p < .01) and resilience (r(83) = -.34, p < .01). Optimism was positively associated with resilience (r(83) = .41, p < .01). Optimism was negatively associated with perceived stress (r(87) = -.58, p < .01). Finally, resilience was negatively associated with perceived stress (r(88) = -.36, p < .01).
Qualitative Data
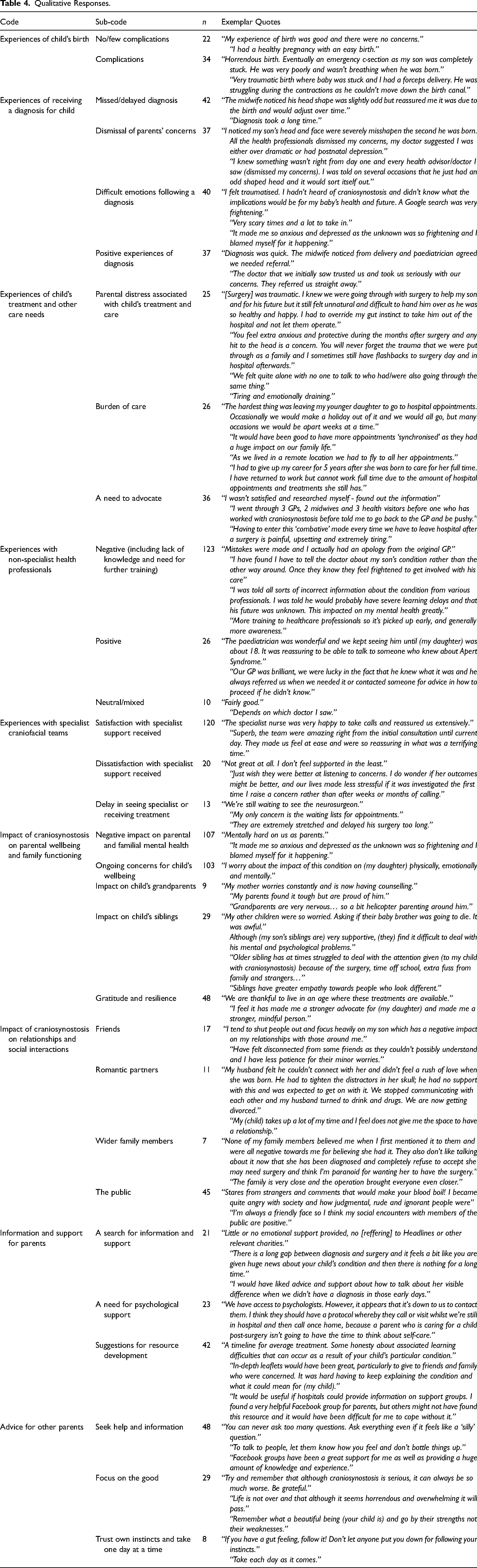
Table 4 outlines the codes and sub-codes identified in the data, and provides exemplar quotes and frequency counts for each. No notable differences were evident in the data based on children’s ages or type of craniosynostosis. In their responses, parents offered qualitative insight into their experiences of the child’s birth and diagnosis, including delayed diagnosis with dismissal of their concerns. Parents noted an equal number of difficult emotions following diagnosis as positive experiences of the diagnosis. When discussing their experiences of treatment and interactions with health professionals, there was pattern of frequent negative experiences with non-specialist health care professionals that was balanced with an equally commonly shared expression of satisfaction with the support received by craniofacial specialists. Responses about the impact of craniosynostosis on their own wellbeing reflected frequent challenges and ongoing concerns for their children’s wellbeing. Parents also noted that extended families’ wellbeing was also impacted, including grandparents and siblings. Parents spoke less frequently about the impact on their relationships with others, with more comments made about interactions with the general public. Parents also commented on the need for more information and support than what is currently available for parents. Finally, they offered advice to other families of children with craniosynostosis, including seeking for support and information ad focusing on the positive.
Qualitative Responses.
Discussion
The aim of the current study was to conduct an initial investigation of psychosocial adjustment among parents of individuals with craniosynostosis, via a UK-wide online survey, with a view to informing psychosocial provision for the family as a whole. The study offers a breadth of quantitative and qualitative data from an understudied population affected by a rare craniofacial condition. Below, findings are summarised, methodological considerations are discussed, and recommendations for future research and clinical practice are made.
Synthesis of Findings
The quantitative data presented indicate that parents of individuals with craniosynostosis may experience higher levels of stress, more symptoms of anxiety, and lower levels of resilience and optimism than the general population. Participating parents also reported significantly more symptoms of depression, although scores remained in the ‘normal’ range. These findings are similar to previous quantitative literature examining the impact of non-syndromic craniosynostosis on parenting stress (Rosenberg et al., 2011) and the psychological impact of other craniofacial conditions on parents, such as CL/P (Sato et al., 2021; Stock, Costa et al., 2020). Additional single-item data demonstrated parents may feel upset, shocked, worried, guilty, and/or blamed by others after receiving their child’s diagnosis of craniosynostosis. Such feelings have also been reported by parents of children born with CL/P (Nelson et al., 2012) and craniofacial microsomia (Luquetti et al., 2018).
Results from the correlation analyses found that most outcomes were related to one another to varying degrees. This suggests that intervening in one area could indirectly improve adjustment in other areas. For example, working to reduce parental anxiety could also help to alleviate symptoms of depression and stress, and increase levels of optimism and resilience. However, further work, with larger samples which would allow for more complex analyses (e.g, regression modelling to determine the factors which are associated with parental psychological wellbeing) would be needed in order to confirm these findings and determine the effectiveness of such an approach for psychological intervention.
Further insight into parents’ experiences of their child’s diagnosis and treatment was provided by the qualitative data. Reports of a difficult birth and challenges around diagnosis were common, including missed/delayed diagnosis, and a dismissal of parents’ concerns by non-specialist health professionals. In previous research related to the diagnostic and care experiences of parents of children with craniofacial conditions, parents have reported a lack of sensitivity, knowledge, and empathy from hospital staff, as well as limited quality information, and issues regarding the impact of a ‘delayed’ diagnosis (Costa et al., 2019; Zerpe et al., 2020). Importantly, research suggests that good relationships with health professionals is imperative for familial adjustment. For example, Stock, Costa and colleagues (2020) found that dissatisfaction with healthcare was a key risk factor for psychological distress in parents of children with CL/P. Further, research has suggested that non-specialist health professionals, such as pediatricians, midwives, and general practitioners, may themselves feel ill-equipped to care for families with rare conditions (Stock and Costa, 2020).
Parents also discussed psychological challenges associated with supporting their child through treatment, in addition to a high burden of care and a need to advocate for their child. Challenges around managing complex medical information and making treatment-related decisions on behalf of their child, in addition to a disruption to daily life due to time-consuming medical appointments, are increasingly well documented in the broader craniofacial literature (Nelson et al., 2012; Johns et al., 2018; Luquetti et al., 2018). In a study of parents of children with rare craniofacial conditions, Feragen and colleagues (2020) found physical and psychological symptoms that could be indicative of medical traumatic stress among parents of children with rare craniofacial conditions, exacerbated by challenges such as a high burden of care and the ongoing weight of responsibility of advocating for their child.
Parents in the current study also referenced the overall psychological impact of the condition on wider family members (including grandparents and siblings). For example, grandparents may experience emotional distress and increased concern, while siblings might feel resentful about receiving comparatively less attention, as well as experiencing anxiety about their sibling’s health. In line with these findings, the potential psychological impact of CL/P on grandparents (Guest et al., 2019) and siblings (Stock et al., 2016) has been documented.
Parents also discussed the impact of their child’s condition on their own relationships, including friendships, romantic relationships, and interactions with members of the public. As noted in previous literature, satisfaction with relationships (including romantic relationships and friendships) could be an important protective factor against poor psychological outcomes in parents of children with craniofacial conditions (Stock et al., 2020). Similarly, perceived stigma and negative social interactions can be a strong setback for parents trying to adjust to the diagnosis (Zeytinoǧlu et al., 2021; Feragen et al., 2022). While some reports were indicative of negative social experiences, others were more positive, and touched on notions such as strengthened familial bonds. Importantly, parents in the current study also reported positive experiences and outcomes associated with having a child with craniosynostosis, both for themselves and other family members. For example, parents reported siblings to have increased knowledge, empathy, and emotional intelligence. For themselves, parents described a sense of personal growth, including feelings of gratitude and the belief they were more resilient as a result of the adversity they had experienced. In line with the findings of the current study, Feragen and colleagues (2020) found that parents of children with rare craniofacial conditions reported positive consequences and personal growth, including a shift in life perspective and increased self-confidence. These findings demonstrate how difficult experiences can be harnessed to facilitate positive learning and growth.
Given the number of challenges identified by participating parents, and the potential for these difficulties to evoke psychological distress, providing appropriate information and support at key times throughout the family’s journey appears to be imperative. Yet, relatively few parents in the current study reported having accessed psychological support, and many commented that existing information and support services were inadequate. Parents were able to offer advice to other families affected by craniosynostosis, including the importance of seeking help and information, focusing on the positives, trusting their own instincts, and taking one day at a time.
Implications for Future Research and Practice
The findings of this study suggest that parents of individuals with craniosynostosis may be at risk of psychological distress. Further, that psychological difficulties in parents may not always be identified and/or addressed in practice, and that families may not be independently accessing the support they need. Understandably, the focus of craniofacial care is predominantly on the child, and craniofacial teams do not always have the funding or capacity to offer support to the wider family. However, as is well known in the broader health literature, the psychological adjustment of the parents can have a considerable effect on the child’s wellbeing and development, and it is therefore important to consider family functioning as a whole. Subsequently, routine psychological screening to identify family members who may be at risk of psychological distress is recommended, as is routine follow up at key points in the child’s journey (e.g in the lead up to and following a major surgery). Several measures suitable for this purpose have been recommended by clinicians and researchers in other areas of craniofacial care, and could also be appropriate for use in the craniosynostosis population (Stock, Marik et al., 2020). In countries where routine psychological support for craniofacial conditions is not yet available, basic strategies could be adopted by all medical providers to improve patient-centred care (Stock, Marik et al., 2020). Further exploration of the types of support currently available to parents and possible ways to close this perceived gap is also recommended. In particular, interventions aimed at increasing parental resilience and coping strategies may be warranted. Trauma-informed resources may also be beneficial in supporting some parents to adjust to the diagnosis and during ‘peak’ times of treatment (Feragen et al., 2020).
In addition to the provision of formal psychological support, self-help resources should also be developed. Parents in the current study offered their own suggestions for future resource development. These included developing reliable information about treatment and additional/associated challenges (e.g learning difficulties), developing leaflets to give to family and friends to increase understanding, and more referrals from the hospital to external sources of support (e.g trusted online support groups). These insights could be incorporated into the development of future support materials. Moreover, information and support materials could be co-produced and evaluated by clinicians, researchers, and parent representatives, to ensure stakeholder agreement and maximum impact for the community.
While experiences with specialist health professionals were generally talked about favourably, experiences with non-specialists were less positive. Specifically, parents felt that non-specialists lacked knowledge of craniosynostosis and felt a need for a more cohesive health service with clearer links between non-specialist and specialist teams. Parents also believed that improving education for non-specialist health professionals with regard to craniofacial conditions, the likely impacts, and the treatment pathway would be beneficial, to ensure that families have access to adequate support. Non-specialist health professionals, such as pediatricians, midwives, and general practitioners are likely to be in contact with families, particularly around the time of the initial diagnosis. As advocated by the current study, additional training around rare conditions for non-specialists has been described as necessary in previous research, to enable positive experiences and prompt referrals to specialist teams and sources of support. As a starting point, one previous study interviewed non-specialist health professionals about their knowledge of craniofacial conditions, and offered suggestions regarding the content and format that a training package might encompass (Stock and Costa, 2020).
Methodological Considerations
This exploratory study has provided important insights into the experiences of parents of children with craniosynostosis and has made attempts to fill gaps in the knowledge base. The findings of this study will go on to inform future work in the area. Nonetheless, a number of limitations must be acknowledged. First, by design, the study involved self-report, which induces a number of challenges such as accuracy and social desirability. Given the nature of the study, it was also not possible to obtain and analyse the medical/surgical history of the families, which is important for contextualising experiences. The most methodologically challenging aspect of this study was that responses were received from a largely heterogenous group of parents, in terms of the age and syndromic status of the child. Responses from parents with older children may have been impacted by recall and/or could have affected the relevance of these experiences to current healthcare systems. For example, parents of younger children may now benefit from clinical psychologists being a part of standard care, which would not have been the case several years ago. Although no significant differences between defined age groups were identified in the quantitative data, these analyses would have likely been affected by the sample size. More rigorous and long-term research examining adjustment across the lifespan is ultimately needed. Similarly, no significant differences were found in parent outcomes due to the presence or absence of a syndrome in the child, nor were they notably evident in the qualitative data. However, again sample sizes become further reduced when categorizing by subgroup. A greater impact of syndromic conditions has been suggested in the literature (Feragen and Stock, 2017) and to further complicate this discussion, recent research has indicated that single suture craniosynostosis can at times be genetic, while not necessarily being related to a syndrome (Wilkie, 2017). Future research with larger samples is needed the determine whether and how the impact of craniosynostosis vary for different families based on type of craniosynostosis and surgical, medical, demographic, and psychosocial factors that may influence outcomes.
Aside from the age and syndromic status of the child, the sample was comprised of predominantly White, relatively well-educated participants, with those from Black and other Minority Ethnic communities and lower socioeconomic status being underrepresented. While not uncommon in research, this becomes problematic when considering that underserved groups may experience poorer outcomes. For example, in a study on psychological functioning in families affected by CL/P, Crerand and colleagues (2015) observed differences in outcomes according to race, ethnicity and type of medical insurance. Again, larger studies are needed to determine the factors that may influence outcomes and to identify potentially vulnerable groups. Further, more than 90 percent of participants were mothers. It is not uncommon in research for fathers to be underrepresented, however, we are lacking important information when considering the unique role that a father plays in their child’s development and in supporting the family overall (Lamb, 2010). In a study of fathers of children with CL/P, Stock and Rumsey (2015) found that fathers are just as affected, and potentially in different ways to mothers, by their child’s diagnosis, and should be offered the same level of involvement in their child’s care, both in research and practice. Future research should devise creative recruitment strategies to widen participation and ensure that target populations are more adequately represented in craniofacial research.
In addition, data were collected only from caregivers of individuals with craniosynostosis. Whilst participants referenced the psychological impact of the condition on wider family members (including grandparents and siblings), data from such groups were not directly obtained. Given the current findings, as well as previous research which has identified a potential impact of craniofacial conditions (CL/P) on the wider family, future studies should aim to directly investigate the possible psychosocial impact of craniosynostosis on the wider family.
Participants were recruited through Headlines Craniofacial Support and therefore, this sub-set of parents cannot be assumed to be representative of the population as a whole. Multi-centre research is likely the most efficient way to access the target population. It is advised that the specialist craniofacial units focus on routinely collecting patient and parent data, including that pertaining to psychosocial outcomes, to better allow for this type of research to be possible in future.
Finally, data were collected until April 2020, which coincided briefly with the first UK national lockdown (26 March 2020) due to the Covid-19 pandemic. The Covid-19 pandemic has had a significant impact on healthcare provision and utilisation worldwide (Moynihan et al., 2021), the impacts of which have been reported among parents of children with CL/P (Costa et al., 2021). However, given the overlap of only a few weeks, there were no mentions of the Covid-19 pandemic by parents in the current data. Nonetheless, it is possible that since data were collected, Covid-19 became more influential for parents.
Conclusions
This study used standardized quantitative outcome measures and qualitative methods to explore the experiences of an under-researched group of parents. In line with previous craniofacial literature, the findings of this study suggest that parents of individuals with craniosynostosis may be at risk of adverse psychosocial outcomes. The findings highlight ways in which parents of individuals with craniosynostosis may be impacted, and offer suggestions for future research and clinical work.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656221102043 - Supplemental material for Raising a Child with Craniosynostosis: Psychosocial Adjustment in Caregivers
Supplemental material, sj-docx-1-cpc-10.1177_10556656221102043 for Raising a Child with Craniosynostosis: Psychosocial Adjustment in Caregivers by Bruna Costa, Wendy Edwards, Karen Wilkinson-Bell and Nicola Marie Stock in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656221102043 - Supplemental material for Raising a Child with Craniosynostosis: Psychosocial Adjustment in Caregivers
Supplemental material, sj-docx-2-cpc-10.1177_10556656221102043 for Raising a Child with Craniosynostosis: Psychosocial Adjustment in Caregivers by Bruna Costa, Wendy Edwards, Karen Wilkinson-Bell and Nicola Marie Stock in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgments
Thank you to our Public Involvement representatives and Dr Natasha Rooney for their input into the design of this study, and to Aida Mikkola for her assistance with the analysis. We are especially grateful to all study participants for candidly sharing their experiences with us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vocational Training Charitable Trust Foundation,
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.