
Abstract
Objective
This study investigated various manifestations of nasal deformities in lesser-form cleft lips, including the minor-form, microform, and mini-microform, by photogrammetric comparison with incomplete cleft lips.
Design
Retrospective study.
Setting
Tertiary university-affiliated hospital.
Participants
A total of 160 patients with unrepaired unilateral incomplete cleft lips ranging from lesser-form to two-thirds way clefts.
Main Outcome Measures
The severity of nasal deformities was assessed by photogrammetric measurements of linear and angular variables. The symmetry ratio between the cleft and non-cleft sides was obtained by measuring various nasal parameters and comparing them among the different labial cleft groups.
Results
The degree of nasal deformities increased with the extent of labial clefts among the 3 labial cleft groups (lesser-form, halfway, and two-thirds way clefts) in terms of alar base width ratio (1.102, 1.197, 1.309; P < .05), nostril width ratio (1.287, 1.387, 1.551; P < .05), and columellar angle (11.5, 14.45, 18.197; P < .05). Each parameter indicated lesser-form, halfway, and two-thirds way clefts, respectively. However, only the lateral lip height ratio (0.942, 0.851, 0.87; P < .05) and nostril width ratio (1.207, 1.35, 1.29; P < .05) significantly differed among the 3 subgroups. Each parameter indicated mini-microform, microform, and minor-form, respectively.
Conclusions
The cleft nasal deformities in lesser-form cleft lip present comparable severities among its subtypes, which implies that the extent of the labial cleft is not correlated with nasal deformities. Each nose in the lesser form cleft should be individually assessed for primary rhinoplasty and requires tailored correction.
Introduction
A lesser-form cleft lip presents the mildest lip and nose deformities. Although the term “lesser” implies subtle deformities of the lip and nose, the clinical manifestations of lesser-form clefts may vary from near-normal to typical abnormalities. Published articles have focused on labial cleft phenotypes. Various nomenclatures have been suggested, such as “occult,” “minimal,” “lesser-form,” and “microform,” which implies that it was difficult to define this disease spectrum by a single criterion.1–8 Onizuka et al 5 classified this type of labial cleft into 5 degrees. The microform cleft lip corresponded to the first degree without lip deformities and the second degree with the notch of vermilion. Thomson and Delpero 9 reported that the microform cleft lip had 3 components: a vermilion notch, an afibrous band of the lip, and an alar deformity. Yuzuriha and Mulliken 6 delineated the spectrum of lesser-form cleft lips into 3 groups: minor, microform, and mini-microform based on the extent of the labial cleft.
While detailed information regarding the nomenclature and repair techniques for labial deformities has been reported, the manifestations of nasal deformities in lesser-form cleft lips have received little attention. The nasal deformities associated with lesser-form cleft lips are variably expressed across a spectrum of near-normal to typical abnormalities. Some evidence of cleft lip nose deformities can be identified as milder conditions with a combination of phenotypes, such as a depressed nostril sill, flattened nostril rim due to displaced alar cartilage, alar base asymmetry, and septal deviation. The severity of labial clefts affects the severity of the nasal imbalance. As Ranta 4 suggested, the degree of nasal deformities correlated directly with the severity of labial deformities but not with the severity of dentoalveolar deformities. Yuzuriha and Mulliken 6 also stated that the manifestation of a nasal deformity in a lesser-form cleft lip could be depicted based on the extent of the affected vermilion–cutaneous junction.
However, nasal deformities in lesser-form clefts have received little attention due to their varying spectrum. We questioned whether the severity of nasal deformities follows the severity of lesser-form labial clefts and what anatomical features distinguish the nasal appearance in this cleft lip. Thus, we performed a photogrammetric comparison of the nose in unrepaired lesser-form cleft lips with that in incomplete cleft lips from halfway to two-thirds way defects and performed a subgroup analysis of lesser-form labial clefts, categorized as minor-form, microform, and mini-microform, to delineate the spectrum of nasal deformities in this population.
Patients and Methods
A total of 160 patients with incomplete cleft lips who visited our outpatient clinic from January 2012 to January 2020 were recruited for this study. The extent of labial clefts and subgroups of lesser-form clefts were assessed by an expert cleft surgeon who is a senior author of this study. The inclusion criteria were as follows: (1) patients with unrepaired incomplete cleft lips, (2) unilateral involvement of cleft lips with a normal contralateral side, (3) appropriate frontal and basilar view photographs, and (4) age ranging from 2 to 12 months. The exclusion criteria were as follows: (1) patients with other craniofacial malformations or associated syndromes, (2) patients with complete cleft lips, and (3) incomplete cleft lips bridged by a Simonart band. Demographic information was obtained regarding the gender, location of the cleft (left or right), patient age at presentation (in months), and the associated cleft alveolus and palate. Patients with lesser-form cleft lips were sub-grouped according to 3 cleft lip types, as suggested by Yuzuriha and Mulliken 6 : minor-form, microform, and mini-microform.
Frontal and basilar view photographs were taken by the same photographer with a Nikon D700 full-frame digital single-lens reflex camera (Nikon Corp., Tokyo, Japan) following the Institute of Medical Illustrators National Guidelines protocol for the Photography of Cleft Audit Patients (2004). 10 To obtain standardized and reproducible results, images that satisfied the following criteria were selected for evaluation: a frontal view in which both ears are visible to indicate minimal rotation and the least nostril is visible to indicate minimal tilt and a basal view in which the nasal tip is projected between the medial canthi and eyebrows with no head rotation. Photographs were taken while the patients were awake in a relaxed position without facial expressions, such as laughing, lip sealing, and crying, to minimize lip and nose distortion.
Photogrammetric analysis was performed independently in the same examiner using Adobe Photoshop CS4 software (Adobe, San Jose, CA, USA), following detailed descriptions of landmarks and parameters. We placed 12 landmarks and then measured 12 inter-landmark distances and 2 angular values using the software (Supplemental Table 1). The measured distances were transformed into ratios of the cleft side to the noncleft side to control variation between patients and minimize linear measurement error. 11 The measurement error was controlled by placing presentative landmarks and reference lines on the photographs. 11 The following values were calculated from the photogrammetric measurements: alar base width ratio, lateral lip height ratio, the vertical distance from alar base to the interpupillary line, nostril width ratio, nostril height ratio, and columellar deviation angle. The proportional value was defined as the ratio of linear measurements obtained from the cleft and the noncleft sides (Supplemental Figure 1).
Informed consent was obtained from all patients for the photographs and medical records used for this research. The design of this study was reviewed and approved by the Ethical Committee of our center.
Statistical Analysis
We validated all photogrammetric measurements by determining the intraobserver agreement with an intraclass correlation coefficient. We randomly selected 20 photographs and obtained the means of each parameter twice by the same examiner in a two-week interval. Data were described as mean ± standard deviation. We compared the mean values of the linear-proportional and angular measurement sequentially using a one-way analysis of variance (ANOVA) test based on the extent of a labial cleft and subgroups of lesser-form clefts. We used a Tukey post-hoc analysis as post-ANOVA to distinguish cleft types with significantly different nasal deformities. The level of significance was 0.05 and confidence intervals were calculated at 95%. We performed statistical analysis using SPSS ver. 20 (IBM Corp., Armonk, NY, USA).
Results
The estimations of coefficients were more than 0.88 and 0.86 for all linear and angular variables, respectively, which showed that there was no significant error in the measurement method.
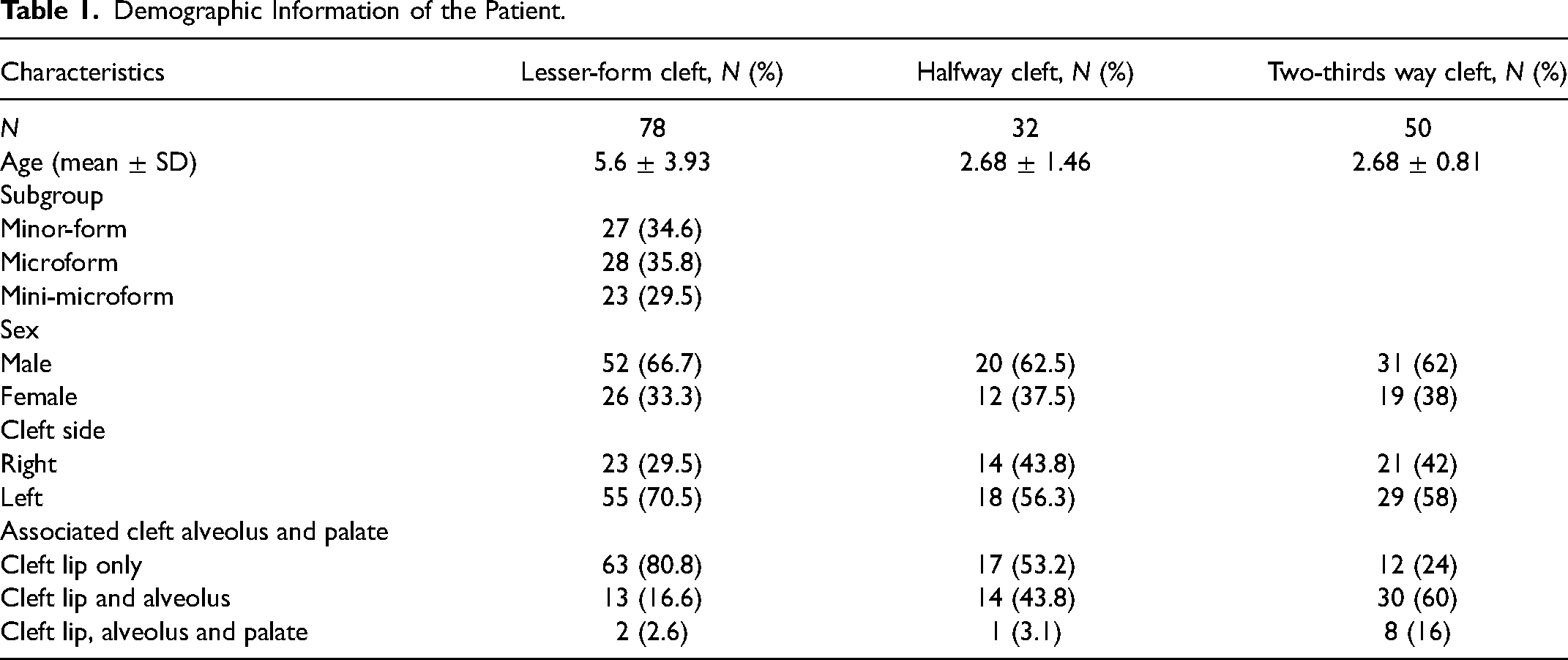
A total of 160 patients with incomplete cleft lips, comprised of 78 patients with lesser-form, 32 patients with halfway and 50 patients with two-thirds way clefts, were included in the study. Patients with lesser-form labial clefts were further categorized into 3 subgroups: 27 patients with minor-form, 28 patients with microform, and 23 patients with mini-microform. In all cleft types, there were more male patients and patients with left-side clefts. A larger cleft type was associated with more involved accompanying cleft alveolus and palate. The patients’ demographic characteristics are summarized in Table 1.
Demographic Information of the Patient.
A comparison among patients with lesser-form, halfway, and two-thirds way cleffts showed that all parameters significantly differed in the severity of nasal deformities, except the nostril height ratio (Supplemental Table 2). The alar base width ratio increased with the extent of labial cleft. The lateral lip height ratio was the highest in halfway clefts, followed by that in the two-thirds way and lesser-form clefts. The vertical distance ratio from the alar base to the interpupillary line increased and the nostril width ratio increased with the extent of labial cleft. The nostril height ratio did not significantly differ among the 3 labial cleft groups. Columellar deviation increased with the extent of labial cleft (Figure 1).
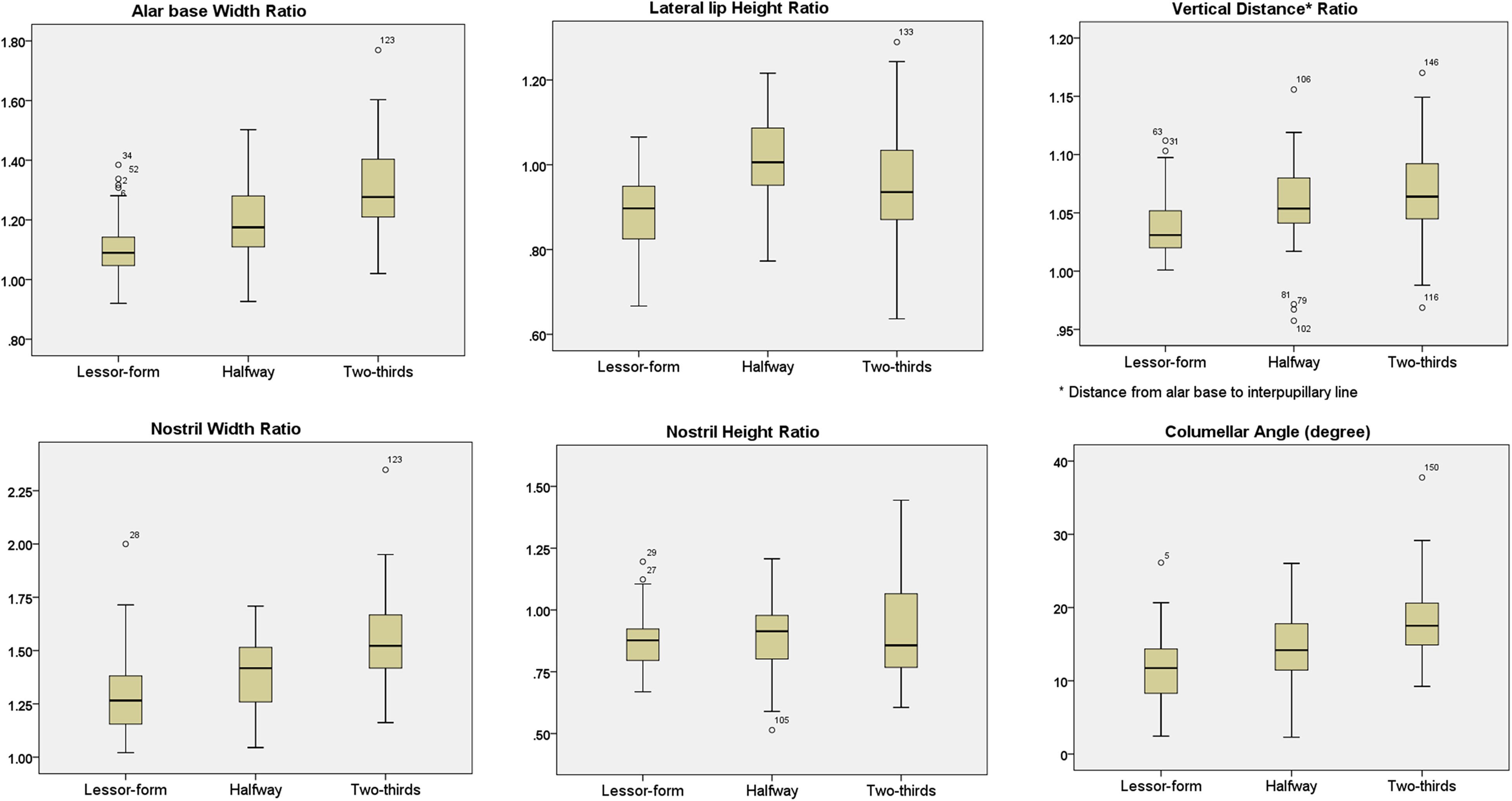
Comparison of nasal deformities among patients with incomplete clefts, including lesser-form, halfway, and two-thirds way clefts.
A comparison among subgroups of patients with lesser-form clefts revealed that 2 nasal parameters, lateral lip height ratio, and nostril width ratio, significantly differed among nasal deformities (Supplemental Table 3). The alar base width ratio showed no significant difference among the 3 groups. The lateral lip height ratio was highest in those with mini-microform clefts, followed by those in the minor-form and microform cleft groups. The vertical distance from the alar base to the interpupillary line ratio did not significantly differ among the 3 groups. The nostril width ratio was highest in the microform clefts, followed by minor-form and microform clefts. The nostril height ratio and columellar deviation showed no significant difference among the 3 groups (Figure 2).
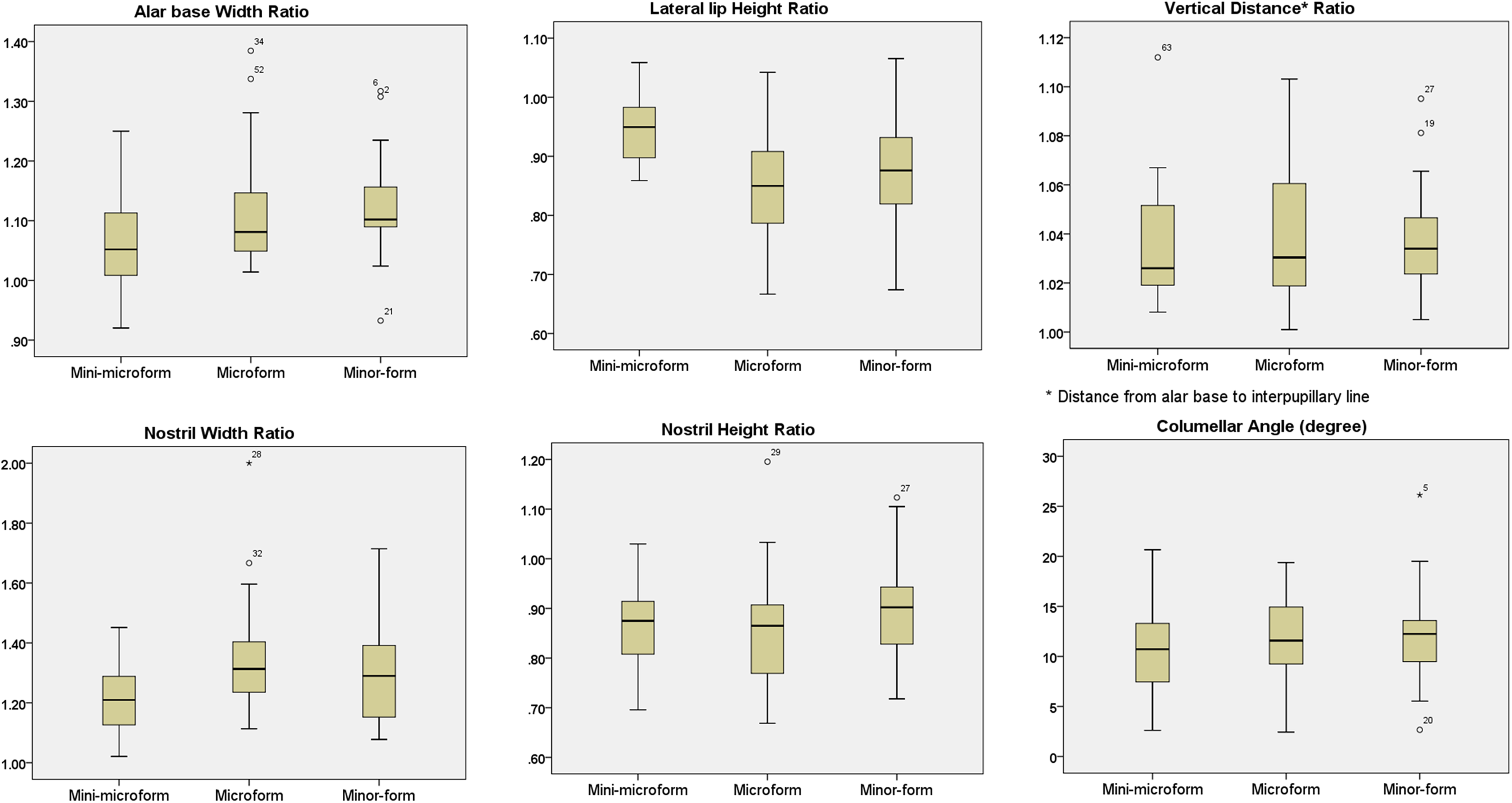
Comparison of nasal deformities among patients within subgroups of lesser-form clefts.
Discussion
Nasal deformities in incomplete cleft lips are typically milder than those in complete cleft lips, requiring less surgical correction. A variety of nasal deformities occur in patients with incomplete cleft lips, including shortening and deviation of the columella, displacement of the lower lateral cartilage, and collapse of the alar base. These results from pathologic changes in the perinasal musculature and distortion of nasal soft tissue and skeletal framework. Changes in the muscular pull of the orbicularis muscle alter the position of the lower lateral cartilage and displace the alar base. Thus, the extent of the labial cleft may affect the severity of nasal distortion. A variable amount of labial defect is present in patients with incomplete clefts, including the lesser-form, halfway, two-thirds way, and Simonart's band. 5 As the primary purpose of this study was to figure out the effect of labial cleft on nasal appearance in patients with incomplete cleft lip, patients who had Simonart's band were excluded from the study, as they were considered a variant form of the complete cleft.
A lesser-form cleft can be further categorized into 3 subgroups, as described by Yuzuriha and Mulliken, 6 based on the appearance of the vermilion–cutaneous junction. A variable degree of nasal deformity is present in each subgroup of lesser-form cleft lips, described as follows: “The minor form has a typical nasal deformity; the microform has a slight change in the sill, alar genu, and 1-2 mm lateral displacement of the alar base; and the mini-microform often has only a depressed sill.” Although they used the term “variable” for nasal shape, it seemed that they assume that the extent of labial cleft might affect the degree of nasal deformity. In our study, we attempted to determine whether nasal deformity appearance was affected by the extent of labial clefts by comparing lesser-form clefts with halfway and two-thirds way defects and by performing a subgroup comparison within the lesser-form clefts.
In this study, the severity of nasal deformities increased with the extent of labial clefts, which was identified in the comparison among the lesser-form, halfway, and two-thirds way clefts. The width of the alar base and distance from the alar base to the interpupillary line increase as the extent of the labial cleft becomes larger and the alar base displaces inferolaterally. The lateral lip height ratio was highest in the halfway clefts, followed by the two-thirds way and lesser-form clefts, sequentially. The lateral lip height ratio may show variable manifestation depending on the location of the alar base and the Noordhoff's point. 12 This value decreases when the alar base moves inferiorly, but it increases when the alar base moves laterally. The location of the Noordhoff point may vary among the patients depending on the thickness of the vermilion and the transition point of the white line. 12 The presence of accompanying cleft alveolus and cleft palate, more frequently identified in the larger cleft group, increases lateral lip height ratio as the lateral lip segment is collapsed and receded away, thereby translocating the Noordhoff's point inferolaterally. Thus, the larger cleft group may have both increasing and decreasing factors that impact this value, showing a relatively high value of standard deviation. The columellar deviation angle is primarily determined by the position of the caudal septum, characterized by a deviation to the noncleft side. 13 Literatures indicate that the septal deviation correlates with the severity of labial clefts, consistent with our study. 14 The cleft-to-noncleft side nostril width ratio followed the severity of the labial cleft, whereas the cleft-to-noncleft side nostril height ratio showed a similar mean value, but with a high value of standard deviation. The size of the nostril is affected by various factors, including septal location, amount of soft tissue in the alar rim, and appearance of nostril sill, and alar base. In general, a larger labial cleft makes more deviation of the septum to the noncleft side, resulting in a smaller nostril on the noncleft side and a larger nostril on the cleft side. Inferolateral displacement of the alar base results in widening of the cleft-side nostril. The nostril height may increase when the nostril sill is depressed, or this value may decrease when the nostril is stretched in a transverse direction by lateral displacement of the alar base, when the septum is deviated, and when there's a redundant soft tissue in the alar columellar junction. The height of the nostril sill also affects the nostril height.
The severity of nasal deformities showed no correlation with the subgroup of lesser-form clefts in this study. Although the alar base width ratio increased with the severity of lesser-form clefts (P-value < .1), some patients with mini-microform clefts showed eccentric values that were beyond the mean value of the minor-form clefts. The lateral lip height was nearly the same between the cleft and noncleft sides in patients with mini-microform clefts, while there was more variation in patients with microform and minor-form clefts. The vertical distance (from alar base to the interpupillary line) ratio showed no significant difference among the cleft groups. Of note, a few patients from all 3 groups showed an approximately 10% of discrepancy in this value. Based on these results, we found that the location of the alar base showed variable manifestation, without correlation with lesser-form cleft types. The columellar deviation angle showed no significant differences among the 3 groups, with all presenting mild deviation from 10° to 12°. Although the discrepancy in the nostril width was mildest in patients with mini-microform clefts than in the other 2 groups, the nostril width and height showed no marked difference among the 3 groups.
The cleft lip nasal deformity variability in lesser form may be explained by intrinsic and extrinsic factors affecting nasal morphology.2,15 The intrinsic nature of the cleft lip nasal deformities may manifest as hypoplastic or malpositioned cartilage. The balance between the nose and the surrounding musculature, including the nasalis, orbicularis, and other facial expression muscles may alter the nose symmetry. These intrinsic and extrinsic factors in patients with cleft palate make a variable presentation of the nose.
Our study is valuable for informing surgeons on which components should be manipulated before correction and on the phenotypic appearance of the nose in the varied spectrum of incomplete cleft lips. Overall, the extent of labial clefts correlated with nasal deformity severity in almost every component of the nose, including the columella, the nostril sill, and the alar rim and base. In lesser-form clefts, however, the extent of labial deformity did not correlate with nasal deformity severity. Various manifestations of nasal deformities in lesser-form clefts were presented in the representative cases (Figure 3).

Various manifestations of cleft nose deformities in lesser-form clefts. (A) A 5-month-old patient with mini-microform cleft showed a moderate-to-severe degree of inferolateral drifting of the alar base and nostril asymmetry. (B) A 4-month-old patient with mini-microform cleft showed a mild degree of alar base displacement and nostril asymmetry. (C) A 4-month-old patient with mini-microform cleft showed a symmetric alar base but an asymmetric nostril with medial skin hooding. (D) A 3-month-old patient with minor-form cleft showed mild lateral displacement of the alar base but a symmetric nostril without columellar deviation. (E) A 3-month-old patient with minor-form cleft showed a moderate degree of inferolateral alar base displacement, and nostril asymmetry without columellar deviation. (F) A 3-month-old patient with minor-form cleft showed typical cleft nose deformities with lateral displacement of the alar base, nostril asymmetry, and septal deviation.
Nasal deformity management in the lesser-form cleft lip can be extrapolated from our study results. The degree of columellar deviation, alar symmetry, and nostril sill appearance should be carefully evaluated before primary correction. The fundamental principle is the independent management of a cleft nose in lesser-form clefts based on nasal appearance, independent of the labial cleft classification. A mini-microform cleft with moderate nasal deformities may necessitate more aggressive correction than a microform cleft. Depending on the required amount of nasal and labial correction, the nose can be managed at the same time through a labial incision or separately through the nasal approach. The standard rotation advancement incision provides the best approach for alar base detachment and septal relocation. If the nose is managed independently from the lip, we favor additional incisions on the nose to handle the columellar deviation and alar asymmetry (Figure 4).
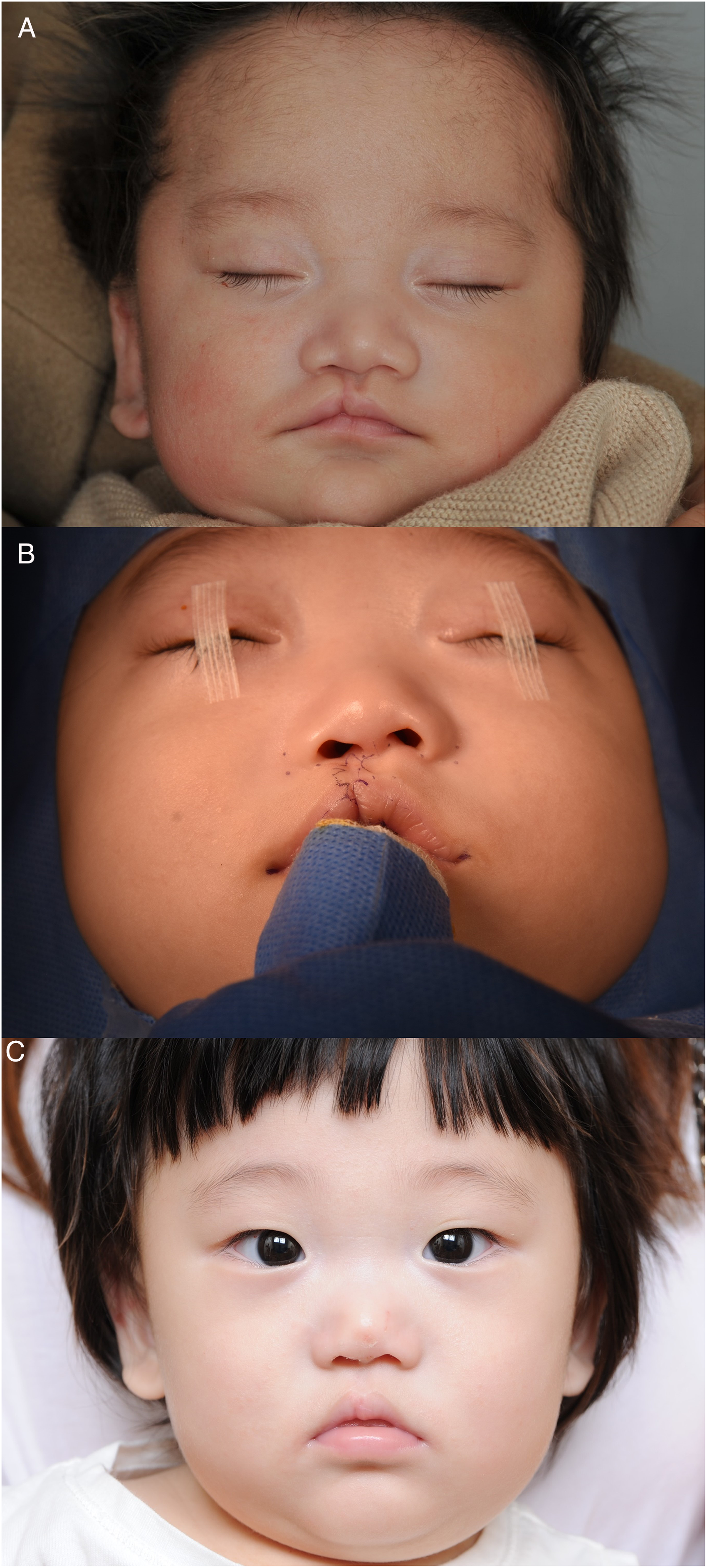
A 3-month-old patient with microform cleft underwent simultaneous correction of the cleft lip and nasal deformity in primary cleft surgery. (A) Preoperative frontal view photograph; (B) intraoperative photograph; and (C) postoperative photograph showing a symmetric appearance of the lip and nose.
Our study had several limitations. As we adopted two-dimensional (2D) photometry, only a proportional and angular value was available for analysis. With the advancement of three-dimensional (3D) photometry, actual measurement values can be obtained indirectly. Given the convex and concave appearance of the lip and nose, measurement with 2D photometry is unreliable for analysis. Another limitation of our study was that only data obtained from unrepaired patients were available. Although most patients in our study were scheduled to undergo primary correction of the lip and nose, we did not include postoperative data due to variations in surgical correction methods. The results of our study suggest a varied spectrum of nasal deformities in patients with incomplete clefts and further perspectives on the nasal appearance in each subtype of lesser-form clefts.
There is no consensus on the efficacy of simultaneous rhinoplasty in primary cleft lip repair on long-term nose growth among cleft surgeons. 16 Data showed that there was no increase in the synchronous correction rate of the cleft lip nasal deformity. In our experience, however, even milder form of nasal deformities in lesser-form cleft lip tends to worsen, along with growth. We perform primary rhinoplasty even for patients with a lesser form of cleft lip. Again, as the manifestations of nasal deformities vary among the lesser form deformity subtypes, each nose in the lesser form cleft deformity should be individually assessed for tailored correction during primary rhinoplasty.
Conclusion
The cleft nasal deformities in lesser-form cleft lip present comparable severities among the minor-form, microform, and mini-microform, which implies that the extent of the labial cleft is not correlated with the severity of nasal deformities in the lesser-form cleft lip. Each nose in the lesser form of cleft deformity should be individually assessed for primary rhinoplasty and requires tailored techniques for correction.
Supplemental Material
sj-jpg-1-cpc-10.1177_10556656221105204 - Supplemental material for Comparison of Cleft Lip Nasal Deformities Between Lesser-Form and Incomplete Cleft Lips: Implication for Primary Rhinoplasty
Supplemental material, sj-jpg-1-cpc-10.1177_10556656221105204 for Comparison of Cleft Lip Nasal Deformities Between Lesser-Form and Incomplete Cleft Lips: Implication for Primary Rhinoplasty by Young Chul Kim, Dae Won Hong and Tae-Suk Oh in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656221105204 - Supplemental material for Comparison of Cleft Lip Nasal Deformities Between Lesser-Form and Incomplete Cleft Lips: Implication for Primary Rhinoplasty
Supplemental material, sj-docx-2-cpc-10.1177_10556656221105204 for Comparison of Cleft Lip Nasal Deformities Between Lesser-Form and Incomplete Cleft Lips: Implication for Primary Rhinoplasty by Young Chul Kim, Dae Won Hong and Tae-Suk Oh in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.