
Abstract

Introduction
Orthognathic procedures are classified as clean-contaminated and are therefore expected to carry a higher risk of peri-operative infection. 1 Accordingly, prophylactic antibiotics are commonly prescribed, though the optimal class, timing, and duration of therapy remain controversial. 2 Despite prophylaxis, infection rates in orthognathic surgeries remain considerably higher than clean-contaminated case infection rates overall. Recent retrospective studies report surgical site infections in 8% to 12% of orthognathic surgeries3–5 as compared to 2.8% of clean-contaminated plastic surgeries and 3.3% of clean-contaminated cases across surgical specialties.6,7 Acknowledging the unique obstacles to antisepsis in orthognathic procedures, we find the literature regarding peri-operative local antiseptic preparation to be sparse and highly heterogeneous. Nevertheless, several antiseptic strategies such as brushing the oral cavity with chlorhexidine, professional preoperative dental cleanings, and nasal decontamination show potential for reducing infectious complications.
Challenges to Antisepsis
The substantial infection rates in orthognathic surgery are intuitive, as the oral cavity hosts one of the highest bacterial concentrations and the greatest microbial diversity in the human body. 8 The nasal cavity is also highly colonized and presents a particular challenge to surgical antisepsis as it acts as a reservoir of Staphylococcus aureus, the most common cause of surgical site infections.9,10 While the nasal mucosa may be unintentionally violated in orthognathic procedures, the sinuses are necessarily involved in maxillary osteotomies and host mixed aerobic and anaerobic flora in 93% of individuals.11–13
Beyond their extensive bacterial colonization, the oral and nasal cavities present several unique challenges to surgical antisepsis. Firstly, limited access and complex anatomy inside the oral and nasal cavities make it difficult to achieve thorough coverage with topical antiseptic solutions. 14 Additionally, most iodine- or alcohol-containing surgical prep solutions achieve the greatest efficacy when allowed to dry. However, saliva, secretions, and humidity in the oral and nasal cavities interfere with this process.
Moreover, bacteria colonizing the teeth and sinuses commonly form biofilms, and as such, display greater resistance to both local antiseptics and systemic antibiotics. 15 Implanted metal plates, screws, and appliances used in orthognathic procedures provide further substrate for biofilm formation. Of patients developing an infection following orthognathic surgery, 26% were reported to have recurrent infection despite antibiotic treatment, and 14% required hardware removal. 5
Finally, post-operative pooling of saliva and food debris along incision sites in the mandibular vestibule likely contribute to the notable incidence of surgical site infection in mandibular surgery via intraoral approaches. 16
Current Practices and Evidence
Preoperative oral antiseptic preparation is routine for most surgeons performing orthognathic surgery. However, outside of the debate over systemic prophylactic antibiotics, little has been published or standardized regarding techniques to mitigate risks of infectious complications. A survey of American Society of Maxillofacial Surgeons members in the year 2000 found that 58% used some form of antiseptic oral preparation, including iodine, clindamycin, chlorhexidine, peroxide, and combination solutions. Notably, the same survey found that most surgeons were uncertain about the impact of such measures on infection or bacterial colonization. 17
Nevertheless, prior studies have demonstrated the efficacy of chlorhexidine and povidone-iodine in transiently reducing bacterial counts in the oral cavity beyond the dilutional and mechanical cleaning effects seen with saline rinses.17–19 As further evidence, scrubbing and rinsing the oral mucosa with povidone-iodine during surgical preparation is associated with lower rates of wound complications following oncologic surgery of the mouth or oropharynx. 20 Preoperative oral chlorhexidine rinse in the surgical holding area by patients undergoing immediate dental implant placement is also associated with reduced bacterial counts in bone debris collected for bone augmentation at the implant site. 21
Reports of preoperative oral decontamination protocols in the orthognathic surgery literature are limited but describe a variety of strategies (Table 1). Some centers report brushing patients’ teeth and tongue with povidone-iodine solution, 4 others rinse intraorally with chlorhexidine,3,22 and one asks patients to brush their teeth and swish with chlorhexidine prior to induction of anesthesia. 23 The most extensive protocol involved brushing the teeth, gingiva, and tongue with chlorhexidine solution both after intubation and at the conclusion of the case, followed by postoperative instructions to brush with chlorhexidine 5 times daily. This single-surgeon cohort reported a 2% overall infection rate. 24 No reports were found of nasal decontamination prior to orthognathic surgery.
Reported Surgical Preparation Techniques in Orthognathic Surgery. a
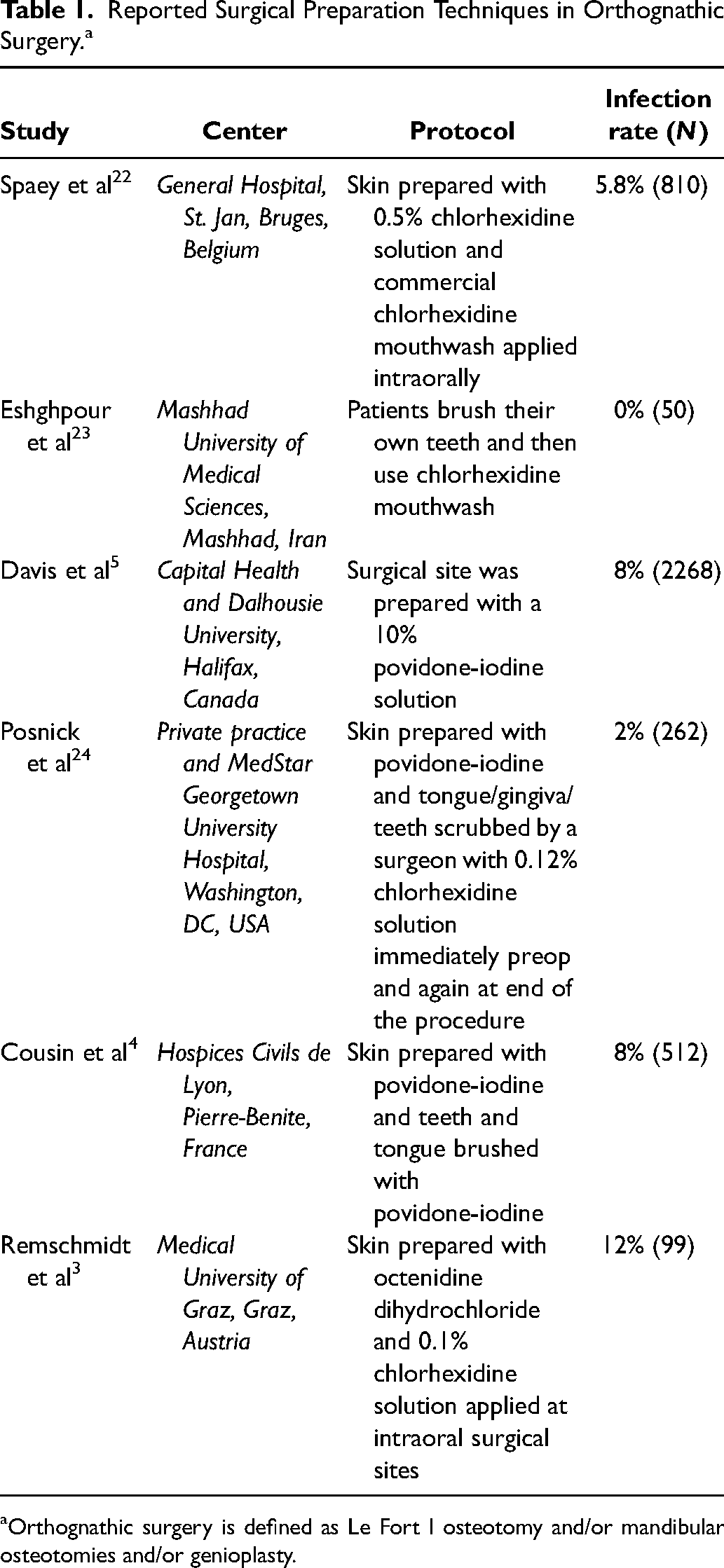
Orthognathic surgery is defined as Le Fort I osteotomy and/or mandibular osteotomies and/or genioplasty.
At our institution, practices similarly vary by surgeon. In nearly all cases, the skin of the face and neck is prepped with povidone-iodine, however, one surgeon forgoes skin preparation for maxillary-only surgery. Some within the department additionally swab intranasally with povidone-iodine, as permitted by nasotracheal intubation. The oral mucosa is either irrigated with chlorhexidine solution or swabbed with gauze saturated in povidone-iodine solution, depending on the surgeon. Two surgeons additionally brush the teeth and orthodontic appliances with either povidone-iodine or chlorhexidine. All patients receive a perioperative cefazolin bolus and some are discharged with a prophylactic course of either cephalexin or amoxicillin-clavulanate, instructions to perform chlorhexidine rinses after meals and before sleep, and saline nasal spray as needed for congestion. No specific antimicrobial measures are taken prior to surgical preparation in the operating room.
Opportunities for Innovation
Careful analysis of the literature hints at additional strategies to improve antisepsis in orthognathic surgery. For example, patients independently swishing chlorhexidine in their mouths is associated with an 8-fold reduction of bacteria in samples taken from between adjacent teeth, while a surgeon swabbing the surfaces of the mouth with gauze soaked in the same chlorhexidine solution showed a minimal effect. 19 This suggests that soft sponges or gauze are insufficient to mechanically disrupt biofilms in the interdental spaces. It is reasonable to assume that brushing would be the most effective technique for reducing bacteria in these areas, but this has yet to be specifically investigated in the context of a single pre-operative treatment.
To go a step further, professional dental cleaning within 2 days prior to orthognathic surgery is associated with a 41% relative reduction in rates of infectious complications, though the study was insufficiently powered to demonstrate statistical significance. 25 That said, it has been our experience that some patients—particularly younger patients and those with orthodontic appliances or dentoalveolar abnormalities that complicate toothbrushing—arrive in the operating room with extensive plaque buildup and even inter-dental particulate matter. These patients, and potentially others as well, would likely benefit from a routine preoperative professional dental cleaning policy. However, we recognize that additional cleanings outside of regular biannual dental visits may be unattainable for many families due to financial and time constraints.
The growing interest in nasal Staphylococcus aureus decolonization within the broader surgical community also raises the question of whether more could be done to decontaminate the nasal cavity prior to orthognathic procedures. Nasal decontamination has halved surgical site infections in orthopedic, cardiothoracic, and even Mohs surgery. 26 As such, it could be expected to have a positive effect on orthognathic procedures occurring in close proximity to the nose and nasopharynx. Comprehensive at-home chlorhexidine bathing and mupirocin nasal ointment regimens have been shown to be the most effective and longest-lasting methods of nasal decolonization, however, a single preoperative treatment of povidone-iodine formulated for the nasal mucosa is sufficient to eliminate positive cultures in 79% of patients colonized with Staphylococcus aureus. 27 Unfortunately, the deactivation of conventional formulations of povidone-iodine by nasal secretions limits its utility for this purpose. 27
Conclusion
Currently, local antiseptic practices in orthognathic surgery are variable and surgeon-dependent, with methods spread through word-of-mouth between colleagues, learned from mentors during training, or simply adapted over years of personal experience. A deficit in prospective, controlled studies has subsequently led to a lack of confidence in the antiseptic measures currently in use. 17 Increased discussions between surgeons regarding their perioperative antiseptic practices may be a first step towards optimizing perioperative management in these cases. Detailing surgical preparation protocols in research publications is another simple strategy for sharing institutional practices with a wide audience. Experimental studies documenting the effects of specific antiseptic techniques on local bacterial load would also be of great interest to many. Finally, prospective controlled studies of local antiseptic strategies and their impact on postoperative infection and complication rates will be necessary. Critically, such studies require an adequate length of follow-up, as the mean time to infection in orthognathic surgery is estimated at one month postoperatively, with hardware complications often taking even longer to surface. 4
We challenge orthognathic surgeons to consider their own antiseptic practices and opportunities to innovate and share their experiences. Given the large volume of orthognathic surgeries performed, even modest reductions in the rate of infectious complications will impact many.
Footnotes
Acknowledgments
The authors thank Drs Joseph Napoli, Eric Granquist, and Lawrence Levin for sharing their surgical experiences and current antiseptic practices.
Ethics/Informed Consent
Ethics review and informed consent are not applicable and are not needed for this manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.W.S. is a consultant for KLS Martin and Synthes. J.A.T. is a co-founder of Ostiio, LLC.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.