
Abstract
Objective
To determine whether method of maxillary advancement in adolescents with cleft palate with or without cleft lip (CP ± L) influences post-operative velopharyngeal function.
Design
Retrospective cohort.
Setting
Pediatric Tertiary Care Hospital.
Participants
One hundred and ninety-nine patients with CP ± L after LeFort I osteotomy for maxillary advancement at our institution between January 2007 and June 2019.
Interventions
LeFort I osteotomy via distraction osteogenesis (DO) or conventional osteotomy (CO).
Main Outcome Measures
Patients who underwent DO or CO were compared for the presence of new velopharyngeal insufficiency (VPI), as measured by perceptual rating by a craniofacial speech-language pathologist.
Results
Of the 199 patients who underwent maxillary advancement, 126 were available for analysis. The DO group was younger, male, and had more severe maxillary hypoplasia. Following surgery, 17/41 (41.5%) of the DO group had new VPI, compared to just 23/85 (27.1%) of the CO group. After adjusting for cleft type and predicted maxillary advancement, however, there was not sufficient evidence to reject the null hypothesis of no difference in risk of post-operative VPI between the two surgical groups (prevalence ratio [PR] 1.40, 95% CI 0.68-2.90). Increased prevalence of VPI after DO versus CO was primarily observed among patients with a pre-operative velopharyngeal need ratio < 0.8 (PR = 2.01, 95% CI 0.79-5.10) and patients with normal velopharyngeal function pre-operatively (PR = 2.86, 95% CI 0.96-8.50).
Conclusion
Our results suggest an increased rather than decreased risk of VPI following DO relative to CO. This association is primarily seen among those with a smaller velopharyngeal ratio or perceptually normal velopharyngeal function pre-operatively.
Keywords
Introduction
LeFort I osteotomy with horizontal advancement of the maxilla is a common surgical procedure used to correct maxillary hypoplasia. Conventional osteotomy (CO), or en bloc maxillary advancement in a single stage, is considered a reliable and safe procedure among patients with primary dentofacial deformities.1–3 The prevalence of maxillary hypoplasia among patients with cleft palate with or without cleft lip (CP ± L) is high, with as many as 65% of patients benefitting from surgical advancement of the maxilla. 4 Individuals with CP ± L, however, present with increased severity of hypoplasia, multi-dimensional maxillary deficiency, and scar tissue from prior surgery, making the conventional approach to LeFort I osteotomy more technically complex with relatively greater chance of negative post-operative sequelae in these patients, particularly relapse of the maxillary segment.1, 5 LeFort I osteotomy with sagittal movement via distraction osteogenesis (DO) has emerged as an alternative approach, as there is evidence that DO can provide more stable occlusal results long-term among patients with severe maxillary deficiency. 6
Velopharyngeal insufficiency (VPI) is also a potential post-operative complication of horizontal maxillary advancement in adolescents with CP ± L. VPI is characterized by nasal air emission and hypernasality during speech production secondary to atypical anatomy of the velopharyngeal (VP) port. The levator veli palatini is the primary muscle contributing to superior and posterior soft palate elevation for VP closure. 7 Re-creation of normal insertion of the levator veli palatini medially within the soft palate is the primary goal of initial soft palate repair. Because of both congenital and iatrogenic differences in VP anatomy not present in the non-CP ± L population and the anatomic relationship between the posterior maxilla and the levator veli palatini, sagittal advancement of the maxilla may interfere with the ability to achieve VP closure post-operatively in patients with CP ± L.8–10
While there is generally consensus that the prevalence of VPI increases after maxillary advancement surgery in adolescents with CP ± L, the magnitude of and subgroups more susceptible to this change are highly variable due to significant heterogeneity in the methodologic approach to these questions in the literature. Following CO, the proportion of patients with a decline in VP function has ranged from 11% to 24% across studies.8, 11–15 Type of cleft was found to be a predictor of VPI in some studies but not in others.11, 16 Similarly, a greater magnitude of advancement needed to achieve normal occlusion has been associated with a greater risk of post-operative VPI only in some studies.14, 15, 17–19
Maxillary advancement surgery is often considered the end of a timeline of care spanning the patient's childhood and occurs at a time of great transition in a young adult's life. 20 Quality of life (QoL) studies in patients with CP ± L suggest a relatively lower QoL in the presence of VPI.21–23 Therefore, it is of great interest to providers, patients, and patients’ families to identify a surgical technique that fulfills the surgery's physiologic and aesthetic purpose long-term while simultaneously minimizing risk of adverse functional changes leading to need for further surgery.
It has been posited that DO could reduce the risk of post-operative VPI compared to CO in individuals with CP ± L because the anatomic changes related to DO occur over a period of time. 24 The results of two small studies support the hypothesis of a reduced risk of VPI in patients who underwent DO after controlling for magnitude of advancement, but incomplete follow-up in both studies raised concern for selection bias in their results, as differences in those who did versus did not return for follow-up were not discussed.24, 25
The present study aimed to address the following questions in a large cohort of patients with CP ± L who underwent LeFort I osteotomy with sagittal maxillary advancement: (1) When a similar magnitude of advancement is required between groups, does the prevalence of post-operative VPI differ between the two surgical techniques and (2) Does the association between surgical approach and risk of post-operative VPI differ according to patient characteristics, including type of cleft, presence of borderline VPI pre-operatively, pre-operative VP need ratio (nasopharyngeal depth divided by soft palate length 26 ), and history of prior VPI surgery. Factors also associated with risk of VPI and indication for surgical approach (eg, magnitude of maxillary advancement) are carefully accounted for in the analysis and effects of different subgroups on results are discussed, thereby enhancing available evidence when considering risk of changes in VP function following surgical advancement of the maxilla in this population.
Methods
Participants
For this retrospective cohort study, eligible participants were identified from an internal access database that includes demographic, diagnostic, and surgical data for all patients treated in the Craniofacial Center over the last 20 years. All patients with CP ± L who underwent initial LeFort I osteotomy for maxillary advancement at our center between January 2007 and June 2019 were extracted from this clinical database for inclusion in this study. For inclusion, patients had to have adequate pre-operative VP function in the presence of a cleft of the secondary palate of any type with or without a cleft lip (CP ± L). Patients with both syndromic and non-syndromic CP ± L were included in the study population, as the relationship between syndrome diagnosis and surgical approach or risk of post-operative VPI was through other variables already included in analyses rather directly associated. Those with cleft lip/alveolus only were excluded, as were patients with repeat LeFort I osteotomy procedures or those with LeFort I osteotomy procedures not involving anterior movement of the maxilla (eg, surgically assisted maxillary expansion). All demographics, surgical history, and medical data obtained from the internal database were verified in the electronic medical record. All participants underwent standard surgical and orthodontic evaluation with lateral cephalometric radiographs as well as pre-/post-operative perceptual evaluation of VP function per clinical protocol. This study was approved through expedited review by the Institutional Review Board at the University of Washington (IRB #STUDY00008156). Because all data utilized in the study were present in the electronic medical record or in internal databases, written consent/assent was waived.
Surgical Characteristics
All participants underwent LeFort I osteotomy with pterygomaxillary disjunction and down-fracture, as described in the literature.2–4 For CO, the newly-mobile maxilla was placed into a prefabricated acrylic surgical splint to obtain intermaxillary fixation then wired together. The newly-mobile maxilla was secured into the splint in its baseline position for DO. Rigid external distractors (RED) were then secured to the temporal bone and the splint and RED device were secured together with wires. After a 3-day latency period, activation of distraction is initiated at 1 mm per day until a class I occlusion relationship is achieved, typically between 7 and 15 days. Over the study period, six surgeons completed maxillary advancement surgery at our institution. Surgical approach classified as DO or CO, the primary comparison of interest, was identified directly from operative reports. As indicated by pre-surgical evaluation, completion of multi-dimensional expansion (as indicated by “multi-segmental osteotomy”), mandibular osteotomy, and alveolar bone graft were also recorded. Individuals undergoing these concurrent procedures remained in the study population, as no evidence exists that suggests a relationship between these procedures and risk of VPI after maxillary advancement.15, 27
Lateral Cephalometric Measurement
A lateral cephalometric radiograph was completed pre-operatively and serially post-operatively, per protocol. All lateral radiographs were taken using the same cephalostat with patient aligned to Frankfurt horizontal, molars in occlusion, and with the lips and soft palate at rest. For analysis, the radiographs closest to the date of surgery pre-operatively and to the date of perceptual VP function evaluation post-operatively were used. Two orthodontists with the Craniofacial Center completed digitized tracings of pre- and post-operative radiographs for each participant using commercially available cephalometric analysis software (Dolphin Imaging Premium 11.95). Magnification differences were accounted for in tracings. For reference, the horizontal axis was established by dropping a line seven degrees from the center of sella turcica (S) to nasion (N).28–30 The vertical axis was then identified by a line drawn perpendicular to the x-axis through S. Documented landmarks are illustrated in Figure 1a. Definitions of each linear measurement using these landmarks are summarized in Figure 1b. Overjet and anterior-posterior maxillary deficiency are two ways to measure the degree of maxillary hypoplasia. In the current study, overjet was chosen as the primary variable associated with indication for surgical approach. Soft palate length and nasopharyngeal depth were measured to calculate the VP need ratio, defined by nasopharyngeal depth in the numerator and soft palate length in the denominator, an anatomic indicator for the ability to achieve VP closure during speech.26, 31–33 Ten percent of radiographs were traced by both orthodontists to evaluate inter-rater reliability. Each orthodontist also retraced 10% of radiographs to evaluate intra-rater reliability.31, 32
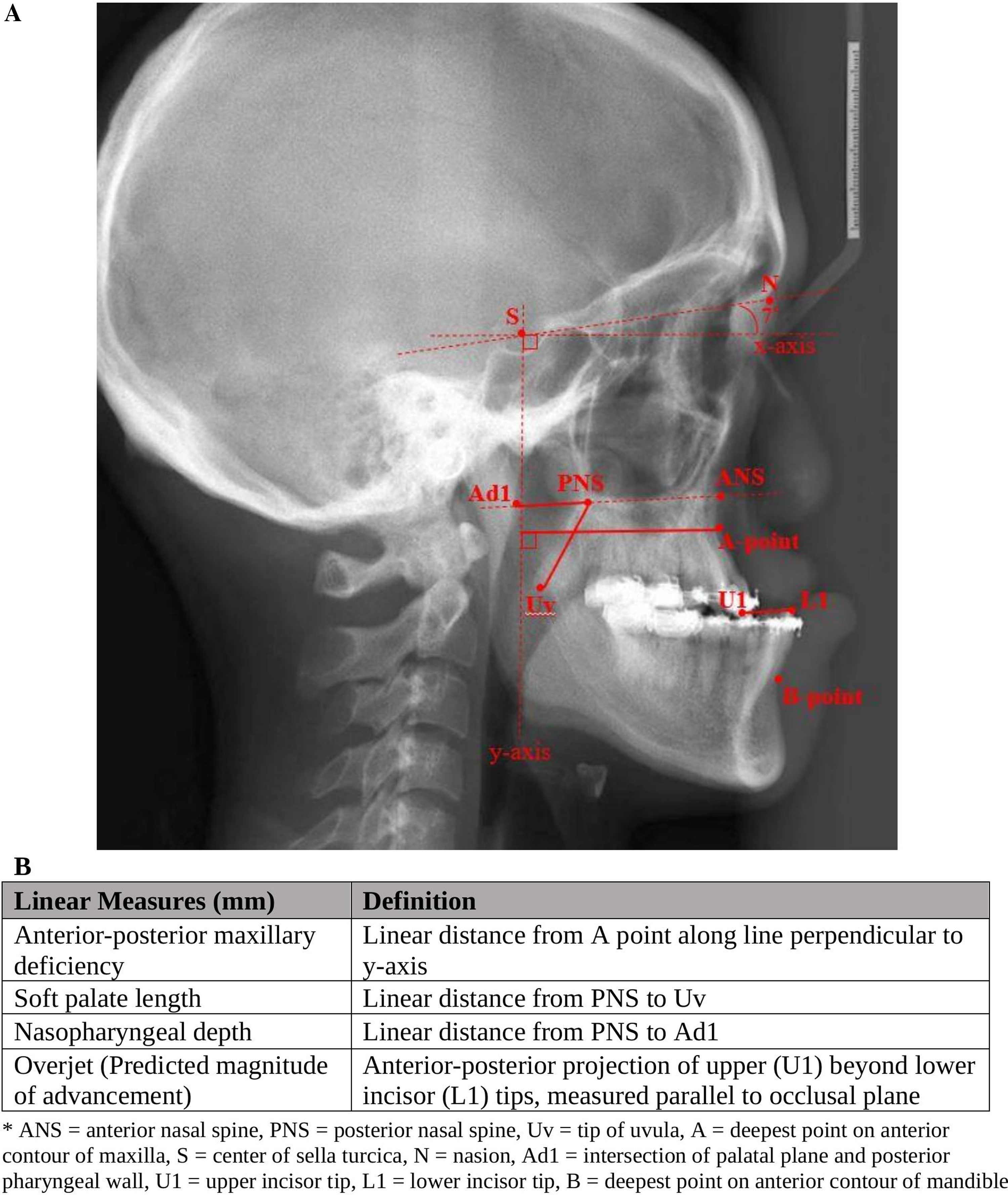
Panel A demonstrates location of landmarks used in linear measurements on lateral cephalometric x-rays. Planes of reference are indicated by a dashed line and linear measurements used in analysis are indicated by solid lines. Panel B provides definitions of each measurement used in analyses.
Perceptual Evaluation of Velopharyngeal Function
Perceptual speech evaluation by a speech-language pathologist (SLP) specializing in the evaluation and management of VP dysfunction has been the standard of care at our institution since 2007. Six SLPs contributed evaluations over the 12-year study period, three of them contributing ratings for less than 2 years, two for half the study period, and another for the entire study period. Severity ratings related to articulation, resonance, and nasal air emission based on overall clinical evaluation are stored in a second internal database specific to speech outcomes. VPI and hypernasality ratings for each eligible participant were extracted from this database for the current study. Both VPI and hypernasality are rated on a 5-point severity scale with definitions as described in Figure 2. In 2014, definitions for levels of hypernasality were reviewed with intent to transition to use of the CAPS-A-AM (Cleft Audit Protocol for Speech-Augmented Americleft Modifications) in our evaluation protocol. 34 Because the definitions for degrees of hypernasality did not meaningfully differ, hypernasality ratings made prior to this transition were also included. Meaningful differences did exist in the definitions for degree of nasal air emission and hyponasality, thus these speech parameters were not analyzed. Our evaluation of VPI severity remained consistent across the study period.
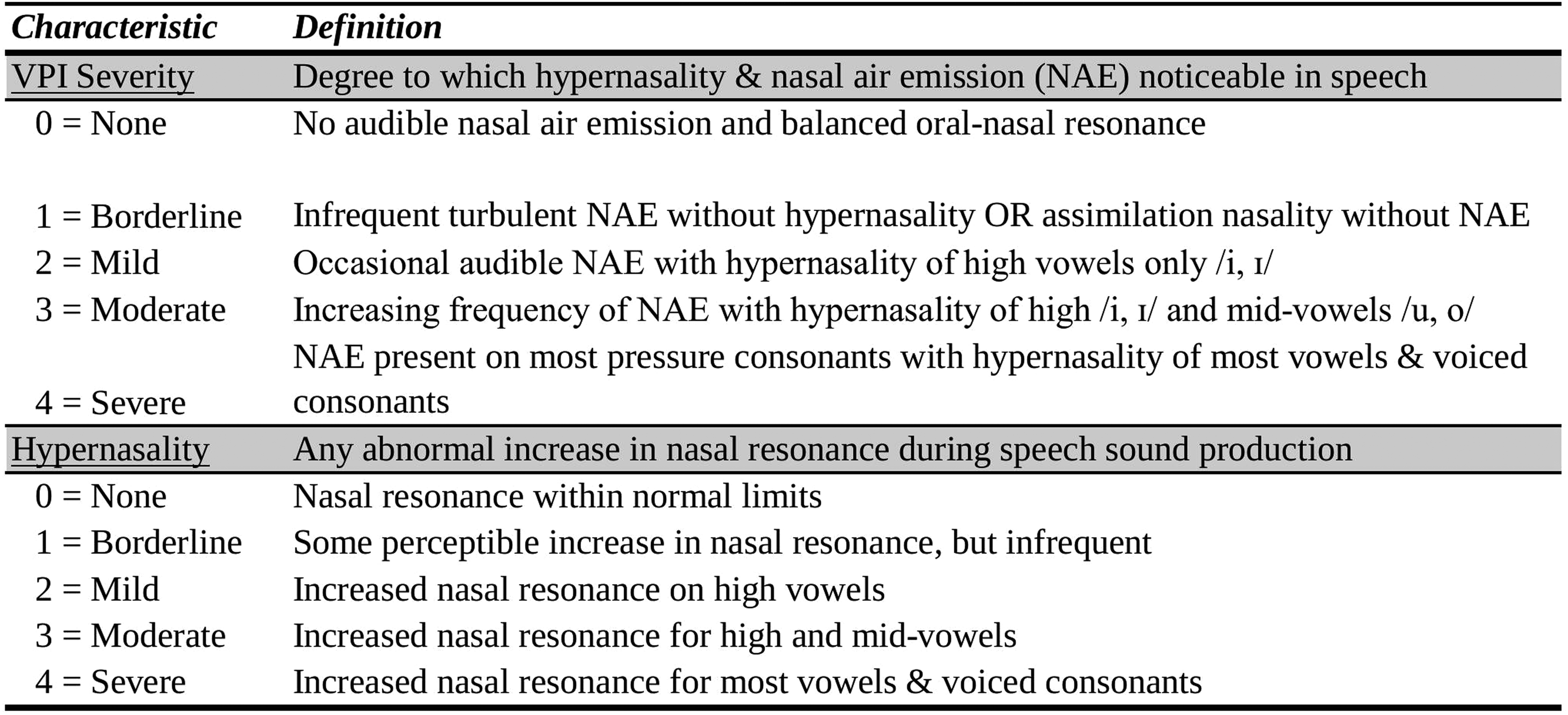
Description of severity levels of velopharyngeal insufficiency (VPI) used to define outcome.
Speech audio recordings of patients included in the study were not available on the entire study cohort, as obtaining recordings did not become a consistent part of our clinical protocol until 2019. Therefore, inter- and intra-rater reliability for hypernasality and VPI (as defined in Figure 2) were assessed using 50 audio recordings of patients with similar age and diagnosis to our study population. These recordings included syllable repetition, sentence repetition and counting 1 to 20 and 60 to 70 (see Appendix A) and were obtained using a Sony Digital ICD Recorder with a Sony Stereo ECM-CS3 lapel microphone in a quiet exam room. Three of the six SLPs (representing 12, 6, and 2 years of the study period) listened to each recording using high-quality over-the-ear headsets. Each of the three SLPs re-rated 20% of audio recordings 2 weeks after initial ratings to measure intra-rater reliability.
Statistical Analysis
Patients were divided into two exposure groups by type of procedure, either DO or CO, as determined from the operative report. The primary outcome was presence of post-operative VPI, defined by a rating of 2 to 4 (mild, moderate, or severe). Post-operative VPI rated as normal or borderline (rating of 0 or 1, respectively) was categorized as absence of VPI. Patients with pre-operative VPI (rating of 2-4) were excluded from analyses to ensure observed post-operative VPI was plausibly associated with surgery. To prevent distortion of the observed association between surgical approach and post-operative VPI, differences in the prevalence of additional variables (potential confounders) between the DO and CO groups were investigated through a priori clinical knowledge as well as a data-driven approach. 35 In general, confounders are defined as variables related in some way to both exposure (surgical approach) and outcome (post-operative VPI). 36 If not adjusted for in analyses, a confounder may lead to biased results. In our study, there were differences observed in the magnitude of maxillary advancement (defined as the linear distance between the between the upper and lower incisal tips) as well as type of cleft between the two surgery groups. Therefore, all analyses were adjusted for these two variables.
Multivariable relative risk regression using the Poisson likelihood function 37 was then run to estimate the difference between DO and CO on the prevalence of post-operative VPI. Effect measures with confidence intervals are reported. Effect of loss to follow-up (missing outcome measurement) between the two surgical groups was investigated using widely-accepted epidemiologic approaches to handling of missing data.38–40 Meaningful differences between those who did and did not return for follow-up were not identified, thus complete-case analysis was considered a valid approach. Analyses were also run to assess whether the association between surgical approach and presence of VPI after surgery differed across patients with different clinical characteristics, including prior history of Furlow palatoplasty (for initial repair or as VPI surgery), prior history of any VPI surgery (Furlow palatoplasty, sphincter pharyngoplasty, or pharyngeal flap), size of pre-operative VP need ratio (dichotomized at 0.8),33, 41 and pre-operative VPI status (rating of 1 vs. 0). Two-way mixed consistency single-measures intra-class correlation coefficients (ICCs) were calculated for all cephalometric measurements, for both inter- and intra-rater reliability. 42 For perceptual speech ratings, weighted kappa 43 and ICCs were calculated for intra- and inter-rater reliability, respectively. Interpretation of reliability coefficients as defined by Cicchetti et al. were used. 44 Independent samples t-tests were used to evaluate consistency of measurements within and between orthodontists contributing cephalometric tracings. All analyses were completed in R, version 4.0.3. 45
Results
After excluding patients who had pre-operative VPI or who underwent LeFort I osteotomy that did not involve anterior displacement of the maxilla, there remained a total of 199 patients who underwent either DO (N = 50) or CO (N = 149) for maxillary advancement over the 12-year study period. Table 1 summarizes baseline patient characteristics, stratified by surgical approach to maxillary advancement. Briefly, those undergoing DO tended to be younger (mean age 15 vs 18.9 years in the CO group), were more likely to be male (74% DO vs 56% CO) and on average required a larger magnitude of maxillary advancement to achieve desired occlusal outcome than those undergoing CO (−11.5 overjet DO vs −3.5 CO). The proportion of Asian individuals was nearly two times as great in the DO group (34%) compared to the CO group (19.3%), while the proportion of white or other race was just modestly greater in the CO group. Those in the CO group were more likely to have a syndrome diagnosis and included a larger proportion of participants with a cleft of the secondary palate than those in the DO group. The proportion of bilateral cleft lip/palate (BCLP) was greater among those undergoing DO while the proportion of unilateral cleft lip/palate (UCLP) was relatively balanced between surgery groups. Presence of borderline pre-operative VP function was relatively balanced between exposure groups. Patients requiring concurrent mandibular setback or advancement were almost entirely confined to the CO group.
Pre-Operative Patient Characteristics Stratified by Type of Surgery.a, b
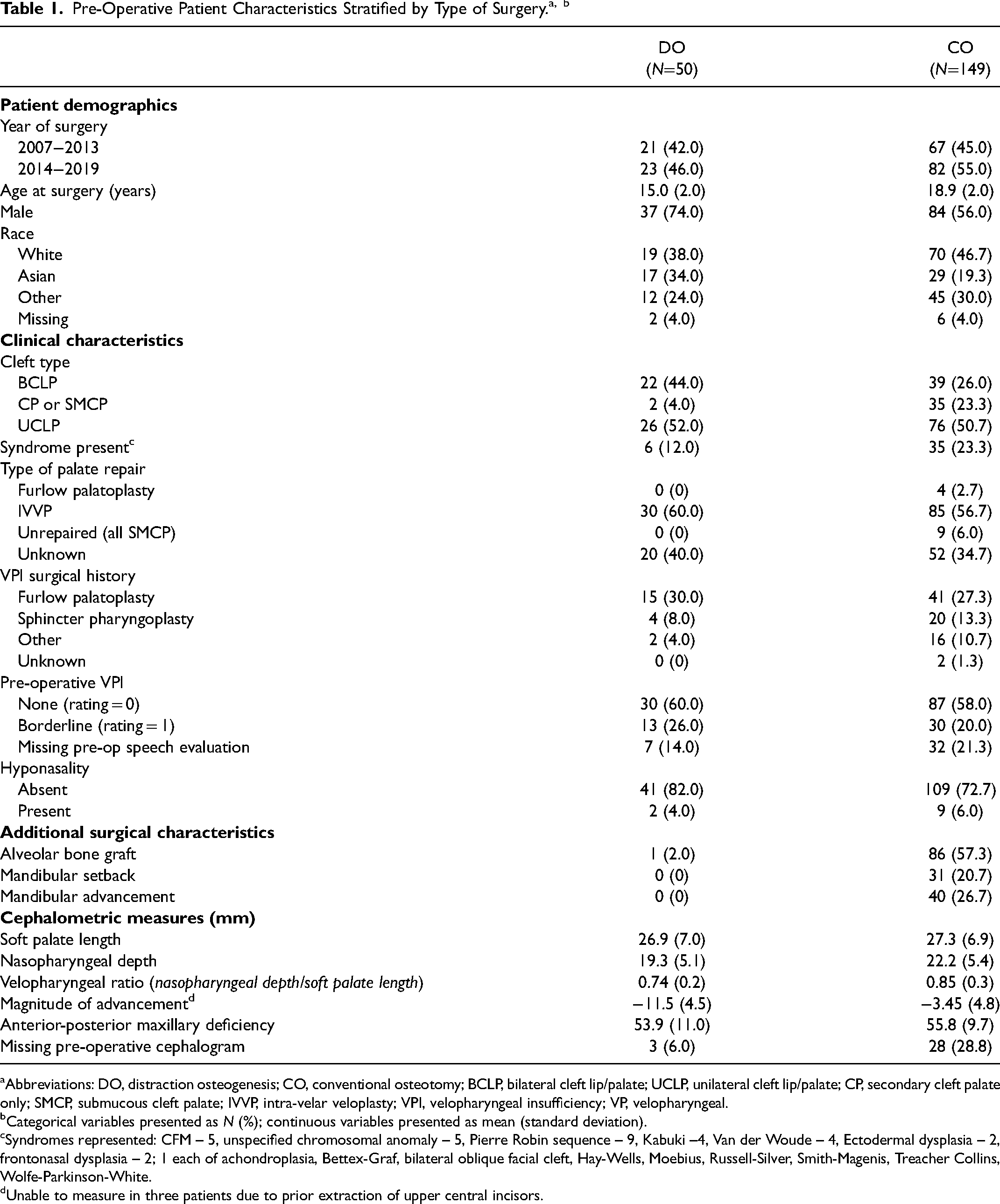
Abbreviations: DO, distraction osteogenesis; CO, conventional osteotomy; BCLP, bilateral cleft lip/palate; UCLP, unilateral cleft lip/palate; CP, secondary cleft palate only; SMCP, submucous cleft palate; IVVP, intra-velar veloplasty; VPI, velopharyngeal insufficiency; VP, velopharyngeal.
Categorical variables presented as N (%); continuous variables presented as mean (standard deviation).
Syndromes represented: CFM – 5, unspecified chromosomal anomaly – 5, Pierre Robin sequence – 9, Kabuki –4, Van der Woude – 4, Ectodermal dysplasia – 2, frontonasal dysplasia – 2; 1 each of achondroplasia, Bettex-Graf, bilateral oblique facial cleft, Hay-Wells, Moebius, Russell-Silver, Smith-Magenis, Treacher Collins, Wolfe-Parkinson-White.
Unable to measure in three patients due to prior extraction of upper central incisors.
Pre-operative cephalometric radiographs completed more than 100 weeks before surgery were considered missing. Median time between pre-operative cephalometric radiographs and date of surgery was 2.93 weeks (IQR 2.14-8.04). Median time between pre-operative speech evaluation and surgery date was 21.6 weeks (IQR 3.00-76.6). Absence of interim VPI surgery was confirmed for all participants. Speech evaluations completed more than 2 years before surgery were considered missing.
Reliability
ICCs revealed good to excellent inter- and intra-rater reliability for all cephalometric measures used in analyses (ICCs ranging from 0.75 to 0.99). ICCs for inter-rater reliability of VPI and hypernasality were 0.77 and 0.75, respectively, also revealing good agreement across the three raters. Weighted kappa values revealed good to excellent intra-rater reliability for each SLP, with values ranging from 0.69 to 0.95 for VPI and hypernasality.
Relative Risk Regression
In this study, relative risk regression methods provide a prevalence ratio (PR) that is a comparison of the likelihood (or prevalence) of post-operative VPI occurring after undergoing DO relative to the likelihood of post-operative VPI in the group that underwent CO for maxillary advancement. Adjustment for differences in additional characteristics between groups (ie, cleft type and magnitude of maxillary advancement) addresses concern for bias in results due to their association with both indication for surgical approach and risk for post-operative VPI. Of the 199 that underwent maxillary advancement during the study period, 73 did not return for post-operative speech evaluation. Therefore, 126 patients were included in the analysis (41 in the DO group and 85 in the CO group). The PRs of VPI were estimated across the whole cohort as well as within the subgroup with UCLP. Small sample size among groups with BCLP or CPO/SMCP did not allow investigation of the association between surgical approach and risk of VPI within these subgroups. Models including the whole cohort were adjusted for type of cleft and magnitude of maxillary advancement, while subgroup models were adjusted just for magnitude of maxillary advancement.
In the DO group, 41.5% of patients (17 of 41) presented with new VPI post-operatively, in contrast to just 21.7% of patients (23 of 85) in the CO group. After adjustment, this PR was 1.40 (95% CI 0.68-2.90), suggesting a 40% higher risk of VPI following DO compared to after CO. However, we are unable to reject the null hypothesis of no difference between groups (P=.36). The modest excess of post-operative VPI among patients in the DO group observed in the entire patient population was also seen when the data for children with UCLP were analyzed independently (adjusted PR 1.49, 95% CI 0.59-3.75, P=.40). Table 2 summarizes these results.
Crude and Adjusted Relative Risk of VPI Comparing DO and CO.a
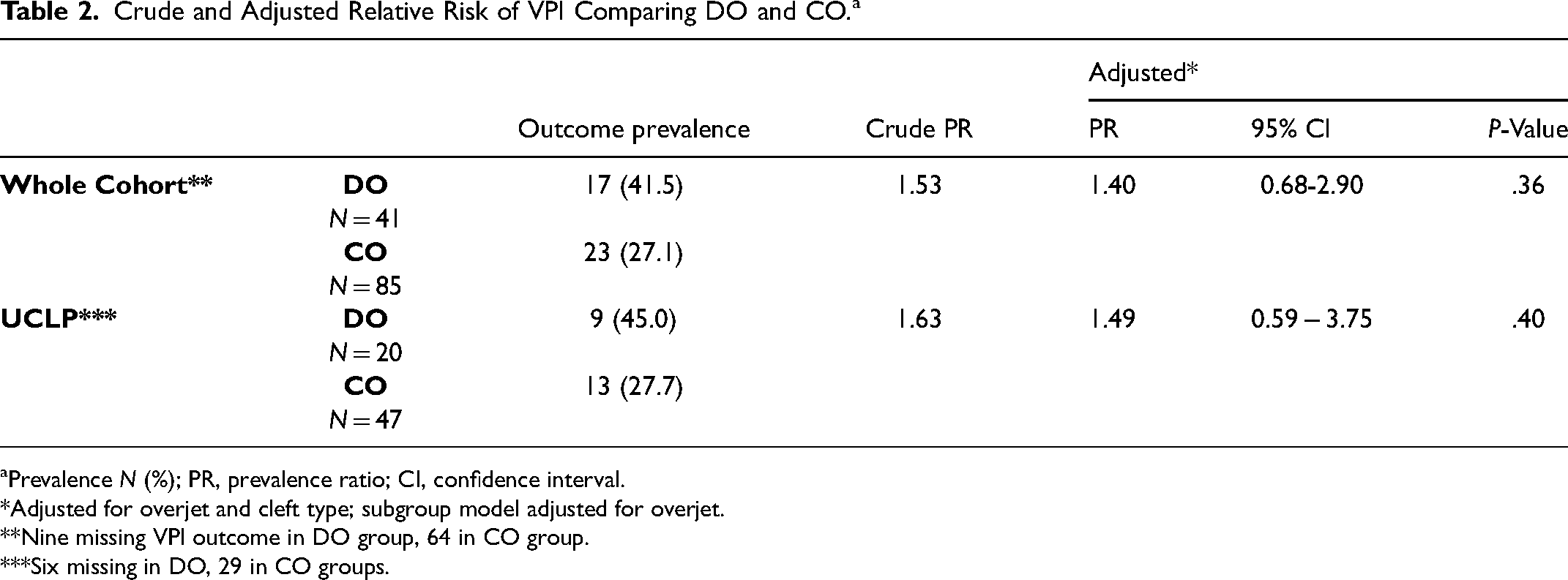
Prevalence N (%); PR, prevalence ratio; CI, confidence interval.
Adjusted for overjet and cleft type; subgroup model adjusted for overjet.
Nine missing VPI outcome in DO group, 64 in CO group.
Six missing in DO, 29 in CO groups.
The forest plot in Figure 3 illustrates results of relative risk regression that compares the PRs for risk of VPI between DO and CO within indicated subgroups. Each shape represents the PR for each additional characteristic and each color allows comparison of the PRs between presence versus absence of that characteristic (eg, between those with vs without history of Furlow palatoplasty). The size of the PR comparing risk of VPI after DO relative to after CO do not meaningfully differ in between groups with (n = 35) or without (n = 91) history of Furlow palatoplasty (PR 1.52, 95% CI 0.46-5.01 for presence of Furlow vs 1.41, 95% CI 0.62-3.16 for no Furlow) or history of any VPI surgery (n = 50, PR 1.4 95% CI 0.5-3.86 with VPI surgery vs n = 76, PR 1.47, 95% CI 0.62-3.52 without VPI surgery) and all of these are comparable to the size of the association observed within the entire cohort (top line). However, an increased prevalence of VPI associated with having undergone DO was primarily seen in patients who had a pre-operative VP need ratio less than 0.8 (n = 66, PR = 2.03, 95% CI 0.80-5.17). Similarly, only in patients with normal pre-surgical VP function (rating of 0) was there an increased risk of VPI associated with receipt of DO (n = 81, PR = 2.85, 95% CI 0.99-8.17).
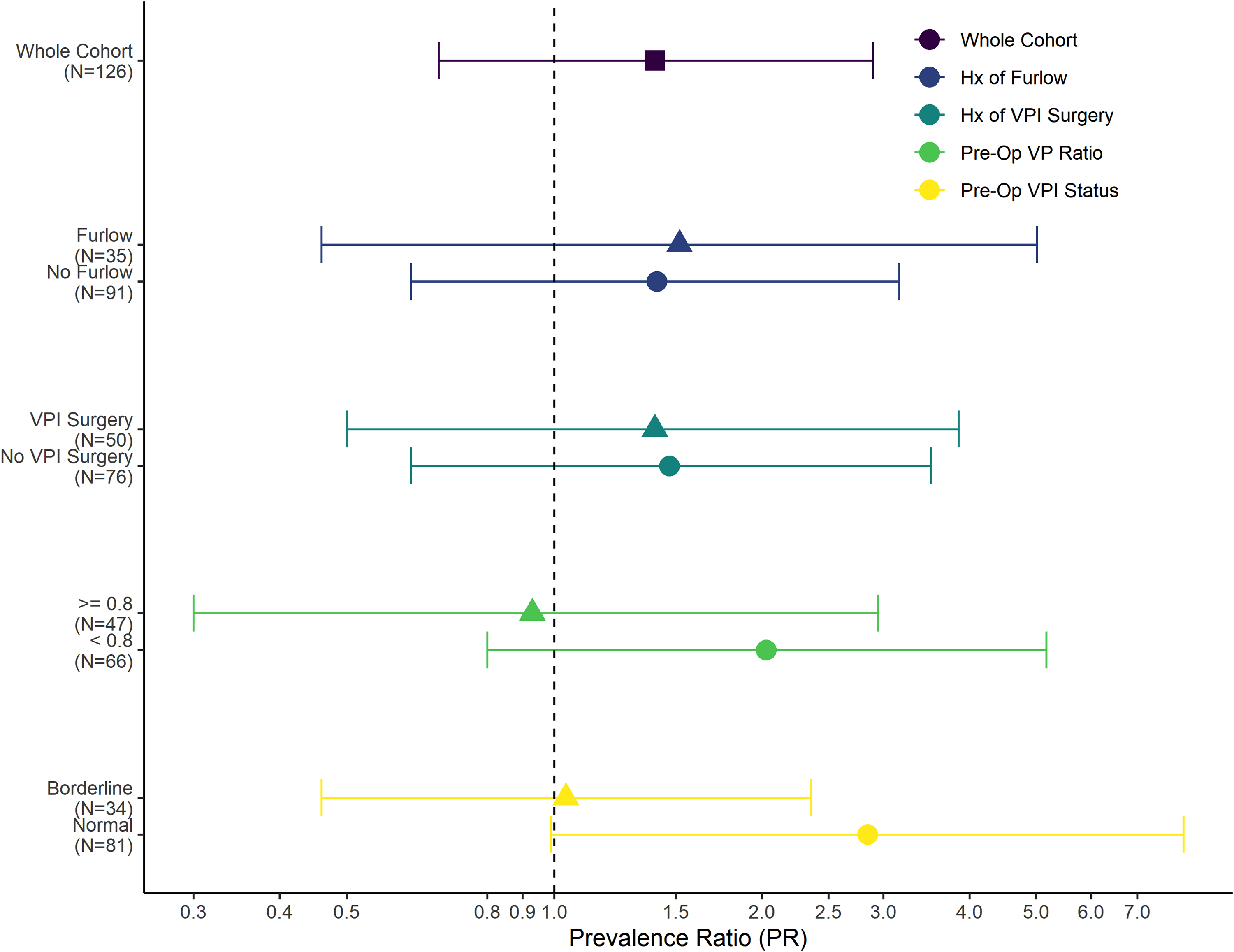
A forest plot depicting the prevalence ratios comparing risk of VPI between DO and CO for presence (line with triangle) versus absence (line with circle) of each characteristic. Results for the whole cohort appear at the top (line with square). Error bars mark the 95% confidence intervals. Null result of a PR = 1.0 (no difference in prevalence of VPI between surgery groups) is shown as a dashed line.
Discussion and Conclusion
After adjustment for relevant confounders, our results suggest a modest increase in prevalence of VPI following DO relative to that among patients following CO for maxillary advancement (PR 1.40, 95% CI 0.68-2.90). Similar results were observed when patients with UCLP were analyzed separately. Wide confidence intervals, however, indicate a range of values where the true value may lie and because these include the null of 1.0, we are unable to reject the null hypothesis in these analyses. Additionally, we observed a trend towards increased post-operative VPI risk for DO relative to CO among participants with a VP need ratio of less than 0.8 (PR 2.0, 95% CI 0.8-5.17) or among those with absence of VPI (rating = 0) pre-operatively (PR 2.85, 95% CI 0.99-8.17). While imprecision exists in these subgroup analyses as well, our results are a high quality measure of a potential association and are consistent with a greater risk of VPI after DO versus CO in these subgroups and would be of high clinical importance if confirmed.
In a randomized trial of patients with CP ± L requiring between 4 and 10 mm of advancement, 47 patients underwent either DO (N = 22) or CO (N = 25). 25 Post-operative data on speech were available for only 10 subjects in the DO group and 11 subjects in the CO group. Using a definition of presence versus absence of hypernasality, 4 of 11 participants in the CO group presented with new hypernasality post-operatively while none of the 11 participants who underwent DO demonstrated new post-operative hypernasality. Comparable results were obtained for other measures of post-operative VP function analyzed in their study, including nasalance values, nasoendoscopic findings, and nasal air emission. A cohort study of individuals with moderate to significant maxillary hypoplasia (projected > 10 mm of advancement) compared prevalence of post-operative VPI between 20 patients who underwent DO and 11 who underwent CO, defining presence of VPI as a score of greater than three on the Pittsburgh Weighted Speech Scale (PWSS).13, 24 They reported that 82% of patients who received CO and 45% of patients who received DO met their criteria for post-operative VPI (z-test to compare proportions between groups, P=.05). Results from both of these studies suggest that the risk of post-operative VPI is lower in those undergoing DO compared to CO, the opposite direction of association than observed in our study. However, differences in measurement of VPI, as well as approach to statistical analysis, suggest need for cautious comparison of results across studies.
In the current study, it is possible that some bias was introduced by our definition of the predicted magnitude of maxillary advancement. While the projection of the upper beyond the lower incisal tip (“overjet” in orthodontic literature) was identified as the best variable to address confounding by indication for surgical approach in the current study, overjet may result in misclassification with respect to the actual anterior maxillary movement required among patients requiring bimaxillary surgery. During study design, we opted to include those undergoing bimaxillary surgery in the study population, as there was no clinical indication that the addition of mandibular surgery would bear on the risk of post-operative VPI. In the two earlier studies, bimaxillary procedures were excluded, whereas in the current study those requiring concurrent mandibular surgery were present only in the CO group. Although sensitivity analysis of a patient subgroup that excluded individuals receiving bimaxillary surgery revealed no change in the observed association, it is possible our results reflect some degree of differential misclassification of the confounder, contributing to the observed increased risk of VPI among patients undergoing DO compared to those undergoing CO. Defining predicted magnitude of advancement in a way that does not rely on mandibular landmarks should be considered in future studies.
Potential for unmeasured confounding in our analysis also warrants mention. While variables suggestive of early surgical history in our cohort (ie, type of initial palate repair and VPI surgical history) did not suggest an imbalance of these across surgery groups, it was noted that the proportion of those of Asian descent in the DO group (34%) was greater than would be anticipated given that just 15% of all patients with CP ± L served in our center identify as Asian. While a sensitivity analysis adjusting for race did not meaningfully alter our results, it is also known that approximately 15% of all patients with CP ± L at our center are internationally adopted and many come from Asian countries. On average, internationally-adopted patients undergo palate repair ten months later than their non-adopted peers and often have variable quality and clarity of their prior surgical history, 46 suggesting inherent differences in this subpopulation compared to patients who received multidisciplinary team care since birth. A post hoc review of our study population did reveal a difference in the proportion of internationally-adopted patients between exposure groups (25% in the DO group vs just 7% in the CO group). While adoption status itself would not alter the effect of surgical approach to maxillary advancement on post-operative VPI, it is plausible that the higher risk of VPI observed in those who underwent DO was due, at least in part, to the larger proportion of that group having suboptimal early surgical history compared to the CO group. Future studies comparing risk of VPI after distraction versus a conventional approach to maxillary advancement in adolescents with CP ± L should ensure availability of data that adequately delineates the complex relationship between early surgical history and later risk in their study design.
While loss to follow-up is a common challenge in retrospective studies, differences observed in the proportion of those who did not return for post-operative speech evaluation across surgical groups (18% in the DO group vs 44% in the CO group) warrants further discussion. In practice, this discrepancy could be attributed to the fact that those undergoing DO tended to be younger and therefore had more opportunity to return for speech evaluation prior to aging out of our pediatric institution at 21 years of age. Aside from age and surgical approach, no other baseline patient characteristics differed between those that did versus did not return for follow-up. Theoretically, it is often assumed that patients who have no speech concerns have a lower likelihood of returning for follow-up, and thus would have a lower likelihood of having been assessed for the presence of post-operative VPI. Making this assumption leads us to consider of the effect differential follow-up on our results. Because a relatively larger proportion of patients who underwent CO did not receive a post-operative speech evaluation, it is plausible that the prevalence of post-operative VPI in this group was spuriously high. If it is assumed that 10% of those with unobserved outcome truly did have VPI post-operatively, this would increase the number of participants with VPI by just one (10% of 9 with unobserved outcome) in the DO group and by six (10% of 62 with unobserved outcome) in the CO group. After accounting for the differences in proportion of unobserved outcome in the two surgery groups, the prevalence of post-operative VPI in both groups would decrease, but the magnitude of this decrease would be greater in the denominator of the PR (the CO group) than it is in the numerator (the DO group). If true, then the magnitude of the risk of VPI after DO relative to CO may be greater in truth than observed in our results. Table 3 illustrates these differences.
Observed Versus Predicted Prevalence of Post-Operative VPI Based on Assumption of 10% of Those That did not Return for Follow-Up as Having VPI.

Subgroup analyses demonstrated some trends in differences in risk of VPI after DO versus CO dependent on how the subgroup was defined. In patients with a VP need ratio of < 0.8 on pre-operative cephalometric radiographs, DO was associated with a two-fold increase in risk of post-operative VPI (PR 2.01, 95% CI 0.79-5.10). Though it would be reasonable to attribute this increase in risk among those with smaller pre-operative VP need ratio to a need for greater magnitude of anterior movement, these results were already adjusted for this variable. Nonetheless, it is possible that adjustment for a more accurate measure of the magnitude of maxillary deficiency—such as the distance from A-point to the line perpendicular to the x-axis at sella turcica—would have led to a PR closer to the null. Sensitivity analyses that adjusted for this definition of advancement rather than overjet did not suggest obvious residual confounding, however.
Despite the greater prevalence of post-operative VPI among those with borderline versus normal pre-operative perceptual VP function (15 of 34 and 21 of 81, respectively, data not shown), the risk of post-operative VPI between DO and CO only differed among those with normal pre-operative VP function, with DO associated with more than a 2.5-fold increase in risk compared to CO (PR 2.86) in this group. The rationale for running this comparison assumed that those with borderline VP function before maxillary advancement would be more likely to develop VPI after surgery. However, the smaller sample size for those presenting with borderline VPI (13 in the DO group and 21 in the CO group) may have precluded our ability to identify an association after adjustment and accounting for missing data. It is also plausible that perceptual ratings of VPI are not sensitive enough to reliably differentiate between truly normal and borderline function and perhaps direct visualization of the VP port (ie, nasopharyngoscopy) would reduce the potential for misclassification in this variable.
Our study highlights the complex relationships between surgical approach, cephalometric measurements, and prior surgical history when comparing distraction to a conventional approach to maxillary advancement on the risk of post-operative VPI in adolescents with CP ± L. To date, all studies investigating whether the type of maxillary advancement surgery influences risk of impaired VP function post-operatively warrant cautious interpretation. Our results suggest an increased rather than a decreased risk of VPI following DO relative to after CO that would be of high clinical importance if confirmed in future studies. Similarly, there is insufficient evidence to suggest that the surgical approach to maxillary advancement has a greater deleterious impact on VP function in some subgroups of patients more than in others. Our results suggest pre-operative VP ratio and presence of no perceptual VPI pre-operatively as characteristics that warrant further evaluation in this regard and form a basis for future studies to best estimate these associations in a rigorous way.
Footnotes
Acknowledgments
The authors would like to thank Annie Nguyen, DDS, for her contribution of lateral cephalometric x-ray measurements needed to evaluate inter-rater reliability.
Authors’ Note
This study was approved through expedited review by the Institutional Review Board at the University of Washington (IRB #STUDY00008156). Because all data utilized in the study were present in the electronic medical record or in internal databases, written consent/assent was waived.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Advancing Translational Sciences (grant number TL1 TR002318).
Appendix
A. Speech sample used in audios reviewed for inter- and intra-rater reliability: