
Abstract
Objective
Using both endoscope and exoscope in cleft soft palate surgery is not widespread, despite the potential advantages related to view magnification, ergonomic posture of the surgeon, and involvement of the surgical team.
Design
The aim of the current study is to compare endoscopic (Olympus Visera©) and exoscopic (Karl-Storz Vitom©) assistance in cleft soft palate surgery in a preclinical cadaver setting.
Setting
A formalin fixed specimen was dissected to mimic the anatomical conditions of a cleft soft palate.
Participants
Ten young surgeons with limited experience in transoral surgery were involved in the exercitation on the specimen.
Interventions
The exercitation consisted of 4 tasks: (1) device setting; (2) identification of muscle plane; (3) muscle suturing; (4) oral mucosa suturing.
Main outcomes
Participants were timed while performing each task both with exoscope and endoscope and asked to fill in 2 questionnaires related to the visual systems used (NASA Task Load System TLS and VAS 1-10).
Results
All surgeons completed the 4 tasks with both the endoscope and exoscope. The execution times were similar except for faster setting of the exoscope. Participants felt that completing surgical exercises using the exoscope required less physical, intellectual, and temporal efforts compared to the endoscope. The exoscope was also more appreciated for its handling, 3D visualization, and limited encumbrance.
Conclusions
Exoscope scored better both at NASA TLS and VAS 1-10 and required a faster setting than endoscope. Further clinical in-vivo studies are required to explore the advantages of these devices in cleft palate repair.
Introduction
Cleft palate surgery is a challenge for the specialist who must reconstruct the complex anatomy of the soft palate with the aim of achieving adequate functional outcomes. 1 In fact, there are several critical issues related to this kind of surgery dictated by the minute anatomical structures to be reconstructed and difficult access through the oral cavity of pediatric patients, which results in poor vision, discomfort for the operator, and limited involvement of the surgical team. 2 Furthermore, it is estimated that 83% of American cleft surgeons are affected by work-related musculo-skeletal injuries due to the inappropriate posture required for palatoplasty procedures. 3
Traditionally, palatoplasty is performed with surgical loupes, which offer good magnification but do not solve the postural problems and scarce staff involvement. In 2003, Sommerlad 4 introduced the use of the microscope for cleft palate repair, emphasizing the potential benefits related to huge magnification, more comfortable posture, and greater involvement of operating room staff. Despite this innovation, surgical loupes are still widely used because of the difficult adaption to the operating microscope and the long learning curve needed. 5 Furthermore, although the microscope has been reported to be suitable for visual assistance of the entire palatoplasty, 5 its use is usually limited to muscular plane dissection, 6 with reduced advantages for posture and surgical team involvement.
In the last years, video assistance using endoscopes supported by an arm holder has been introduced for cleft soft palate surgery, allowing to perform surgery with both hands free and to magnify the surgical field on a widescreen thanks to the use of a 0° optic camera connected to a light source. 7
More recently, exoscopy has been introduced in a variety of head and neck surgical settings.8–10 The 2D-3D camera provides a magnification of the surgical field vision up to ×10 and broadcast images on a 4k 3D widescreen, with minimal encumbrance from the arm holder. Meier et al 11 performed 8 exoscope-assisted cleft palate repair procedures, exploiting these advantages with promising results.
The endoscope and exoscope share the potential to guarantee optimal visualization of the minute anatomical structures to be reconstructed, improve the ergonomics and comfort of the surgeon with greater involvement of the operating room staff, and the possibility record the procedure. Despite encouraging results, neither system has yet found adequate diffusion in the field of cleft palate surgery, and an in-depth comparison of these technological systems is lacking.
The aim of the current study is to provide an objective and subjective comparison of video assistance to cleft palate repair procedures through exoscope and endoscope-based procedures, by evaluating the use of the 2 devices in a controlled preclinical setting.
Materials and Methods
A fixed-formalin adult human head was dissected in the Anatomical Training Center of the University of Brescia. The specimen was donated by the voluntary body donation program of the Center for Anatomy and Cell Biology of the Medical University of Vienna. The donor provided written informed consent prior to death for the body use in medical education and research. The arterial system was injected via the common carotid and vertebral arteries with silicone rubber (Xiameter, Midland, MI, USA) stained with red Pintasol (Mixol Red E-L3mix, Kirchheim unter Teck, Germany). The head was placed on a special holder in modest hyperextension (30°) and mouth opening was ensured by a Dingman mouth opener. The soft palate was dissected by a senior cleft surgeon (K.T.) to mimic the anatomical conditions of a cleft. This procedure consisted in the median incision of the soft palate from the posterior nasal spine to the uvula, dissection of the nasal mucosal, muscular plane (levator veli palatini muscle), and oral mucosa. Finally, the nasal mucosal plane was sutured in order to facilitate the execution of the tasks.
Ten beginner surgeons (Head and Neck Specialty Registrars at the 1st year of their 4-year training course, none of them has ever performed a cleft palate repair independently) with limited experience in transoral surgery were asked to perform 4 tasks of surgical cleft repair simulation, as follows (Figure 1A to D, Supplemental Video 1):
Device setting including mobilization and focus adjustment. Detection and isolation of the muscle plane bilaterally. Suture of the muscular plane with a single 5/0 stitch. Suture of the oral mucosa with a single 5/0 stitch.
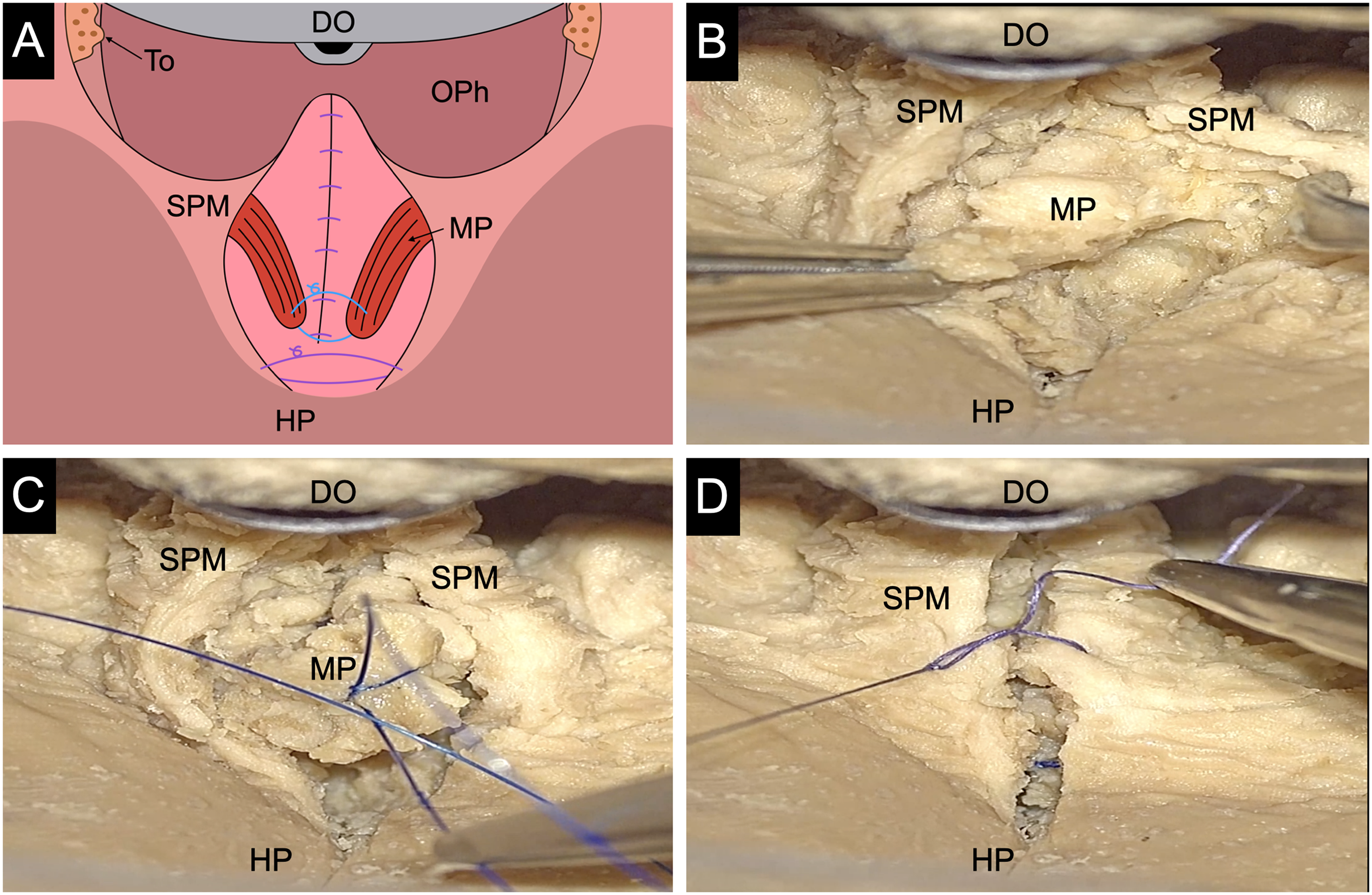
Tasks. A: Schematization of the oropharyngeal view after cleft palate simulation. B: Isolation of the muscle plane (MP) from the soft palate mucosa (SPM) (Task 2). C: Suture of the MP (Task 3). D: Suture of the SPM (Task 4).
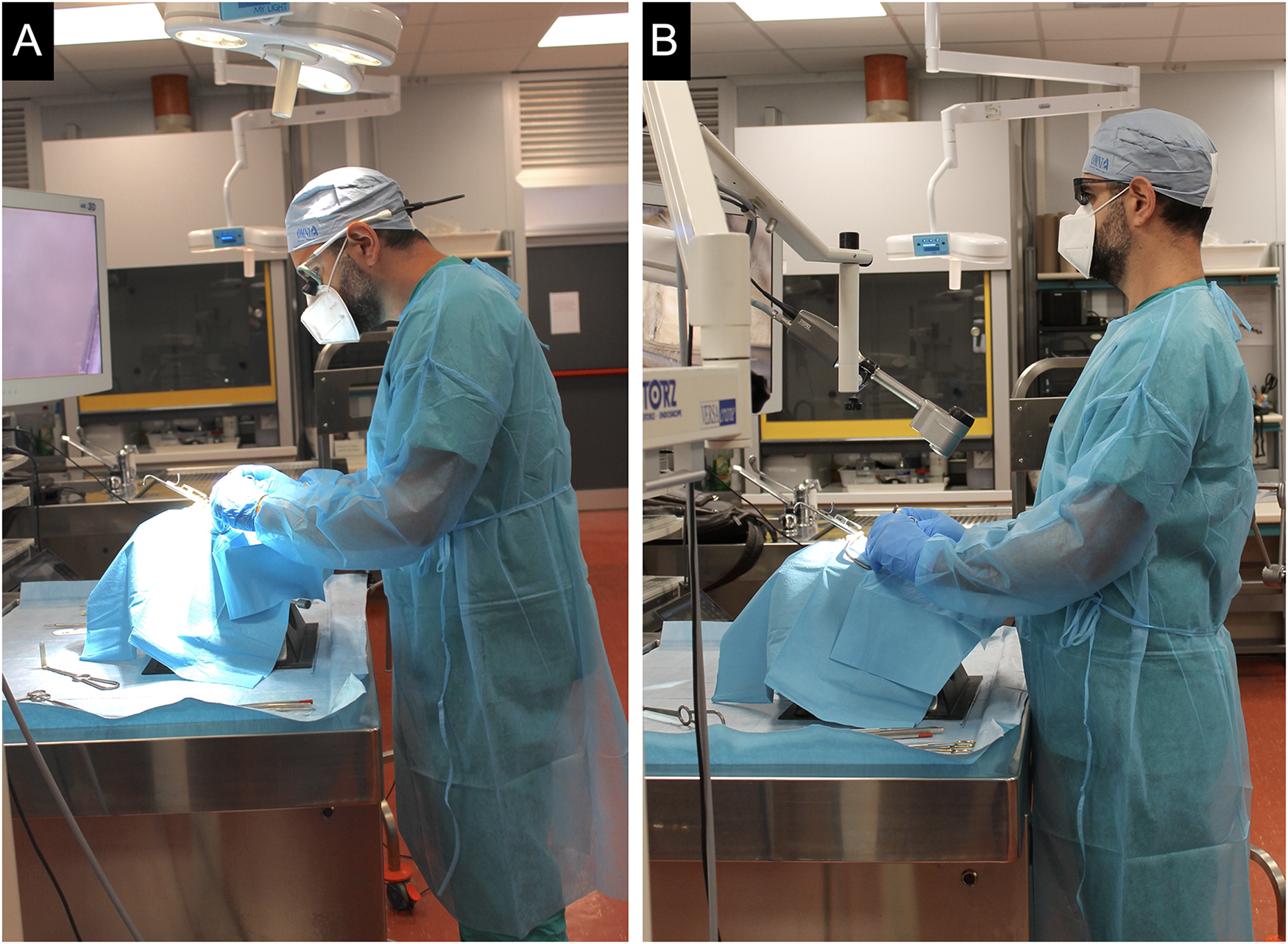
These procedures were performed under visual assistance with an endoscope (Olympus Visera© 4k, 0° 4-mm caliber optic, 2D images, magnification up to ×3, equipped with an articulated arm holder system and a 4k 55′′ widescreen), and an exoscope (Karl-Storz Vitom© 3D 4k, 2D and 3D images, magnification up to ×10, equipped with an articulated arm holder system and a 4k 55′′ widescreen) (Figure 2 A to D).

Settings. A: Exoscope setting. B: Endoscope setting. C: Extraoral positioning of the exoscope camera. D: Intraoral positioning of the tip of the endoscope.
The visual assistance system used was randomly assigned. Once the first set of procedures had been performed, after a 48-h waiting period, participants were asked to repeat the procedure with the help of the competing visual system.
Successful completion of the exercises was evaluated by the senior cleft surgeon (K.T.) and operative times were recorded.
At the end of the exercises with both exoscope and endoscope assistance, participants were asked to complete 2 questionnaires, namely the NASA Task Load System (TLS) questionnaire 12 and a VAS 1-10 questionnaire.
The NASA TLS questionnaire 12 is a validated multidimensional scale that provides a general workload score on a scale based on the weighted average of 6 subscales: mental demand, physical demand, temporal demand, performance, effort, and frustration.
The perception of these items during the exercises with the exoscope and endoscope was expressed on a scale from 1 to 5, where 1 is very low and 5 is very high. Supplemental Appendix 1 shows the NASA TLS questionnaire used in the current study.
With the VAS 1-10 questionnaire, participants were invited to express their judgment (on a scale from 1 to 10 in which 1 is the worst experience and 10 the best) on both the exoscope and endoscope, related to the instrument setting, handling, image quality, 3-dimensionality of the image, and encumbrance of the device.
Supplemental Appendix 2 shows the VAS 1-10 questionnaire used in the study.
Statistical analysis of operative times was carried out with a student t-test after performing normality tests assessment. Statistical significance was set at P<.05.
Results
All surgeons successfully completed the 4 tasks with both exoscope and endoscope.
Timing
The mean execution times under visual assistance with the exoscope and endoscope are reported in Table 1 (see also Supplemental Table 2 for detailed data). No significant difference was seen when comparing execution times with the 2 systems, except for device setting (1st Task) (P = .00002).
Mean Execution Time for the 4 Tasks Using Exoscope and Endoscope, Expressed in Seconds.

Nasa TLS
According to the participants, use of the exoscope was less intellectually, physically, and temporally demanding compared to use of the endoscope. The efforts required and perceived frustration were also lower during exoscopic video-assistance. Finally, the overall performance was perceived as less challenging and qualitatively superior using the exoscope. Figure 3 shows the averages of the NASA TLS scores scored by participants. Table 3 (Supplemental Material) shows the NASA TLS scores of each participant.
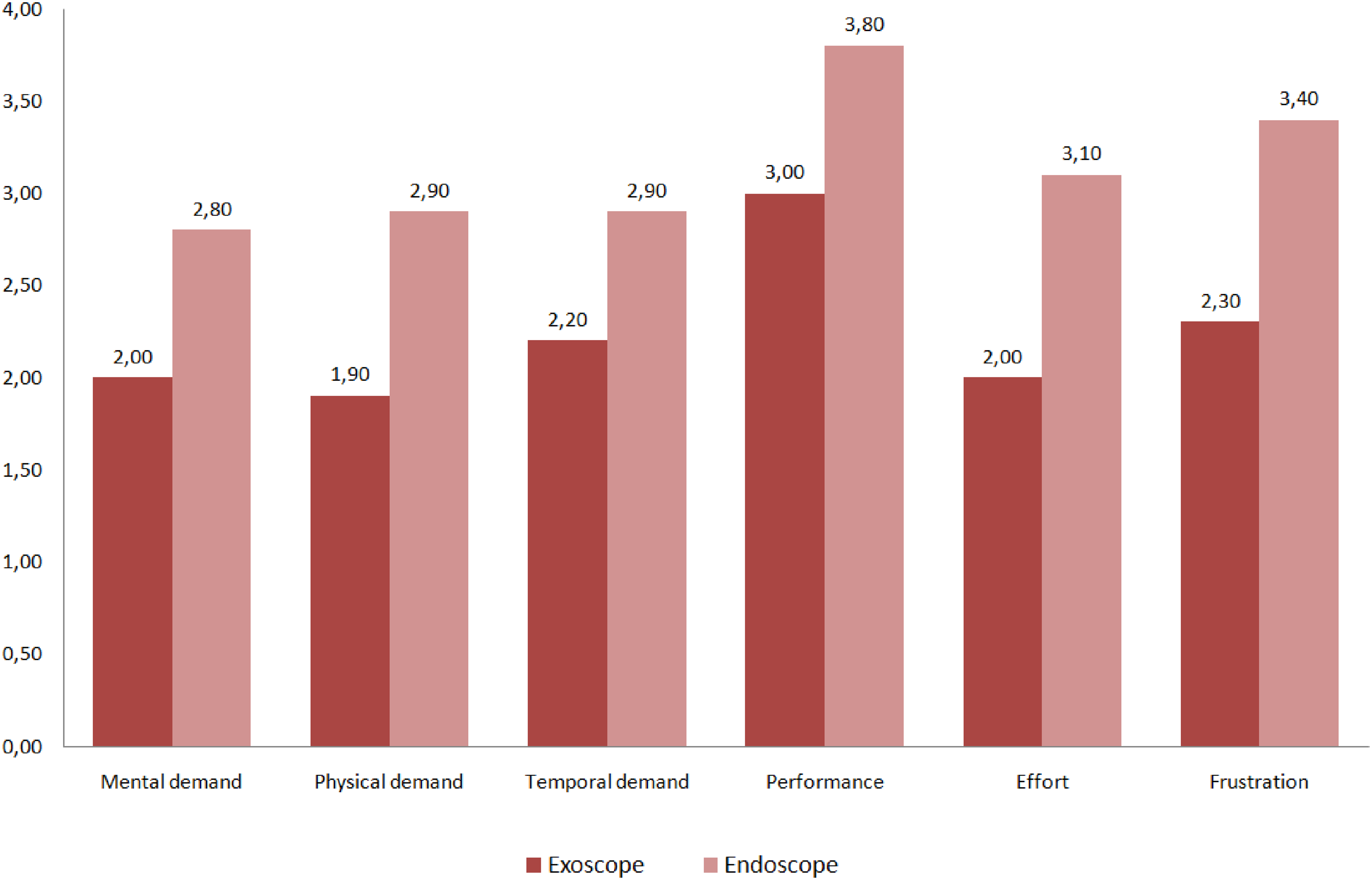
NASA TLS scores. Comparison of the NASA TLS mean scores provided by participants for exoscope and endoscope (1 = very low and 5 = very high).
VAS 1-10
According to the VAS 1-10 questionnaire, use of the exoscope was superior to that of the endoscope for setting (average score 8.70 vs 4.50), handling (8.50 vs 6.40), image quality (9.20 vs 6.80), 3-dimensionality (9.40 vs 5.00), and limited encumbrance (9.00 vs 4.00). Figure 4 shows the mean VAS 1-10 scores for both the exoscope and endoscope. Table 4 (Supplemental Material) shows these scores in detail.
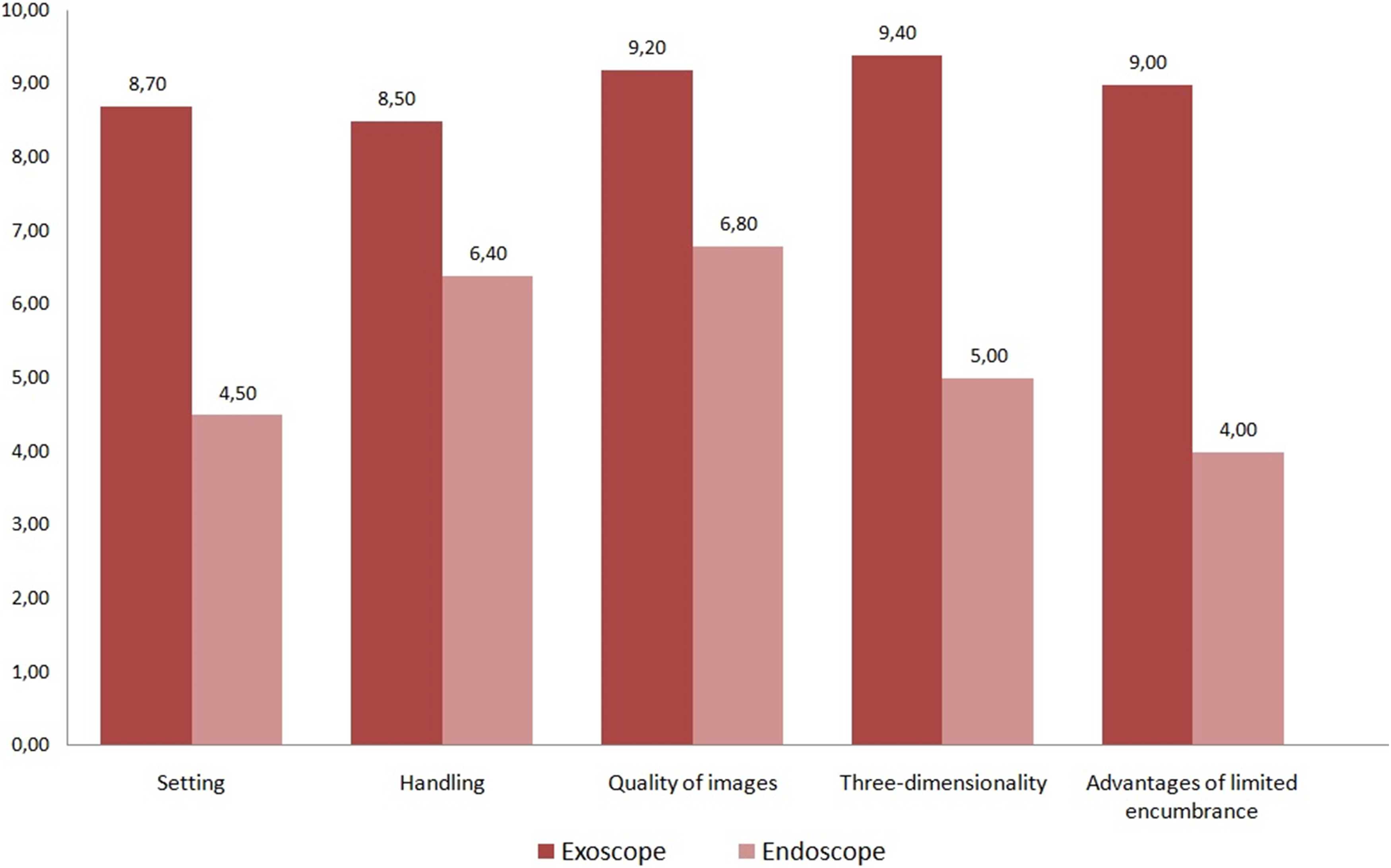
VAS scores. Comparison of the VAS 1-10 mean scores provided by participants for exoscope and endoscope (1 = worse experience, 10 = best experience).
Discussion
Use of the endoscope and exoscope in cleft palate surgery has been reported in a very limited number of studies. Levites et al described the experience of a single operator in 45 cases of endoscopic video-assisted palatoplasty, 7 while Meier et al reported a case series of 8 cleft palate repairs using exoscopic video-assistance. 11 Both studies reported in-vivo clinical experiences of the same cleft surgeon using a single video system, with no comparison between the 2 devices. The current study is comparing, subjectively and objectively, the use of the exoscope and endoscope for cleft palate repair, reporting the experience of a group of 10 beginner surgeons in a preclinical setting.
With the aim of maximizing the objectivity of the analysis, we intentionally selected a group of novice surgeons to reduce execution and judgement bias due to previous experience. The experience of senior cleft surgeons could have led to an unconscious comparison with the methods traditionally used in their practice, influencing the score assigned to these new technologies with some prejudices. Furthermore, while aware that a cadaver research setting is not completely adherent to the surgical reality, the preclinical environment allowed for comparison of constant conditions.
Despite the absence of transoral experience, all participants successfully completed the tasks with both the exoscope and endoscope, demonstrating the compatibility of these 2 systems with this kind of surgery.
The performance times for the tasks herein considered were similar for the 2 tools, except for Task 1, which was lower using the exoscope. The endoscopic manual holders used in the study did not allow easy fine adjustment movements. This was partially solved by the remote control available in the exoscope system. Furthermore, the 0° 4-mm-caliber optic, given the lower magnification power, had to be positioned near the oral cavity, in contact with the suspension system, making this setting more challenging. The disadvantage related to the proximity of the instrument to the oral cavity could probably be obviated by the adoption of higher magnification optic as for other surgical procedure (eg, laparoscopic surgery).
While the objective analysis did not show substantial differences, subjective judgment was clearly in favor of the exoscope. The NASA TLS and VAS 1-10 questionnaires gave feedback in line with the times observed, favoring the setting and handling of the exoscope compared to the less intuitive endoscope. In addition, the exoscope has the advantage of being extraoral while the endoscope, being adherent to the blade of the Dingman mouth opener, presented non-negligible intraoral encumbrance (Figure 2C and D). The benefits of the reduced steric impact of the exoscope were recognized in the VAS 1-10 questionnaire by all the participants. NASA TLS data showed intermediate levels of performance and frustration with both the technologies, likely linked to participants’ lack of confidence with cleft palate surgery.
Both the endoscope and exoscope allow for upright posture and reduced physical effort7, 11: these advantages were confirmed by the results of the NASA TLS questionnaire that showed an average physical effort of 1.90 for the exoscope and 2.90 for the endoscope (Figure 5).
Surgeon's posture. Surgeon's posture during a cleft palate procedure with surgical loupes (A) and with the exoscope (B).
The greater magnifying power of the exoscope compared to the endoscope (10× vs 3×) and the possibility of providing 3-dimensional images are characteristics that were intuitively appreciated by study participants, with a higher satisfaction score for the exoscope especially for the 3D images (VAS 9.40 vs 5.00). Both the exoscope and endoscope provided 4k images on 55′′ widescreens, ensuring ideal vision not only for operators but also for all participants. This feature allowed to show clearly and effectively the exercises to all participants and to evaluate its completion by the senior cleft surgeon. This advantage could be exploited especially for training and shadowing of cleft surgeons.13, 14 The possibility of creating surgical videos can also represent an added value for the surgical training all over the world, especially in developing countries where the access to these devices can be limited.
The exercise in a cadaver lab, combined with the use of video systems, was able to reproduce a plausible scenario on a single research model. However, some limits must be underlined:
- The use of an adult specimen in formalin with an iatrogenic cleft soft palate does not render all the difficulties of in-vivo surgery, characterized by small working volume, presence of blood hampering the vision of dissection planes, and consistency of delicate tissues. - The duration of the exercises is less than the overall duration of a palatoplasty. The subjective judgement, especially in terms of physical and mental demand and frustration, could change in case of longer surgical exercises in favor of 1 of the 2 technologies. Performing the entire palatoplasty on the same specimen several times would have severely compromised its anatomy and tissues. - The exoscope and endoscope were not compared to the systems traditionally used for cleft palate surgery such as surgical loupes and microscope. Surgical loupes were not possessed by all the surgeons enrolled in the current study and, as personal devices, cannot be shared. The microscope, on the other hand, has not been used since it is traditionally reserved only for dissection of the muscular plane,
6
with completion of the suture usually performed with surgical loupes. Therefore, the microscope would not have been suitable to analyze suturing of the muscular plane and oral mucosa (Tasks 3 and 4). In this light, with the endoscope and exoscope assisting the surgeon in all the cleft surgery phases of, time-consuming changes were avoided. Both systems are potentially capable to video-assist the entire procedure showing all areas needing dissection in cleft soft palate surgery. The remote control available for the exoscope allows to zoom and move within the operating field if necessary, without moving the device. - Although the 2 systems provided encouraging results in the current preclinical setting, they require an in-vivo clinical experience and prospective multicenter studies. The use of these technologies is more widespread in otolaryngology and neurosurgery and they are already available in many centers. The 2 devices can use the same video system and the same 4k monitor. The exoscope and the endoscope equipped with 0°optic lens and a 4k camera have similar costs. Any cleft centers that want to introduce these technologies in their practice could potentially share their costs with other units. Furthermore, to promote the diffusion of the exoscopic technology and to overcome the limits related to its costs, low-cost exoscopes have been proposed to expand access to videoassistance system.
15
An in-depth comparison of the 2 devices should also consider the effects of short- and long-term posture on cleft surgeons. Furthermore, it would be interesting to compare operating times, clinical outcomes, and costs of procedures with the help of an exoscope and endoscope, in order to evaluate which system produces more value.16, 17 Finally, 4k digital images provided by both systems could offer potential advantages in terms of analyzing large data set using artificial intelligence, a field still limitedly explored in Head and Neck surgery.
18
Conclusions
Exoscope and endoscope visual assistance have been shown to be valid for cleft palate surgery, with comparable performance times for each operative task. Overall, the exoscope was more appreciated by the participants involved in the study, especially regarding its easier setting, 3D vision, and limited encumbrance. Despite the promising preclinical data, further clinical comparisons are needed before widespread dissemination of these systems in cleft palate surgery.
Supplemental Material
sj-doc-1-cpc-10.1177_10556656221139340 - Supplemental material for Video-Assisted Cleft Palate Surgery: Preclinical Comparison Between Endoscope- and Exoscope-Based Approaches
Supplemental material, sj-doc-1-cpc-10.1177_10556656221139340 for Video-Assisted Cleft Palate Surgery: Preclinical Comparison Between Endoscope- and Exoscope-Based Approaches by Karim Tewfik, Vittorio Rampinelli, Dante Burlini, Barbara Buffoli, Rita Rezzani, Alberto Deganello, Giovanni Felisati and Cesare Piazza in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-doc-2-cpc-10.1177_10556656221139340 - Supplemental material for Video-Assisted Cleft Palate Surgery: Preclinical Comparison Between Endoscope- and Exoscope-Based Approaches
Supplemental material, sj-doc-2-cpc-10.1177_10556656221139340 for Video-Assisted Cleft Palate Surgery: Preclinical Comparison Between Endoscope- and Exoscope-Based Approaches by Karim Tewfik, Vittorio Rampinelli, Dante Burlini, Barbara Buffoli, Rita Rezzani, Alberto Deganello, Giovanni Felisati and Cesare Piazza in The Cleft Palate Craniofacial Journal
Supplemental Material
Footnotes
Acknowledgments
The authors sincerely thank who donated their bodies to science so that anatomical research could be performed. The donors and their family deserve our highest gratitude. The Authors thank the Center for Anatomy and Cell Biology of the Medical University of Vienna for the provision of the anatomical specimens.
Authors’ Note
The specimen was donated by the voluntary body donation program of the Center for Anatomy and Cell Biology of the Medical University of Vienna.
Author contributions
Karim Tewfik: conceptualization, methodology, writing—original draft preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
The work has been approved by the Ethical Committee of University of Brescia.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.