
Abstract
Objective
Compare the maxillary growth of patients with Unilateral Cleft treated with pre-surgical Functional Maxillary Orthopedic (FMO) and that of who underwent a surgical procedure with no previous use of appliances.
Design
Prospective study, the patients were divided into 2 groups. G1, was composed of 12 patients who received no pre-surgical intervention and cheilorhinoplasty at 6 months of age and G2, included 12 patients treated using Pre-Surgical Funtional Maxilary Orthopedic; they underwent no surgery during the study. Measurements were taken at three times: before the first month of life, at 6 months and between 9-12 months of age. Cleft distance (anterior, medium and posterior), maxillary width (anterior, medium and posterior) and minor and major segment width were analyzed.
Results
Alveolar Cleft decrease was 79.82% in G1 and 52% in G2. Posterior Cleft decrease was 24.1% in G1 and 41.77% in G2. Greater Segment Width increase was 24.53% for the patients in G1, and 37.47% for the patients in G2. As for Inter Canine Width, a decrease of 5.16% in G1 and an increase of 9.19% in G2 were found. Medium Arch Width only increased in a statistically significant manner in G2 9.02%.
Conclusions
Surgery allowed for the closure of the alveolar cleft. FMO made it possible to close the anterior and the posterior clefts through the growth of the maxillary segments, increased the transverse growth of the maxilla and could prevent maxillary collapse. Each team must individually evaluate whether to indicate or not the use of preoperative orthopedics.
Introduction
Treatment of patients with cleft lip and palate is complex and includes surgical and non-surgical multidisciplinary procedures. Primary surgery involves lip closure to restore oral competence and facial symmetry, and hard and soft palate surgery to develop speech and deglutition functions. Initial treatment may be applied using pre-surgical infant orthopedic, in order to reduce the severity of the initial pathology in the mouth and the nose while helping regulate functions such as deglutition and feeding. Alternatively, surgery may be applied with no previous orthodontic care.
The use of Pre Surgical Infant Orthopedic (PSIO) is controversial: some studies have shown that its association with surgical treatment fosters a better nasal symmetry and reduces cleft severity.1–3 Nevertheless, it has been reported that the use of PSIO is not always necessary for a proper alveolar growth, and previous studies suggest that the cleft size may be reduced without orthopedic devices.4,5
Many studies have published case series of patients who were treated either with or without pre-surgical orthopedics, but few of them compare case series of patients with and without such treatment.
The aim of the present study was to compare the maxillary growth of cleft patients who were treated with pre-surgical Functional Maxillary Orthopedic (FMO) and the maxillary growth of cleft patients who underwent a surgical procedure (cheiloplasty) with no previous use of appliances.
Methods
This is a prospective, longitudinal study undertaken as a collaborative project between two institutions: CAIF/AFISSUR - Centro de Atención Integral del Labio Leporino y la Asociación para la Rehabilitación y Promoción Social del Labio y Paladar Hendido – an outpatient clinic that belongs to the Healthcare Department in Paraná and Curitiba (PR Brazil)− and the Pediatric Maxillofacial Surgery Unit at the Vall d’Hebron University Hospital (HUVH) in Barcelona, Spain. The study was previously approved by the Institutional Review Board of both institutions. (CAIF CNS 466/2012 and HUVH PR(AG)449/2017).
Inclusion criteria were the following: patients with complete unilateral cleft lip and palate who suffered no associated syndromes.
Plaster casts were evaluated for 24 patients, who were divided into 2 groups:
Group 1 (G1): This was the patient sample from Brazil and included patients who were treated without FMO. Impressions were taken in alginate and cast in hard dental stone. Impressions were scanned with the 3shape Dental System software using a high-sensitivity 3D-scan device (Ceramill Map 400+) and were exported as a stereolithographic file (STL) on which computer-based measurements would be taken.
Impressions were taken at three different stages: (T1) at 1 month of age; (T2) 6 months before the cheiloplasty was performed, by the same surgeon, using the Fisher technique for the lip and the Skoog technique for the nose; and (T3) at 12 months of age, before palatoplasty (Table 1).
Group Division According to the Period of Analysis.

Group 2 (G2): This was the patient sample from Barcelona and included patients treated with pre-surgical FMO and nasal molding. Impressions were taken with alginate and cast in hard dental stone type III, scanned using the Dentaurum Orthoscan scanner and software and were exported as a STL on which computer-based measurements would be taken.
Impressions were taken at three different stages: (T1) in the first week of the patient's life, (T2) at 6 months of age and (T3) between 9 and 11 months of age, before combined cheilorhinoplasty and palatoplasty surgery. Models evaluated for Group 2 received no previous surgical treatment and no lip taping treatment, and only the use of pre-surgical FMO was evaluated (Table 1).
In patients treated with pre-surgical Functional Maxillary Orthopedic, a model modification technique was used, according to Mc Niel's 6 and Grayson's 7 modified technique. First of all, the plaster model is waxed so that the cleft space is filled in and space is provided for the bone to grow. The wax coating should provide continuity to the palatal vault, and its height in the alveolar part should be equal to that of the maxillary segments. Cross-sectionally, a round arch should be built by adding wax to the vestibular and anterior area of the lesser segment, in order to allow for growth in these directions.
Afterwards, Dr. Pannaci's modification is applied8,9 by scratching the plaster in the model with a putty knife in those zones where higher mechanically-induced stimulation is expected; particularly, the medial palatal area of the greater segment and the palatal area of the lesser segment (Figure 1). On this model, an acrylic plate is made using a self-curing acrylic resin. The procedure, including impression procedures, the model modification technique and the creation of a new plate was performed every month. Once the alveolar cleft had been reduced to less than 5 mm, a nasal stent was added following Grayson's technique, 7 and once the stent was placed the plate was attached using oral adhesives such as Corega® in order to maintain the plate firmly positioned in the mouth and to properly position the stent.

A model without wax (left) and the same model (right) on the following month; the model has been wax-coated and the zone where the plaster model will be scratched has been sketched in pencil.
Models were measured using the Autodesk Inventor Professional 2021 software, using measures described by Mazaheri 10 and Botticelli et al. 11
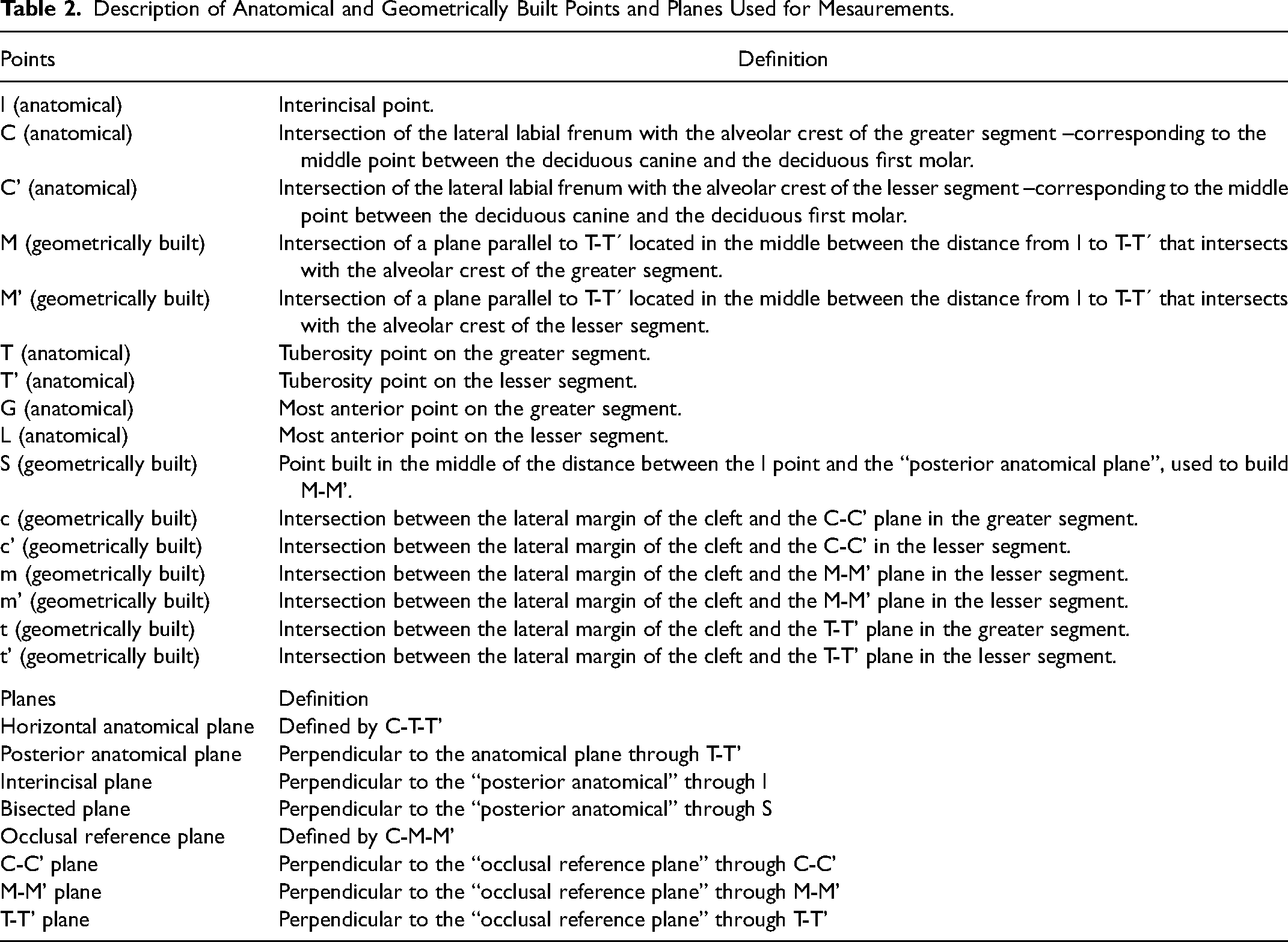
Seven anatomical reference points were defined: interincisal point (I), most anterior point on the greater segment (G), most anterior point of the lesser segment (L), canine groove on the major segment (C), canine groove on the lesser segment (C’), tuberosity point on the greater segment (T), and tuberosity point on the lesser segment (T’). Using the anatomical points as a reference, geometric points were established as shown in Table 2.
Description of Anatomical and Geometrically Built Points and Planes Used for Mesaurements.
The following anthropometric measurements were obtained (Figure 2):
Alveolar Cleft Distance (AC) between G-L. Medium Cleft Distance (MC), between m-m’. Posterior Cleft Distance (PC) between t-t’. Greater Segment Width (GSW) M-m. Lesser Segment Width (LSW) M’-m’. Intercanine Width (ICW) between C-C’. Posterior arch width (PAW) between T-T’. Medium Arch Width (MAW) between M-M´.
Results
We analyzed the measurements obtained (both in mm ± SD and in %) in order to assess whether an increase or a reduction had taken place (Tables 3 and 4).
Alveolar Cleft Distance (AC)
A reduction of the alveolar cleft distance (G-L) was observed over time; the amount of the reduction differed between the groups. Initial measurements for the G2 group were higher than those for the G1 group.
For the patients in G1, a statistically significant reduction was found in all stages: a 17.82% reduction (1.74 mm) was observed between T1 and T2, and a higher reduction (75.52%, 6.07 mm) could be observed between T2 and T3. The total reduction between T1 and T3 amounted to 79.82% (7.81 mm).
For the patients in G2, the reduction observed between T1 and T2 was statistically significant (35%). However, the reduction observed between T2 and T3 was not significant (26.26%). In this group, the reduction observed between T1 and T3 amounted to 52.07%, which was statistically significant.
Medium Cleft Distance (MC)
Despite the reduction of Medium Cleft Distance (MC) value in both groups, no time-related statistically significant difference was observed at any age.
Posterior Cleft Distance (PC)
Statistically significant differences were observed for Posterior Cleft Distance (PC) measurements in both groups. For the patients in G1, the reduction between T1 and T2 was 20.97%, and the total reduction T1-T3 was 24.70%. For the patients in G2, a statistically significant reduction was detected between T1 and T2 (32.15%) and between T1 and T3 (41.77%). The percentage reduction was bigger for the patients in G2 (41.77%) than for those in G1 (24.70%).
Greater Segment Width (GSW) and Lesser Segment Width (LSW)
For the patients in G1, statistical significance could only be observed when comparing T1 to T3 (24.53%) in terms of the growth of the Greater Segment Width (GSW). As opposed to that, for patients in G2, statistical significance was observed between T1 and T2 (23.04%) and between T1 and T3 (37.47%). In particular, the increase observed for the patients in G2 was bigger than that observed for the patients in G1 (37.47% and 24.53%, respectively).
When comparing lesser segment measurements no significant differences were found between any of the stages either in G1 or in G2. Nevertheless, growth could be observed in both groups in a similar manner.
Intercanine Width (ICW)
Intercanine Width (ICW) increase was statistically significant for the patients in G2 only. In this case, ICW increased between T1 and T2 (8.93%) and between T1 and T3 (9.19%). For the patients in G1, ICW gradually diminished over time (−1,62%), but no statistically significant values were obtained.
Posterior Arch Width (PAW)
In terms of Posterior Arch Width (PAW), the differences observed were not statistically significant at any stage, either for the patients in G1 or for those in G2.
Medium Arch Width (MAW)
In terms of Medium Arch Width (MAW), no statistically significant differences were found for the patients in G1. Even so, a slight reduction was observed between T2 and T3, and a slight increase was detected between T1 and T3. For the patients in G2, an increase was detected at the three stages; the differences were statistically significant between T1 and T2 (8.9%, 3.43 mm) and between T1 and T3 (9.92%, 3.48 mm).
Discussion
It should be noted that, by taking buccal records (pictures, models, scans, measurements), better diagnosis and treatment planning processes may be achieved. Besides, by taking such records we may perform a longitudinal evaluation of the treatments applied, and decide on the use of a treatment. 12
Anthropometric measurements of the models make it possible to study the development and growth of the palate in cleft patients, and they are the best choice when it comes to undertaking a quantitative evaluation of children with cleft palate. 13
There is no standard procedure for the treatment of cleft lip and palate. Every institution uses its own protocols, makes its own approaches and operates on patients at different ages. 14 This is due to the low level of evidence provided by the available studies, given that patient samples for this pathology are highly heterogeneous, that it is difficult to coordinate data obtained from multicentric studies and that longitudinal studies are scarce, which hinders the long-term follow-up of results. In spite of that, enough evidence is available to guide surgeons in treatment and point out the effect of cheiloplasty-induced molding on alveolar segments as a consequence of the pressure applied by the reconstructed lip, and suggest that cheiloplasty alone could promote the same effects as those of pre-surgical molding.5,14,15 However, this unguided alveolar molding could cause the minor segment to collapse into the major segment, restricting transverse growth. 13
In this context, Pre-surgical infant orthopedics (PSIO) stands out as an initial treatment before surgery, but it remains a controversial topic due to the lack of appropriate studies, and different results, which reduces the level of evidence available for this therapy.16–18 Many reports have demonstrated the immediate effects of PSIO on cleft patients, before cheiloplasty helps to narrow the alveolar clefts and, accordingly, facilitates the task of surgeons in performing primary cleft lip closure.3,19–22
The comparison between measurements obtained when using several treatments (or lack thereof) and the measurements obtained for spontaneous growth will provide a very useful reference to guide the clinician when having to choose between different kinds of treatment for each patient in particular.
In this context, the aim of the study was to evaluate two different treatments (in 2 different centers), the anthropometric changes observed in the maxillary growth over three stages when using pre-surgical orthopedics – represented by FMO– and when using cheiloplasty after 6 months with no previous treatment.
In our study, we observed a statistically significant reduction of alveolar cleft width in G1 (surgery only). A 1,74 mm (17,83%) of reduction was found before cheiloplasty, this is associed to a natural growth, suggesting that the palatal plates may have narrowed spontaneously. 4 A 7.81 mm (79.82%) reduction was found after cheiloplasty. Our data corroborate the study by Huang et al. 23 and Pontes et al. 4
Despite the fact that, when treatment started, patients in G2 (FMO) showed wider clefts with a smaller circumference –according to Peltomäki et al., 24 in patients with wider clefts, smaller arch circumferences, shorter arch lengths, or both, growth was hindered – in the group that was treated with FMO an appropriate cleft closure was achieved before surgery (closure amounted to 52.07%, 5.92 mm between T1 and T3). The reduction between T1 and T2 was 4 mm (35%) almost three times greater than the natural growth of the patient observed at this same time in G1.
Very few studies evaluate the reduction of the cleft in the posterior part of the arch, despite the fact that it is closely related to velopharyngeal function and fistula incidence.25,26 In this study, we can observe a statistically significant decrease of Posterior Cleft (PG) in G1 (3.16 mm, 24.70%). As for G2 (those patients who had been treated with FMO) showed a reduction of 6.15 mm, a statistically significant reduction of 41.77%, which is almost twice as much as that observed in G1.
As for the Medium Arch Width (MAW), the only statistically significant growth measures observed were found in G2 (FMO), where a 3.48-mm increase (9.92%) was found. Whereas growth was observed in the posterior arch width for both groups, none of them showed statistically significant differences.
In terms of Intercanine Width (ICW), a statistically significant increase was found in G2 (FMO), where a 2.80-mm increase (9.19%) was observed between T1 and T3. As opposed to that, a 1.63-mm (5.16%) reduction was found in G1, but results were not statistically significant. 13
With the three measurements evaluated –intercanine width, maxillary width in the medium region and maxillary width in the posterior region – it may be observed that this kind or orthopedic treatment is not restrictive from the point of view of growth, as a reduction in the cleft was observed both in the anterior and the posterior region, accompanied by growth of the maxillary segments and growth in arch widths. The fact that segments are larger and maxillary widths are wider, along with a lower cleft width, could be indicative of a better growth and of less maxillary collapse after surgical closure. This is in agreement with the study by Shetty et al. in 2017, 1 which showed that the reduction of the intersegmental distance caused by the use of FMO improves symmetry and stability, which could prevent collapse in the long-term.
In agreement with what was published by Grayson et al. 3 and Okhiria et al. 27 regarding the fact that greater Palatal Cleft Width predicts an increased risk for unfavorable outcomes in cleft palate repair, the reduction of the severity of the initial deformity −in particular in the most severe cases − could lead to better surgical outcomes.
In this study, we only measured some points in the patient's maxillary, but therapy with pre-surgical FMO encompasses many other aspects apart from the anatomical aspects involved in the maxillary. For this reason, in order to be able to perform a complete evaluation of when to use this therapy and which patients would benefit most from it, it would be necessary to assess other aspects. Such aspects would include the following: feeding, normalization of tongue positioning and swallowing function, burden of care for patients and the team, reduction of the need for an alveolar graft, presence or absence of fistulae, Nasal Molding and cost reduction for the whole treatment.20,28–30
Conclusions
Surgical treatment for lip and nasal closure allows for the anterior alveolar closure of the maxillary cleft, with a slight collapse of intercanine width.
Treatment with pre-surgical FMO allows for the anterior and posterior closure of the cleft palate through the growth of the maxillary segments; transverse distance and maxillary growth are increased, which could prevent maxillary collapse in the long-term.
However, more comparative studies, with larger samples, are required.
Every multidisciplinary team should evaluate every patient in order to decide whether to perform FMO treatment, taking several aspects into account. These would include patient characteristics, anatomical features, cleft width, place of residence, and the team's limitations to apply treatment.
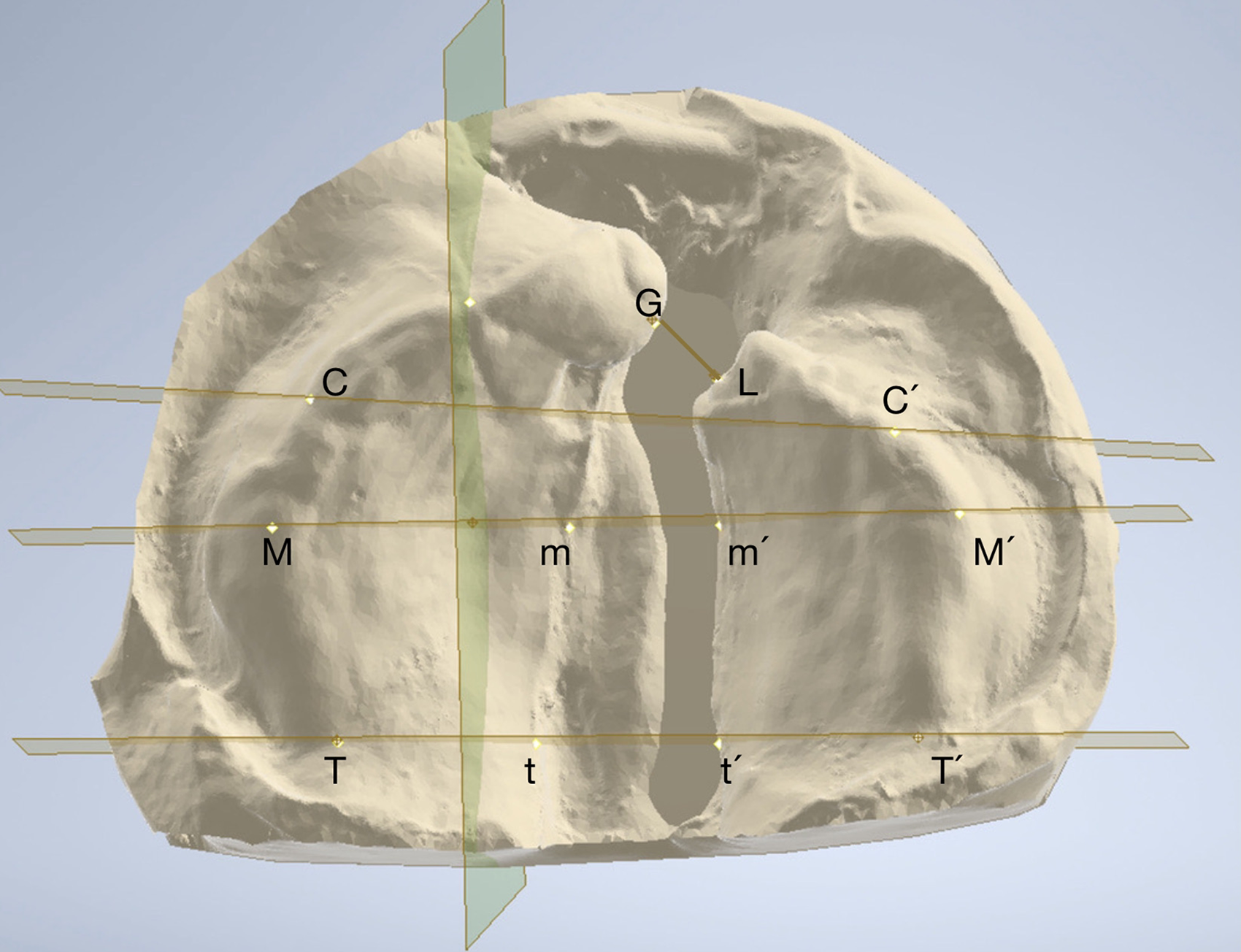
Points and measurements. A depiction of the points from which planes are drawn and measurements are made.
Measurements and Standard Deviation on the anThropometric Measurements for G1 and G2.
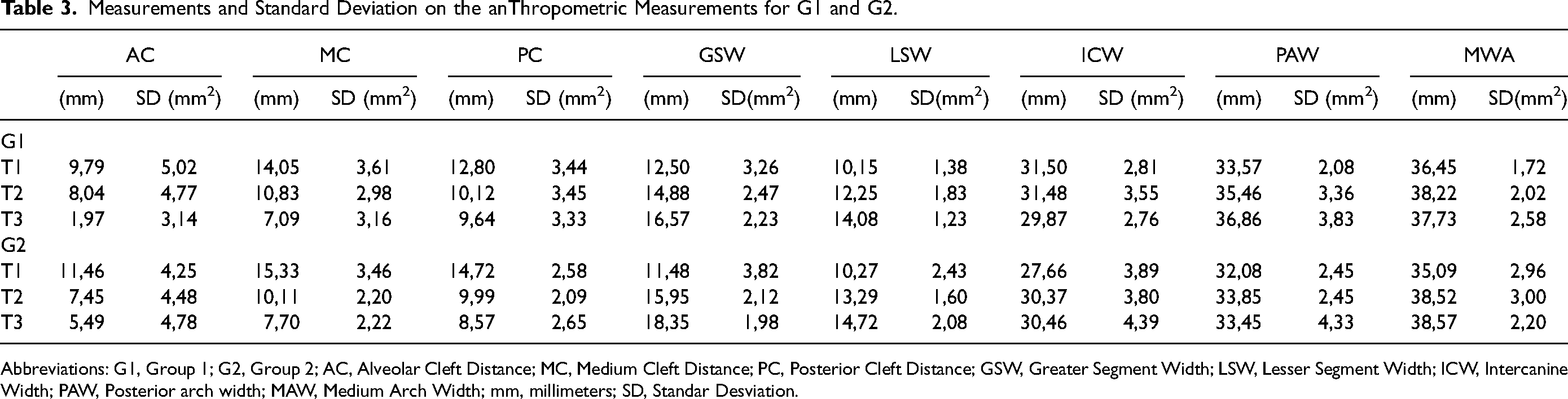
Abbreviations: G1, Group 1; G2, Group 2; AC, Alveolar Cleft Distance; MC, Medium Cleft Distance; PC, Posterior Cleft Distance; GSW, Greater Segment Width; LSW, Lesser Segment Width; ICW, Intercanine Width; PAW, Posterior arch width; MAW, Medium Arch Width; mm, millimeters; SD, Standar Desviation.
Variations of Measurements in Percentage and mm.
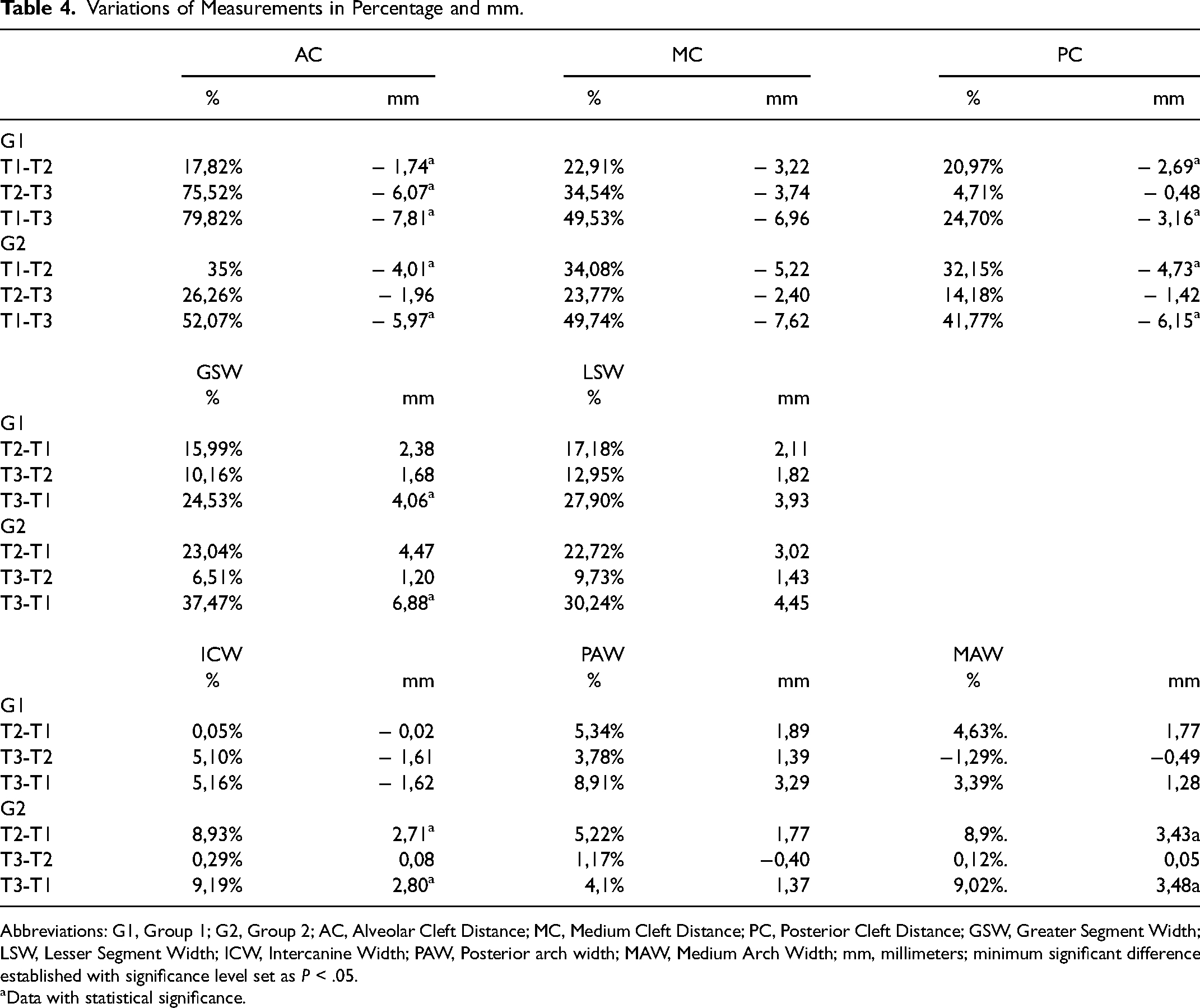
Abbreviations: G1, Group 1; G2, Group 2; AC, Alveolar Cleft Distance; MC, Medium Cleft Distance; PC, Posterior Cleft Distance; GSW, Greater Segment Width; LSW, Lesser Segment Width; ICW, Intercanine Width; PAW, Posterior arch width; MAW, Medium Arch Width; mm, millimeters; minimum significant difference established with significance level set as P < .05.
Data with statistical significance.
Footnotes
Anonymized Text
The study was previously approved by the Institutional Review Board of both institutions. (CAIF CNS 466/2012 and HUVH PR(AG)449/2017).
Others Contributors
Gabriella Callegaris, MD; Felipe Boni Pontes, MD; Montserrat Munill Ferrer MD; Terisita Pannacci Padrón, DDS; Coro Bescós Atín, MD, PhD, EBOMFS; Rosa Pujol Pina Scientific Translations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.