
Abstract
Objective
Currently there is variation in perioperative care of orthognathic surgery patients and limited clinical practice guidelines. The current orthognathic surgery practice patterns among US academic OMFS training centers have not been described. The purpose of this study is to describe the practice patterns among US academic OMFS training centers.
Design
The study design is cross-sectional. Data was collected through a survey of the sample.
Setting
OMFS programs in the US.
Participants
Academic OMFS. 573 surgeons were contacted and 85 responses were received.
Main Outcome Measure
Descriptive and bivariate statistics were reported.
Results
Respondents were 87% male and worked in full-time academic (80%), part-time academic (19%), or military settings (1%). Thirty-one percent have practiced for 30 years or more and then 29% with 11–20 years, 18% with 21–30 years, 12% with 6–10 years and 11% with 1–5 years. Twenty-six percent of respondents perform 20–40 orthognathic surgeries a year, 22% perform less than 20 surgeries a year, 21% perform 40–60 surgeries per year, and 19% perform more than 100 surgeries per year. Intraoperatively, 48% of surgeons request a mean arterial pressure of 60–64 mmHg, 25% utilize tranexamic acid (TXA), 85% report a blood loss of less than 400 milliliters, and 93% report a blood transfusion rate of <1%.
Conclusion
There are variations in orthognathic surgery practice patterns with limited clinical practice guidelines. Only 13 of the 32 survey questions had a single response holding a simple majority. This study demonstrates the need for further research and evidence-based protocols and decision making.
Introduction
Orthognathic surgery is widely used to correct dentofacial deformities, relieve upper airway obstructions, and improve facial aesthetics. Orthognathic surgery and perioperative management continue to undergo innovation in the domains of virtual surgical planning, custom (patient specific) cutting guides and plates which are also referred to as patient specific implants (PSIs), intraoperative anesthesia management, and perioperative care. With these recent innovations and variations in surgical education, the current standard of practice of orthognathic surgery in academic oral and maxillofacial surgery (OMFS) centers has not been described and clinical practice guidelines are limited in detail. 1 Academic OMFS centers are of interest as they represent the state of education for the next generation of orthognathic surgeons.
The purpose of this study is to describe the current practice patterns for orthognathic surgery among US academic OMF surgeons. The hypothesis is that there is large variability in orthognathic surgery practice patterns at US academic training centers. The specific aims are 1) to describe the current practice patterns of US academic OMFS 2) to describe differences in practice patterns between different surgical volume surgeons and between surgeons with different times spent in practice.
Materials and Methods
The investigators designed and implemented a cross-sectional survey to describe current practice patterns for orthognathic surgery among academic OMFS. The survey was sent to US academic OMFS via email and collected anonymously through Qualtrics (Provo, UT). The survey was limited to full-time and part-time US academic OMFS. The survey included demographic, practice variables, intraoperative variables, and postoperative variables.
Demographic variables included gender, age, practice setting (ie, full or part-time academic surgery), geographic location, American Board of Oral and Maxillofacial Surgeons Diplomate status, and number of years in practice.
Practice variables included the number of orthognathic surgeries operated per year, location of surgery (outpatient or office based surgery center versus hospital), the utilization of Advanced Practice Providers, percentage of orthognathic surgeries that are bimaxillary osteotomies, and percentage of Le Fort I osteotomies that are segmental.
Intraoperative practice variables included average surgical time, number of surgical assistants, method of intraoperative blood pressure monitoring (traditional non-invasive blood pressure cuff, invasive arterial continuous monitoring, or non-invasive continuous arterial monitoring), requested intraoperative mean arterial pressure, use of tranexamic acid (TXA), estimated intraoperative blood loss, percentage of patients who receive a blood transfusion, choice of perioperative antibiotics, and use of foley catheter.
Surgical variables included method of transfer of the virtual plan to the patient during surgery (ie occlusal wafers versus PSIs), maxilla first versus mandible first surgical sequencing, management of third molars, preference of fixation for sagittal ramus osteotomies, preference of method of intraoperative vertical dimension measurement, use of alar cinch, use of and maintenance of final occlusal splints (wafers)
Postoperative variables include length of hospital stay (LOS) after surgery, use of an enhanced recovery after surgery (ERAS) protocol, choice and duration of postoperative antibiotics use, steroid use patterns, level of care for postoperative admission and use of postoperative facial dressing. Descriptive and bivariate statistics were reported. The University of Alabama at Birmingham Institutional Review Board granted exemption status (IRB-300007531).
Results
Surveys were sent to 573 surgeons listed as faculty of the 51 accredited US Oral and Maxillofacial Surgery programs and faculty of OMFS programs. Responses to 85 surveys were received.
Demographic Data
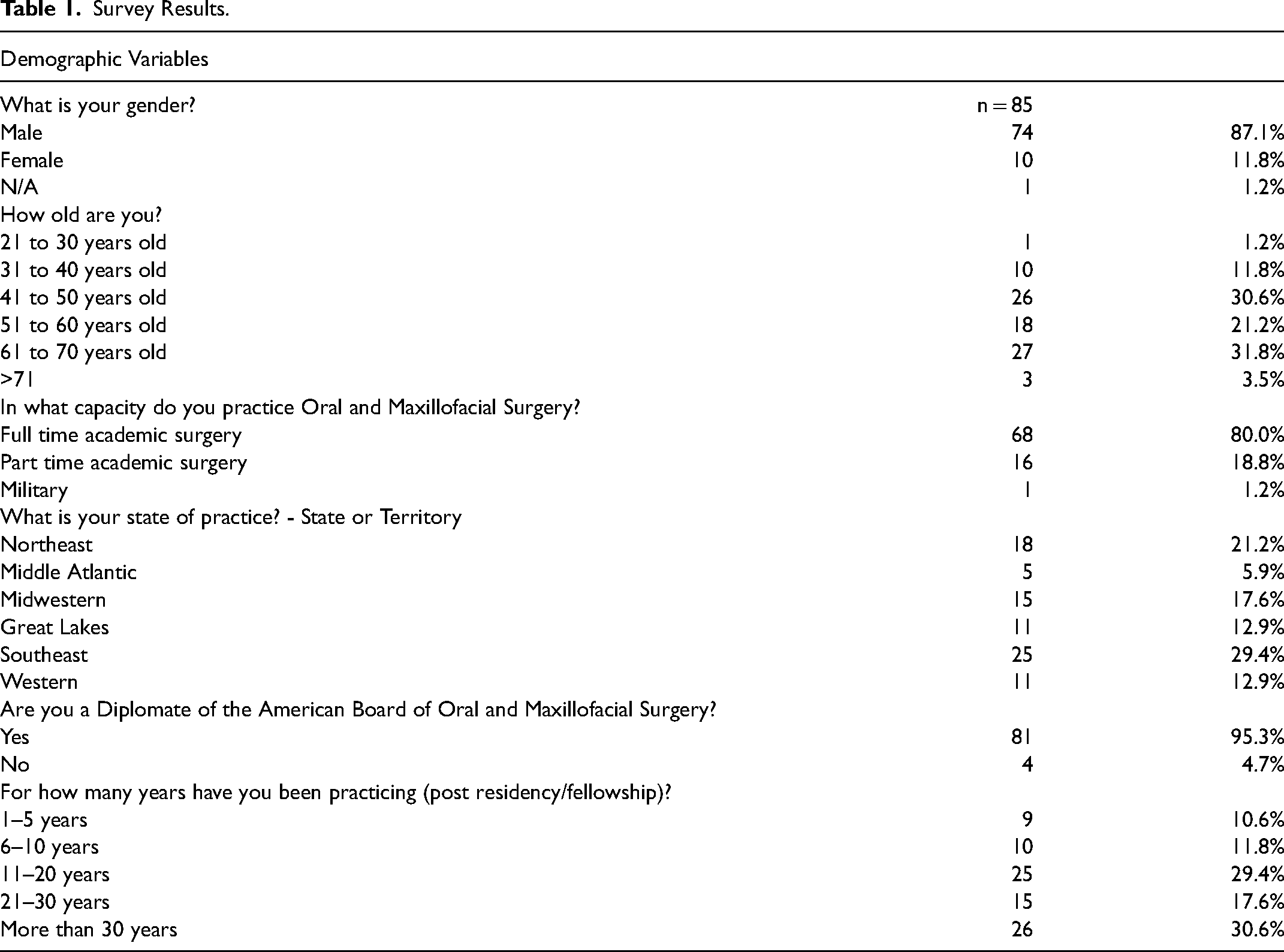
Eighty-seven percent of the respondents were male (Table 1). For age, the largest demographic was 61 to 70 years of age (32%) followed by 41–50 years of age (31%). Eighty percent practice full time academic surgery, 19% part time academic surgery and 1% military. Geographic responses were reported by AAOMS regions; 29% of respondents from the Southeast, 21% from the Northeast, 18% from the Midwestern, 13% from the Great Lakes, 13% from the Western region, and 6% from the Middle Atlantic. Ninety-five percent of respondents were certified by the American Board of OMFS. Thirty-one percent have more than 30 years of practice experience, 29% with 11–20 years, 18% with 21–30 years, 12% with 6–10 years and 11% with 1–5 years.
Survey Results.
(Continued)
Practice Variables
Twenty-six percent of respondents reported to operate 20–40 orthognathic surgeries a year, 22% operate less than 20 surgeries a year, 21% operate 40–60 surgeries per year, and 19% operate more than 100 surgeries per year. Fourteen percent of surgeons perform some or all of their bimaxillary osteotomies at office-based surgery centers or ambulatory surgery centers. Only 18% of surgeons utilize Advanced Practice Providers. Sixty-two percent of surgeons reported over 60% of their surgeries are bimaxillary osteotomies. Eighty-three percent reported less than 60% of their Le Fort I osteotomies are segmental.
Intraoperative Variables
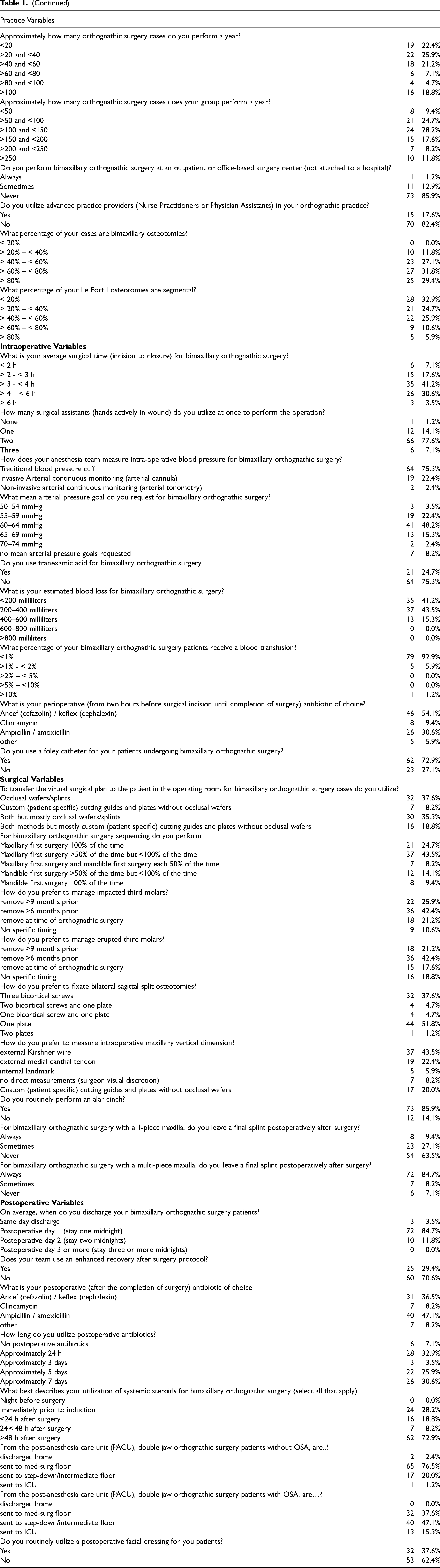
In regards to bimaxillary orthognathic surgery operative times, 41% reported 3-4 h, 31% 4–6 h, 18% 2-3 h, 7% less than 2 h, and 4% greater than 6 h. Seventy-eight percent utilize two surgical assistants.
Seventy-five percent use a traditional non-invasive blood pressure cuff for intraoperative blood pressure monitoring, 22% utilize invasive arterial continuous monitoring, and 2% utilize non-invasive continuous monitoring. Intraoperatively, 48% of surgeons request a mean arterial pressure of 60–64 mmHg, 25% utilize TXA, 85% report a blood loss of less than 400 milliliters, and 93% report a blood transfusion rate of less than 1%.
Perioperative choice of antibiotic was cefazolin (54%), ampicillin (31%), clindamycin (9%), and other (6%). An indwelling foley catheter is used intraoperatively for 73% of respondents.
Surgical Variables
To transfer the virtual surgical plan to the patient during the operation, 38% use only occlusal wafers/splints, 8% use PSIs, 35% use both methods but mostly occlusal wafers/splints, and 19% use both methods but mostly PSIs. Twenty-five percent exclusively perform maxillary first surgery and 44% perform maxillary first surgery in the majority of surgeries. Only 9% of respondents reported to exclusively perform mandibular first sequencing for bimaxillary orthognathic surgery.
For management of erupted and impacted third molars, the majority of surgeons preferred to remove third molars prior >6–9 months prior to surgery. Fifty-eight percent of surgeons fixate their bilateral sagittal ramus osteotomies with one monocortical plate and 38% with three bicortical screws. To establish the intraoperative vertical dimension, 66% use an external landmark reference point, 20% use custom (patient specific) cutting guides and plates, 6% use an internal landmark reference point, and 8% do not use direct patient measurements to establish the vertical dimension. Eighty-six percent routinely perform an alar base cinch. Sixty-three percent never leave a final splint secured to the dentition after a one piece Le Fort I osteotomy while 85% always leave a final splint secured to the dentition after a multi-piece Le Fort I osteotomy.
Postoperative Variables
The majority of respondents (85%) discharge their bimaxillary osteotomy patients on post-operative day 1. The minority of respondents (29%) report utilizing an ERAS protocol for bimaxillary surgery. For postoperative antibiotic choice, 47% use amoxicillin, 37% cefalexin, 8% clindamycin, 8% other. Thirty-three percent utilize postoperative antibiotics for approximately 24 h after surgery, 31% for 7 days after surgery, and 26% for 5 days after surgery. The majority of respondents (73%) use steroids greater than 48 h after surgery.
After discharge from the post-anesthesia care unit (PACU), patients without obstructive sleep apnea are most often admitted to a med-surg floor and patients with obstructive sleep apnea are most often admitted to a step-down or intermediate level of care floor. The majority of respondents do not utilize a postoperative facial dressing.
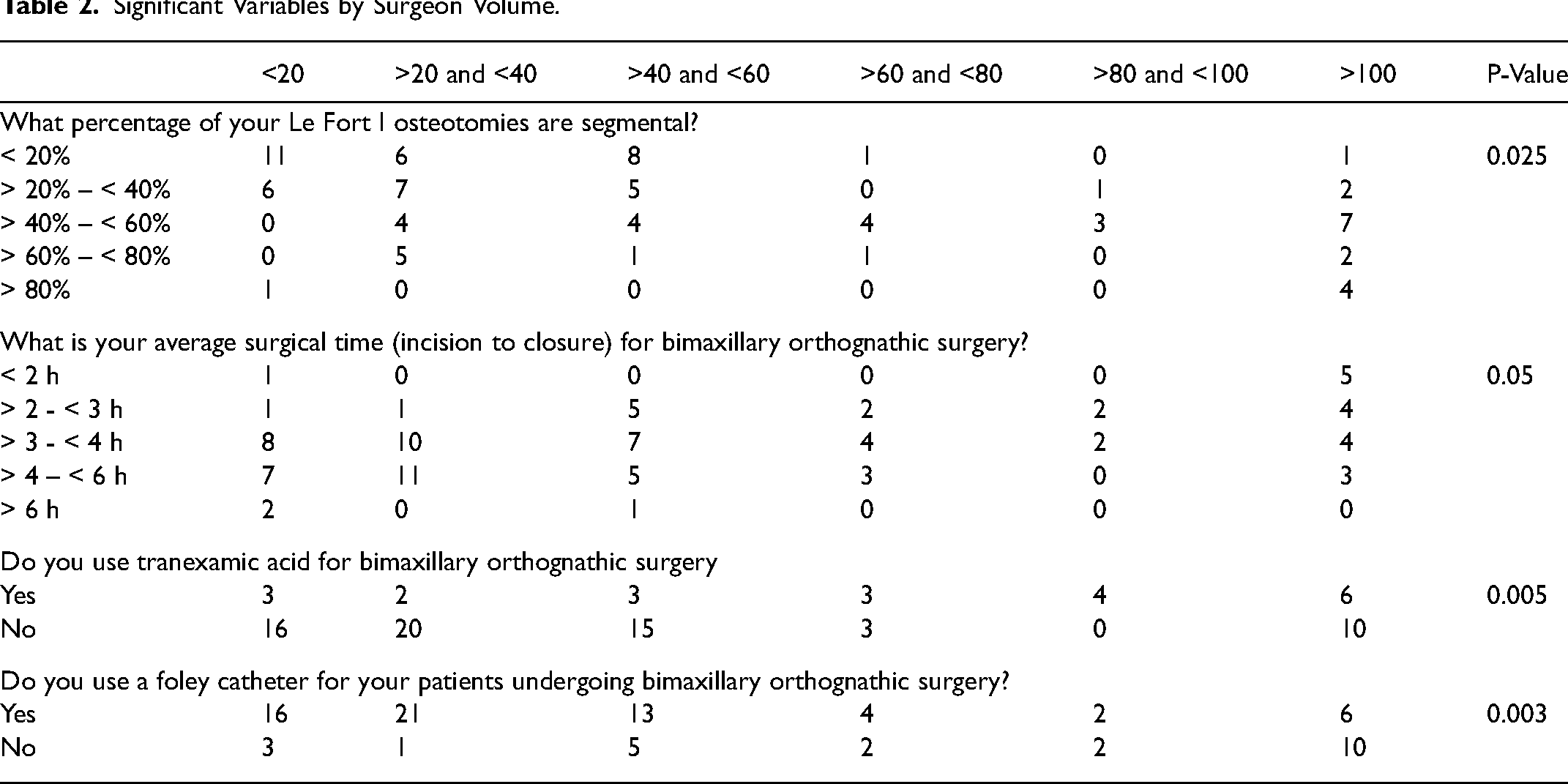
Respondent surgical volume was found to show statistically significant differences in the percentage of segmental Le Fort I osteotomies (P <0.02) (Table 2). Lower volume surgeons had the highest percentage of single-piece Le Fort I osteotomies. Surgical volume also showed significant differences in average surgical time for bimaxillary surgery (P = 0.05), use of TXA (P < 0.01), and use of a foley catheter (P < 0.01). Surgeon volume was not associated with surgeon age or years of practice.
Significant Variables by Surgeon Volume.
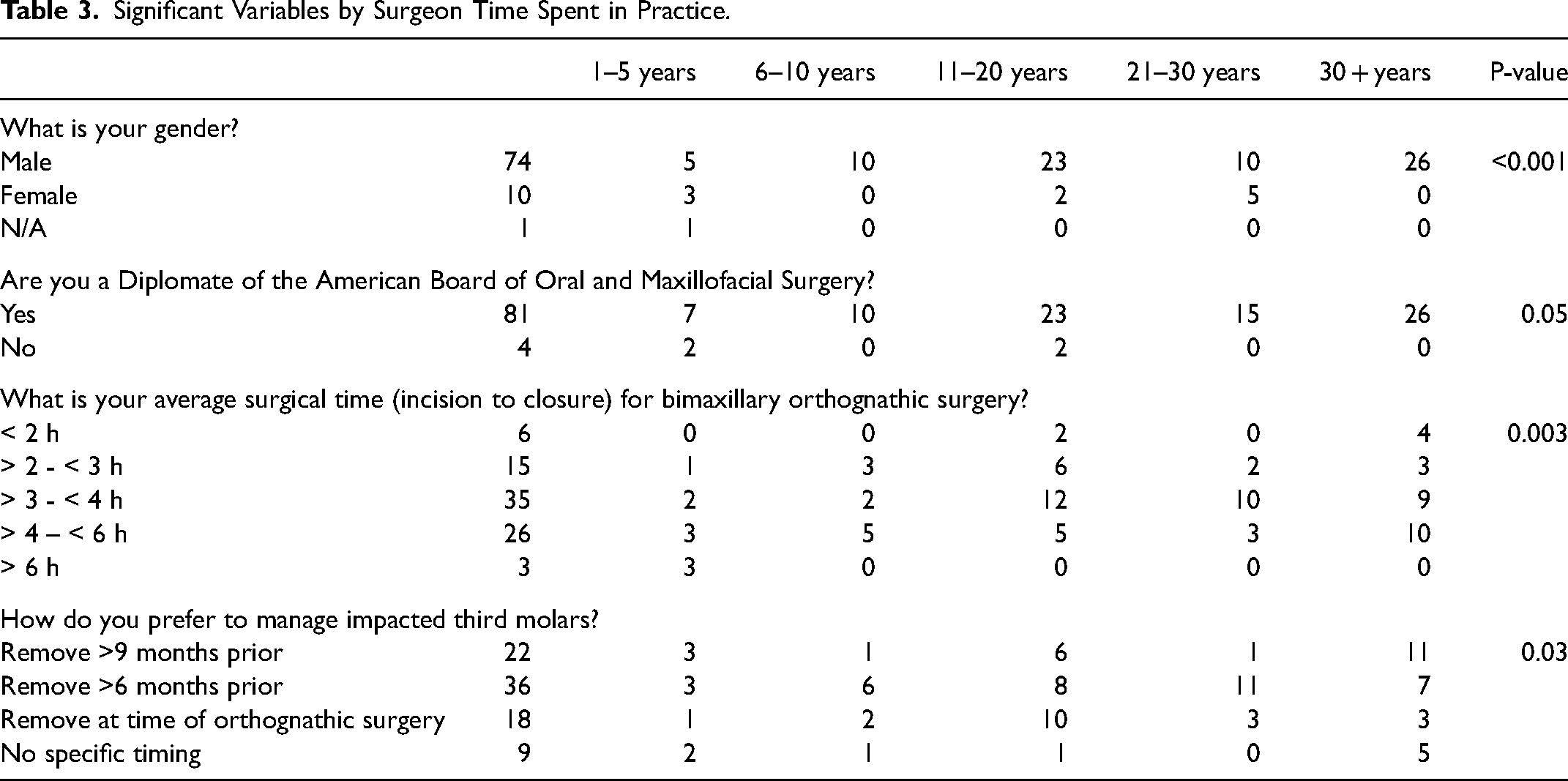
Respondent years spent practicing post residency or fellowship show statistically significant differences in gender (P <0.001) with longer practicing surgeons tending to be males (Table 3). Longer practicing surgeons were more likely to be diplomats of the American Board of OMFS (P = 0.05). Years spent practicing also showed significant differences in average surgical time for bimaxillary surgery (P < 0.01) and management of impacted third molars (P < 0.05).
Significant Variables by Surgeon Time Spent in Practice.
Discussion
The purpose of this study was to describe the current practice patterns among US academic OMFS. We hypothesized that there would be large variability in orthognathic surgery practice patterns at US academic training centers. We aimed 1) to describe the current practice patterns of US academic OMFS 2) to describe differences in practice patterns between different surgical volume surgeons.
The results of the study confirm that there is wide variety in orthognathic surgery practice patterns, only 13 of the 32 of the practice and surgical variables had a single response holding a simple majority (>50%). The results of this study demonstrate the need for further research to allow for evidence-based protocols and decision making and a focused curriculum for orthognathic surgeons in training.
Our response rate was similar to other survey based research, and all regions were represented.2–5 The largest demographic was 61–70 years of age. This demographic will be transitioning out of the workforce in the near future suggesting that a shortage of academic OMFS orthognathic surgeons may occur. For the respondent group, the majority of surgeons operate less than 60 orthognathic surgeries per year with an outlier group operating greater than 100 surgeries a year. Berlin et al. has documented a trend of centralization of care for orthognathic surgery with an annual increase in the rate of patients treated at high-volume hospitals. 6 Berlin and Gupta have both documented that high volume hospitals are less likely to experience complications or extended length of stay, and recommend regional collaboration and quality improvement through identification and dissemination of best practices.
In regards to the percentage of orthognathic surgeries that are double jaws, the largest response was 60–80% of surgeries. Review of the Nationwide Inpatient Sample (NIS) for the years 1999–2011 demonstrates that in the US, approximately 38% of orthognathic surgery surgeries were double jaw osteotomies.6,7 This discrepancy could be a function of academic centers performing a higher percentage of double jaw surgeries relative to single jaw surgeries, or could be a trend that has occurred over the last decade and not captured in the NIS data. 6 The largest response for percentage of Le Fort I osteotomies that are segmental was <20%. This agrees with a single center study by Steinbacher et al. where 21% of Le Fort osteotomies were segmental however is in discordance with the NIS data from 1999–2011 where 76% of all Le Fort I osteotomies were segmental.8,9
The majority of surgeons reported an operative time under 4 h for double jaw orthognathic surgery. The literature demonstrates multiple groups reporting operative times > 4 h, however as longer operative times are associated with increased swelling, rates of postoperative nausea and vomiting (PONV), and longer hospital stays, surgical efficiency has gained focus.9–16
There is limited data regarding the methods of intraoperative blood pressure monitoring for orthognathic surgery patients. In 2021, a single center retrospective study of bimaxillary surgeries by Lee et al. documented that 44.2% of surgeries used invasive arterial continuous monitoring. 17 Only 23% of the respondents routinely use invasive arterial continuous monitoring. The respondents also reported an average estimated blood loss of <400 mL with a <1% transfusion rate with the largest response requesting an intraoperative mean arterial pressure of 60–64 mmHg. A systematic review examining blood loss in orthognathic surgery over a 30 year period reported an average blood loss of 436 mL, higher than the majority of respondents. 18 Improvement in operative times, decrease in intraoperative blood loss, and relaxation of intraoperative mean arterial pressure goals may account for the low use of intra-arterial monitoring.
Tranexamic acid is a lysine analog that prevents activation of plasmin and limits fibrinolysis. Only 25% of respondents utilize TXA despite multiple meta-analyses documenting a decrease in blood loss and improvement in surgical field with the use of TXA in orthognathic surgery.19–24
Twenty-seven percent of respondents do not use a foley catheter. The American College of Surgeons National Safety and Quality Improvement Project best practices guidelines for limiting catheter associated urinary tract infections limits perioperative use to selected surgical parameters. Two of the parameters potentially relate to the orthognathic surgery patient: 1) anticipated prolonged duration of surgery (>3 h), and 2) need for intraoperative monitoring of urinary output (with low MAPs, allows for indirect measure of kidney perfusion through urine output). With reported OR times decreasing for bimaxillary osteotomies, many orthognathic surgeons may benefit from re-evaluation of the use of a foley catheter for routine surgeries.
Our study found no consensus regarding use of perioperative antibiotic type or duration. Preoperatively, the most used antibiotic is cefazolin/cephalexin while postoperatively, the most used antibiotic is ampicillin/amoxicillin. This suggests some surgeons change their perioperative antibiotic coverage during the perioperative window. Thirty-three percent of respondents only use antibiotics 24 h after surgery while 31% use antibiotics for 7 days after surgery and 26% for 5 days after surgery. Multiple systematic reviews and meta-analyses evaluate perioperative antibiotic use in orthognathic surgery. Preoperative antibiotics are recommended with good quality of evidence but the benefit of prolonged therapy or which antibiotic is recommended remains uncertain.25–29
Seventy-three percent of respondents use steroids greater than 48 h after surgery. Currently, there is no ideal therapeutic perioperative steroid regimen supported by systematic reviews and meta-analyses and no studies report risk of airway compromise or risk of reintubation.30–33 Perioperative systemic corticosteroids have been shown to reduce facial edema and may reduce PONV.30,33 However, there are no benefits on neurosensory recovery or decrease of hospital length of stay.30,33 Weber and Griffin completed a randomized double blind prospective trial where patients undergoing bilateral sagittal splits were randomized into three groups: 1) placebo, 2) preoperative dexamethasone 16 mg intravenously, and 3) preoperative dexamethasone 16 mg intravenously with three postoperative 8 mg doses every 6 h. 34 There was significant reduction in facial swelling on postoperative day 1 in both dexamethasone groups as compared to the placebo. There was no difference between the two dexamethasone groups; suggesting the glucocorticoid treatment may have a ceiling effect.
Naran et al. indicate that while PSIs are highly accurate and useful, the cost has limited widespread use. 35 Although 69% of respondents perform maxillary first surgery in the majority of their surgeries, mandible-first surgery has become more widely used. PSIs have recently gained traction in bimaxillary orthognathic surgery however only 27% of respondent academic surgeons use PSIs in the majority of their surgeries.
Extraction of third molars is often performed at the time of orthognathic surgery and does not significantly increase operative time or incidence of “bad” split during sagittal ramus osteotomies, however, the majority of respondents prefer to remove third molars at least 6 months prior to surgery.36,37
An in vitro study by Ribeiro-Junior et al. demonstrated that bicortical screws provides better stabilization of bone segments with or without locking miniplates, however 58% of respondents fixate their sagittal ramus osteotomies with a single monocortical plate. 38 This suggests that while a monocortical plate was not demonstrated as the strongest fixation technique in vitro, a monocortical plate may be of sufficient fixation strength in vivo. Unfortunately this topic has not been well reported in vivo to date.
In 1991, Polido, Ellis, and Sinn documented the superiority of external reference points over internal reference points in defining the intraoperative maxillary vertical position. Despite this, 6% of respondents utilize an internal landmark reference point when defining the intraoperative vertical dimension and 8% do not directly measure when using occlusal wafers/splints. Twenty percent reported to set the vertical dimension through PSIs which does not require defining the intraoperative maxillary vertical position.
Only 29% of study participants use an ERAS protocol. ERAS protocols are an evidence-based, fast-track approach to surgery, which relies upon perioperative care protocols, designed to attenuate the stress response during the perioperative period. Stratton et al. implemented an ERAS protocol designed to decrease opioid use and decrease incidence of PONV for patients undergoing orthognathic surgery. After implementation of the ERAS protocol, their patients received less opioids and had a lower incidence of PONV. 39 While ERAS protocols have been shown to be effective for orthognathic surgery they have yet to be implemented and formally adopted by the ERAS society.39,40
Eight-five percent of study participants discharge their bimaxillary osteotomy patients postoperative day 1. Bowe et al. and Huamán et al. independently reported hospital length of stay in large respective samples where the average length of stay was 1.2 days and 1.3 days respectively.15,41 Fifteen percent of respondents admit their orthognathic surgery patients with OSA to the intensive care unit (ICU) postoperatively. A recent study by Lee et al. retrospectively evaluated 104 maxillomandibular advancement patients finding no difference in mean SpO2 nadir, postoperative complication rate, or hospital length of stay (LOS) between patients admitted to the ICU or surgical floor. 42
There are limitations to this study that merit discussion; most relating to survey-based research. The respondents who completed the study reported performing a relatively high number of surgeries per year which suggests that individuals who do not perform orthognathic surgery may have self-selected from the study group. As the respondent data is anonymous, we are unable to determine if each academic program is represented. Second, the data is self-reported, as such, recall and surgeon bias may impact the data. Lastly, the respondents interpretation of the survey question may vary despite effort to design clear questions and responses.
Conclusion
Currently there is large variation in orthognathic surgery practice patterns among academic OMFS with limited clinical practice guidelines. While advances have been made towards an evidence-based practice, adequate data is still lacking from many key decision points. Only 13 of the 32 survey questions had a single response holding a simple majority (>50%). The results of this study demonstrate the need for a focused curriculum for orthognathic surgeons-in-training and further research to allow for evidence-based protocols and decision making.
Footnotes
Acknowledgements
This project was supported by the Oral and Maxillofacial Surgery Foundation Student Research Training Award (GB).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Oral and Maxillofacial Surgery Foundation, (Student Research Training Award).