
Abstract
EDS (Ehlers-Danlos Syndrome) is a heterogenous group of inheritable connective tissue disorders that commonly precludes patients from being elective surgical candidates. Patients with EDS are at a higher risk of increased bleeding, delayed wound healing, and temporomandibular joint pain refractory to treatment. Historically, patients with EDS and TMJ disorders are considered inappropriate surgical candidates due to a higher risk of delayed wound healing, increased risk for uncontrolled post-surgical bleeding, and unsubstantiated outcomes in regards to elective orthognathic surgery. A review of the literature demonstrates a paucity of data accounting the use of orthognathic surgery and maxillary-mandibular advancement in patients with EDS. The present study reports on the use of orthognathic double jaw surgery in a patient with a known diagnosis of hypermobile EDS, history of TMJ subluxation and pain. This case describes a 47-year-old woman with a history of hypermobile EDS who presented with Angle Class II malocclusion, Class II skeletal pattern, and clockwise rotation of the occlusal plane associated with pain at the bilateral TMJs. She underwent maxillary-mandibular advancement with counterclockwise rotation of the occlusal plane and genioplasty. The surgery was without complications, and at 22 months follow up, the patient healed uneventfully with improvement of pain and range of motion. This case report demonstrates that with diligent patient selection, orthognathic surgery in patients with EDS can be safe and effective and should not be an absolute contraindication.
Keywords
Introduction
The Ehlers-Danlos Syndromes (EDS) are a group of inherited connective tissue disorders characterized by joint hypermobility, skin hyperextensibility, and fragility of vessel walls. There are at least 13 recognized subtypes, and the prevalence ranges from 1 in 5000 to 1 in 500. 1 Due to tissue and ligamentous laxity, patients with EDS often present with recurrent temporomandibular joint (TMJ) subluxation and pain refractory to most treatment methods. 2 Patients also tend to have excessive bleeding, such as when brushing their teeth, traumatic injuries, and during routine surgery despite no inherent coagulopathy. 3 The oral mucosa is especially vulnerable, frequently contributing to the development of intraoral ulcers. Postoperatively, thorough monitoring of the incisions is necessary because of an increased risk of hematoma, delayed wound healing, and infection.
In the literature review, there were two reported EDS patients who had both undergone single jaw orthognathic surgery. 4 At 3 months follow-up, one patient had limited mouth opening, poor occlusion, and persistent pain at the left TMJ. The patient also had infection of the osteosynthesis plates which were subsequently removed. 4 The literature largely recommends conservative treatment for patients with EDS due to fear of possible postoperative complications and poor outcomes.5,6 However, the literature is scarce in reporting on the successful use of double jaw orthognathic surgery in a patient diagnosed with Ehlers Danlos Syndrome.
The aim of this report was to review the literature for orthognathic surgery in patients with EDS and report an EDS case with refractory TMJ pain who underwent 2-jaw surgery with concurrent genioplasty with a follow-up period at 22 months.
Review of the Literature
A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist guided online search of SCOPUS, Pubmed, Embase, and Cochrane was conducted for all recorded history to present time by two independent reviewers. The following search terms were used in all online registries as the following: “Ehlers-Danlos AND orthognathic surgery,” “Ehlers-Danlos AND orthognathic,” “Ehlers-Danlos AND craniofacial surgery,” “Ehlers-Danlos AND double jaw,” “Ehlers-Danlos AND double jaw surgery,” “Ehlers-Danlos AND occlusal surgery,” and “Ehlers-Danlos AND maxillofacial surgery.” Inclusion criteria included any patients with reported a diagnosis of Ehlers Danlos, a diagnosed occlusal discrepancy, and had craniofacial surgical intervention(s) (eg, single maxillary, single mandibular jaw surgery or double jaw surgery). Exclusion criteria included any patients that were managed with non-operative means and no follow up. Outcomes included type of craniofacial surgery and any associated complications.
There was significant paucity in the literature in terms of results for EDS and orthognathic surgery (Figure 1). Over seven keyword searches per databases (n=4) were conducted with 58 results and only 5 papers fulfilling full review criteria, for a total of 21 patients. There were two patients that reported to have had orthognathic surgery with clinically diagnosed EDS: surgically assisted rapid palatal expansion (SARPE) and Le Fort I osteotomy (n=1), SARPE with bilateral sagittal split osteotomy (BSSO) and genioplasty (n=1). 4 The review did not find any publications describing EDS patients with double jaw surgery. The remaining 19 EDS patients underwent various localized craniofacial surgeries including isolated teeth extraction (n=8), SARPE (n=3), disc repositioning and myofascial flaps (n=2), TMJ arthrocentesis (n=1), TMJ discopexy (n=1), disc fusion and capsule plication (n=1), surgical orthodontic camouflage (n=1), abscess drainage (n=1), and removal of osteosynthesis hardware (n=1).4–8
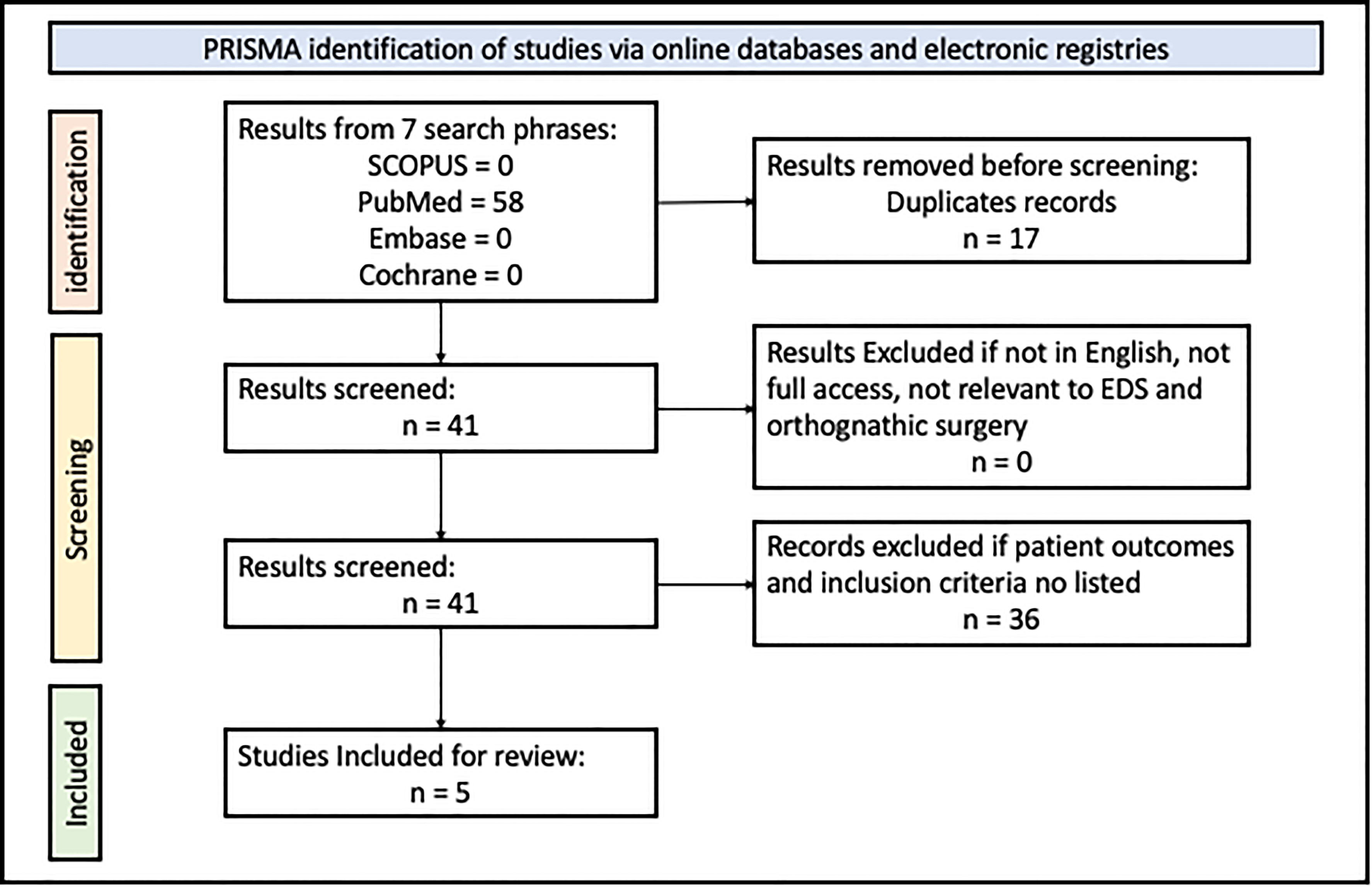
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) search query of keyword phrases for orthognathic surgery in ehlers-danlos syndrome patients.
Case Report
Case Report (CARE) checklist guidelines were adhered in the reporting of the following case. All photographic imaging of the patient was taken with a signed institutional patient photographic consent provided for the purposes of publication in an academic peer reviewed journal.
The current report describes a 47-year-old female with a history of hypermobile EDS who presented complaining of pain at the level of bilateral TMJs. She reported constantly protruding her mandible to improve her speech and dental occlusion. Clinically, she had Angle Class II malocclusion, Class II skeletal pattern with a retrognathic mandible, deficient mandible and chin with clockwise rotation of the occlusal plane (Figure 2). She had an Index of Orthognathic Functional Treatment (IOFTN) score of 4.9 She had excess gingival exposure of greater than 3mm while smiling. 9 The overjet was 6mm, overbite was 1mm with functional difficulties, and had facial asymmetry with occlusal disturbance. The patient started with Angle Class II malocclusion, Class II skeletal pattern and was decompensated lingually tilting the mandibular incisors and labially tilting the maxillary incisors which provided appropriate space and bite closure. The pre-surgical orthodontic decompensation was paramount to provide successful post-operative occlusion after double jaw advancement. Past medical history was notable for fibromyalgia, irritable bowel syndrome, myofascial muscle pain and spinal stenosis. She had a previous rhinoplasty by another provider. The patient's preoperative Apnea Hypopnea Index (AHI) was 3.3 indicating no sleep apnea present. AHI evaluation is routinely performed pre-operatively in adult patients undergoing orthognathic surgery to identify any underlying obstructive pathology. Magnetic resonance imaging showed bilateral anteriorly and laterally displaced discs without reduction, while the computed tomography showed right greater than left TMJ degenerative joint disease (Figure 3).

Intraoral photographs demonstrated preoperative angle class II malocclusion on frontal and lateral view (top) and improvement in occlusion on frontal and lateral view (bottom) at 1 month pre-operatively.
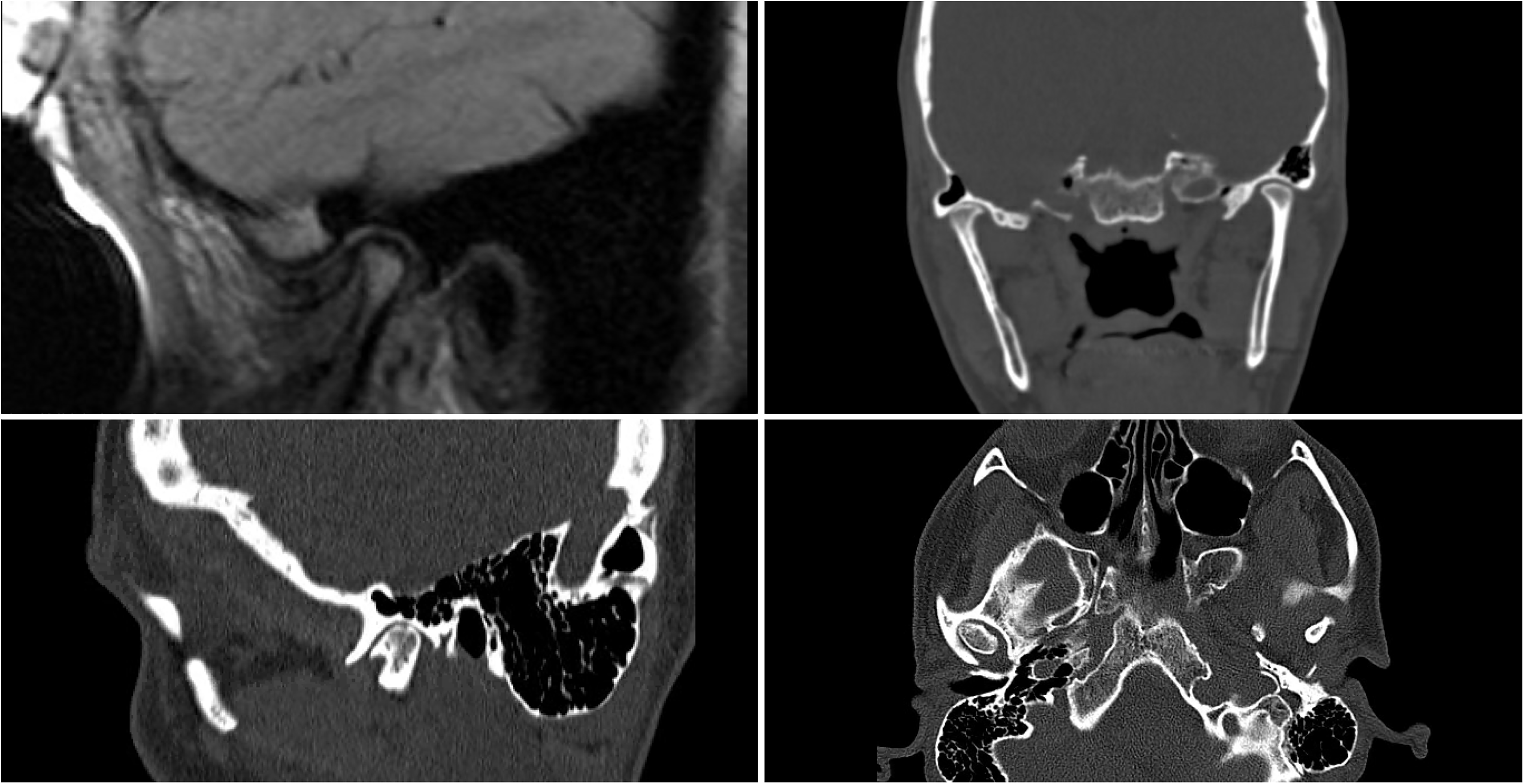
Magnetic resonance imaging (MRI) and computed topography (CT) of the patient's temporomandibular joint month-25 pre-operatively. The MRI (top left) demonstrates noticeable anterior displacement of the articular disc. The coronal CT (top right) demonstrates destruction of the cartilaginous interface with direct contact of the condyle with the fossa on right greater than left. Sagittal cut (bottom left) and axial cut (bottom right) of the pre-operative CT scan reiterating condylar to glenoid fossa degenerative changes.
Cephalometric Findings
The patient initially underwent a period of conservative treatment with occlusal splinting, anti-inflammatory and muscle relaxants. She had failed treatment and then underwent maxillary-mandibular advancement with counter-clockwise rotation of the occlusal plane, advancement and lengthening sliding genioplasty based on soft tissue cephalometric analysis (Figure 4). The patient presented with a Class II skeletal relationship confirmed by ANB and Witts, bimaxillary deficiency (decreased SNA and SNB), decreased anterior cranial base length, increased SN-Mandibular angle, well compensated and proclined lower incisors, and increased naso-labial angle. Initially the mandible surgery was performed first followed by maxillary advancement (Figures 5, 6, and 7).
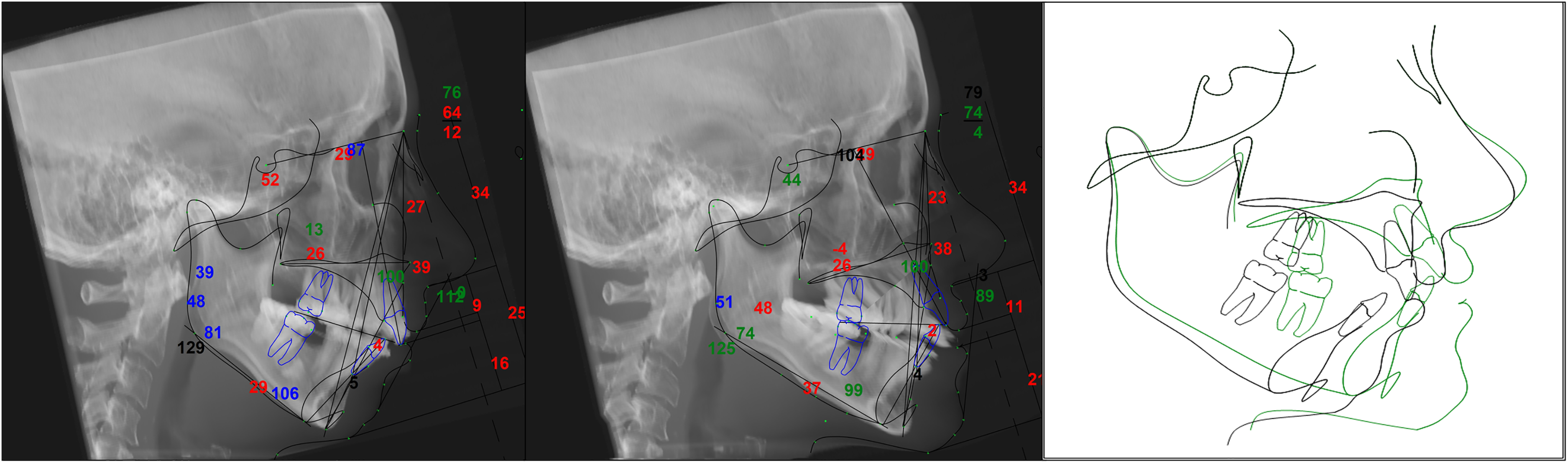
Pre-operative at 1-month (left), superimposed cephalometric tracings (middle), and post-operative at 22-months (right) cephalometric radiographs with the anatomical tracings.
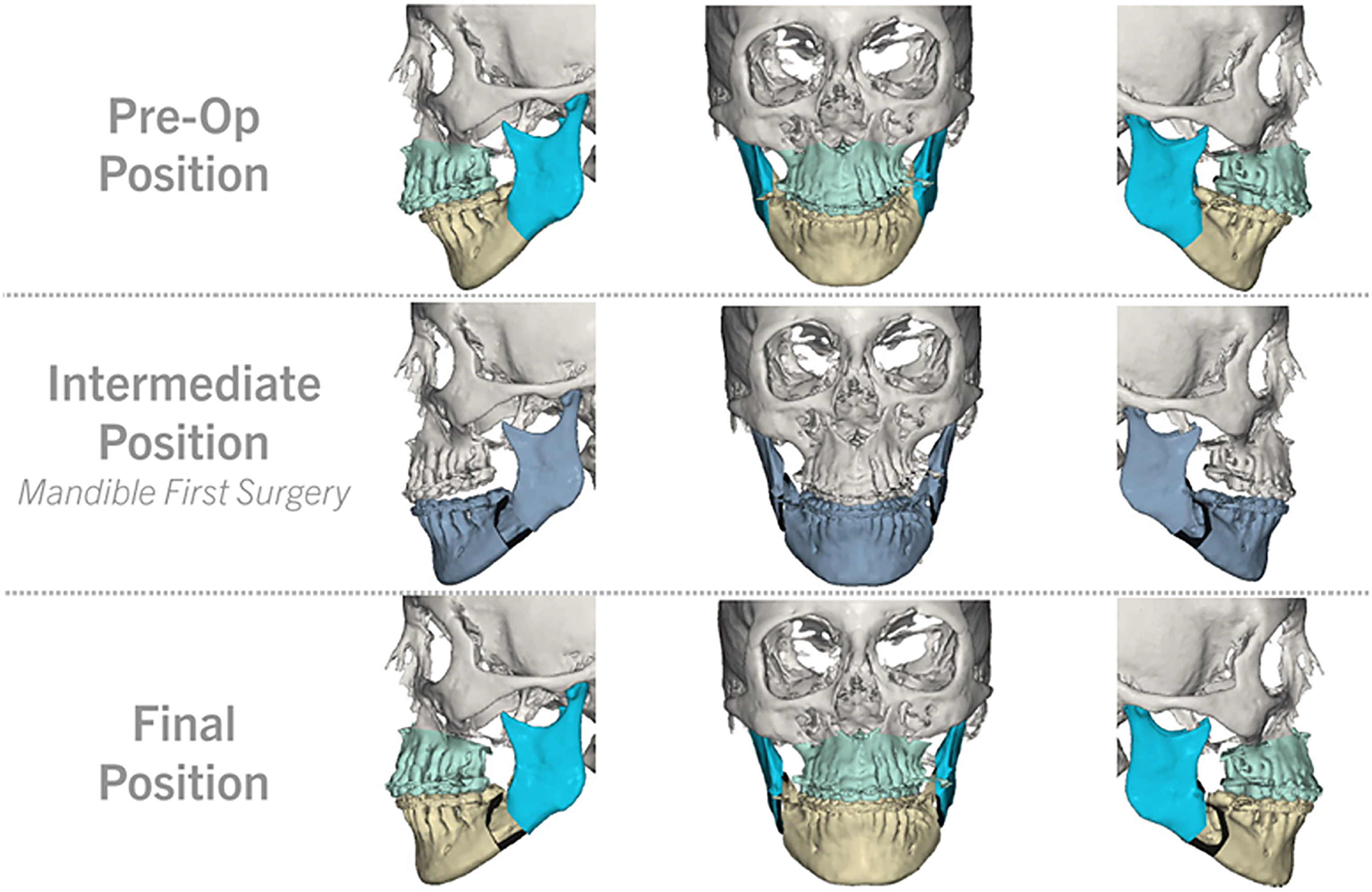
Virtual surgical planning of mandible first double jaw surgery with anterior-posterior and lateral views of the pre-operative, intermediate, and post-operative planned positions. Maxillary-mandibular advancement with counter-clockwise rotation of the occlusal plane 11 degrees and 1.7 degrees clockwise correction of the cant was performed. Her pogonion was advanced 15.2 mm with the bilateral sagittal split osteotomy of the mandible, and the chin was advanced 4 mm with sliding genioplasty.
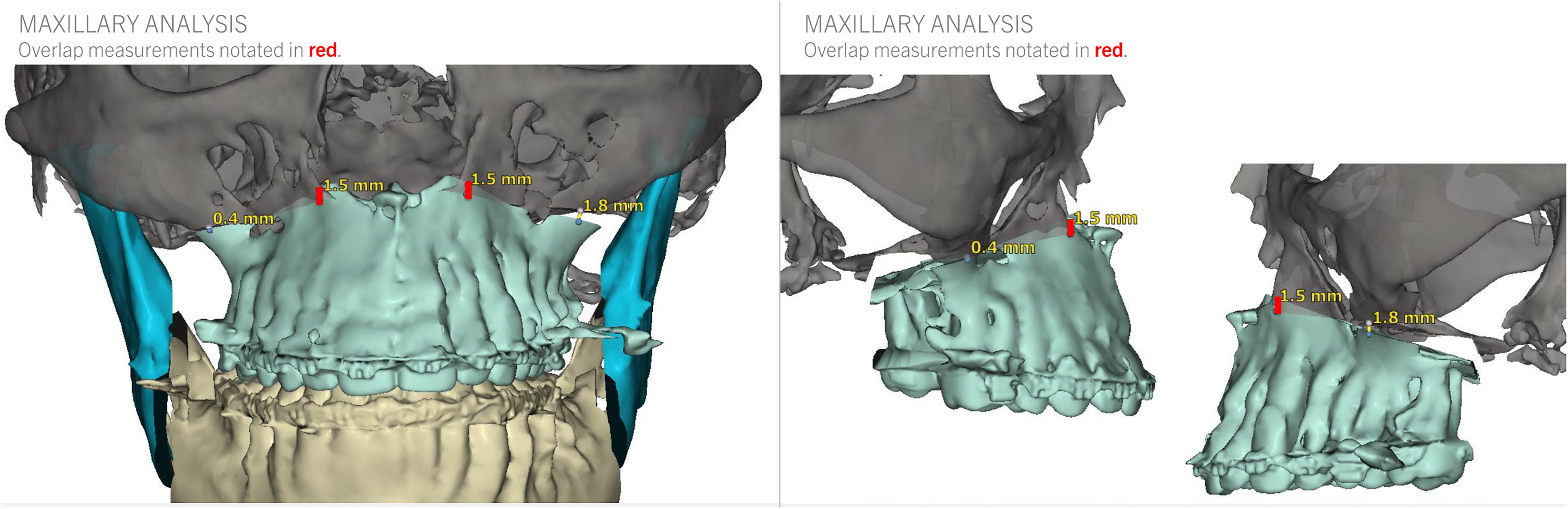
Virtual surgical planning for the maxillary predictions after bilateral leFort I osteotomy and maxillary advancement.
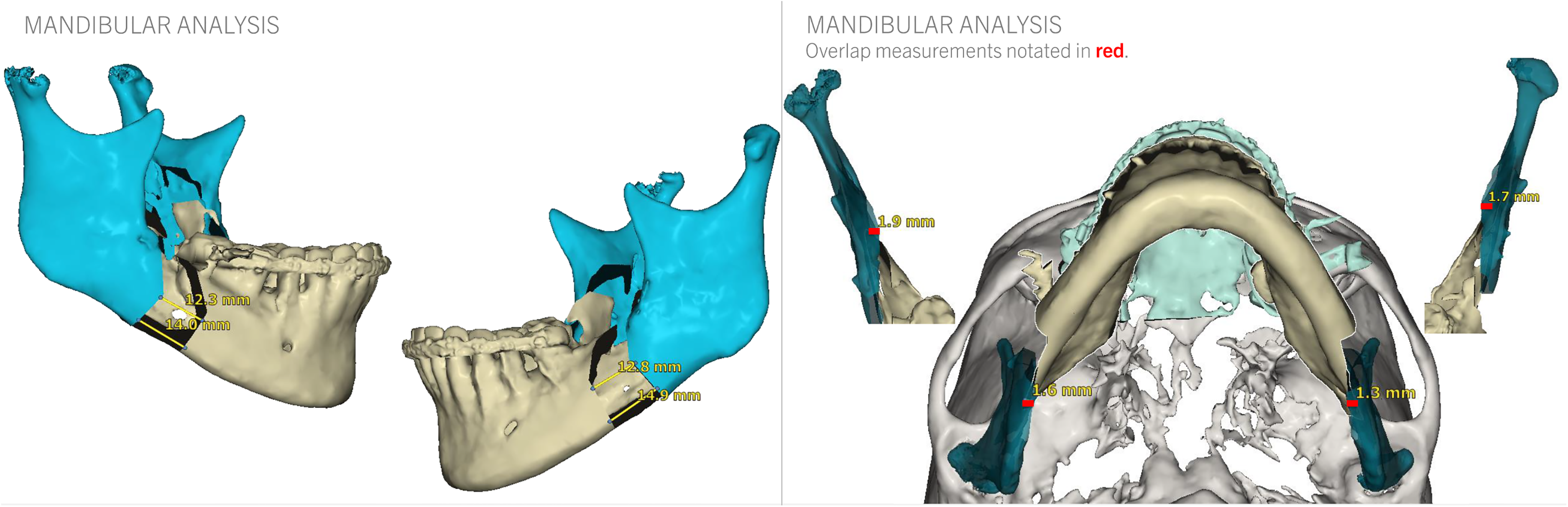
Virtual surgical planning for the mandibular predictions after bilateral sagittal split osteotomy advancement.
Summary of Treatment
The upper incisors were advanced 5 mm and impacted 4 mm. The dental midline was corrected to the facial midline. The pogonion was advanced 15.2 mm with the bilateral sagittal split osteotomy of the mandible, and the chin was further advanced 4 mm. Bone grafts harvested from the palatine bone and posterior maxilla were used to graft the anterior maxilla. The occlusal plane was rotated counter-clockwise 11 degrees and there was 1.7 degrees clockwise correction of the cant. She had improvement in her submandibular area solely with the use of mandibular advancement and genioplasty and without submental liposuction. Her hemoglobin dropped from 13.0 g/dl preoperatively to 6.7 g/dl on day one and 9.3 g/dl on day two after the surgery. Clinically, she was stable and did not require blood transfusion. She healed uneventfully without any complications.
At the 22nd month follow-up, the patient had a stable and improved symptomatic result (Figures 8 and 9). At her 1-month, 6-month, and 12-month follow up she was healing appropriately, no complications associated with EDS including delayed wound healing, episodes of bleeding, ecchymosis or mucosal ulceration. It was noted during her follow up appointments that her nasal width increased, she had resolution in bilateral TMJ pain at 1-month post-op, and improvement in her frontal, profile, cervicomental angle and facial projection. The patient reported significant improvement in her orofacial pain during the masticatory movements. The maximal interincisal opening was 40 mm on active mouth opening with translation (right and left) and protrusion of the mandible at 10 mm. The fatigue reported during the day and the aesthetic balance of the face were both improved after the surgery. At 22-month follow up, rigid and stable fixation was demonstrated on panoramic imaging (Figure 10).

Frontal 1-month pre-operative and 22-month post-operative photographs at follow up. Top left is pre-operative frontal view at rest. Top right is post-operative frontal view at rest. Bottom left is pre-operative frontal view on smile. Bottom right is post-operative frontal view on smile.

Lateral 1-month pre-operative and 22-month post-operative photographs at follow up. Top left is pre-operative lateral view at rest. Top right is post-operative lateral view at rest. Bottom left is pre-operative lateral view on smile. Bottom right is post-operative lateral view on smile.
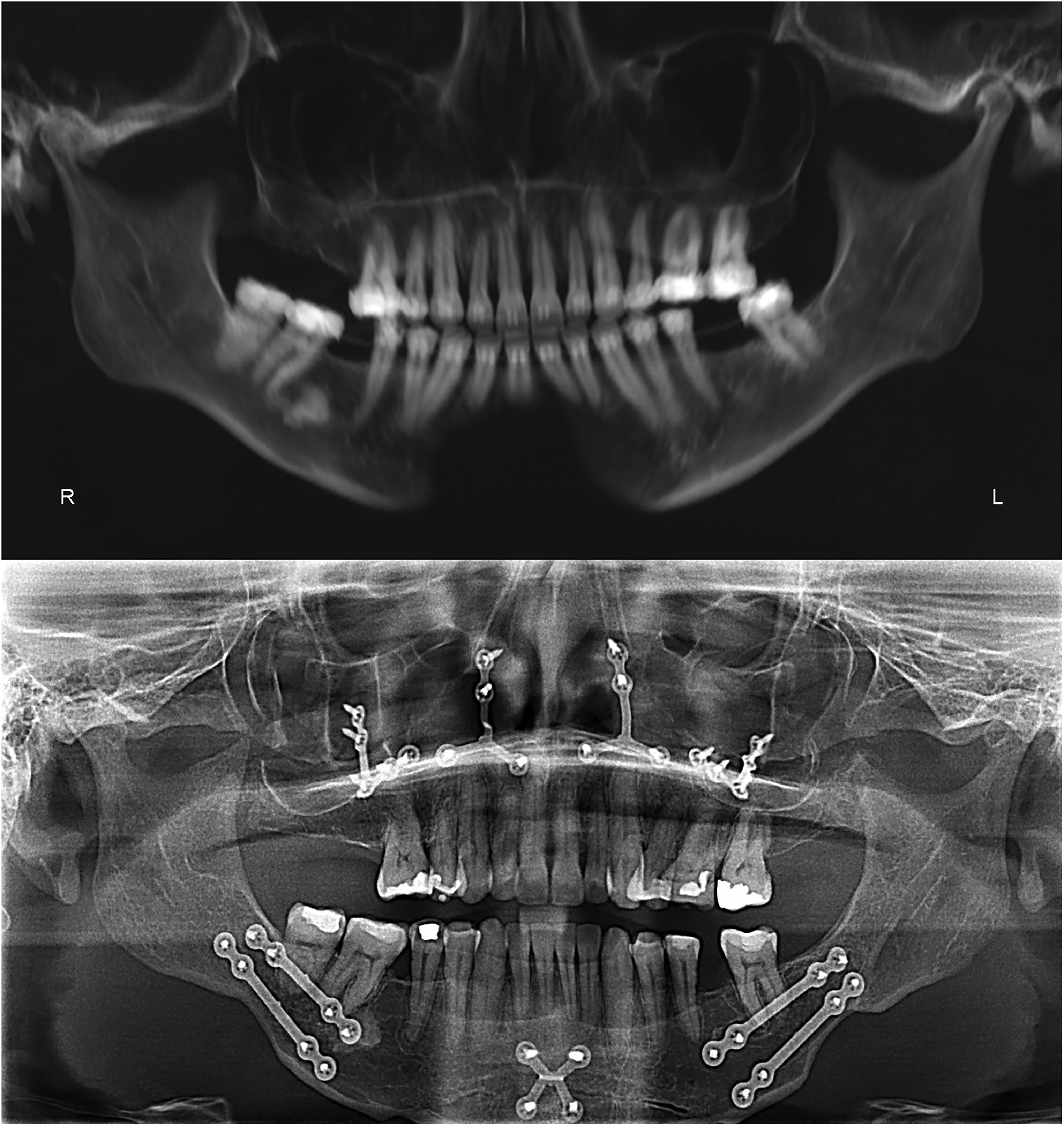
(Top) 1-month pre-operative panoramic x-ray imaging. (Bottom) Panoramic x-ray imaging at 22 month follow up with the bilateral sagittal split osteotomy fixation plates, genioplasty plate and bilateral maxillary medial and lateral buttress fixation plates with appropriate union. KLS Martin (Arnett plates) were used for the mandible with 2 plates on each side with 2 screws on each side of the osteotomy per plate. For the maxilla, a medial and lateral buttress plate was used with at least 2 screws on each side of the osteotomy plate. The genioplasty plate had 2 unicortical screws on each side of the osteotomy. All the screws were 5 mm in length and 2 mm in width. The patient was placed on 2 medium 4 oz. guiding elastics 3/16" after the surgery and soft food for 6 weeks when she was gradually transitioned to a normal diet over the following 6 weeks. She used rubber bands at night up to 3 months after the surgery.
Discussion
EDS are a heterogenous group of inheritable connective tissue disorders that affects up to 9% in US populations and 1 in 150,000 in southern English populations.10–12 Although knowing the correct diagnosis is important, all subtypes of EDS carry some increased risk of poor wound healing, abnormal scarring, and bleeding complications.13–17 Vascular EDS carries the greatest risk for severe bleeding and anesthesia complications such as tracheal rupture.10,18 Therefore, some authors have considered EDS to be an absolute contraindication for elective surgery. 10
Many patients with EDS have Angle Class II or III malocclusion, TMJ pain, functional limitations and are treated with orthodontic camouflage due to the risks of skin bruising, poor healing, and exacerbating temporomandibular disorders.5,7 Only two patients with EDS were reported in the literature of having orthognathic surgery, most likely due to fear of complications during or after the surgery. One patient with an Angle Class III malocclusion, was treated by SARPE distraction osteogenesis and a Le Fort I osteotomy without a complication. 4 The other patient with Angle Class II malocclusion was treated with SARPE, BSSO and genioplasty. However, at 3-months post-op the authors found limited mouth opening, poor occlusion, and persistent pain at the left TMJ. 4 The review of the literature demonstrated limited clinical scenarios of EDS and orthognathic surgery but all relevant studies are vehemently steadfast that EDS patients are poor surgical candidates making treatment options restricted.
In our patient with the clinically diagnosed hypermobile EDS subtype (hEDS), we did not report any complication during or after the surgery. Muscular spasms, TMJ pain and masticatory muscles pain improved after the surgery, due to severe malocclusion correction. Before the corrective surgery, the patient reported constantly protruding the mandible when speaking and eating in order to improve her function. The patient had orthodontic decompensation before the surgery and orthodontic treatment after the 2-jaw surgery was performed. Debate exists as to whether orthognathic surgery can worsen or improve TMJ symptoms with no prospective or retrospective analysis corroborating either claim.19–24 For patients with TMJ pain, reproducing the original condylar position is difficult as too much pressure can be inadvertently placed against the articular discs and exacerbate the symptoms. However, an unfavorable condylar position can be created with BSSO. These conditions can potentially result in joint noise or pain and can worsen any pre-existing TMD symptoms. 25 In our patient, utilization of 2 plates and unicortical screws on each side, avoidance of condylar bearing fragment torque, and gentle posterior and superior placement of the condyle prevented displacement and malposition of the condyle. During the surgery, there was also the same amount of bleeding as expected with a typical orthognathic case. The hemoglobin level decreased after the surgery, but the patient was well and did not require any blood transfusion.
At 22-month follow-up, the result was stable with complete healing of the osteotomies. Frontal and lateral views did not demonstrate any evident recurrence or relapse. Studies have shown that postsurgical relapse mainly occurs in the first few months after surgery, although, the authors admit that there is debate within the field. 26 Most studies on post-operative relapse and stability only record data until 1 year after the surgery as authors assume relapse would occur within this timeframe. 27 The present case and review of the literature aids surgeons in conceptualizing the importance of pre surgical evaluation in high risk patients undergoing elective orthognathic surgery at a longer duration of 22 months. The patient presented benefited greatly from her orthognathic surgery from a functional as well as aesthetic perspective. She had improvement in her occlusal discrepancy, maxilla-mandibular projection and cervico-mental angle. We feel her functional improvements, reduced TMJ subluxation and pain, achievement in planned orthodontic post-operative occlusal goals and patient self-reported aesthetic satisfaction without any complications deems this a valuable option in patients with hypermobile EDS.
Limitations to the study include the small number of papers and small cohort of EDS patients to have undergone orthognathic surgery. From this study, it cannot be determined if EDS and orthognathic surgery have any association in regards to outcomes or complication profile. The present analysis does demonstrate that these patients are understudied and further prospective studies are necessary to determine any statistical relationship. This analysis does provide orthognathic surgeons with a successful example that under proper care and guidance, EDS should not be regarded as an absolute contraindication for elective surgery.
Conclusion
EDS is a dynamic disease with various presentations and a high risk profile. Therefore, orthognathic surgical consideration should be met with great caution and based upon patients’ needs in an individualized approach. The literature is sparse in terms of how or if surgical management in patients with EDS with recalcitrant TMJ and persistent pain is beneficial. This case contributes to the existing literature base an account of orthognathic surgery performed safely in a patient with EDS while improving patient malocclusion, pain, and cosmetic appearance.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231152632 - Supplemental material for Orthognathic Surgery in Ehlers-Danlos Syndrome: Review of the Literature and Case Report
Supplemental material, sj-docx-1-cpc-10.1177_10556656231152632 for Orthognathic Surgery in Ehlers-Danlos Syndrome: Review of the Literature and Case Report by Anthony DeLeonibus, Joseph Bogart, Bahar Bassiri Gharb and Antonio Rampazzo in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
None
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Ethical/Consent
All photographic imaging of the patient was taken with a signed institutional patient photographic consent provided for the purposes of publication in an academic peer reviewed journal.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.