
Abstract
Objectives
The ideal time for nasoalveolar molding (NAM) of infants with cleft lip and/or palate (CLP) is the first weeks after birth. The burden and responsibility that this method of treatment imposes on parents may result in incompliance. The coronavirus (COVID-19) pandemic and the redirection of health resources can make the situation worse. Therefore, this study evaluated the anxiety, complications, and incompliance of parents undergoing NAM during the COVID-19 pandemic.
Materials and methods
Demographic data of 35 infants with CLP treated during the COVID-19 pandemic, compliance and level of anxiety of both parents in addition to their complications were reported. The association between different variables and incompliance was evaluated by simple and multiple logistic regressions. The level of significance was considered at P value less than 0.05.
Results
The highest level of parental anxiety related to the NAM process was the delay in ending the treatment. Meanwhile, the reason for the highest level of anxiety related to attending the treatment sessions was the probability of the infant's COVID-19 infection. Fathers expressed lower levels of anxiety than mothers, significantly. The most prevalent NAM complication was skin irritation. Parents of younger infants (≤28 days) and those with a history of COVID-19 infection were more compliant.
Conclusions
COVID-19 pandemic caused a significant increase in the level of anxiety in both parents, mainly due to the delay in treatment ending and the possibility of infant's infection. Moreover, considering the importance of treatment time, parents of younger infants were more compliant with the NAM process.
Introduction
The coronavirus disease 2019 (COVID-19), which was declared a pandemic on 11th March 2020 1 caused over 510 million infections and more than 6 million deaths globally (https://covid19.who.int/ accessed 3th May 2022). Governments adopted several restrictions such as wearing masks, social distancing, quarantine, and travel bans to tackle the pandemic. 2 Redirection of medical and human resources to providing pandemic services and the importance of protecting the patients and health workers led to the suspension of unurgent treatments.3,4
Cleft lip and palate (CLP) is the most common congenital craniofacial anomaly, 5 which may result in feeding, speaking, and psychosocial issues.6–8 Presurgical nasoalveolar molding (NAM) introduced by Grayson and Cutting 9 is an effective approach to improve surgical outcomes by reduction of the size of the deformity, reducing complexity and cost of the treatment, declining the need for further surgery, increasing long-term patency of the nasal and upper airway and enhancing aesthetic results.10–16 A recent systematic review concluded that the psychosocial advantages of NAM outweighed its burdens. 17 It is worth mentioning that NAM should be started in the early weeks after birth to achieve the best outcomes. 18 Since the COVID-19 pandemic caused a suspension in elective treatments, some therapeutic procedures for children with CLP were deferred during the pandemic. 19 Therefore, adherence of the parents of those children to early treatment through this period is essential.
Generally, parents of children with CLP experience feelings of confusion, distress, guilt, 20 loss of control, helplessness, and depression 21 since the diagnosis of deformity at birth or earlier. It was reported that the Edinburgh Post-partum Depression Scale of parents of patients with CLP was higher than average. Mothers were less sensitive to their infant's signals and had less contact with their children at 2 months. However, a reduction in maternal stress based on the parenting stress scale has been reported following the start of treatment up to 4 months. 22 It has been claimed that compliance with NAM may be inadequate 23 due to the stress and responsibilities that the treatment imposes on the parents.24,25 In addition, parents of children with CLP are more vulnerable to anxiety and depression, 26 which may even be worsened by the pandemic.
The present study was aimed at evaluating the level of anxiety and compliance of parents of infants with cleft lip and/or palate (CL/CLP) and complications of patients referred to the cleft clinic of to receive NAM treatment during COVID-19 pandemic. The relationship between different variables and parental incompliance with NAM treatment was also investigated.
Materials and Methods
The present study was approved by the research ethics committee of the dental school of with the reference number. Parents of infants referred to the cleft clinic of the dental school of during the 2 years of the COVID-19 pandemic from March 2020 to May 2022 were asked to participate in the study. Informed consent was obtained from the parents. The questionnaires were coded, and the patient's name was not mentioned to keep the information confidential.
The demographic data of infants including gender, age, and type of cleft, were collected based on their diagnostic records. Their birth order and the history of CL/CLP of their siblings were asked from their mothers.
Parents were also asked about their demographic data covering their age and level of education; the living city, as well as the history of CL/CLP in parents and their relatives, travel restrictions during the pandemic, and the history of COVID-19 infection of themselves or their relatives. The overall COVID-19-related anxiety of the parents including the anxiety about the effect of the pandemic or its restrictions on the NAM treatment and their satisfaction with the clinic staff's commitment to the COVID-19 health protocols were recorded using a numeric rating scale (NRS) which rated from 0 to 10. 27 Any factors that could lead to parents’ stress and anxiety regarding the pandemic and their infant's treatment were evaluated. Parents were asked to answer several questions regarding anxieties about the treatment process and attending the appointments. They had to choose from five possible answers on the Likert scale including very low, low, moderate, high, or very high levels of anxiety.28–29 Internal consistency of questions regarding anxieties about the treatment process, including anxiety of delay in treatment ending, disruption of treatment outcome and breakage of the appliance, and the impossibility of arranging an emergency visit because of the pandemic-related restrictions, was evaluated by Cronbach's alpha of 0.75. Internal consistency of questions regarding anxieties about attending the appointments, including the anxiety of restriction of inter- or intra-city travel, risk of the infection on public transportation, risk of the infection of infant or parents, and economic issues during the pandemic, was measured by Cronbach's alpha of 0.76. Additionally, the complications related to the use of the NAM appliance were recorded. The compliance of parents with the NAM process was also recorded according to the reports of their responsible clinician considering two items: how much the parents followed the instructions of appliance usage and how regularly they attended the predetermined appointments.
Statistical Analysis
Qualitative variables were summarized by count and percentage. Means and standard deviations were reported for quantitative variables. Simple and multiple logistic regressions assessed the relationship between independent variables and incompliance. Variables with a P value less than 0.2 in simple regression tests opted for further analysis by multiple regression tests. Considering logistic regression analysis to detect a significant (type one error equal to 0.05) relationship between categorical independent and dependent variables in this study, by 35 cases, we had 80% statistical power to detect at least 45% and 55% differences (with baseline frequencies of 5% and 15%, respectively). The anxiety level of parents was compared with each other using Wilcoxon signed rank test. Variables related to anxiety about the treatment process were compared with each other by the Friedman test. The level of significance was considered at a p-Value less than 0.05.
Results
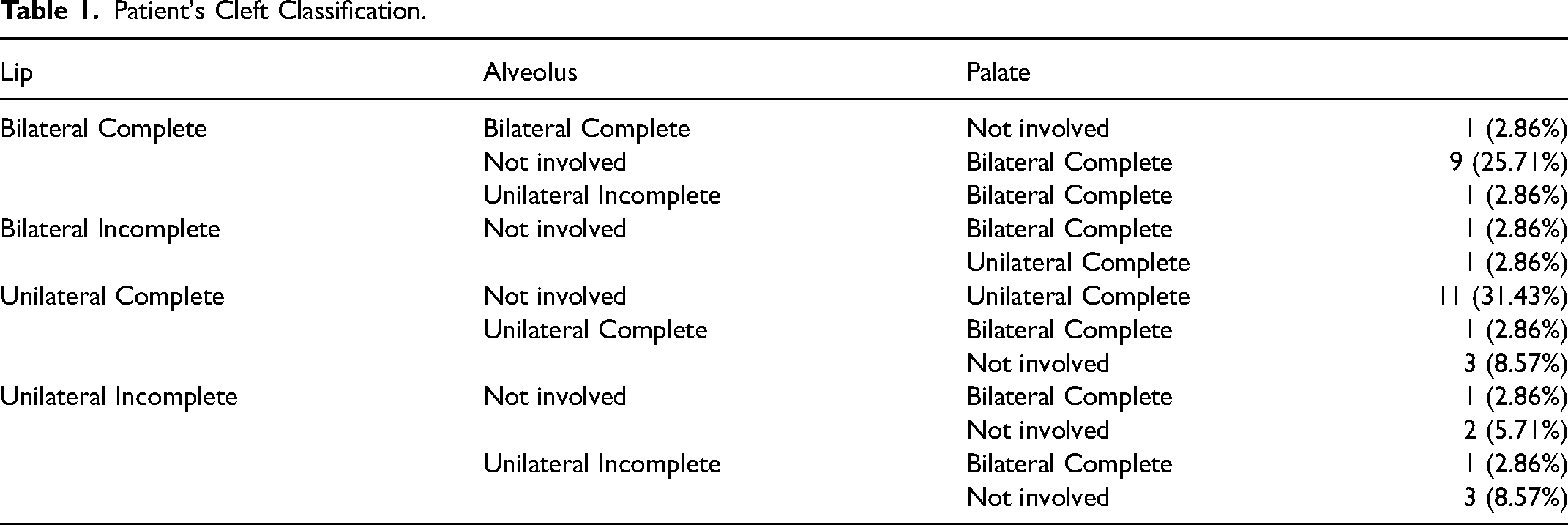
Parents of all infants born with CL/CLP who were referred to our cleft clinic during the COVID-19 pandemic were asked to participate in this study. However, some were excluded due to parents’ refusal to enter the study or receiving the NAM treatment, infants having syndromes, and unfortunately losing one infant. Consequently, the questionnaires were completed by parents of 35 infants. Patients consisted of 13 females (37.1%) and 22 males (62.9%). Seventeen (48.6%) patients were neonates (≤28 d), and 18 patients (51.4%) were older than 28 days. The mean weight at the first visit was 4.06 kilograms (SD=1.04). The classification of patients’ clefts is illustrated in Table 1.
Patient's Cleft Classification.
Parents’ Anxiety
Parents were asked about their anxiety related to the effect of the pandemic on NAM treatment (Table 2). High and very high anxiety levels were considered substantial and reported as H/VH levels of anxiety. The most prevalent H/VH level of anxiety among mothers and fathers was a delay in treatment ending, followed by anxiety about treatment outcomes and anxiety about appliance breakage and lack of access to the clinic in mothers, respectively. Anxiety about treatment outcomes, appliance breakage, and lack of access to the clinic resulted in the same prevalence of H/VH anxiety among fathers. There were no significant differences between the anxiety about the delay in treatment ending, treatment outcomes, appliance breakage, and lack of access to the clinic neither in the mothers’ group (P=0.29) nor the fathers’ group (0.4) using the Friedman test. However, Wilcoxon Signed Ranks Test showed significant differences between mothers and fathers regarding these issues (P<0.05).
Prevalence of H/VH Levels of Anxiety among Mothers and Fathers.
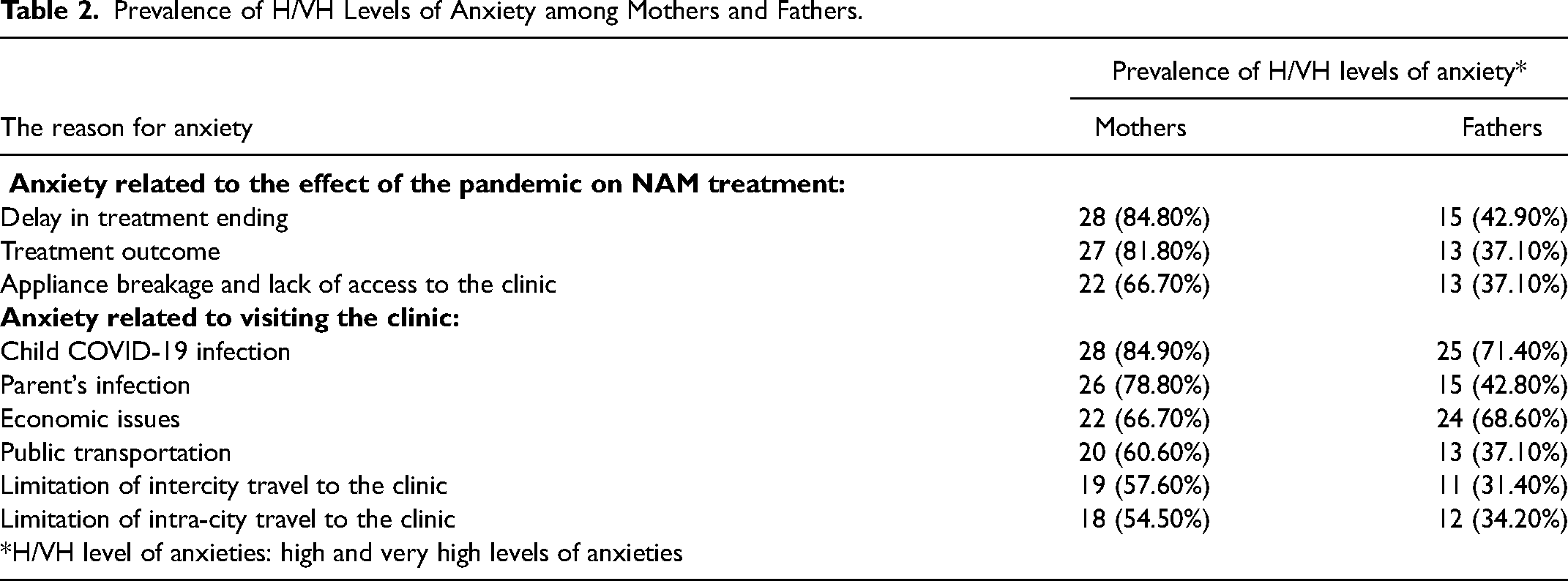
Parents were also asked about their anxieties related to visiting the clinic (Table 2). The reason that caused the most H/VH level of anxiety was the anxiety about child COVID-19 infection in both mothers and fathers groups. Among mothers, the second H/VH level of anxiety was anxiety about the parent's infection, followed by anxiety about economic issues, the safety of public transportation, and the limitation of intercity and intra-city travel to the clinic, respectively. Among fathers, the second H/VH level of anxiety was economic issues, followed by anxiety about the parent's infection, public transportation safety, intercity limitations, and intra-city travel to the clinic, respectively.
Incompliance
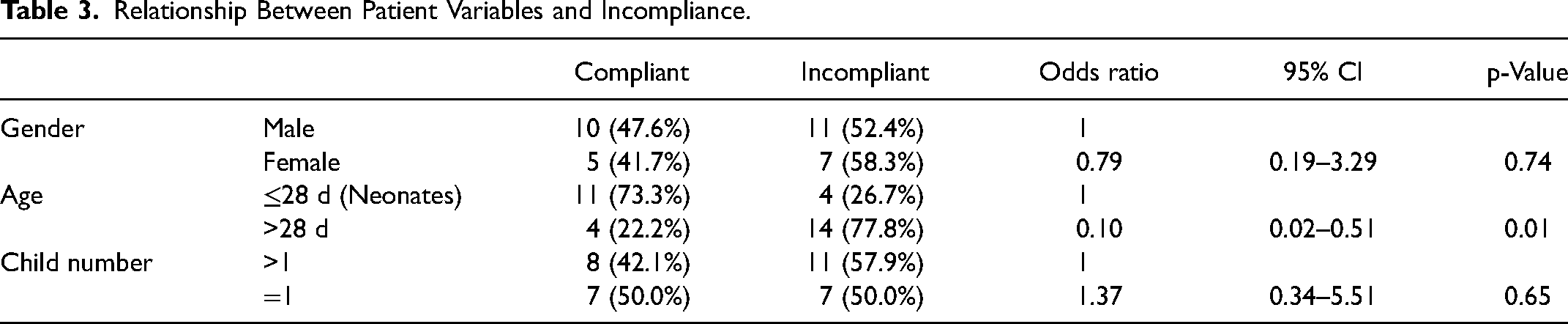
The relationship between the infant's variables and incompliance is shown in Table 3. Multiple regression analysis represented a significant relationship between the patient's age (P= 0.04, CI: 0.03–0.93) and compliance. So, parents of neonates (≤28 d) were more compliant as their incompliance was 0.10 times that of older patients.
Relationship Between Patient Variables and Incompliance.
The relationship between parents’ variables and compliance is illustrated in Tables 4 and 5. According to the multiple regression analysis, the history of the Covid-19 infection of the parents or their relatives showed a significant association with compliance (P= 0.04, 95%CI: 1.14–39.35). Parents without a history of infection were 6.69 times more incompliant than parents with this history. Results indicated no significant differences between the other variables and compliance (Table 3–5). However, there were considerable differences among some variables. For instance, educated mothers with academic degrees were more compliant (57.1%) than less educated mothers (42.3%), Table 4. Fathers without economic problems were more compliant (54.5%) than fathers with this issue (40.9%), Table 5. Patients who lived in Tehran (the capital city) and the suburb were more compliant (61.1%) than those who came from farther cities (26.7%), Table 5.
Relationship Between Mother Variables and two Types of Anxiety with Incompliance.
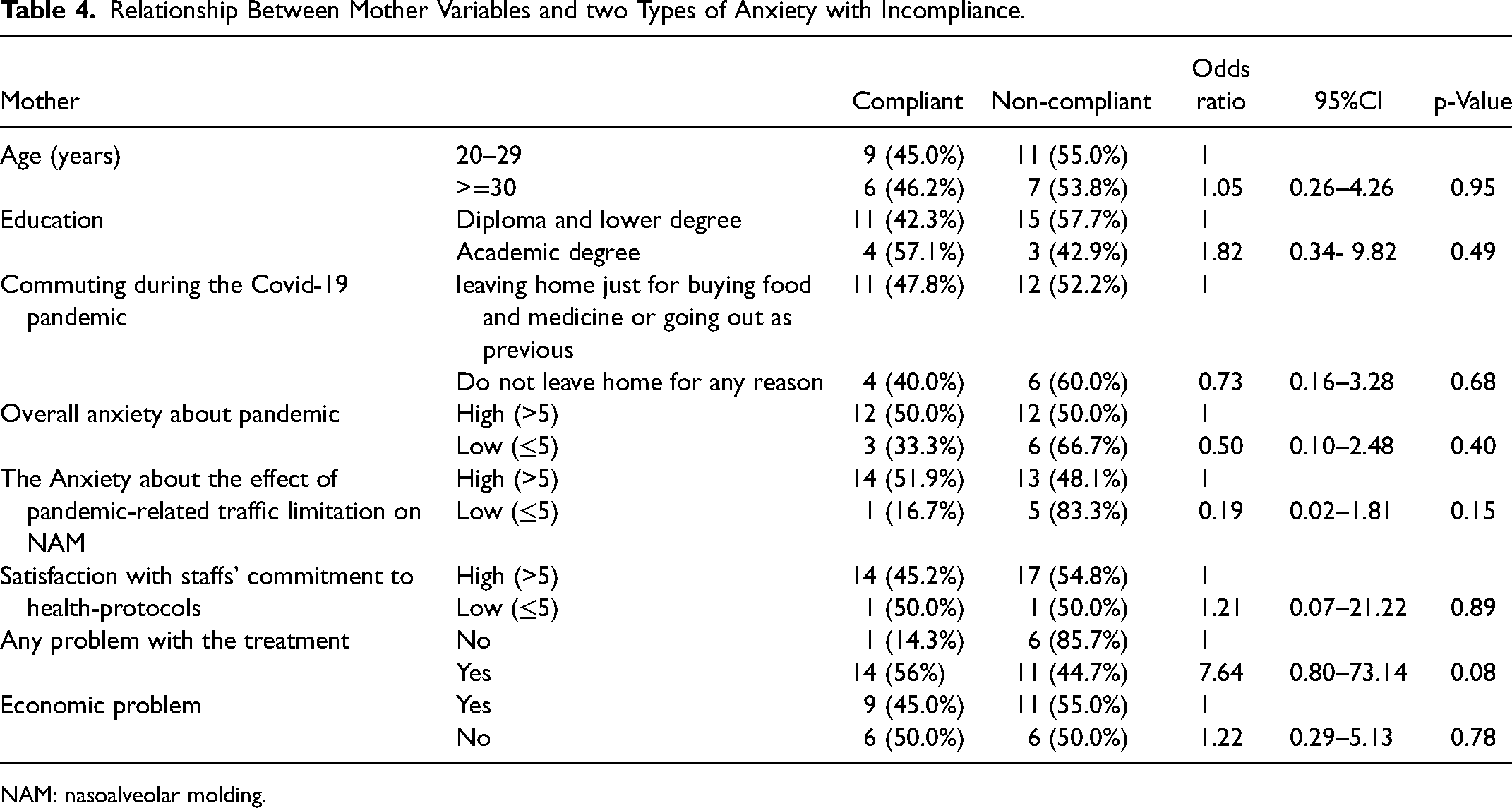
NAM: nasoalveolar molding.
Relationship Between Father Variables and two Types of Anxiety with Incompliance.
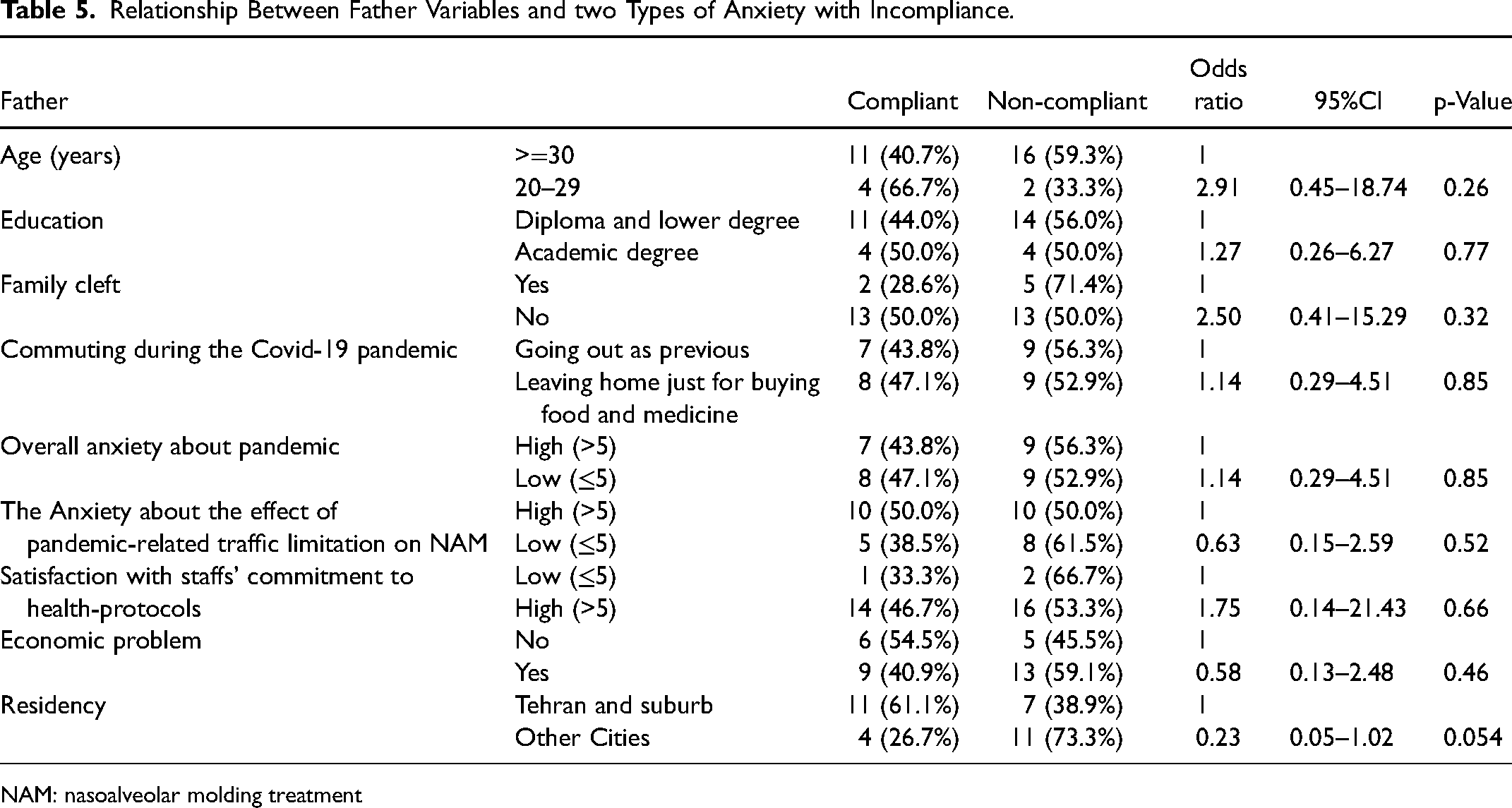
NAM: nasoalveolar molding treatment
Complications
Treatment-related problems that parents encountered are also reported in Table 6. The most common complication, with 54.55% prevalence (n=18), was skin irritation caused by tapes, followed by mouth irritation (n=9, 27.27%) and nostril irritation (n=7, 21.21%). Following this, five (15.15%) parents reported uncertainty about their proper appliance usage; one (3.03%) declared appliance breakage but none lost their appliances. Parents of seven patients (20%) declared no complications.
Complications Related to the NAM Appliance.
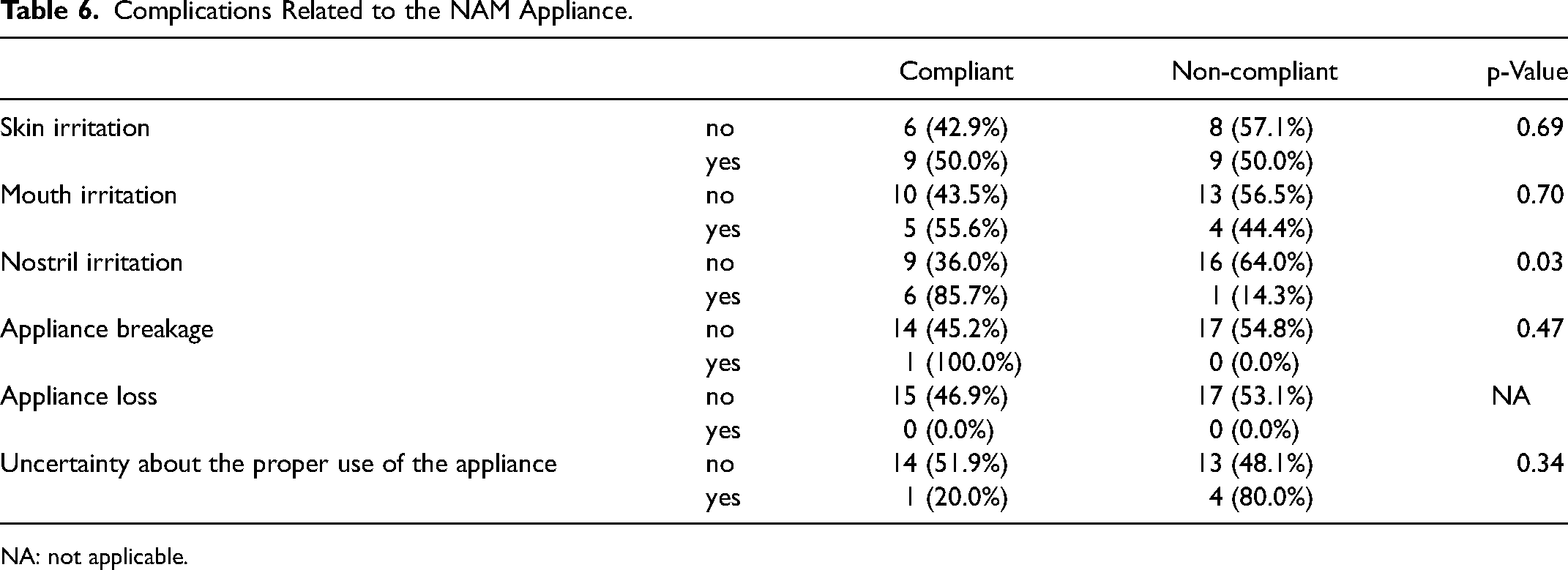
NA: not applicable.
Discussion
In the present study, parents of 35 infants with CL/CLP undergoing NAM treatment during the 2 years of the COVID-19 pandemic were asked about their anxiety and complications. Their commitment to treatment and its relationship with different variables were also considered.
The results indicated that the most H/VH level of anxiety of both mothers and fathers was the delay in treatment ends. Similarly, in a study conducted in the same center during COVID-19, prolongation of the treatment was the first concern reported by orthodontic patients. 30 Treatment outcome was the second cause of parents’ anxiety. Mothers’ low H/VH level of anxiety was the appliance breakage and impossibility of an emergency visit arrangement, which for fathers was not different from the anxiety of treatment outcome. Fathers had significantly lower anxiety levels for all the above issues than mothers. Several other studies reported higher stress, symptoms, and depression levels for mothers compared to fathers during the COVID-19 pandemic.31,32
The first anxiety issue of both parents related to visiting the clinic was the possibility of the child getting infected by COVID-19. The anxiety about getting infected may result in avoidance of attending the appointments. Other experiments also found a decline and delay in visiting the physician following the COVID-19 pandemic outbreak in patients with chronic diseases.33,34 However, Salas et al. stated that regular visits of infants (<1 year), unlike all other age groups, did not decline during the pandemic. 35 The second reason for the anxiety among mothers, was the parents’ infection. The higher anxiety reported for the child's infection rather than the parents’ infection may be due to the inability of the child to comply with health protocols such as wearing a mask. Unlike mothers, the second cause of the fathers’ anxiety was economic issues. It has been indicated that financial issues can affect patients with chronic diseases 36 and also the parents of children with chronic diseases during the COVID-19 pandemic. 37 Mothers’ anxiety about the safety of public transportation regarding COVID-19 infection was higher than fathers. The anxiety levels about the limitation of intercity and intra-city travel to the clinic were close to each other regardless of the place of residence, although with higher levels in mothers than fathers. It seems that less geographical accessibility won't necessarily result in higher anxiety. On the contrary, Yantzi et al. showed that distance to the hospital had a substantial impact on the family relationship of families with a child having a chronic disease. 38 Regardless of the effect of distance on anxiety and stress, considering the various challenges these parents face, any efforts for improving their situation are beneficial.
The two factors with a significant relationship with incompliance were the age of the patient and the history of Covid-19 infection of the parents or their relatives, according to multiple regression analysis. The parents of younger patients (age ≤28 days) showed more compliance, so their incompliance rate was 0.10 times that of older infants. Perhaps the higher compliance of these parents is because of better acceptance of the appliance by younger infants. It is not out of mind that younger infants can adapt and get used to the appliance more easily, while older patients may have more compliance problems. In the Levy-Bercowski et al. experiment, seven (26%) patients removed the appliance with their tongue and 3 (11%) with their hands. 23 In addition, as mentioned previously, the best time for NAM is the first weeks after birth. 18 It is also stated that maternal estrogen in infant cartilage during the first few weeks of birth helps maintain the high plasticity of cartilage, 39 which makes cartilage more amenable to molding. Therefore, the sooner the NAM treatment starts, the less incompliance, and superior treatment outcomes are expected. Amazingly, parents without a history of the COVID-19 infection of themselves or their relatives were 6.69 times more incompliant than parents with this history. Maybe those with a history of infection believe that they are less prone to re-infection and, therefore, were not so timid about attending the appointments. While in the study performed in the same center, no significant relationship was found between the history of COVID-19 infection and attending the appointments. 30 Another study represented higher avoidance, stress, anxiety, and so on for the infected healthcare workers compared to their non-infected peers. 40 Although no statistically significant differences were found between other variables and compliance, the following descriptive findings seemed logically correct. Highly educated mothers, fathers with higher economic status, and those who were less far from the clinic were more compliant, Tables 4 and 5. A larger sample size was probably required to report these relationships as significant.
Soft tissue irritation was the most prevalent complication of NAM in our patients. Skin irritation, mouth irritation, and nostril irritation occurred in 18 (54.55%), 9 (27.27%), and 7 (21.21%) of them, respectively. Nostril irritation resulted in diligently following the treatment, Table 6. This complication probably bothers the infant more and makes him/her restless. Similarly, Levy-Bercowski et al. observed soft tissue irritation in 20 (74%) and asymmetric arch in 2 (7%) of their patients undergoing NAM treatment. 23 Soft tissue irritation was the most common complication among the orthodontic patients of during COVID-19 pandemic. 30
We met some limitations in the current study. Firstly, our sample size was limited because of the low prevalence of the CL/CLP and also the number of patients referred to the clinic mentioned above during the COVID-19 pandemic. Multi-center studies are highly recommended to strengthen the findings and improve the generalizability of the results. We conducted a one-center study because of the differences in the treatment plans with other available cleft centers. Secondly, the duration of the study was limited to the pandemic span. Nevertheless, the findings of this study might be useful for clinicians to understand their patients’ needs in similar situations since COVID-19 won't be the last viral pandemic. Despite several powerful studies regarding the parents of children with CLP, 41 there is still a lack of conclusive evidence in this field. 42 Further studies are suggested to figure out the concerns and complications of the parents to help them cope with the child's situation and facilitate the condition for them to follow the treatment soon after the birth committedly.
Conclusion
The results of this study indicated that the most prevalent anxiety issue for the parents of infants with CL/CLP undergoing NAM during the pandemic was the delay in ending the NAM treatment. They were highly anxious about the infants getting infected while visiting the clinic. In general, mothers reported higher anxiety levels, while fathers were more worried about economic issues. The most prevalent complication of NAM treatment was soft tissue irritation. Parents with younger infants (age ≤28 days) and those with a history of infection were more compliant than their peers. Therefore, the findings of this study suggested the early onset of NAM is a positive factor in improving the parents’ compliance.
Footnotes
Acknowledgements
We would like to express our gratitude to Craniomaxillofacial Research Center for their support, as this study was funded and supported by Craniomaxillofacial Research Center of Tehran University of Medical Sciences (TUMS); Grant no: 1400–1–133–52430.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
The present study was approved by the research ethics committee of dental school of TUMS with the reference number of IR.TUMS.AMIRALAM.REC.1400.021.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Craniomaxillofacial Research Center of Tehran University of Medical Sciences, (grant number 1400-1-133-52430 )