
Abstract
Objective
To determine the association between prenatal care and cleft lip with or without cleft palate (CL ± P) and examine differences in newborn complications among infants diagnosed with CL ± P as a function of prenatal care
Design
Population-based retrospective cohort study
Setting
2018 United States National Vital Statistics System—Natality component (NVSS-N) was used to examine nationwide birth certificate data
Participants
3,414,338 infants from the 2018 National Vital Statistics System, of which 1,699 had CL ± P
Main Outcome Measure
Diagnosis of CL ± P and presence of newborn complications as a function of prenatal care
Results
Significant differences were found among various infant- and mother-specific variables when baseline comparisons were made between infants with and without CL ± P. After controlling for baseline differences, results indicated decreased odds of a diagnosis of CL ± P in cases where overall adequate prenatal care was obtained (OR = .841; 95% CI .757, .934), including prenatal care beginning in the 1st trimester (OR = .839; 95% CI .750, .939) and an adequate number of prenatal visits received (OR = .864; 95% CI .764, .976). Of infants with CL ± P, reduced odds of the infant admitted to the neonatal intensive care unit (OR = .777; 95% CI .613, .985) or transferred (OR = .601; 95% CI .407, .888) were apparent when adequate prenatal care was received.
Conclusion
Results suggest adequate prenatal care not only reduces the likelihood of CL ± P in infants but may also decrease the severity of negative outcomes in infants diagnosed with CL ± P. These findings emphasize necessity for adequate prenatal care.
Introduction
In the United States, cleft lip with or without cleft palate (CL ± P) is one of the most common birth defects, present in 1 of every 940 infants. 1 CL ± P occurs when there is a defect in the formation of the primary and/or secondary palate during embryonic development. Health outcomes of infants born with CL ± P usually involve multiple surgeries and potential issues with speech, feeding, dentition, and psychosocial wellbeing. Treatment for these concerns may place substantial social, emotional, and financial burdens on affected individuals and their families. Despite the relatively high prevalence and impact of CL ± P compared to other congenital anomalies, the specific cause of this condition is still unknown.
Research has demonstrated the etiology of oral clefts, along with the differences in prevalence across different races and ethnicities. Specific genes have been identified as increasing the risk of oral clefts in individuals. The genes identified included 1q32.2, 10q25.3, 17p13.1, 20q12, and 16p13.3. 2 Risk of CL ± P can also vary across different racial/ethnic groups. The lowest prevalence of oral clefts has been observed among populations derived from African descent from both inside and outside of the United States, 3 with the highest prevalence of oral clefts being observed among populations derived from Asian descent. 4 Further, lower rates of CL ± P and cleft palate only have been reported in children with non-Hispanic Black parents.4,5 Cleft palate only occurs at a lower rate amongst infants of Hispanic mothers and fathers when compared to infants of non-Hispanic White parents. 6 The cause of these differences across ethnicities and races is unknown, but possible contributors reported in the literature include access to quality healthcare or maternal health during pregnancy. 7
Many studies have supported the relationship between socioeconomic status and orofacial clefting. Lower socioeconomic status has been associated with an increased prevalence of oral clefts. The main factors of socioeconomic status that were associated with oral clefts were high poverty, low level of educational attainment, and increased material deprivation, such as the mother living in a neighborhood of low socioeconomic status or being unemployed.8–13 Conversely, some studies have demonstrated no connection between low socioeconomic status and increased prevalence of oral clefts, but rather a connection between maternal factors, such as cigarette or alcohol use, and increased prevalence of oral clefts.5,11,12 Therefore, there is a strong justification for investigating a possible connection between maternal socioeconomic status and the risk of infants being born with CL ± P. The health issues resulting from orofacial clefting may lead to a financial burden due to medical costs and potential decreased employability. As a result, poverty and lower socioeconomic status may continue and become further exacerbated, trapping families in a cycle of impoverishment.14,15
Other maternal factors have also been associated with CL ± P. The use of substances such as tobacco, alcohol, and anti-convulsants during pregnancy have been found to increase the risk of CL ± P. Nutritional deficiencies, such as low levels of folate or zinc, have also been linked to an increased risk of CL ± P or cleft palate only in infants.16–20 Additionally, maternal weight gain during pregnancy, body mass index, and the existence of health conditions such as pre-pregnancy or gestational diabetes, pre-pregnancy or gestational hypertension, or hypertension eclampsia may also be related to prevalence of oral clefts. 21 Factors such as these can affect a newborn's birth weight, maturity level, and the prevalence of birth defects.21,22 Although research has analyzed the effect of the aforementioned factors on infants in general, minimal investigation into the effects of these factors on infants born with CL ± P has occurred. One method of reducing the negative influence of these factors may be through prenatal care.
Prenatal care is an important factor related to the health outcomes of infants. Ideally, prenatal care begins in the first trimester and consists of 5 + visits to the maternal primary physician.23,24 Prenatal care also includes maintaining a healthy lifestyle, controlling existing health conditions, quitting smoking or the use of certain drugs, and not consuming alcohol. 23 Many of these components are not only beneficial to the mother, but are especially important to having a healthy pregnancy and giving birth to a healthy infant. 25 Research has demonstrated that increasing prenatal care measures positively impact the health outcomes of infants; conversely, inadequate prenatal care has been associated with an increased risk for preterm births, low infant birth weight, and CL ± P. 21 While there are surely numerous factors that contribute to whether or not a mother receives adequate prenatal care, research has shown that mothers with a higher education level tend to be more informed and have better access to adequate care and nutrition during pregnancy, which has been reported in the literature to be protective against CL ± P. 6 It is important to understand how socioeconomic status can affect access to healthcare, especially healthcare that affects mothers and infants, as prenatal care is essential healthcare for every expectant mother.
Across the United States, access to prenatal care has been associated with higher socioeconomic status and education level. Delays in prenatal care have also been associated with a diagnosis of CL ± P. 21 Therefore, several confounding variables known to impact the prevalence of CL ± P, such as maternal smoking, alcohol use, or even race, may also be responsible for impacting prenatal care. It is also unclear how adequacy of prenatal care impacts infants born with CL ± P, but it is known that delays in prenatal care can increase the risk of CL ± P. 21 The purpose of this study was to (1) determine the association between prenatal care and CL ± P while controlling for between-group differences, and (2) examine differences in the occurrence and type of newborn complications as a function of prenatal care among infants diagnosed with CL ± P. It was hypothesized that adequate prenatal care would be associated with reduced odds of CL ± P as well as reduced odds of complications at birth among those infants with CL ± P
Methods
Study Sample
The analysis used a deidentified, public access dataset. Institutional review board review was not required per institutional policy. Data from the 2018 US National Vital Statistics System—Natality component (NVSS-N) was used for this study, which is a publicly accessible database from the Centers for Disease Control and Prevention. 26 The vital statistics dataset contains data related to births, deaths, marriages, divorces, and deaths during pregnancy from all 50 states. 26 The NVSS publishes birth data online annually, which is titled Natality (N) and contains data from only births that occurred in the 50 states. The Natality online databases include paternal and maternal demographic characteristics, medical and public service utilization, maternal behavior and health characteristics, and infants’ health characteristics. 26 Participants of this study were infants born with and without CL ± P from the Natality database of the NVSS. It has been observed that CL ± P is more strongly linked to environmental factors, such as maternal health and socioeconomic factors, compared to cleft palate only.4,6 Thus, infants with cleft palate only were not included.
Sample Characteristics
The sample characteristics of mothers of infants with and without CL ± P were analyzed, which included the mothers’ age, race, nativity, education, payment method for delivery, weight gain during pregnancy, body mass index, prior smoking record, smoking record during pregnancy, and the presence of pre-pregnancy or gestational diabetes, pre-pregnancy or gestational hypertension, or hypertension eclampsia. Information regarding the month prenatal care began and the number of prenatal care visits attended was also included. The sample characteristics of the infants included their sex, birth weight, cleft-related diagnosis, APGAR score, and whether they had different congenital anomalies, a chromosomal disorder, and/or required assisted ventilation for over six hours. The APGAR (Appearance, Pulse, Grimace, Activity, and Respiration) score is a quick means by which doctors evaluate the health of an infant at 1 and 5 min post-birth and considers the infant's heart rate, respiratory effort, tonicity of muscles, reflex irritability, and skin color. 26
Overall Adequate Prenatal Care Measure
Overall adequate prenatal care was operationally defined in this study using values to represent both quantity (the total number of prenatal care visits received) and duration (the trimester at which visits began). According to the Kessner Index, inadequate prenatal care was defined as 0-4 visits, intermediate was defined as 5-8 visits, and any number of visits greater than 9 was considered adequate. 24 “Intermediate” and “adequate” levels of care were combined into one category to create a binary variable: Inadequate (0-4 visits) or not (5 + visits). Based off the month that prenatal care began, any care that began at or before the first trimester was considered adequate, with inadequate prenatal care beginning any time after the first trimester. 23
Data Analysis
Data were analyzed using chi-square tests of independence for the comparison of categorical variables and independent t-tests for the comparison of continuous variables. Binary logistic regressions were used to determine odds of presenting with CL ± P as a function of prenatal care and the odds of experiencing complications at birth among infants born with CL ± P as a function of overall adequate prenatal care. Odds of presenting with CL ± P as a function of prenatal care were generated using children without CL ± P as the reference group while controlling for while controlling for statistically significant maternal and infant characteristics (maternal: age, nation of birth, race, education, type of payment for delivery, weight gain, body mass index, cigarette use before pregnancy and in 1st trimester, pre-pregnancy and gestational diabetes, pre-pregnancy and gestational hypertension, hypertension eclampsia; infant: sex, birth weight). Odds of complicating conditions at birth among infants born with CL ± P were generated using infants born with CL ± P without overall adequate prenatal care as the reference group while also controlling for statistically significant maternal and infant characteristics (maternal: age, nation of birth, race, education, payment method for delivery, weight gain, body mass index, cigarette use in the 1st trimester, plurality; infant: birth weight). Severity outcomes were defined as the infant being born with CL ± P plus any reported newborn complication. These potential newborn complications, as reported by the NVSS-N, included: transfer of the infant after birth, admission to the neonatal intensive care unit (NICU), assisted ventilation immediately after birth, assisted ventilation within 6 hours of birth, lack of surfactant, use of antibiotics after birth, presence of seizures, and birth before 37 weeks (prematurity).
Results
Maternal and Infant Characteristics
Among the 3 414 338 infants in the NVSS-N, the 1699 infants diagnosed with CL ± P were comprised of significantly more males compared to the group of infants without CL ± P (62.3% vs. 50.9%, respectively), X2 (1, N = 3 414 338) = 88.14, P < .001. A significant difference was also present, X2 (3, N = 3 414 338) = 113.67, P < .001, in infant birth weight between infants born with and without CL ± P. Of the infants born with CL ± P, only 93.2% were born between 2500-8165 grams, while 97.2% of infants born without CL ± P were born within this range.
Table 1 presents the demographic characteristics of the population of mothers studied. The average age of the mothers in the sample differed significantly, t (3 414 336) = 2.10, P = .035, with the average age of mothers of infants with CL ± P being 28.67 years and the average age of mothers of infants without CL ± P being 28.97 years. Significant racial/ethnic differences were present, X2 (7, N = 3 414 338) = 107.46, P < .001, in the make-up of mothers of infants with and without CL ± P, for non-Hispanic White mothers (58.7% vs. 52.0%, respectively), non-Hispanic Black mothers (7.5% vs. 13.9%, respectively), and non-Hispanic Asian mothers (4.6% vs. 6.5%, respectively). Significant differences were present, X2 (4, N = 3 414 338) = 34.72, P < .001, in comparisons of education levels of mothers as a function of CL ± P, with a greater percentage of mothers of infants with CL ± P versus those without CL ± P not finishing high school (15.1% vs. 12.4%) and a lesser percentage of them having a bachelor's degree or higher (27.0% vs. 33.3%). The mothers’ nativity also differed significantly, X2 (2, N = 3 414 338) = 15.28, P < .001, with a greater percentage of mothers of infants with CL ± P being born in the United States (80.4%) as compared to mothers of infants without CL ± P (76.6%). The payment method for delivery also differed significantly, X2 (4, N = 3 414 338) = 30.39, P < .001, where a greater percentage of mothers of infants with CL ± P (47.7%) used Medicaid as the source of payment than mothers of infants without CL ± P (41.4%); fewer were labeled as private pay (44.3%) than mothers of infants without CL ± P (49.8%).
Demographics of Infants with and without CL ± P in the 2018 Natality Database.
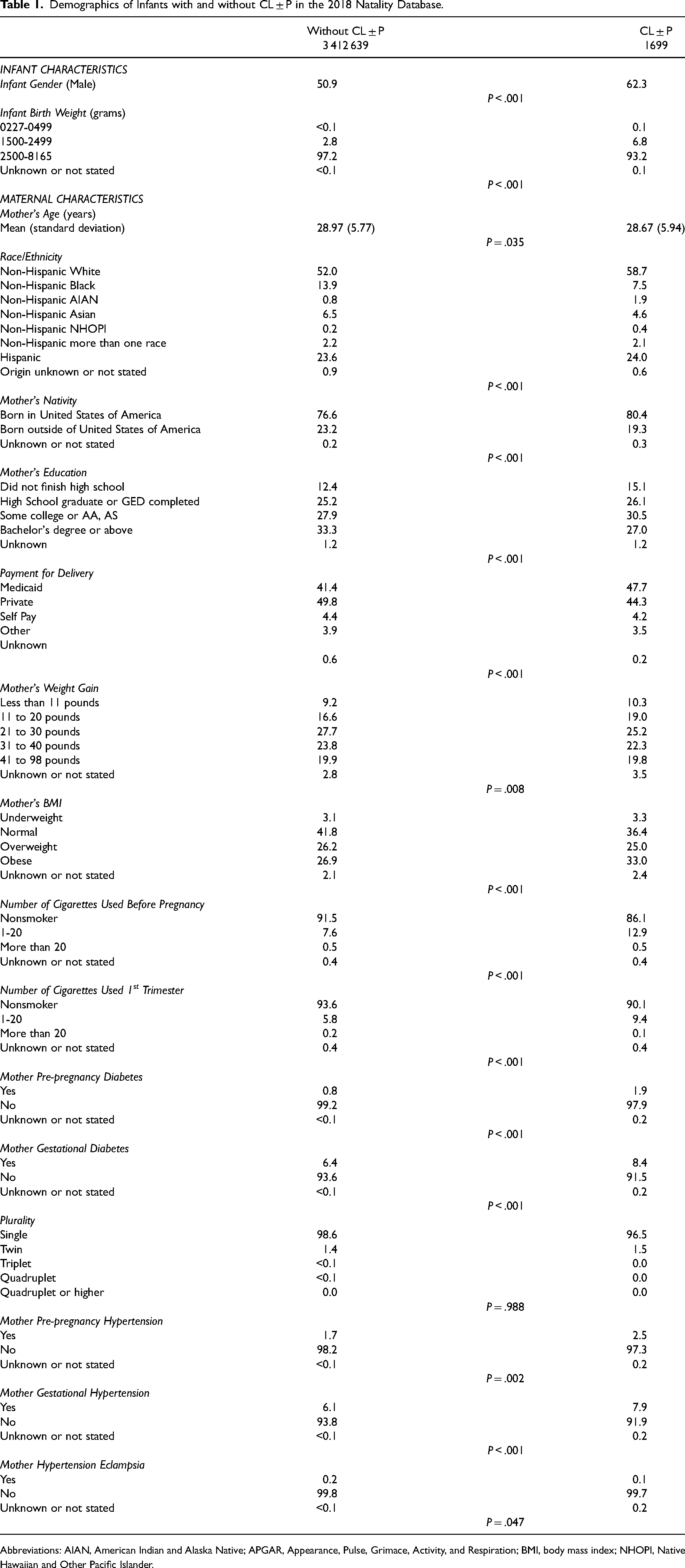
Abbreviations: AIAN, American Indian and Alaska Native; APGAR, Appearance, Pulse, Grimace, Activity, and Respiration; BMI, body mass index; NHOPI, Native Hawaiian and Other Pacific Islander.
Table 1 also presents health characteristics of mothers prior to and during pregnancy. The mothers’ pregnancy weight gain differed significantly, X2 (5, N = 3 414 338) = 15.73, P = .008, with 29.3% of mothers of infants with CL ± P gaining 20 pounds or less compared to 25.8% among of mothers of infants without CL ± P. Body mass index of the mothers differed significantly, X2 (4, N = 3 414 338) = 36.52, P < .001, with 36.4% of mothers with infants with CL ± P being classified as normal, compared to 41.8% of mothers with infants without CL ± P. Mothers of infants with CL ± P were significantly more likely, X2 (3, N = 3 414 338) = 70.19, P < .001, to have smoked 1-20 cigarettes prior to pregnancy (12.9%) when compared to mothers of infants without CL ± P (7.6%). Further, only 90.1% of mothers of infants with CL ± P abstained from cigarette use, while 93.6% of mothers of infants without CL ± P did not smoke at all during the 1st trimester of pregnancy; this difference was significant, X2 (3, N = 3 414 338) = 39.65, P < .001. Mothers with pre-pregnancy diabetes were significantly more likely, X2 (2, N = 3 414 338) = 34.67, P < .001, to give birth to an infant with CL ± P than an infant without CL ± P (1.9% vs. 0.8%, respectively). Mothers with gestational diabetes were also significantly more likely, X2 (2, N = 3 414 338) = 17.11, P < .001, to give birth to an infant with CL ± P (8.4%). For a complete breakdown of health characteristics of mothers prior to and during pregnancy, see Table 1.
Impact of Prenatal Care
The impact of prenatal care was analyzed using logistic models, with infants without CL ± P as the reference group and controlling for infant sex and birth weight, as well as maternal age, nation of birth, race, education, type of payment delivery, weight gain, body mass index, cigarette use before pregnancy and in the 1st trimester, pre-pregnancy and gestational diabetes, pre-pregnancy and gestational hypertension, and hypertension eclampsia. Mothers who received an adequate number of prenatal visits were at reduced odds of having an infant diagnosed with CL ± P (OR = .864; 95% CI .764, .976). That is, those with CL ± P tended to have a reduced number of prenatal care visits than what is clinically recommended. Mothers who began prenatal care within the first trimester were also at reduced odds of giving birth to an infant with CL ± P (OR = .839; 95% CI. 750, .939). That is, those with CL ± P tended to begin prenatal care visits later than what is clinically recommended. It is possible that mothers could have begun care in the 1st trimester but not have attended an adequate number of prenatal care visits; it is also possible that mothers could have attended an adequate number of prenatal care visits but began prenatal care after the 1st trimester. It was found that mothers who received overall adequate prenatal care, considering both the trimester at which prenatal care was initiated and the number of prenatal care visits attended, were also at reduced odds of giving birth to an infant with CL ± P (OR = .841; 95% CI .757, .934) (Table 2). In such, those with CL ± P tended to have reduced frequency and delayed timing of prenatal care visits compared to what is clinically recommended.
Measures of Odds Ratio Between the Presence of CL ± P in Infants and Variables Characterizing Prenatal Care, in the 2018 Natality Dataset.
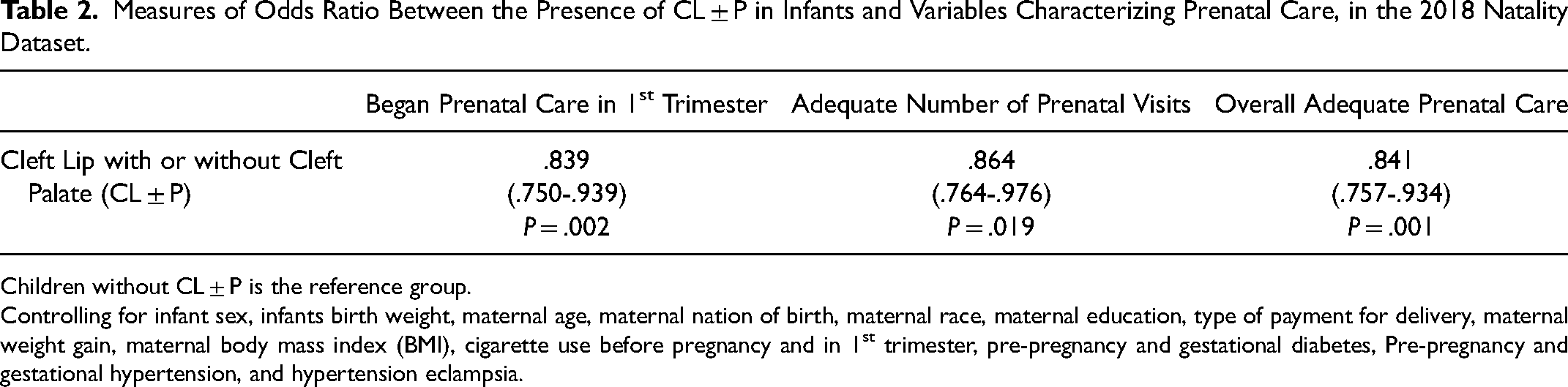
Children without CL ± P is the reference group.
Controlling for infant sex, infants birth weight, maternal age, maternal nation of birth, maternal race, maternal education, type of payment for delivery, maternal weight gain, maternal body mass index (BMI), cigarette use before pregnancy and in 1st trimester, pre-pregnancy and gestational diabetes, Pre-pregnancy and gestational hypertension, and hypertension eclampsia.
Multiple logistic regression analyses were used to examine the odds of newborn complications in infants born with CL ± P as a function of overall adequate/inadequate prenatal care. Using infants with CL ± P and without overall adequate prenatal care as the reference group, and controlling for baseline differences between the two groups, infants with CL ± P with overall adequate prenatal care were at reduced odds for being transferred within 24 hours (OR = .407; 95% CI .407, .888). Additionally, infants with CL ± P and overall adequate prenatal care were at reduced odds for being admitted to the NICU (OR = .777; 95% CI .613, .985) (Table 3). That is, those with CL ± P and inadequate prenatal care tended to be admitted to the NICU or transferred within 24 hours of birth.
Measures of Odds Ratio Between Overall Adequate Prenatal Care and Newborn Complications in Infants Born with CL ± P, in the 2018 Natality Dataset.
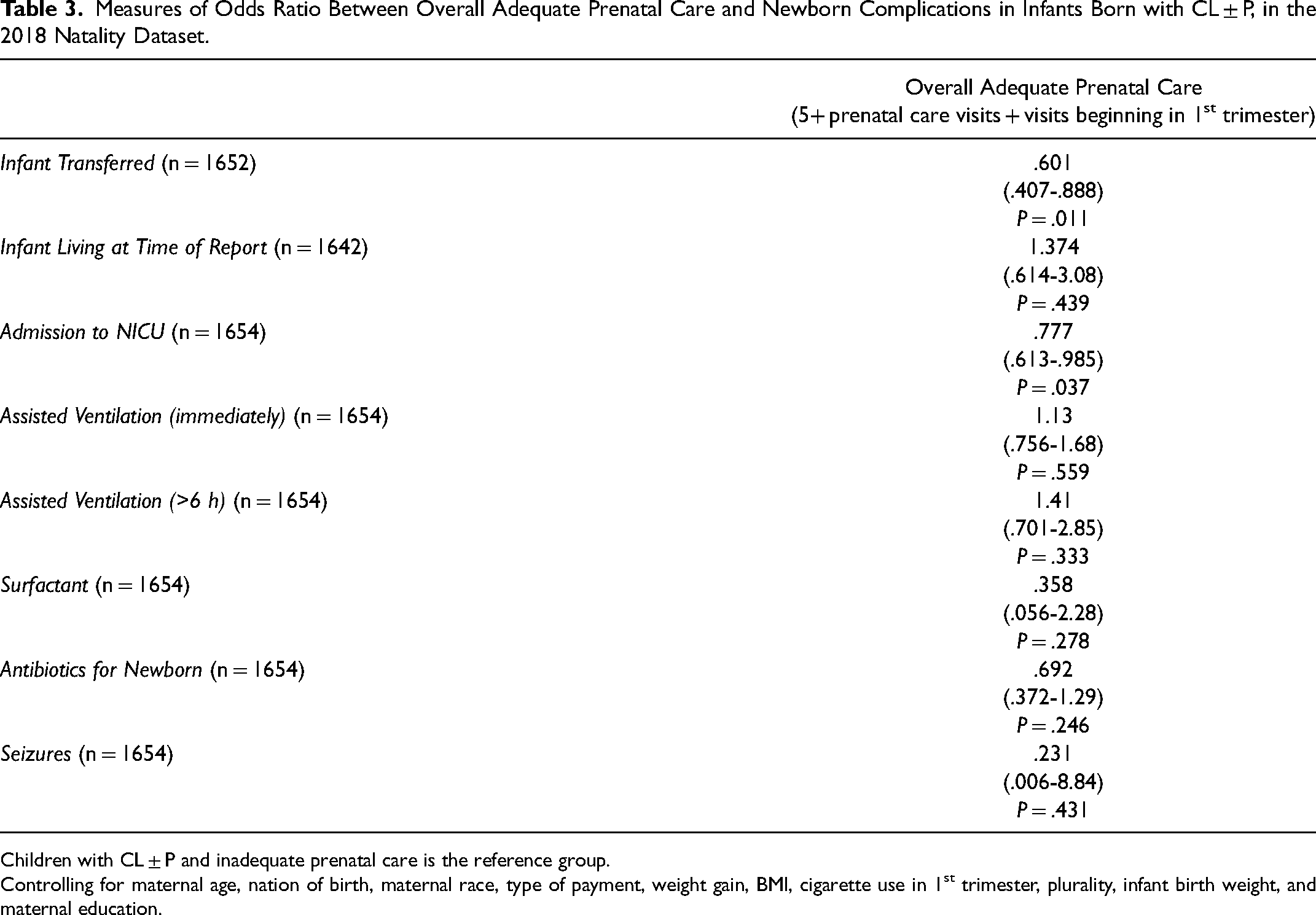
Children with CL ± P and inadequate prenatal care is the reference group.
Controlling for maternal age, nation of birth, maternal race, type of payment, weight gain, BMI, cigarette use in 1st trimester, plurality, infant birth weight, and maternal education.
Discussion
The purpose of this study was to determine the association between adequate prenatal care and CL ± P while controlling for between group differences and to conduct a preliminary examination of newborn complications among infants with CL ± P as a function of prenatal care adequacy. Based on current results, a relationship exists between reduced occurrences of CL ± P and adequate prenatal care as well as the related socioeconomic/demographic variables that may contribute to a mother receiving (or not receiving) adequate prenatal care. Along with this, overall adequate prenatal care was associated with reduced odds of admission to the NICU. The findings also suggested reduced odds of transfer within 24 hours of infants with overall adequate prenatal care and CL ± P compared to those with inadequate prenatal care and CL ± P. A summary can be viewed in Figure 1. This research supports the existing knowledge of the benefits of prenatal care on infant health outcomes and diagnosis of CL ± P.6,21 In cases of adequate prenatal care, interventions that may protect against transfer or admission to the NICU could be started, or at least discussed, prenatally.
An infographic summarizing the impact of adequate prenatal care.
Adequate prenatal care is any care that begins at or before the end of the first trimester. Along with this, any number of prenatal care visits greater than 5 is considered adequate with any number of visits below 4 considered inadequate.23,24 CL ± P has been linked to socioeconomic factors, specifically lower socioeconomic status and increased risk of an infant being born with CL ± P. 4 Those with lower socioeconomic status are also less likely to receive prenatal care. 27 Socioeconomic factors, such as lower education level and family income below the cutoff for poverty, have been linked with diagnosis of oral clefts. 10 Mothers of a lower education level may not be as informed of prenatal care guidelines or importance, and related financial constraints may inhibit access to healthcare services.
Results of the present study indicate a relationship between reduced occurrence of CL ± P and adequate prenatal care. Although intriguing, these results do not allow for assignment of causality, nor does it specify the mechanisms of change that bring about the finding of adequate prenatal care resulting in reduced odds of CL ± P or severity of outcomes within CL ± P. Thus, we cannot say that achieving a certain number of prenatal care visits and/or starting prenatal care within the first trimester is protective against a diagnosis of CL ± P or severe outcomes for individuals with CL ± P. However, as Raghavan and colleagues (2018) suggest, clinical guidance can still be offered in the absence of full understanding of risk factors. 28 Because those born with CL ± P tend to have been exposed to inadequate prenatal care, possibilities include advocating for folic acid supplementation29,30 and making families aware of environmental risk factors that have been associated with increased odds of CL ± P. 31 Additionally, infants with CL ± P who are born to mothers at risk for prenatal care disparities should be monitored more closely for requiring transfer within 24 hours and/or NICU admission. While current findings are certainly supportive of prenatal care, future studies are needed to unravel the relative contributions of various aspects of prenatal care and how they might defend against a diagnosis of CL ± P or more severe outcomes for those with CL ± P.
The literature has reported that mothers of infants with CL ± P were more likely to pay for delivery via Medicaid, suggesting that mothers with a lower income are more likely to give birth to an infant with CL ± P.32,33 Mothers who live in poverty may not have the financial means to pay for adequate prenatal care, including not only office visits but also prenatal vitamins, thus highlighting existing disparities and inequalities in our healthcare system. Additionally, nutritional deficiencies have been linked to increasing the risk of CL ± P due to their role in embryonic development. The presence of folate, B-6, and zinc have been shown to reduce the risk of CL ± P.11–13 Potential ways to address these disparities in obstetric healthcare could be increasing the number of programs and types of programs that provide education to expectant mothers of lower socioeconomic status, specifically with respect to prenatal care. Support of mothers from programs such as the Special Supplemental Program for Women, Infants, and Children (WIC), which is a program that supports low income mothers and infants that are at risk for health and nutritional problems, has been found to reduce rates of low and very low birth weight in infants, resulting in a decrease in neonatal mortality and morbidity. 34 By supporting women both educationally and financially, they may be more likely to seek and obtain adequate prenatal care, potentially decreasing the number and severity of congenital anomalies.
Women of poorer health are more likely to give birth to an infant with CL ± P. An important component of prenatal care includes monitoring maternal personal health, such as maintaining preexisting health conditions, abstaining from the use of cigarettes and alcohol, maintaining a healthy weight, and living an overall active lifestyle. 23 Our findings align with previous literature showing the association between maternal smoking during pregnancy and an increased risk of CL ± P.19,35,36 Additionally, our findings show increased odds of CL ± P with maternal smoking, specifically during the first trimester of pregnancy. This was also supported by the findings of Vu and colleagues. 6 Other maternal health risk factors, such as a less-than-average weight gain during pregnancy, maternal obesity, pre-pregnancy and gestational diabetes, pre-pregnancy and gestational hypertension, and hypertension eclampsia, were also related to increased risk of CL ± P. These findings were further consistent with prior research. 6 Although the mechanism behind this is unknown, prior literature has suggested that maternal health issues increasing the risk of CL ± P may be associated with differences in maternal metabolic and physiological processes due to those health issues.37,38 Future research should aim to compare the physiological and metabolic processes in healthy mothers and those in mothers with health issues to determine their impact on diagnosis of CL ± P in infants.
Along with the number of visits, the timely initiation of prenatal care was found to be important as well. Mothers who began prenatal care in the first trimester were found to be significantly less likely to give birth to an infant with CL ± P. When care begins in the first trimester, infants’ development is better supported by healthy habits of the mother along with essential nutrients for growth, and infants may be more likely to develop healthily. The primary and secondary palate, the areas affected by CL ± P, form between weeks 6-12 of pregnancy. 39 Since the first prenatal visit typically occurs between weeks 6-8 of pregnancy, it is unlikely changes made during or after this visit have any impact on reducing the likelihood of CL ± P. 23 However, it may be possible that mothers trying to conceive are already initiating certain prenatal care measures (eg, smoking cessation, prenatal vitamins) prior to becoming pregnant, resulting in reduced risk for CL ± P. Future research should explore differences in congenital anomalies among women trying to conceive versus unplanned pregnancy.
Our study also found that infants with CL ± P who received adequate prenatal care were significantly less likely to be admitted to the NICU or transferred within 24 hours. A diagnosis of CL ± P in and of itself is not typically life threatening. Admission to the NICU or transferring facilities may indicate that there are additional health concerns that extend beyond the diagnosis of CL ± P that could potentially be related to reduced prenatal care. Inadequate prenatal care visits may offer fewer opportunities to diagnose CL ± P prenatally, leaving the healthcare providers and family less prepared. Infants with CL ± P can usually feed sufficiently with a cleft-adapted bottle; however, if the cleft is found at the time of birth, the hospital may not have the knowledge or resources available to help the infant feed. 40 Admission to the NICU or transfer of the infant to a different facility can add undue stress to the infant and family and disrupt mother-infant bonding and attachment. Mothers can experience a high amount of grief, fear, and guilt associated with their infants’ health issues. 41 If newborn complications following birth can be reduced, the mental health of new mothers may be improved.
Limitations
While this study has many positive aspects, there are also limitations. First, this study only examined infants with CL ± P. Future research should consider infants born with cleft lip only or cleft palate only as well. This could help to see what aspects of prenatal care affect each clefting diagnosis the most. This study does not take into the account the severity of the clefting diagnosis (eg, unilateral, bilateral) and could be improved by considering the severity of the cleft while relating it back to the level of prenatal care received. This study is also limited to only live births as well as the severity outcomes of those infants prior to discharge from the hospital. Future studies could be improved by investigating the effect of prenatal care on the long-term health outcomes, including perinatal morbidity and mortality, of infants born with CL ± P. Future research is warranted to determine any impact of aborted pregnancies, as research has shown a relationship between reduced prenatal care visits and pregnancy termination. 42 Third, there is potential response bias from mothers reporting their level of care utilized along with factors such as alcohol and cigarette use. Mothers may have underreported aspects of care (such as substance use) due to the stigma surrounding these aspects. Lastly, with such a large database, it is important to practice caution when interpreting these results. While several significant associations have been reported in the present study, causation cannot be inferred from these results. There are also some statistically significant findings that are likely clinically insignificant (eg, maternal age difference).
Conclusion
The adequacy of prenatal care impacts infant health related to CL ± P. This study confirmed an increased odds of infants being born with CL ± P when mothers did not receive adequate prenatal care. Mothers of infants with CL ± P tended to begin prenatal care visits later and experience less frequent visits throughout pregnancy compared to current clinical recommendations. Findings also suggest that infants with CL ± P tend to experience reduced complications immediately post-birth when adequate prenatal care was received. Specifically, infants with CL ± P and inadequate prenatal care tended to be admitted to the NICU or transferred within 24 hours of birth. These findings highlight the need to increase education and access to adequate prenatal care, especially to those at risk based on maternal factors such as lower socioeconomic status. From a clinical standpoint, healthcare providers should continue to promote current prenatal care guidelines and help facilitate compliance for their patients. Further research is necessary to understand the underlying health conditions and physiological processes that affect early health outcomes of infants with CL ± P as well as prevent newborn complications within this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of General Medical Sciences, (grant number P20GM103432)
Research Ethics and Patient Consent
The analysis used a deidentified, public access dataset. Institutional review board review was not required per institutional policy.