
Abstract
Osteosarcomas arising within the pterygomaxillary/infratemporal fossa region are rare among the pediatric population. Survival rates are most influenced by tumor resection with negative margins, which can be dependent on surgical accessibility of the tumor site. The pterygomaxillary/infratemporal fossa location poses several challenges to safe and adequate tumor resection, including proximity of the facial nerve and great vessels and scarring associated with traditional transfacial approaches. In this article, we present the case of a 6-year-old boy with an osteosarcoma of the left pterygomaxillary/infratemporal fossa region successfully managed with an “oncoplastic” approach, incorporating the use of CAD/CAM and mixed reality technologies.
Keywords
Introduction
Head and neck osteosarcoma comprises approximately 8% of pediatric and adolescent osteosarcomas overall.1–7 Among children and adolescents, osteosarcoma has a mean age of diagnosis of 9–11 years and a peak age incidence of 10–19 years, coinciding with pubertal growth onset and growth spurts.3–5,8,9 When osteosarcoma arises in the head and neck, the mean age of presentation is approximately 10–15 years higher than osteosarcoma of other bones in the body and tends to have a male, Black, and Hispanic predominance.3,5,9 The mandible and maxilla are the most common sites for facial lesions.2,5,7,8,10,11 Osteosarcomas rarely arise within the pterygomaxillary region/infratemporal fossa.12–14 When involving the mandible and maxilla, the main symptoms of osteosarcoma are pain, swelling, and ulceration. 5 Pain is typically attributable to compression of adjacent nerves or periosteal impingement. 2
Predisposing factors for osteosarcoma include prior exposure to ionizing radiation, tumor suppressor gene mutations, helicase family gene defects, Paget's disease, and fibrous dysplasia.1,5,6,9,11,15 Exposure to several chemical substances has also been linked to formation of osteosarcoma.1,9 The 5-year relative survival rate after diagnosis with osteosarcoma is approximately 68%, though this decreases with increasing age at diagnosis.1,3,5 Osteosarcoma of the facial bones tends to have a lower risk of distant metastases, but a higher risk of local recurrence post-surgical resection.10,16
Treatment of osteosarcoma requires a multidisciplinary approach.4,8,13,14 Conventional treatment typically consists of neoadjuvant and adjuvant chemotherapy following surgical resection.1,3,15 While chemotherapy regimens are attributed to increased survival rates, the mainstay of treatment is complete surgical resection. 8 Survival rates are primarily increased by negative margins after surgical resection, though staging, size, metastases, local recurrence, and percentage of tumor cells destroyed after neoadjuvant chemotherapy are also significant factors.1–3,8,15 Tumor site is a proposed contributor to survival, as tumor accessibility contributes to surgical outcomes.3,11,13 Tumors within the pterygomaxillary recess/infratemporal fossa are difficult to access surgically, and resection may be associated with significant risks, including facial nerve injury and extensive scarring from transfacial incisional approaches.13,14,17 Detailed planning is needed to ensure maximization of function and minimization of morbidity with surgical treatment. Optimization of cosmesis is also of importance in young, growing children.
In this report, we present the case of a 6-year-old male patient with a primary osteosarcoma of the left pterygomaxillary/infratemporal fossa region and introduce the concept of an “oncoplastic” approach to resection. While “oncoplastic” approaches have been described in other anatomic regions for soft tissue surgery (e.g., breast cancer surgery), analogous approaches in craniomaxillofacial surgery have heretofore not been emphasized.18–20 The current case also represents an example of the incorporation of mixed reality and computer-aided design/computer-aided manufacturing (CAD/CAM) technologies in the planning of pterygomaxillary tumor resection and reconstruction.
Case
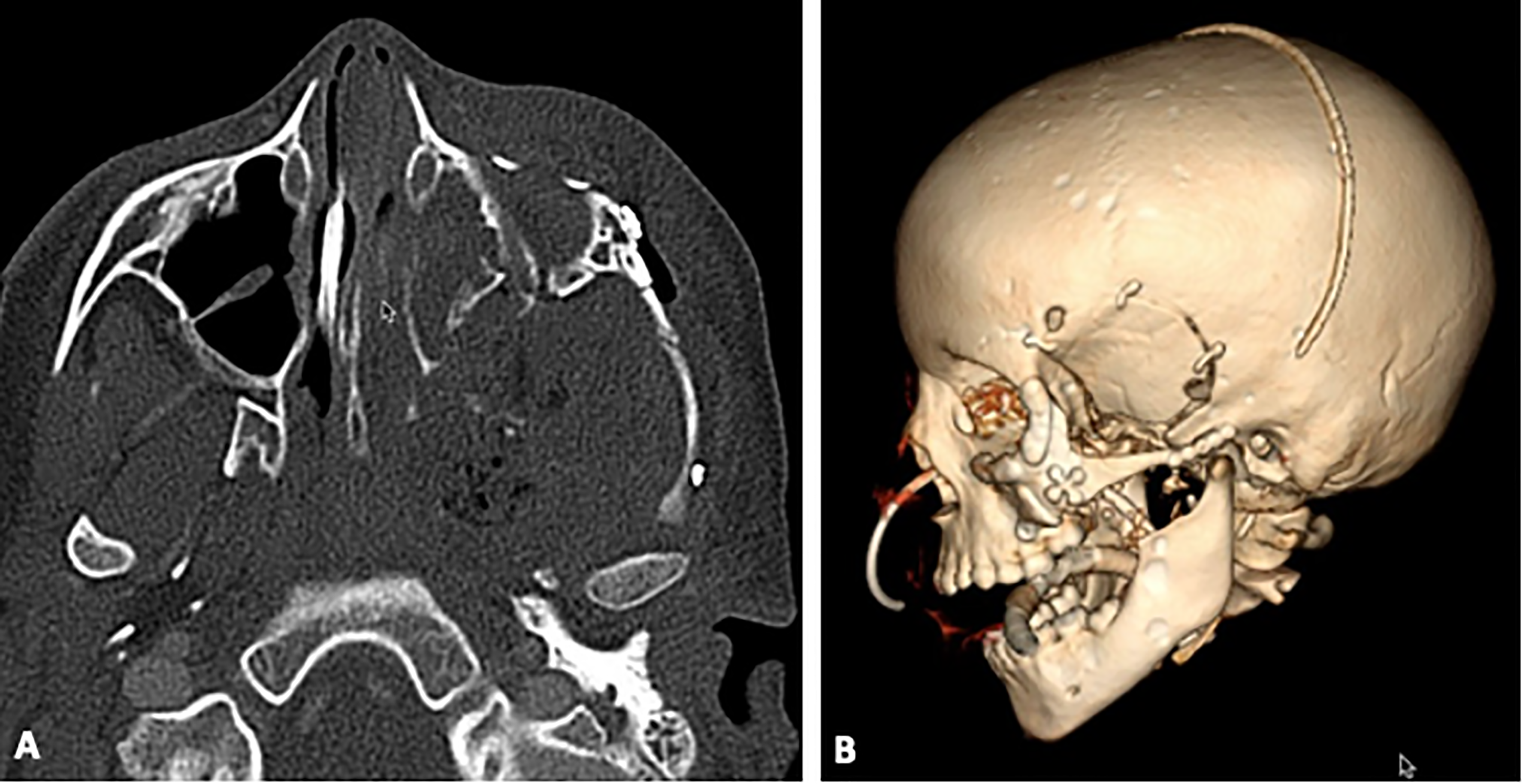
A 6-year-old male with no significant past medical history presented to our hospital with a 1-month history of left temporomandibular joint and masticatory pain, unrelieved with non-steroidal anti-inflammatory medications. Imaging of the facial bones in our Emergency Department demonstrated a heterogeneously enhancing large mass with a sunburst-type aggressive periosteal reaction measuring 4.1 × 4.7 cm (Figure 1). The mass was located at the left pterygoid plate/maxillary tuberosity and extended to involve the left zygomatic arch and skull base of the infratemporal fossa. The mass was biopsied through a nasopharyngeal endoscopic approach, and a diagnosis of primary osteosarcoma was made. A whole-body PET CT further characterized the tumor as an intensely hypermetabolic and aggressive left parapharyngeal mass extending to the infratemporal fossa. Oncology was consulted, and neoadjuvant chemotherapy consisting of doxorubicin, cisplatin, methotrexate, and leucovorin was administered in 2 cycles, each lasting 5 weeks. This was transitioned to a regimen of ifosfamide, etoposide, and MESNA for two cycles, each lasting 4 weeks. Following completion of neoadjuvant chemotherapy, repeat imaging was obtained, showing a significant reduction in tumor size on CT to 3.7 × 2.8 × 3.3 cm. PET CT also showed an improvement, with the tumor now featuring low-level hypermetabolic activity. Clinically, the patient had no symptoms other than chemotherapy-induced weight loss. Preoperative workup was normal except for anemia.
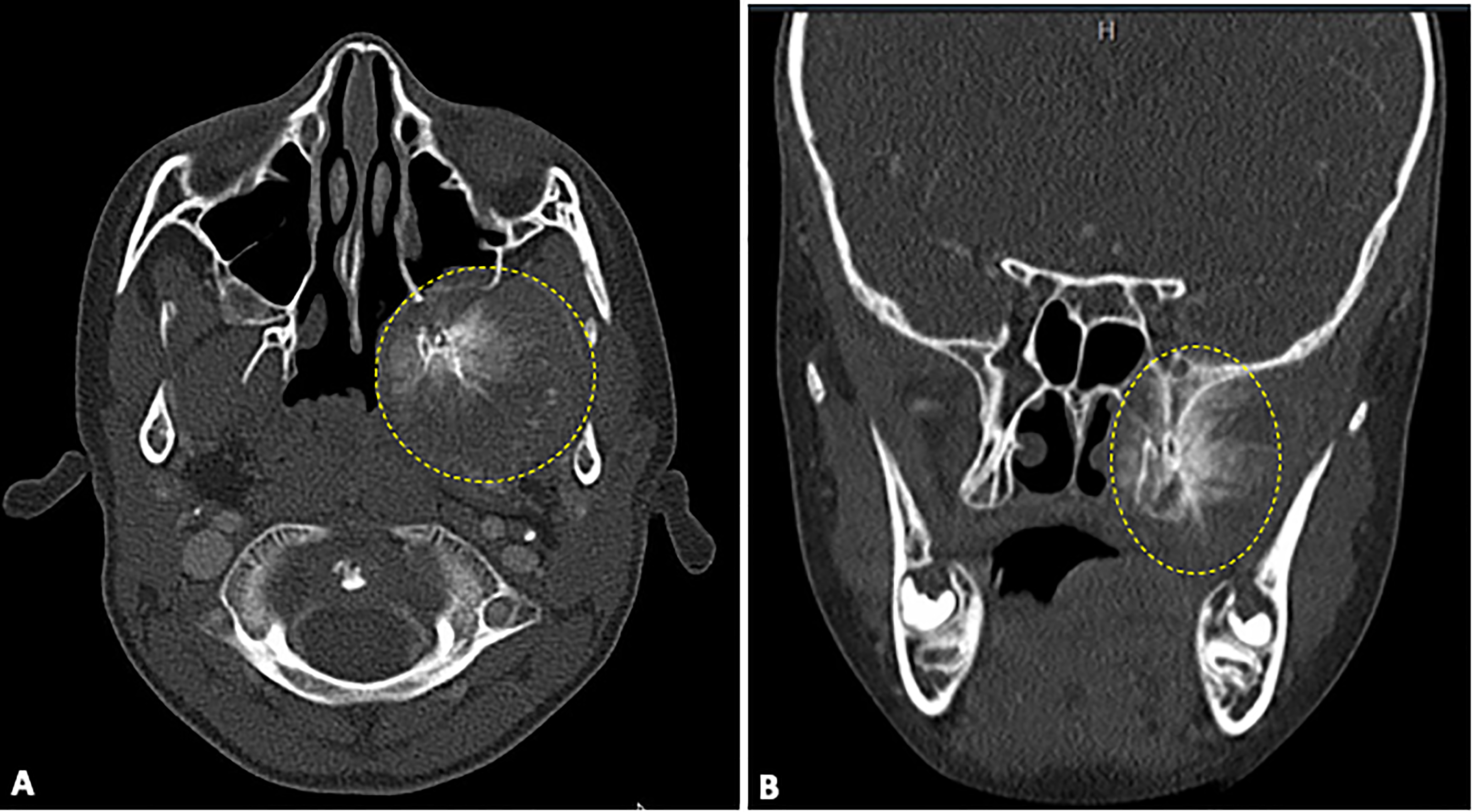
Axial (A) and coronal plane (B) CT images of pterygomaxillary/infratemporal fossa tumor prior to chemotherapy, with dotted lines denoting areas of involvement.
Surgical consultations were now obtained for resection of the mass. An opinion was rendered at an outside institution for an open Weber-Ferguson transfacial incision and left hemi-maxillectomy to approach the pterygomaxillary/infratemporal fossa. No plans were made for neurosurgical consultation with this approach, and the family was informed that the mass would be inoperable with frank involvement of the cranial base. At our institution, an alternative, multi-disciplinary approach involving Neurosurgery and Plastic Surgery was formulated for temporal craniotomy and skull base tumor resection from above, aided by osteotomies to remove the zygomatic arch. In addition, osteotomy of the zygoma and resection through a maxillary intraoral vestibular approach, as well as osteotomy of the coronoid process and resection through a mandibular intraoral vestibular approach, was proposed. These approaches were favored to allow maximal tumor resection through a cosmetically advantageous bicoronal scalp incision and hidden intraoral incisions, while at the same time allowing for reconstruction of the facial skeleton with minimal disfigurement and no disruption of the dentition. Mixed reality was utilized in the multi-disciplinary team's planning approach to map out the full three-dimensional extent of the tumor and its proximity to critical anatomic structures such as the great vessels and skull base, as well as to explain the procedure in detail to the patient and his family (Figure 2).
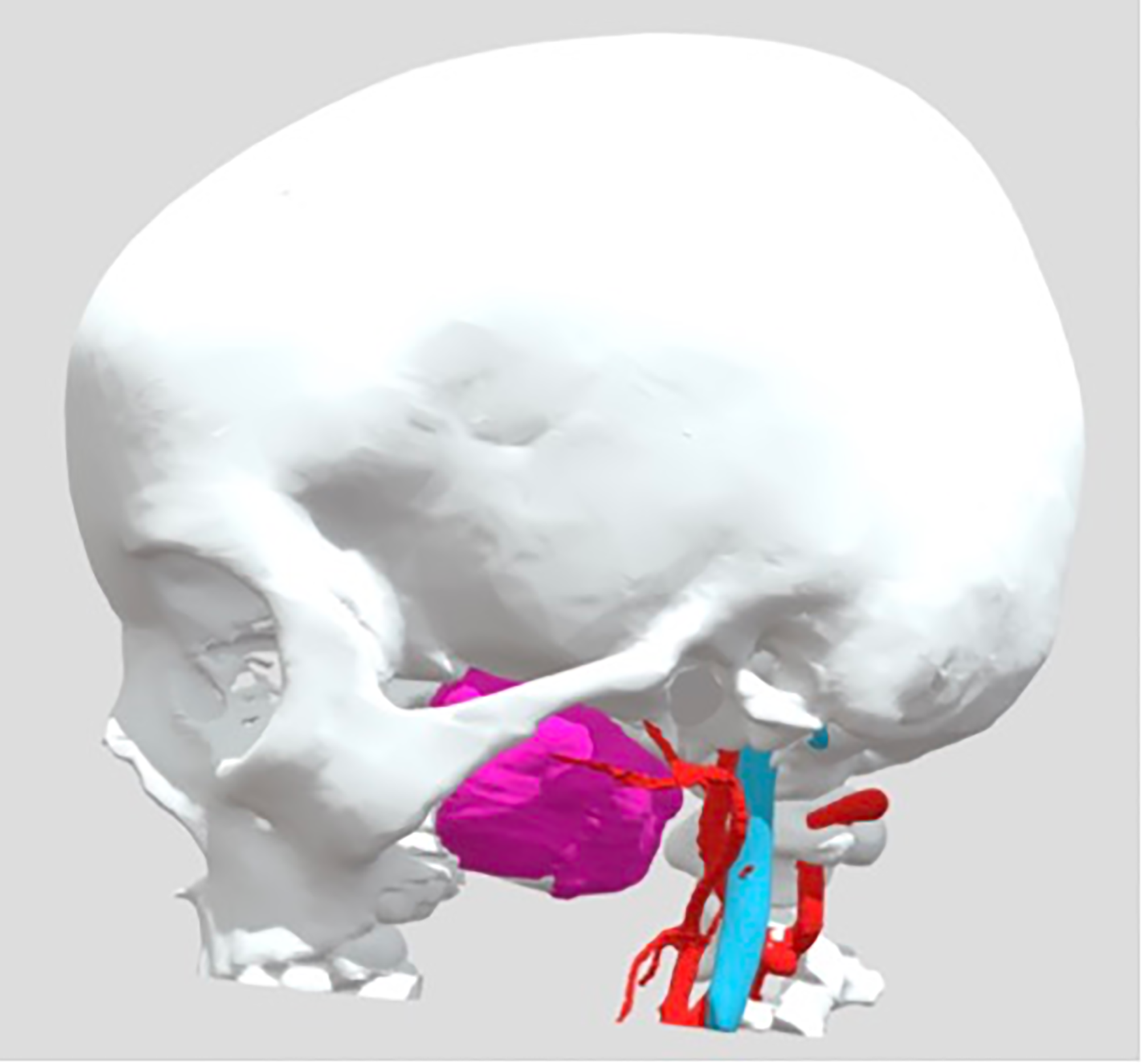
Demonstration of 3D modeling of tumor (pink mass), which was fabricated as handheld model for surgical discussion and also incorporated digitally into mixed reality planning for discussion and manipulation in 3D space. Note proximity to skull base and great vessels.
Prior to the day of surgery, virtual planning was again employed to create customized cutting guides for the zygomatic osteotomies as well as customized titanium reconstruction plates for precise anatomic alignment of the bones after tumor resection (Figure 3). Submental intubation was performed on the day of surgery to facilitate the craniotomy and intraoral approaches. A left subtarsal incision was also utilized to provide additional access to the zygoma. Following resection of the upper third of the tumor via a temporal craniotomy and zygomatic arch osteotomy, the middle third was approached via zygomatic body osteotomies through a maxillary vestibular incision. The remainder of the tumor (i.e., inferior third) was removed following coronoidectomy with an extended mandibular vestibular incision intraorally (Figure 4). The tumor appeared as a spiculated dense, woody mass amenable to piecemeal resection. The zygomatic body and arch were reduced and fixated back according to the preoperative planning. Stock titanium plates were used to re-fixate the zygomatic arch to the temporal articulation, however the zygomatic body was most accurately readapted through the use of custom guides, pre-drilled holes, and custom hardware, avoiding rotational deformity and facial asymmetry. The patient was extubated successfully at the conclusion of surgery. Post-operative CT scanning demonstrated clearance of the great majority of the tumor, with only focal scattered radiodense spicules (Figure 5). Pathology revealed a 98% chemotherapy-related tumor treatment effect.
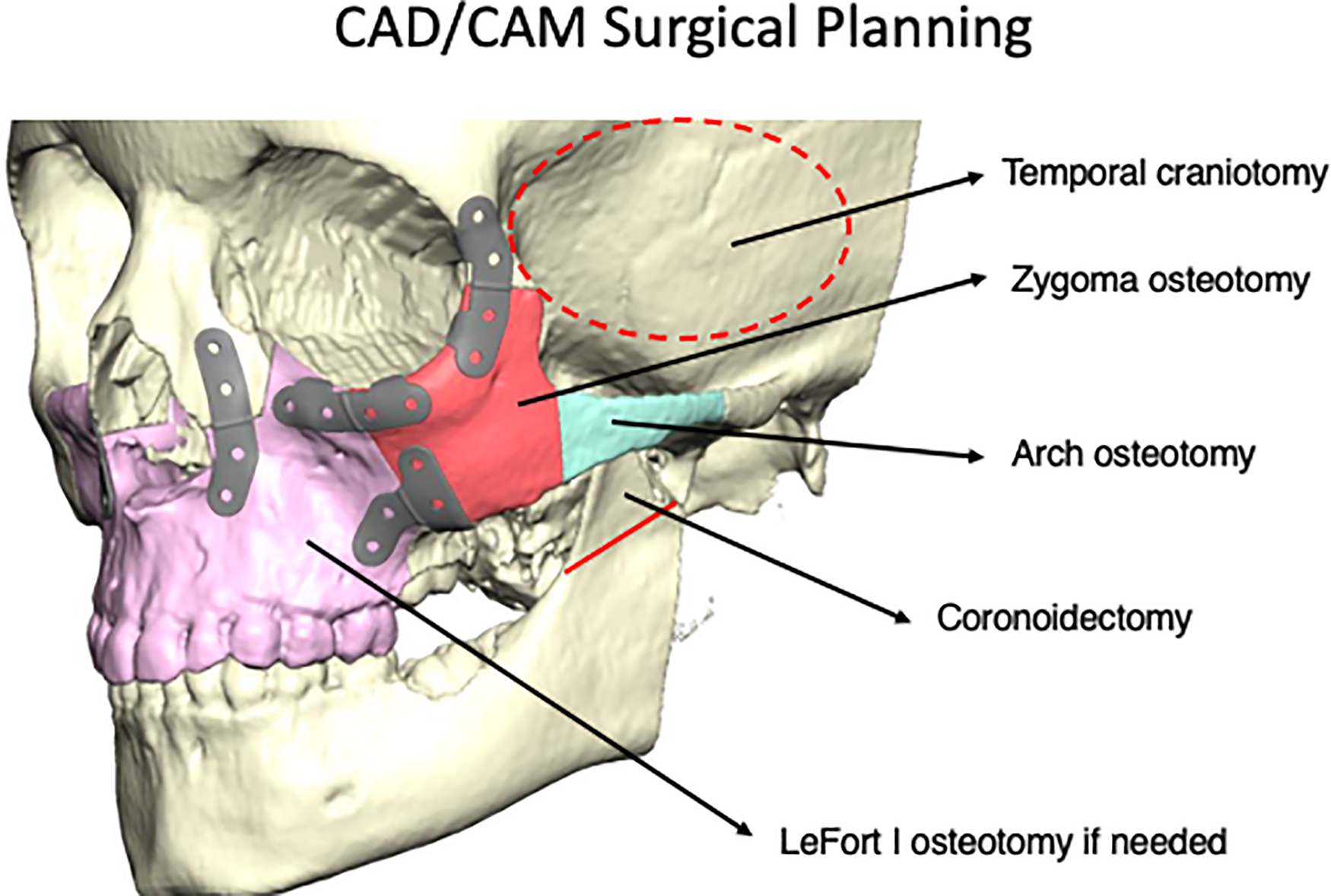
CAD/CAM planning and production of customized fixation. Planning included: (1) temporal craniotomy; (2) zygomatic arch osteotomy; (3) zygomatic body osteotomy; (4) mandibular coronoidectomy; and (5) LeFort I osteotomy if needed. In this case, complete tumor resection was feasible without the need for LeFort I osteotomy.
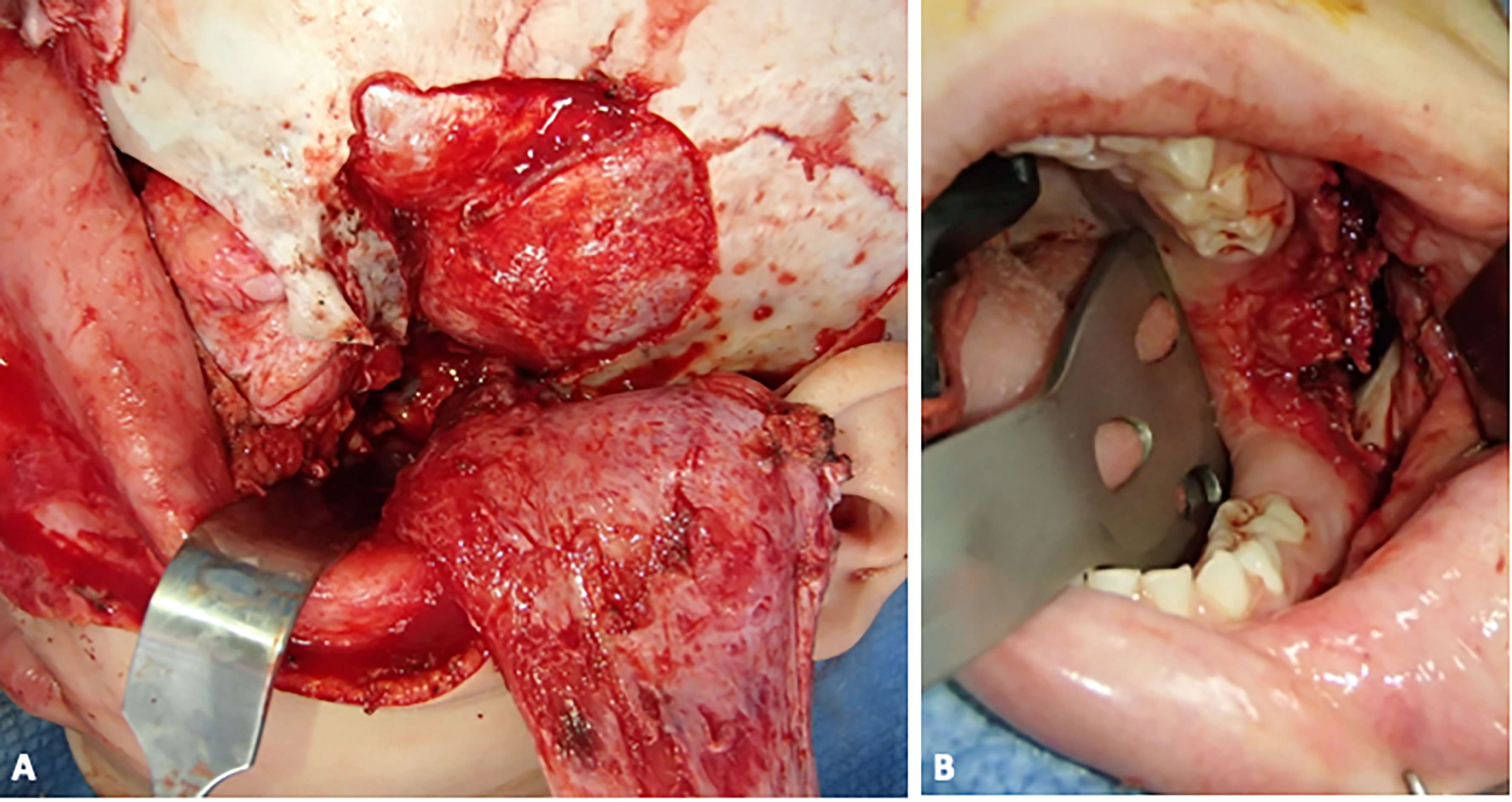
(A) intraoperative photo showing temporal craniotomy, retracted temporalis muscle/pericranial flap, and access to the infratemporal fossa after osteotomy of the zygoma and arch; (B) intraoperative photo showing intraoral mandibular vestibular approach, facilitated by coronoidectomy.
(A) axial postoperative CT image demonstrating clearance of tumor; (B) postoperative 3D CT reconstruction showing re-plated zygoma, arch, and temporal bone.
The patient did well postoperatively and experienced no major complications. Minor complications included temporary limitation in mouth range of opening, which has improved over time with physiotherapy, and left frontal branch weakness, which has nearly full resolved. Facial cosmesis is excellent, and occlusion is undisturbed (Figure 6). Four weeks postoperatively, the patient started adjuvant chemotherapy with doxorubicin, ifosfamide, MESNA, methotrexate, and leucovorin. He has now completed chemotherapy as well as adjuvant radiation therapy and, at the present time, has no evidence of active disease.

Four month postoperative facial and occlusal photographs of patient.
Discussion
Osteosarcoma is a lesion that most typically develops in the metaphysis of long bones, though it can develop in any bone of the body.1–3,8,9,15,16 With an annual incidence of 5.6 cases per million children under the age of 15, it is typically locally destructive and has a high recurrence rate.4,8,15 Primary lesions in the head and neck region are relatively infrequent, and particularly rare within the pterygomaxillary recess/infratemporal fossa.1–4,8,16 The infratemporal fossa is a region bordered by the maxillary sinus anteriorly, the temporal and sphenoid bones superiorly, the ascending ramus of the mandible and the temporalis muscle laterally, the lateral pterygoid plate medially, and by a horizontal plane defined by the inferior border of the mandibular angle inferiorly.12–14 Several important neurovascular structures traverse this space, including the maxillary and mandibular branches of the trigeminal nerve.12,13 Adjacent to this area is the internal carotid artery. 12 Historically, tumors located within the infratemporal fossa have proven challenging to resect.12,13 Concern arises from potential damage not only to structures within the fossa, but also to structures situated along the approach to the fossa. Surgical complications have been reported to occur between 17% and 64% of the time, and include morbidity to the facial nerve.4,13,14,17 Mortality amongst the approaches has been estimated at 8%.13,14 Precise planning for tumors in the pterygomaxillary/infratemporal fossa region is therefore paramount to maximize safety and cosmesis as well as to minimize morbidity.
In the present case, we elected for a surgical approach that would enable complete resection of tumor from the pterygomaxillary/infratemporal fossa region while allowing for aesthetically favorable reconstruction and avoidance of extensive transfacial scarring. Such an approach may be categorized as “oncoplastic,” signifying that traditional reconstructive principles are blended with oncologic aims to enable a therapeutic, yet structure-preserving, outcome. 18 Though the term has traditionally been associated with oncologic and reconstructive breast surgery, this approach can also be applied to craniomaxillofacial tumor surgeries.18,19 For such cases, techniques may be borrowed from craniomaxillofacial trauma reconstruction or from reconstructive approaches to congenital deformities. We have previously reported on the latter in a complex case of central giant cell granuloma of the mandible in a 3 year-old child, in which a costochondral graft was utilized in a similar manner to its well described role in hemifacial microsomia. 20 For our 6 year-old patient in this report, the oncoplastic approach involved separate osteotomies of the zygomatic body and arch via typical incisions employed in trauma cases (e.g., bicoronal incision, subtarsal incision, and intraoral maxillary vestibular incision). Corodonidectomy was also performed via an intraoral mandibular vestibular incision to access the inferior portion of the tumor with the mouth maximally propped open, akin to what would be performed for a case of pediatric temporomandibular joint ankylosis. 21
Success in the present case was facilitated not only through the use of an oncoplastic approach, but also through the incorporation of mixed reality and CAD/CAM technologies. Virtual planning and CAD/CAM cutting guides and customized plates continue to be used in many craniomaxillofacial applications, including complex panfacial trauma, cranial vault remodeling surgery, orthognathic surgery, and oncologic head and neck reconstructive surgery.22–27 Benefits are wide-ranging, and include improved accuracy of reduction in trauma cases, improved predictability in cranial surgery, reduced preoperative planning time in jaw surgery, and precision composite tissue restoration in oncologic surgery.23,24,28,29 Operative time may also be reduced with the incorporation of customized technologies, as may cost if fewer subsequent revisions are needed due to the superiority/accuracy of the initial result. When osteotomies are performed, as in this case, primarily for exposure, intraoperative bending of stock plates on the preoperative anatomy is certainly an alternative strategy. While this may help reduce costs, the ability to minimize rotational deformities when multiple degrees of freedom exist is a distinct advantage (e.g., when both the zygomatic body and arch have been independently disassembled). As with the malreduction of zygomatic fractures, subtle rotational deformities can result in malar underprojection and appreciable facial asymmetry. Customized hardware can minimize these tendencies and also obviate the need for intraoperative CT scanning in the periorbital region.
Mixed reality is another adjunctive technology that is increasingly being employed in craniomaxillofacial surgery for training, patient/family education, and surgeon preparation.25–27,30–33 The technology allows for depth perception and better visualization of structures including the complicated shapes found in the craniomaxillofacial skeleton. As with the incorporation of CAD/CAM technology, the introduction of mixed reality has been suggested to reduce operative time, reduce complications, and facilitate more aesthetic outcomes.22,23,28,29 In tumor cases, another invaluable aspect of mixed reality is the ability to more precisely pinpoint the proximity of the mass to critical anatomic structures such as the skull base and great vessels. Furthermore, the technology could allow one to simulate pre-operatively which portions of the tumor are amenable to resection through which approaches (e.g., the hard-to-reach inferior “tail” of the current mass through an intraoral mandibular vestibular approach and coronoidectomy. Mixed reality can, quite literally, add another dimension of planning beyond the typical two-dimensional “tumble” and “spin” sequences available on most hospital radiographic imaging systems. Finally, should a portion of tumor be left behind with an oncoplastic approach compared with a traditional transfacial approach, mixed reality technologies could serve a further advantage in highlighting the most direct path to the remaining mass.
It is important to note that, unlike in adults, pediatric tumors of the head and neck region do not fall neatly within the purview of any single surgical specialty. Traditional approaches such maxillectomy or hemi-maxillectomy may engender significant morbidity for the growing child, in whom free microsurgical tissue transfer may be technically more complex, and in whom results over time may be less predictable with growth. Nutritional consequences with the loss of the maxillary dentition may be a particularly adverse consequence as well. From a psychological point of view, extensive transfacial scarring may also negatively impact quality of life. As the frequency of particular subtypes of pediatric sarcoma or other tumors amenable to surgical treatment continues to be delineated, a more extensive cataloguing of oncoplastic techniques in the craniomaxillofacial region will be of particular benefit.
Conclusion
Osteosarcoma of the pterygomaxillary region/infratemporal fossa in pediatric patients is an exceedingly rare diagnosis, and surgical treatment is challenging. While chemotherapy has increasingly improved outcomes, surgery remains a mainstay of osteosarcoma treatment. We have described an oncoplastic approach to surgical management to minimize morbidity, preserve function, and maximize cosmesis. The approach incorporates the use of techniques from congenital and trauma reconstructive surgery in the craniomaxillofacial skeleton. CAD/CAM and mixed reality technologies has further increased the reliability of surgery for such tumors, and represents an advance not only for medical practitioner, but for the patient and family in terms of promoting greater understanding and participation in the process.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article