
Abstract
Objective
This study investigates the effectiveness of demineralized bone matrix (DBX) to close alveolar clefts in patients previously treated with bone morphogenic protein-2 (BMP-2) who remained with bone nonunion.
Design
This is an IRB-approved retrospective, single-center study.
Setting
This study was conducted at a tertiary academic center
Patients/Participants
We searched for all surgical encounters with the Current Procedural Terminology (CPT) code 42210 from the years 2013–2019. Included patients were diagnosed with cleft alveolus, previous BMP-2 exposure and required revision bone grafting during mixed dentition for persistent alveolar defects.
Interventions
17 patients underwent revision alveolar bone grafting (ABG) with either DBX (n = 10) or autograft (n = 7) to repair persistent bony cleft.
Main Outcome Measure(s)
The primary study outcome measured was alveolar bone graft revision failure described as continued alveolar nonunion.
Results
The median age at revision ABG was 13.1 ± 3.3 years, with a mean follow-up time of 4.9 years (1.1–9.2 years). Patients were 53% male, 47% had a unilateral cleft lip and alveolus. 58.8% of patients were treated with DBX in the cleft, 41.2% treated with autograft from iliac crest. Overall, 11.8% (n = 2) of all revisions failed, requiring a second revision. The average time to reoperation was 2.06 years, and both were re-grafted with autograft. There was no statistically significant difference between the type of bone graft source used and the failure rate obtained (P = .1544).
Conclusions
DBX and autologous iliac crest bone grafts achieve similar alveolar union rates during revision ABG in patients treated with previous BMP-2 to the alveolar cleft.
Introduction
Orofacial clefts are among the most common surgical congenital defects, occurring in 1 out of every 630 births. 1 In addition to affecting the lip and palate, orofacial clefts often extend into the alveolus, requiring a separate reconstruction. The gold standard of alveolar reconstruction is iliac crest bone grafting, performed when the patient is in mixed dentition. 2 However, iliac crest bone graft is associated with donor site morbidity, including pain, potential difficulty ambulating, widened scar, infection or hematoma and nerve damage.3,4
Donor site morbidity has prompted the search for bone graft substitutes, most notably demineralized bone matrix (DBM). DBM is a form of allograft derived from cadaveric bone, treated with acid to remove mineral components while retaining its osteoconductive and osteo-inductive potential. 5 DBX (manufactured by Medtronic) is a DBM product mixed with hyaluronic acid as a viscous carrier. Surgeons have used DBX to promote osteogenesis and repair bone defects. 5 Well-known applications include the closure of orthopedic bony defects and spinal fusion in adults. Newer applications, however, show promise for use in children with orofacial clefts; DBX has been found to be a non-inferior alternative to autologous bone grafting for secondary alveolar bone grafting in cases where autologous primary grafting has failed. 6 This application is significant since up to 32% of patients with alveolar clefting may require secondary revision. 3
Given these promising results, we sought to investigate the use of DBX in patients previously treated with bone morphogenetic protein-2 (BMP-2) to their alveolar cleft with continued bony defect. Bone morphogenetic proteins (BMP) are naturally occurring osteogenic proteins in bone, essential to bone healing and remodeling. 6 BMP-2 is the most widely studied agent for craniofacial applications 7 including alveolar cleft repair,8,9 and some surgeons expanded its use off-label to attempt “graft-less” repair in pediatric patients8,10–12 However, widespread use of BMP-2 remains limited today as evidence has emerged suggesting BMP-2 may result in ectopic bone formation, osteolytic defects, carcinogenesis, severe edema and wound healing complications in non-craniofacial applications.13–15 In addition, it is unknown how previous use of this osteogenic bone factor ages long term or interacts with bone growth factors used in subsequent surgeries, especially those occurring many years later.
The cleft-craniofacial center at our institution follows a cohort of patients previously treated with BMP-2 to the alveolar cleft by a previous surgeon. Currently, there are no studies investigating the use of DBX for revision alveoloplasty in patients previously exposed to BMP-2 who continue to have an alveolar bony defect. Many of the families of these patients remain motivated to avoid the donor site morbidity of autologous grafting, and DBX provides an attractive alternative to iliac crest harvest. Because DBX has been shown an effective alternative for revision bone grafting in cleft patients treated with previous iliac bone graft, 16 we hypothesize that DBX is a safe and effective alternative to autologous iliac bone grafting for these patients who have failed their initial “boneless” bone graft procedure.
Methods
Patients and Study Design
In this IRB-approved, retrospective, single-center study, we searched for all surgical encounters with the Current Procedural Terminology (CPT) code 42210 (Palatoplasty for cleft palate, with the closure of alveolar ridge; with bone graft to alveolar ridge) from the years 2013–2019. We included all patients diagnosed with cleft alveolus under the age of 18 who underwent prior alveolar surgeries using BMP-2. Excluded patients were those without prior BMP-2 use, those with less than 12 months of follow-up time, and those undergoing concurrent orthognathic surgeries at bone grafting (such as maxillary advancement).
Surgical Methods and Surgeons
Under general endotracheal anesthesia, two experienced cleft surgeons performed all revision alveolar bone grafting (ABG) procedures. Gingival mucoperiosteal flaps were elevated and closed posteriorly to create a watertight soft tissue envelope for grafting. Either autologous bone graft only or demineralized bone matrix (DBX) was used to fill the cleft defect and then a sliding gingival flap used to close the repair. Autologous bone graft sources were derived from the iliac crest.
Chart Review and Data Extraction
From each chart reviewed, we extracted the following variables: gender, age at the time of surgery, cleft subtype, prior BMP use, type of bone grafting, hospital length of stay, follow-up time, and graft failure. Our primary outcome was graft failure defined as the need for further surgery to close a persistent alveolar bony defect. A standard scoring index was not used for postoperative assessment because periapical imaging data was not available for enough patients for meaningful review. We looked at postoperative CT-generated panorexes and used these as a proxy to assess bony union via the Bergland index. Each patient included in this study had a follow-up interval of at least 12 months post-op to allow for time to capture graft failure. Secondary outcomes measured included length of stay, operative time, and in-patient narcotic requirements. We excluded surgeries with additional procedures (eg, revision of cleft lip at time of bone grafting) from calculating operative times. We used integer days to calculate the length of stay and measured pain requirements in morphine equivalent doses/kg/day. We also sought out short term complications such as hematoma, surgical site infection, readmission in the first six weeks after discharge and long-term complications such as pain and/or paresthesia at six month follow up for each chart reviewed.
Statistical Analysis
We used GraphPad-Prism 6 software (La Jolla, CA) for statistical analysis. We used Fisher's exact test for categorical comparisons. Parametric, continuous variables were analyzed using the Student t-test. A P-value of <.05 was considered statistically significant.
Results
Current Procedural Terminology (CPT) code search for “42210” resulted in 28 unique patients with 37 surgeries. After excluding patients without prior BMP-2 exposure, those undergoing repeat grafting, and patients with less than 12 months of follow-up, 17 unique patients with 17 surgeries remained. This process is highlighted in Figure 1. The median age at revision alveolar bone grafting (ABG) was 13.1 ± 3.3 years, with a mean follow-up time of 4.9 years (1.1–9.2 years). Data regarding age at primary alveoloplasty with BMP-2 was limited to 11/17 patients (64.7%), however when this data set was analyzed, the age for initial alveoploplasty with BMP2 was varied with mean of 4.09 years (SD 3.3). Patient demographics were similar between the sexes (53.0% male, n = 9) and among cleft subtypes (53% bilateral, n = 9). Ten patients were treated with DBX only to their bony alveolar cleft (58.8%), and seven received autologous bone grafts (41.2%). One patient underwent nasoalveolar molding (NAM) during infancy.
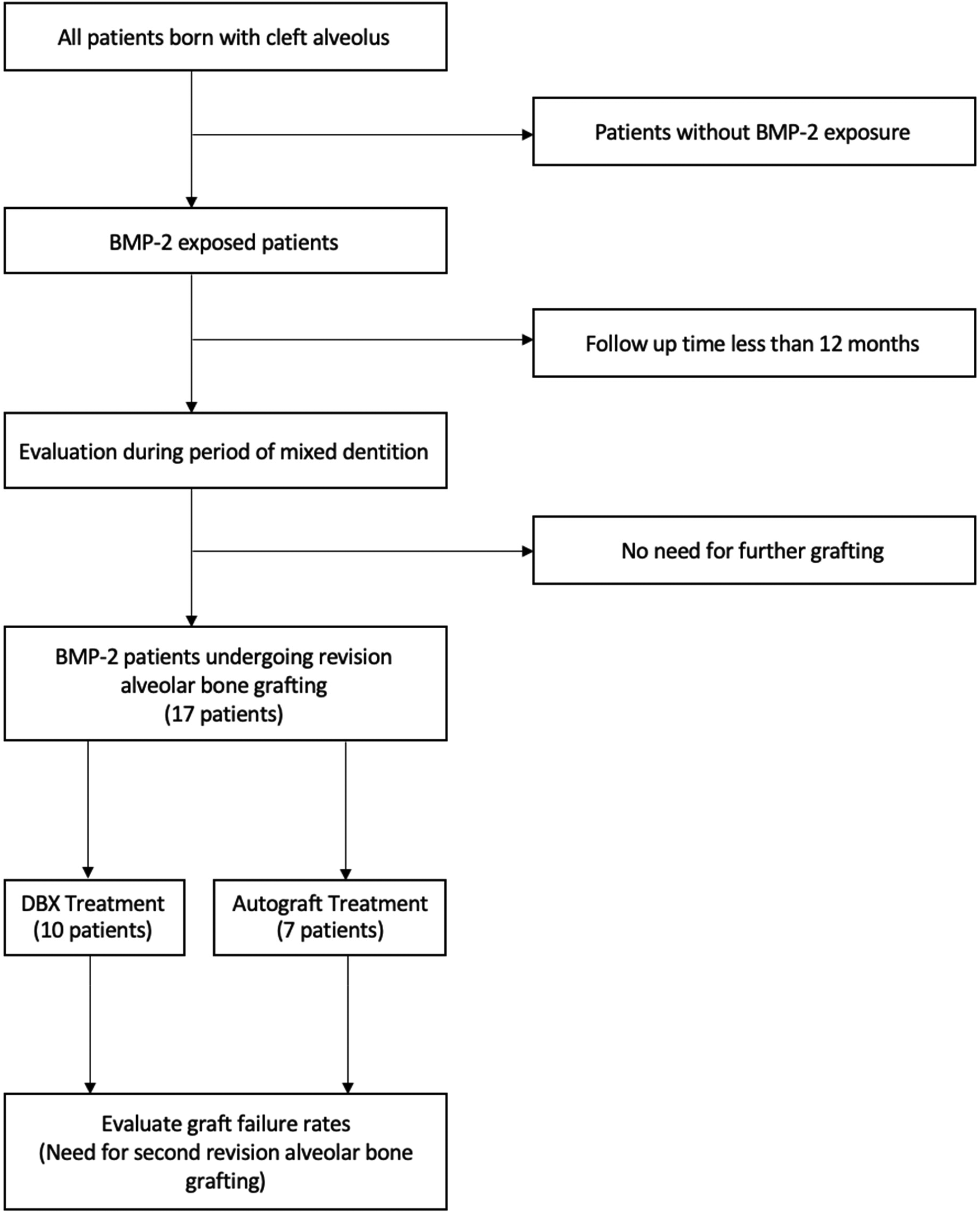
Study Design. Flowchart describing the process that led to the inclusion of the 17 patients undergoing bone grafting in mixed dentition following BMP-2 exposure in infancy.
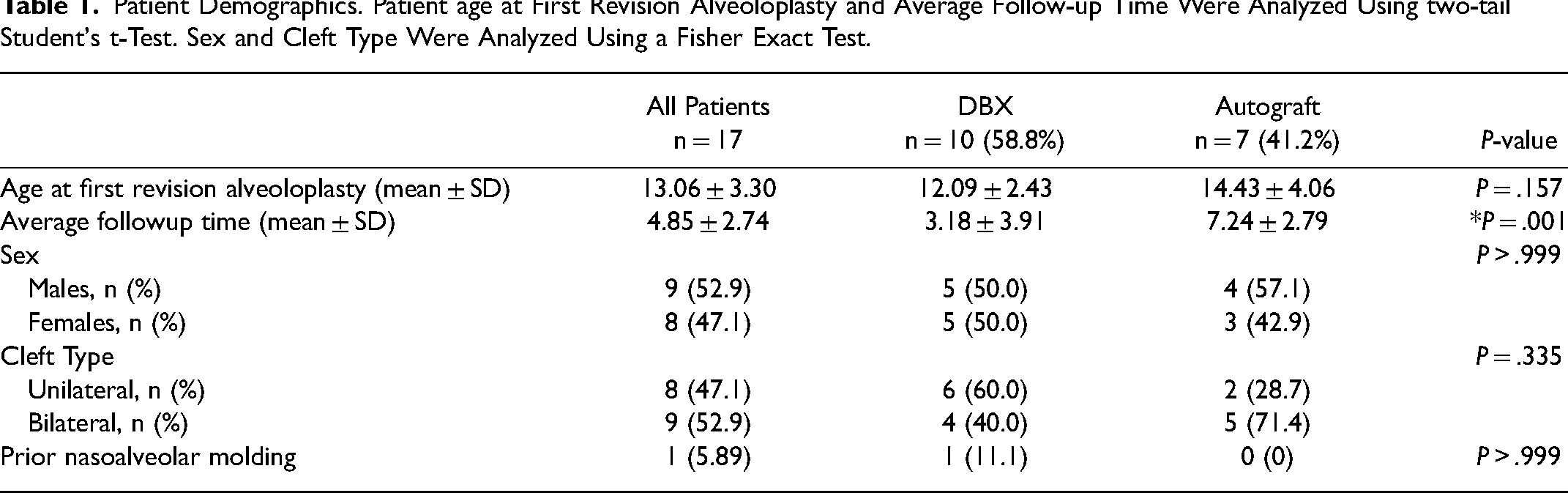
Patients were stratified by graft subtype to either patient receiving demineralized bone matrix (DBX) only (n = 10, 58.8%) or those receiving autograft (n = 7, 41.2%). Although patients receiving autograft had longer follow-up time (7.24 ± 2.79 versus 3.18 ± 3.91, P = .00049), there were no other differences between the two groups when analyzed by age, sex, cleft type, or prior alveolar molding (Table 1) suggesting the two subgroups were similar in composition. Overall, 11.8% (n = 2) of all reconstructions failed, requiring a second surgical procedure. When comparing patients with alveolar union to those who required further surgery, the groups were similar in age, follow-up time, sex, cleft subtypes, and use of nasoalveolar molding. Three patients had postoperative periapicals available for scoring with the Bergland index. Six individuals had CT-generated panorexes taken an average of 392 days post-operatively (range 144–894 days), which we also evaluated using a Bergland index. Two individuals had bilateral clefts, yielding a total of 8 clefts which were evaluated. Of these, the average Bergland score was 1.25 postoperatively (with a score of 1 indicating complete union and 4 indicating no bony union).
Patient Demographics. Patient age at First Revision Alveoloplasty and Average Follow-up Time Were Analyzed Using two-tail Student's t-Test. Sex and Cleft Type Were Analyzed Using a Fisher Exact Test.
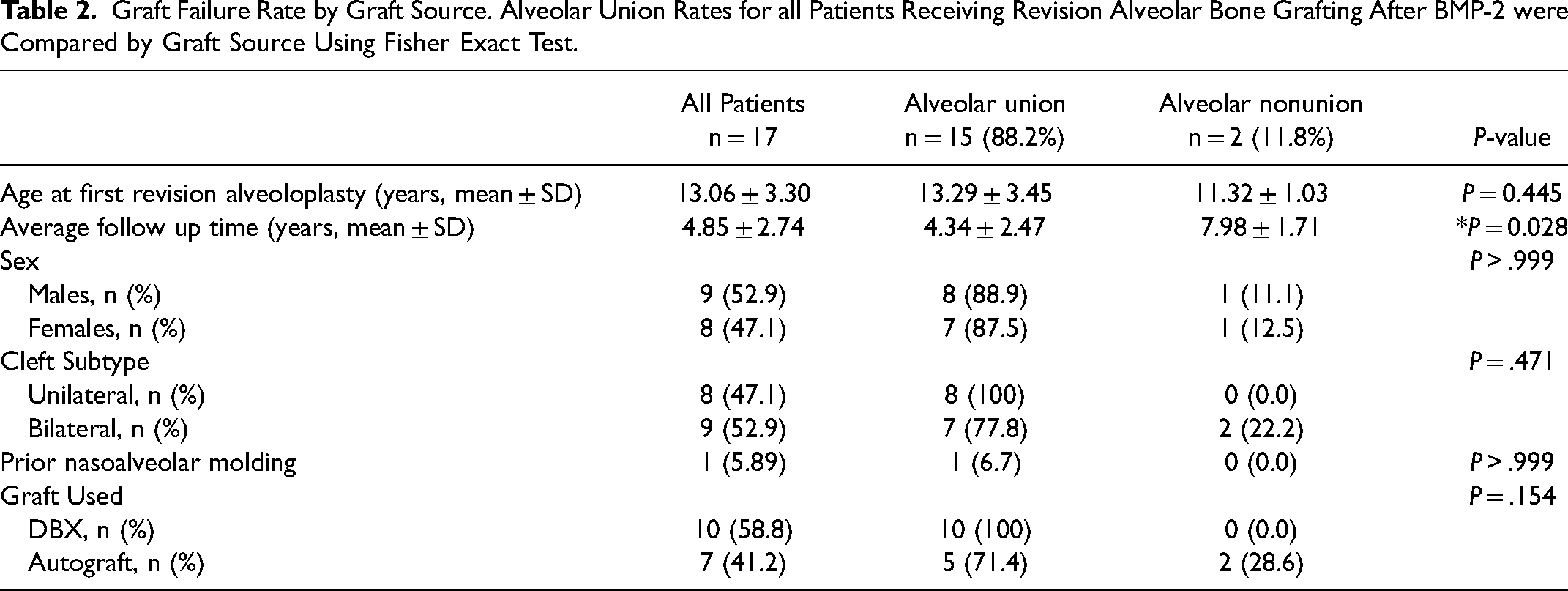
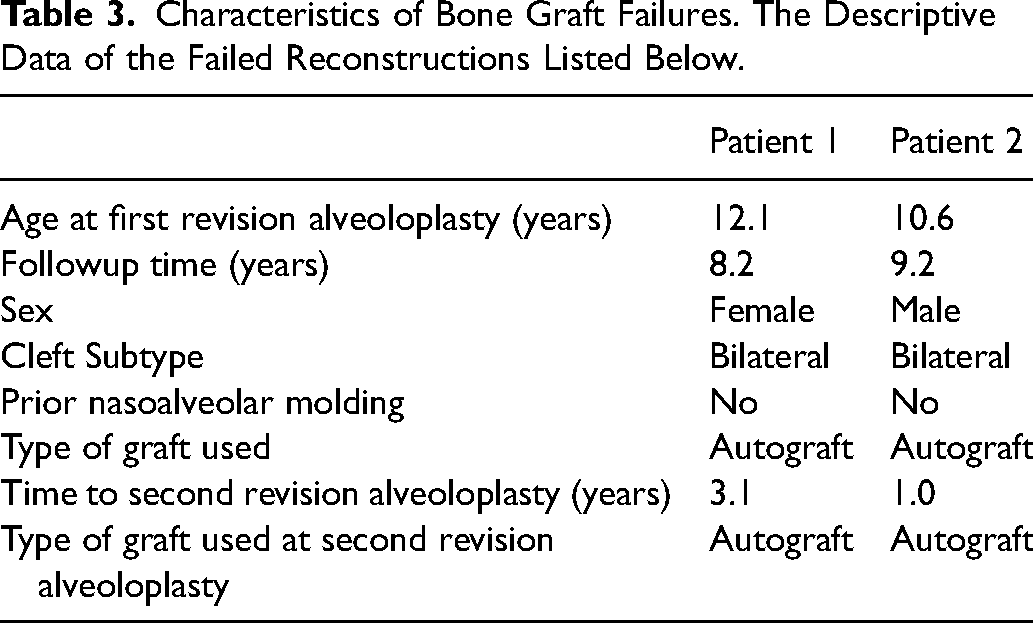
Revision alveolar grafting with demineralized bone matrix had a lower graft failure rate than autograft (0% versus 28.6%), but this difference was not statistically significant (Table 2). The average time to reoperation in the reconstructions that failed was 2.06 years. These failures were both bilateral clefts treated with autograft at the first revision who went on to union after a second round of autologous grafting (Table 3). Surgery with DBX was significantly faster (2.45 ± 1.1 h) versus autograft (5.28 ± 1.85, P = .00123) and also had a significantly shorter length of hospitalization (0.5 ± 0.53 days versus 1.29 ± 0.49 days, P = .00709) (Table 4). We found no short or long-term donor site complications.
Graft Failure Rate by Graft Source. Alveolar Union Rates for all Patients Receiving Revision Alveolar Bone Grafting After BMP-2 were Compared by Graft Source Using Fisher Exact Test.
Characteristics of Bone Graft Failures. The Descriptive Data of the Failed Reconstructions Listed Below.
Perioperative Characteristics: Operative Time, Length of Stay and Narcotic Requirements Were all Compared by Subtype Using two-sided Student t-test.

Discussion
Alveolar clefts typically occur at or near the maxillary lateral incisor, mesial to the canine.5–7 There are many techniques described to repair the bony defect in the cleft alveolus. With the use of nasoalveolar molding, repair can be performed as early as in infancy with a soft tissue gingivoperiosteoplasty. This procedure relies on the osteoinductive capabilities of infant periosteum to create bone after repair. Others perform early primary bone grafting in infancy to promote early alveolar closure most often with a rib graft. Effect of these early closures on facial growth have been widely debated.5,7,10 More commonly, repair of the alveolus occurs later in childhood during mixed dentition with soft tissue flaps and autogenous bone grafting. This is timed often after orthodontic expansion of the arch and ideally before tooth canine tooth eruption. 3 Termed secondary alveolar bone grafting, this is the most common standard of care, typically performed around ages 7–12 years when tooth development is at the appropriate stage. 8
Regardless of technique, alveolar cleft repair serves to unite the maxillary segments to stabilize occlusion and provide support to the dentition while also obliterating the nasal fistula and adding support to the alar base. 5 A successful procedure is assessed by restored continuity of the alveolus the stability of the arch, closure of the oronasal fistula, and adequate volume of the bone matrix for tooth eruption and alignment. 16 Without proper repair, alveolar clefts produce functional and cosmetic impairment ranging from non-eruption, instability, or loss of teeth in the cleft area, malocclusion, nasal asymmetry, poor speech and difficulty with hygiene. 5
Autograft use is associated with donor site morbidity, including pain, hematoma, scarring potential nerve injury and infection.7,17 Bone allograft sources such as DBX are an attractive alternative to avoid this morbidity. The discovery of bone morphogenetic protein (BMP) as an agent in the allograft demineralized bone matrix (DBM) by Marshall Urist led to the clinical use of allograft first in orthopedic surgery and then in maxillofacial surgery officially after 2007.9,10 It has been used successfully in revision alveoloplasty after failed primary alveolar bone graft as well as to augment allograft in revision alveolar grafting. 15
Another alternative source to autologous bone graft is use of recombinant human bone morphogenic protein-2 (BMP-2). Bone morphogenetic protein-2 and 7 (BMP-2, BMP-7) are cytokine members of the TGF-beta gene family and are the most studied form of the BMP family for maxillofacial surgery. They stimulate osteoblast activity by inducing differentiation of osteoprogenitor and mesenchymal stem cells into functional osteoblasts and thus promote bone formation.5,12–14 BMP-2 as recombinant human (rh)BMP-2, a bone-graft substitute, is approved by the Food and Drug Administration (FDA) for use in spinal fusion as well as some oral and maxillofacial grafting procedures. It has been studied off label for treatment of alveolar clefts in a few centers and found to effectively create bone in the defect that behaved similarly to other bone graft material allowing dental eruption, orthodontic movement and dental implant placement in the initial follow up period.9,10 More recent meta-analysis of BMP-2 use in alveolar cleft repair found bone creation to be effective or higher with BMP-2 compared to traditional autologous grafting, however found a high risk of bias in the articles reviewed.18–20 True clinical trials are required to verify these results which are lacking currently. In addition, complications associated with BMP-2 use have been reported including ectopic bone formation, osteolytic defects, carcinogenesis, wound complications, severe soft tissue swelling, dysphagia, and respiratory compromise,12,14,17 although these have not been reported in association with cleft ABG procedures. There is also an unclear link between BMP-2 application and carcinogenesis 12 that may be dose dependent. Because of these concerns, the regular use of rhBMP-2 in alveolar reconstruction is not yet widespread despite similar advantages to bone allografts.
When bony union does not occur in patients previously treated with BMP-2, revision alveoloplasty is required. Allograft such as DBX carries the similar advantages of avoiding donor site morbidity with a proven track record of safety in revision alveoloplasty.15,21 We follow a cohort of patients some of whom were attracted to this center originally because of the unique opportunity to attempt alveolar closure without a donor site using BMP-2. This has remained a priority to some families making allograft use for revision in the case of BMP-2 failure an attractive alternative to traditional bone. In this study, we sought to determine how DBX allograft performed versus traditional iliac crest bone grafting for closure of persistent bony defects in patients during revision alveoloplasty.
Our study found use of DBX was not inferior to autograft when used in revision alveolar bone grafting in patients who were previously treated with BMP-2 with a 0% failure rate in the DBX group versus 28.6% in the autograft group as measured by need for further surgery to unite the alveolar segments and complete orthodontics. This finding corroborates with existing literature in patients undergoing revision alveolar bone grafting with DBX after traditional failed alveoloplasty with autograft. 15 In this population, we elected to repeat iliac crest bone graft for the two instances of autologous bone graft failure given this is the gold standard. However, this study shows use of DBX for revision alveolar grafting post BMP-2 failure provides an effective option for patients and families that remain opposed to the added recovery and potential morbidity associated with traditional iliac crest bone harvest.
Our study also examined other potential benefits of considering DBX as an alternative to allograft for revision alveoloplasty in patients previously treated with BMP-2. There was a statistically significant difference in operative times between these techniques with DBX taking 2.3 h versus iliac crest allograft 4.4 h (P = .0058). This is not unexpected and confirms one advantage of DBX use allowing avoidance of the donor site harvest portion of the case. When examining hospital length of stay with DBX versus autograft, our study also found a statistically significant reduction in length of stay with DBX use (0.56 days vs. 1.15 days P = .0495). In addition, there was a trend for decreased use of narcotic pain medications as measured by morphine equivalent doses (MED) in the hospital with DBX patients requiring 0.93 MEC and allograft patients 1.51 MEC that did not reach statistical significance (P = .07).
Limitations
This study is limited by its retrospective nature and relatively small sample size reflecting the cohort of children followed. The sample size may underpower our findings. The decision to use allograft (DBX) versus autograft was not randomized instead with family preference often the driving choice of surgery technique after informed discussion. In addition, this study longitudinally follows two surgeons which may have refined their surgical technicques with experience, potentially impacting success rates.
Another limitation of our study was that we were unable to employ a radiographic measure of graft outcome with standard scoring such as the Bergland index.22,23 Our cleft population is managed primarily by outside orthodontic providers who complete the radiographic imaging post alveolar bone graft as part of their ongoing care. Despite contacting these offices, obtaining hard copies of outside periapical films in a retrospective manner was only possible in a limited number of patients (n = 3). Given the associated extra cost and risks of radiation to the patient, it is not our current practice to obtain duplicated imaging within the hospital system unless clinically indicated. We did retrospectively examine CT scans of individuals who received postoperative CT scans in an effort to evaluate bridging. Of these, the average Bergland score was 1.25 postoperatively, consistent with our clinical findings of adequete bony bridging to support the progression of orthodontia. With improvements in the electronic medical records system, our team is now working on more consistently obtaining and archiving outside radiographs for the benefits of future study. Although CT scans are not routinely used in our practice, routine CT scans in future studies pre and postoperatively could allow volumetric analysis to better quantify union. Future prospective studies with standardized post-operative imaging protocols are needed to better capture potential subtle differences in bony volume and union pattern when evaluating overall graft success.
Although our sample was similar in demographics regarding patient sex, age and even cleft type between treatment groups, the effect of cleft width was not able to be examined and may have affected results (Table 2). The failure cases both involved bilateral clefts treated with autograft which is not unexpected given the higher overall rate of regrafting needed overall in this cleft subset. However, bilateral clefts were equally represented in both treatment groups (DBX = 4, allograft = 5 with P = .46), so this is not likely the only reason other than chance for higher failure of allograft detected which was not overall statistically significant.
Although follow-up time was significantly different between the groups (DBX = mean of 3 years and allograft = mean of 8 years) (Table 1), the two failures requiring regrafting were noted and completed by 1 and 3 years in the failure cases indicating this follow up was likely sufficient to capture most graft failure. Future prospective studies are needed to further address these potential biases.
Conclusion
Demineralized bone matrix (DBX) and autologous bone grafting were found to have similar failure rates during revision alveolar reconstruction in patients previously treated with bone morphogenetic protein 2 (BMP-2). Although further studies are needed, the comparable outcomes and reduced potential donor site morbidity, surgical time, hospital length of stay, and use of pain medications suggest that DBX allograft is an attractive and viable alternative to autograft in this patient cohort. Continued long term follow up of dental reconstruction in these patients is needed to confirm stable results.
Footnotes
Acknowledgements
None.
Authors Note
This work contained in this manuscript was presented at American Cleft Palate-Craniofacial Association, September 30, 2018; Portland Oregon American Society of Plastic Surgeons Virtual Conference, September 15, 2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.