
Abstract
Objective
Accurate nationwide epidemiological evidence is vital to study the seasonal, geographic, and ethnic influence on the trends of orofacial cleft prevalence in Kuwait.
Design
Data obtained from the National Center for Health Information and Ministry of Health Hospital digital records were reviewed retrospectively to identify patients with orofacial clefts (OFC) using the ICD-10 diagnostic codes. The Jonckheere-Terpstra test was used to assess the trend of birth prevalence across the different years. The associations of types of OFC with ethnic and geographic influences were tested with chi-square or Fisher's exact tests, while the strength of that association was tested with multi-nominal logistic regression.
Results
Birth prevalence in Kuwait ranged from 0.75–2.55 per 1000 live births (0.73- 2.73 among Kuwaitis, 0.60–3.27 among non-Kuwaitis), with no statistically significant change observed during the past 28 years. The risk of unilateral cleft lip and palate was eight times higher during summer compared to Autumn, while the risk of cleft lip and palate remained lower during winter. Jahra (OR-7.76, CI- 1.51–39.80), Farwaneya (OR-6.65, CI- 1.34–33.06), and Hawalli (OR-6.72, CI- 1.26–35.98) governorates had higher odds of bilateral cleft lip when compared to Mubarak Alkabeer.
Conclusions
The study outcome is an indicator to improve patient care and customize healthcare infrastructure in the Ministry of Health. It also provides insight to develop projections of future needs. Future studies should focus on understanding the factors that might be a potential contributor to the seasonal change observed in the prevalence of OFC.
Introduction
Orofacial clefts (OFC) are the most common congenital defects, with a prevalence of 0.57–2.62 per 1000 live births worldwide. 1 Cleft lip (CL) results from the failure of the emergence of the median and lateral nasal processes and the maxillary prominence around the 6th week of pregnancy, while cleft palate (CP) is caused by a lack of fusion of palatal shelves during the period between the 8th and 12th week. 2 CL and CP can occur in isolation or together. Previously published evidence from Kuwait, based on the data from a single center study, reported a mean birth prevalence with a wide range of 0.57–1.56 per 1000 live birth.3,4 Although genetic, epigenetic, and environmental factors have been investigated, well-designed studies in Kuwait are minimal.
Kuwait is a relatively small country but represents a mixture of multiple ethnicities, where 70% of the population are non-nationals, with 1.1 million Arab and 1.4 million Asian expatriates. 5 On the other hand, the nationals are mostly of Arab origins, with high rates of consanguinity. 6 Comparing a highly homogenous group (Kuwaitis) to another from different backgrounds (Non-Kuwaitis) can provide a unique epigenetic insight into a multifactorial congenital anomaly like OFC. The socialized healthcare system in a relatively geographically small country allows good documentation of cases from all ethnic and socioeconomic backgrounds, leading to a near-complete representation of all groups and more accurate comparisons. Although the findings of this study pertain to data collected from Kuwait, conclusions can also be drawn for other Middle Eastern, Arab, and Asian populations who constitute the majority of the local community. 5
To understand the impact of OFC in the Kuwaiti community and better estimate the burden of care for the families and healthcare system, it is vital to obtain accurate epidemiological evidence that includes the prevalence of orofacial clefts and the factors influencing it. This will improve the quality of life of patients with OFC and provide a source to understand further these birth defects’ etiology and pathogenesis.
The etiology of OFC is still not fully understood. However, environment and genetics play major roles in cleft lip and palate development. If an individual is susceptible genetically, then additional environmental factors may trigger cleft development. Therefore, OFC is considered a multifactorial disorder with a complex etiology. 7 Possible teratological factors include smoking, drug/alcohol consumption, and deficient nutrient intake during the first trimester. 7 Other possible environmental factors include air/water pollution, lack of direct sunlight, and seasonal variation.8,9
The authors hypothesize that seasonal, geographic, and ethnic factors play a role in the prevalence of OFC in Kuwait. Thus, this study aims to assess the trend of birth prevalence over the past 28 years and explore the seasonal, geographic, and ethnic influences.
Materials and Methods
Ethical approval for this study was obtained from the ethical committee for conducting medical research at the Ministry of Health (MOH)s, Kuwait (IRB #1333/2020) and in agreement with the guidelines of the Helsinki Declaration (as revised in 1975). National Center for Health Information (NCHI) records were obtained and reviewed retrospectively to identify patients with oral cleft diagnosis using the ICD-10 diagnostic codes. 10 The codes were entered into the NCHI database through the medical team at all MOH hospitals upon discharge or mortality. In addition, local digital records at the following hospitals were examined, where similar codes were entered into the local server; Albabtain Center for Burns & Plastic Surgery, Alamiri Craniofacial Orthodontic Clinic, Kuwait Medical Genetic Center (KMGC), Farwaneya Hospital, Adan Hospital, Jahra Hospital, Mubarak Alkabeer Hospital, Maternity Hospital, and Zain Otorhinolaryngology Hospital. Logbooks representing outpatient clinics at the Plastic Surgery and Craniofacial Orthodontics outpatient Clinics were also reviewed.
Home birth is not practiced in Kuwait, 11 thus, all births are delivered in a licensed healthcare facility. All births in the governmental sector and treatment received later in life would have been in one of the included hospitals. At the time of data collection, the NCHI, the hospitals’ digital records, and outpatient clinics’ logbooks represent the only means of documentation in the Ministry of Health. For all patients included, the nationality, area of residency, date of birth, and gender information were recorded. Duplicate records were removed after being matched with unique civil identification number and birthdate. Live birth data from 1992 through 2019 were obtained from the NCHI and used to calculate the year-wise prevalence of OFC per 1000 live births.
For data collected from 1992–1993, the authors converted descriptions of the cleft diagnosis to the corresponding ICD-10 codes. Surgeons have used these descriptions in Albabtian Plastic Surgery Hospital medical records, the only hospital at the time where patients with craniofacial deformities were treated. In 1994, the ICD-10 was integrated into Kuwait's NCHI database following the WHO guidelines. 12 Table 1 presents details of the ICD-10 codes used.
Clinical Cleft Descriptions and the Corresponding ICD-10 Codes with the Order of Severity.
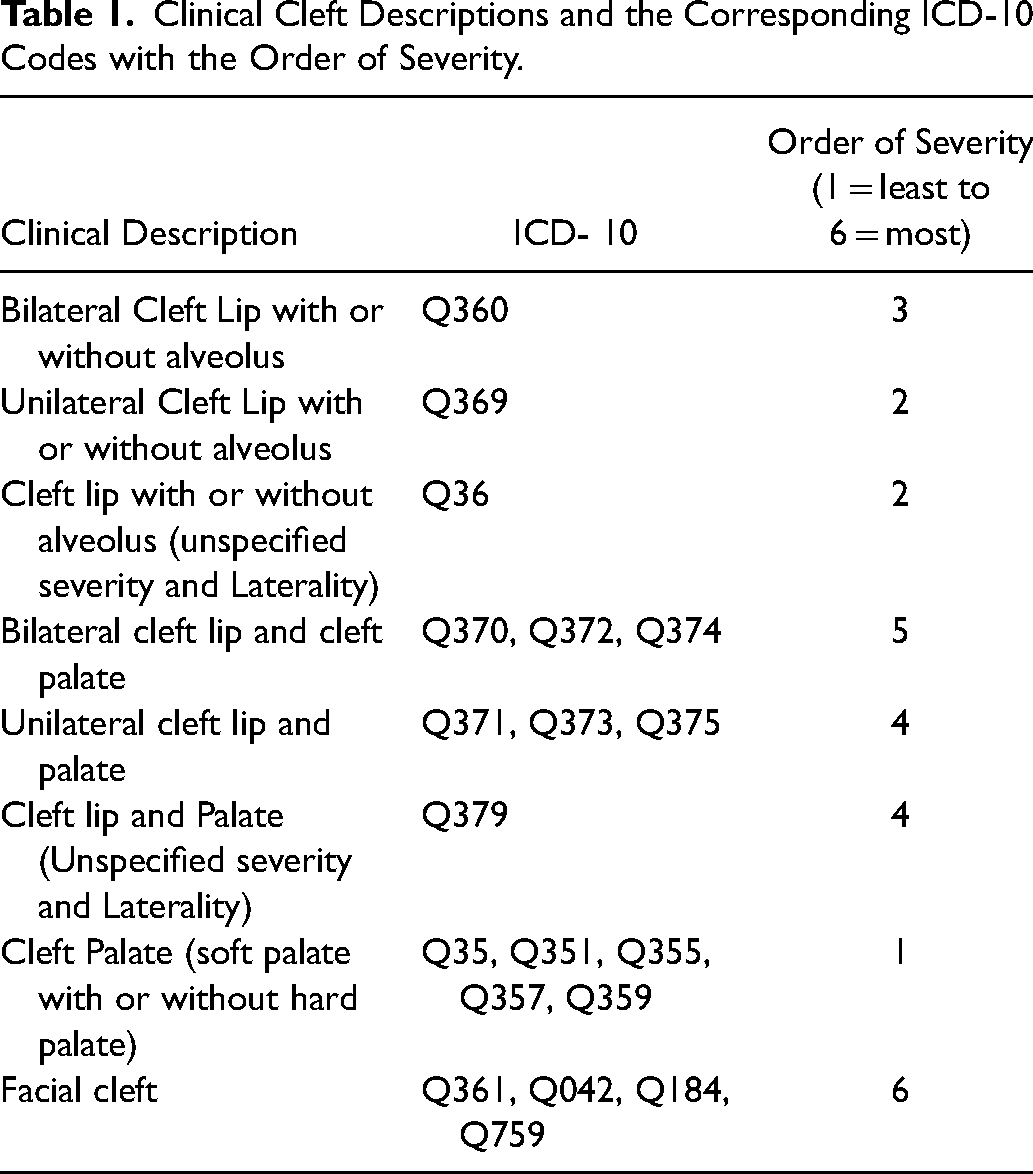
The clefts were categorized on a six-level classification based on type and laterality. Bilateral cleft is considered more severe than unilateral, as it increases the burden of care on the individual and the healthcare system by increasing the number of surgeries, 13 degree of deformity, 13 degree of pharyngeal airway space reduction,, 14 and the associated dental anomalies. 15 Bilateral cases have also shown more dental developmental delays compared to unilateral cases. 16 Cleft palate was classified as less severe than unilateral or bilateral cleft lip/alveolus with or without palate as it is associated with less burden of care. 17
In cases with other associated syndromes, the NCHI database includes a principal diagnosis (OFC clefts) and other diagnoses. These include Q75.4 (Treacher Collins syndrome), Q02 (microcephaly), Q549 (Hypospadias), and Q203 (Discordant ventriculoarterial connection), etc. For such diagnoses, the case is marked as syndromic. In addition, medical charts were reviewed when available at the Plastic Surgery and Craniofacial orthodontic clinics for other diagnosed anomalies/syndromes.
The study used descriptive statistics to illustrate basic demographic characteristics. Since the year-wise birth prevalence of OFC was not normally distributed, Jonckheere-Terpstra test was used to assess the trend of birth prevalence across the different years. Mann-Whitney U-Test was used to analyze the difference in the birth prevalence comparing Kuwaitis and non-Kuwaitis. A subgroup analysis for the trend of birth prevalence was also performed for the year 1997–2019 after excluding the data from 1992–1996 due to the possibility of incomplete data collection. During the early 1990s, medical data and records registration was not optimal as the healthcare system was still recovering from the first gulf war.
A chi-square test/Fisher's exact test was performed to test for association between types of OFC and demographic and environmental factors. Multi-nominal logistic regression was also performed to evaluate the association of demographic and environmental factors with types of OFC (ICD classification). The model included all the variables in the bivariate analysis, such as governorates, gender, nationality, syndrome, and seasons The statistical analysis was performed using the IBM Statistical Package for the Social Sciences (SPSS) version 22.0 (IBM Corp, Armonk, New York) data processing software. Results are presented as odds ratio (OR) and 95% confidence intervals (CI).
Results
A total of 3473 patient records were identified. After excluding duplicates, the study analyzed 2664 records. Table 2 summarizes the cleft diagnosis and its distribution across demographic variables. More than half the sample were Kuwaiti nationals (56.2%), with a male-to-female ratio of 1:0.85. Non-Kuwaiti nationals were mainly of Southern & Southeastern Asia and Arab origin. About 35% of the OFC cases were diagnosed with CP (soft palate with or without hard palate), followed by around 25% of the sample having unilateral CL with or without alveolus. Almost 10% of cases were diagnosed with unilateral CLP, while around 6% were diagnosed with bilateral CLP and CLP with unspecified severity and laterality. Of the total OFC patients included in this study, 5.4% had one type of facial cleft. Of the unilateral cases, 62.5% were on the left, and 37.5% were on the right. Table 2 also summarizes the total number of cases with the results of bivariate analysis of the independent variables.
Distribution of ICD Across Demographic Variables.
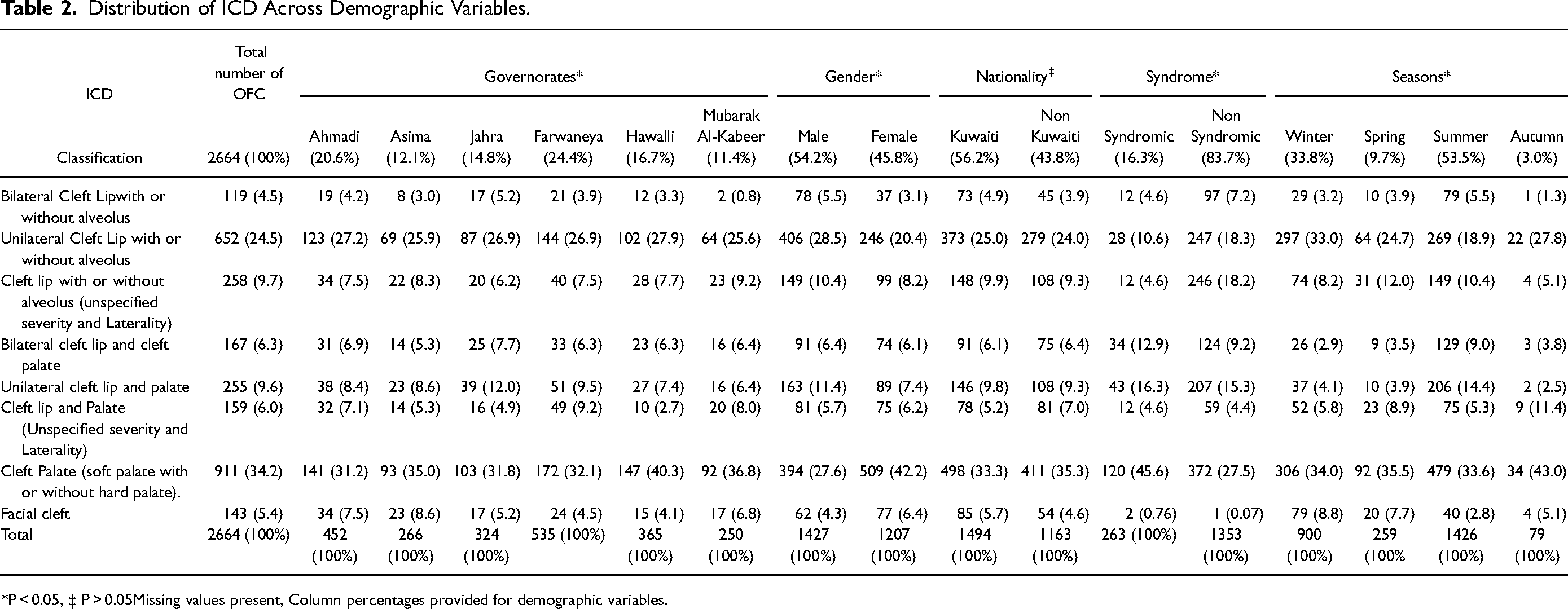
*P < 0.05, ‡ P > 0.05Missing values present, Column percentages provided for demographic variables.
Around 83.7% of OFC patients were observed to be non-syndromic when compared to 16.3% that reported some form of associated syndromes. Trisomy anomalies (2.7%) were the most reported syndrome among this group. The distribution of OFC among syndromic and non-syndromic patients was significantly different (P < 0.001). Among the syndromic patients, the majority had CP (45.6%), followed by unilateral CL (16.3%) and bilateral CLP (12.9%). The results also showed a significantly higher number of OFC cases among males compared to females (P < 0.001) (Table 2). However, a higher percentage of females (42.2%) reported CP compared to the male sample (27.6%), while unilateral CL with or without alveolus and unilateral CLP were higher in males. While comparing bilateral CL with facial cleft, males were more likely to have bilateral CL (OR-2.14, CI-1.20–3.85). Similarly, when compared to facial cleft, males were almost two times more at risk of having unilateral CL with or without alveolus (OR-1.95, CI- 1.33- 2.86), and unilateral cleft lip and palate (OR-2.12, CI- 1.33–3.-38) (Table 3).
Multinominal Logistic Regression Models for the Association Between Governorate, Gender, Nationality and Seasons and Types of Oro Facial Clefts After Adjusting for Covariates.
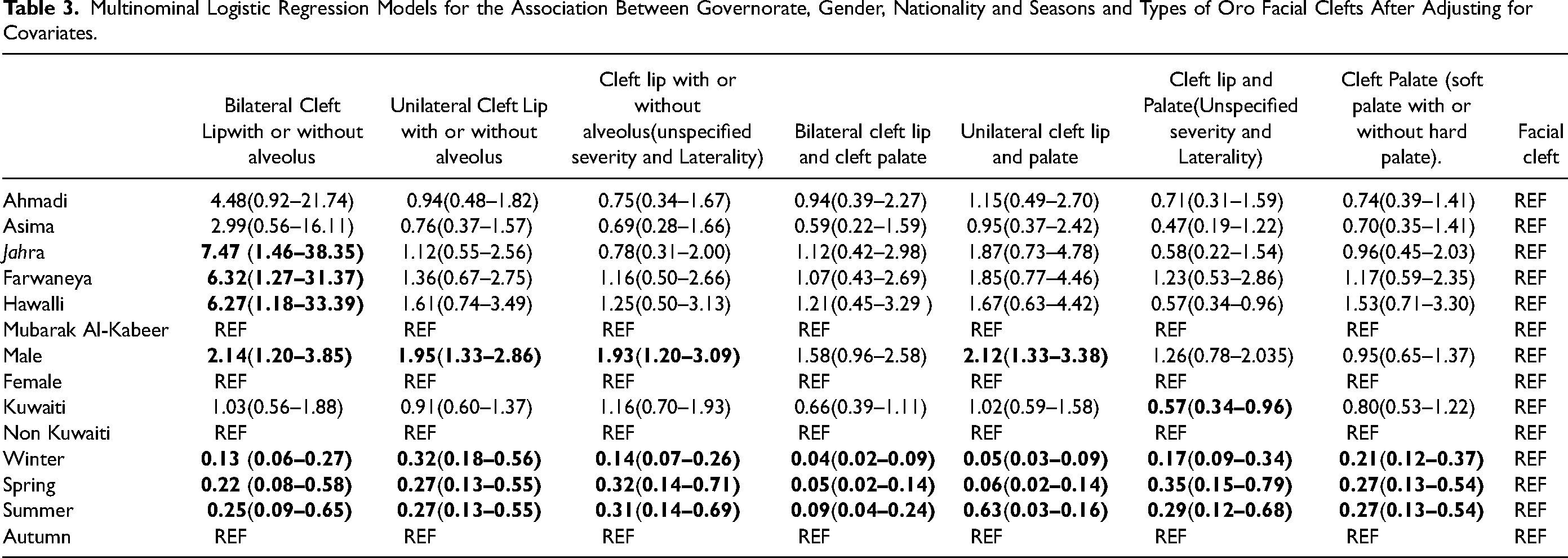
The seasonal changes had a statistically significant influence on the number of OFC cases (P < 0.01) (Table 2). A higher prevalence of OFC was recorded in summer (53.5%) followed by winter (33.8%) season when compared to spring (9.7%) and Autumn (3.0%). When adjusted for other independent variables in the multinomial regression model, the odds of having all other types of OFC compared to facial cleft remained lower during winter, spring, and summer than Autumn (Table 3).
In the bivariate analysis, the nationality status of the samples did not show any significant influence (P = 0.276) on the type of OFC cases (Table 2). On adjusting for other independent variables, while comparing cleft lip and palate with facial cleft, the odds of having cleft lip and palate were slightly lower among Kuwaiti nationals (OR-0.57, CI-0.34–0.96) when compared to non-Kuwaitis (Table 3).
Figure 1 shows the number of OFC case distributions in Kuwait's six governorates and 48 districts. Around one-fourth of the OFC cases resided in Farwaneya Governate (24.4%), and the least number of patients were reported from Mubarak Alkabeer Governorate (11.4%). In the bivariate analysis, the governorate-wise distribution reflected a significant difference in the types of OFC cases (Table 3). Interpreting the regression model (Table3) showed that Jahra (OR-7.47 CI- 1.46–38.35), Farwaneya (OR-6.32, CI- 1.27–31.37), and Hawalli (OR-6.27, CI- 1.18–33.39) governorates had higher odds of bilateral cleft lip than facial cleft when compared to Mubarak Alkabeer.
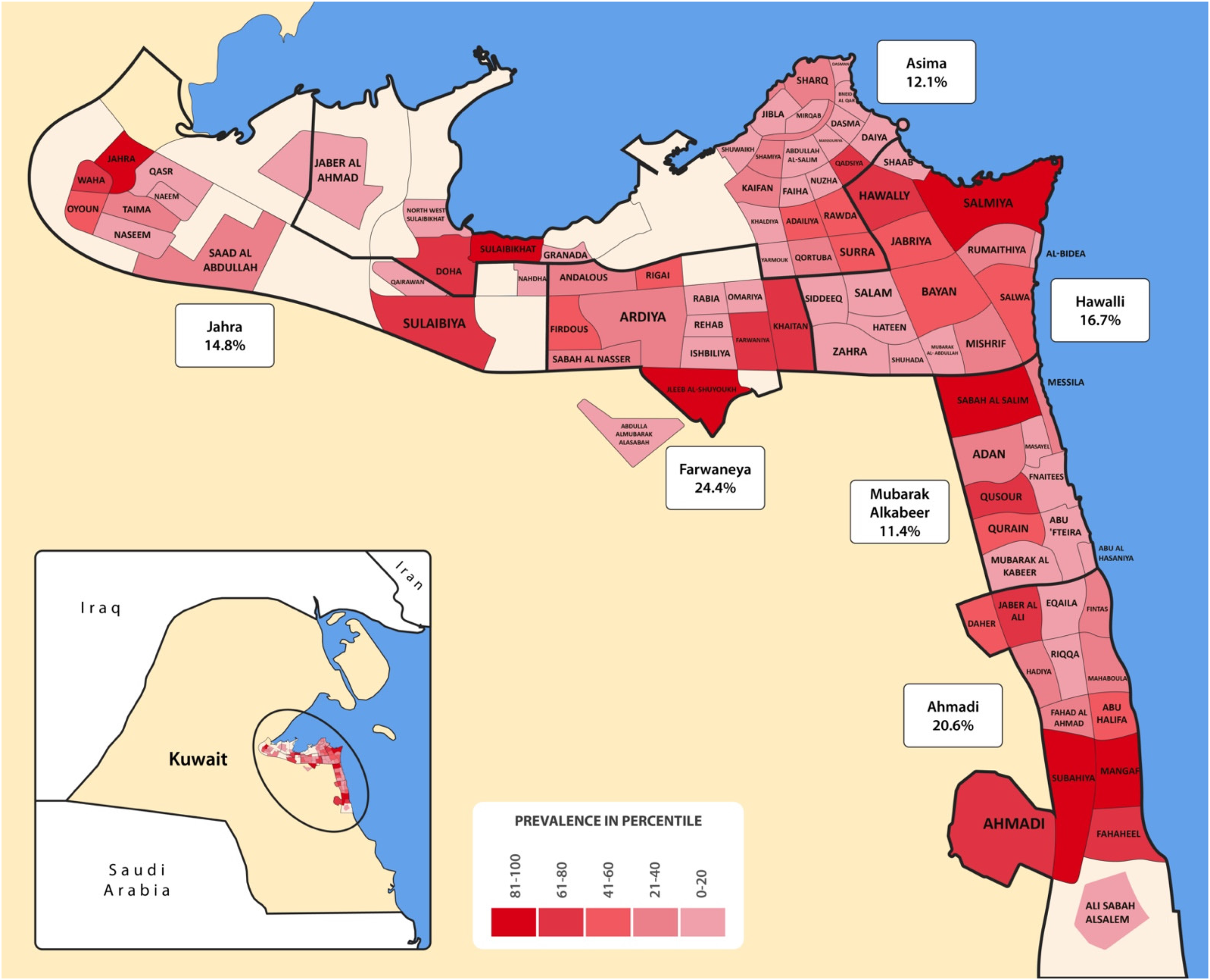
Choropleth map representing the geographic distribution of Oro-facial cleft cases in each governate, visualizing the districts birth prevalence percentiles.
The trend analysis showed no statistically significant trend for birth prevalence over the past 28 years (1992–2019) (Std J-T statistic = -0.296, P = 0.767). The mean birth prevalence over the years was 1.50/1000 live births. However, the birth prevalence was highest in 2005 (2.55/1000 live births), and the lowest recorded was 0.75/1000 live births in 1995. Birth prevalence in Kuwait ranged from 0.75–2.55 per 1000 live births (0.73–2.73 among Kuwaitis and 0.60-.3.27 among non-Kuwaitis). The mean birth prevalence for Kuwaiti nationals (1.42/1000 live births) was slightly lower than for non-Kuwaiti nationals (1.61/1000 live births). A Mann-Whitney U test was performed to assess the mean birth prevalence between Kuwaiti and non-Kuwaiti nationals. However, no difference was observed between the two groups (P = 0.32).
The subgroup analysis for data from 1997–2019 (23 years) showed a statistically significant trend for birth prevalence (Std J-T statistic = -2.536, P = 0.011). The highest birth prevalence was in 2005 (2.55/1000 live births), and the lowest recorded was 0.75/1000 live births in 2003 (Figure 2).
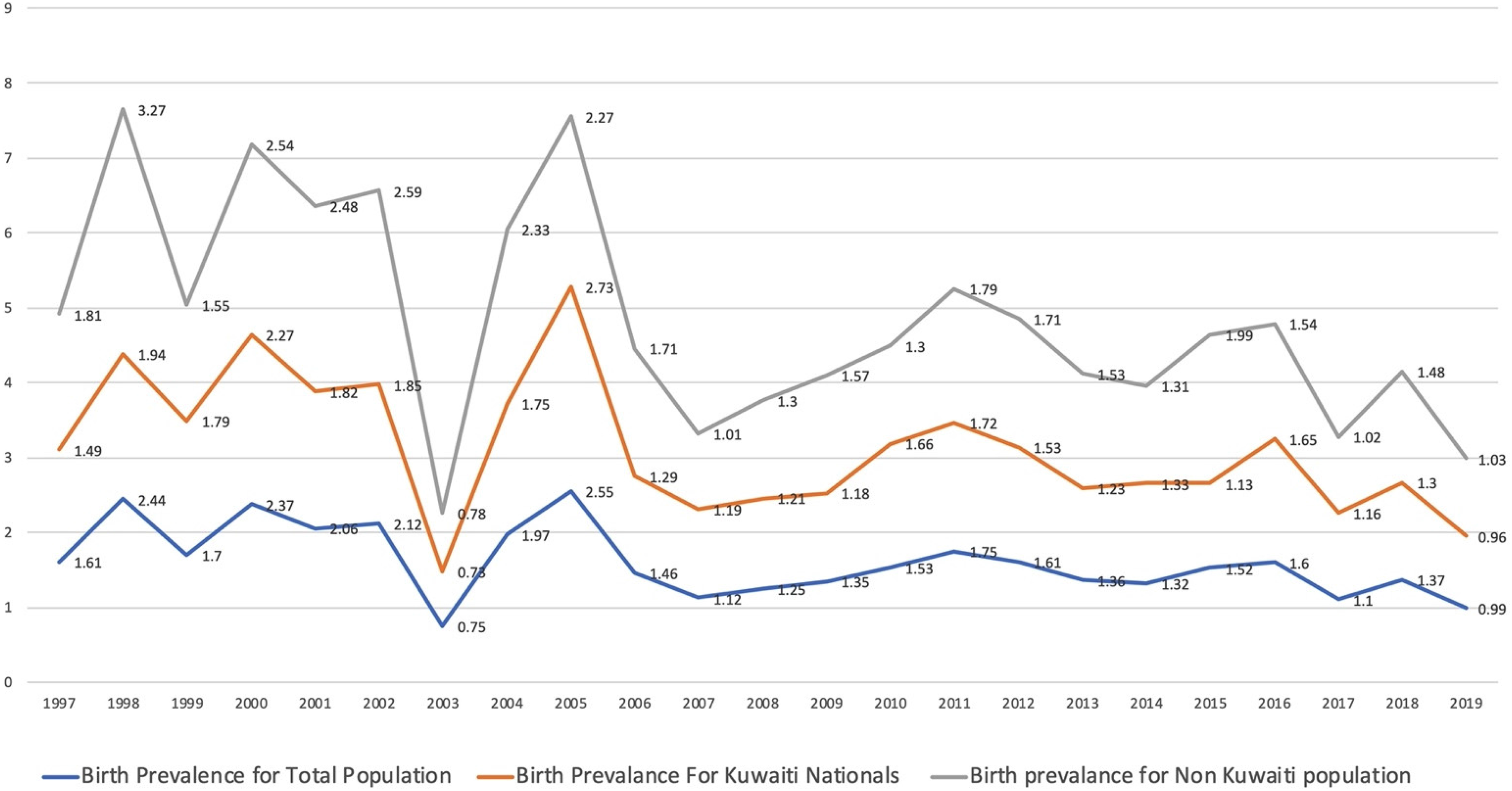
Trends in the birth prevalence of patients with oral clefts in Kuwait.
Discussion
We hypothesized that environmental and ethnic factors play a role in the prevalence of OFC; thus, we explored their roles and assessed the associated trend of birth prevalence over the past 28 years.
Comparing our findings to the birth prevalence of other races indicated that the Kuwaiti ethnicity birth prevalence is comparable to that of the Caucasian and Asian populations, less than that of native Americans and more than the African birth prevalence. 1 Regionally, our findings, 0.75–2.55 per 1000 live births, are closely comparable to data from the region, such as findings from Saudi Arabia and Iran, which reached 2.19 and 2.4, respectively.3,18–24 In the Kingdom of Saudi Arabia, the prevalence rate ranged from 0.3 to 2.4 per 1000 live births.3,18–21 In Oman, 10 health institutes and national registry data were retrospectively reviewed, and the prevalence was found to be 1.5 per 1000 live births. 25 In these studies, the population comprised nationals or mainly nationals. In the United Arab Emirates, a single hospital-based study concluded the prevalence of oral clefts to be 0.5 per live birth, 26 with a similar prevalence of cleft palates in Bahrain. 27
The prevalence rate of orofacial clefts in Yemen was similar to that previously reported among white Caucasians. 28 In Jordan, findings have ranged from 1.39 to 2.4 per 1000 live births,29,30 while the range was 2.14–1.79 per 1000 live births in Iran.22–24 Data from Palestine showed a prevalence of 1.05/1000 live births in a single hospital-based study conducted in Jerusalem. 31
In Kuwait, the male-to-female ratio was 1:0.85, which agrees with the findings of many studies worldwide.18,29 Similarly, cleft palate was the most common oral cleft, which was similar to previous findings from Kuwait, 6 and other countries such as Nigeria, 32 Saudi Arabia, 20 and Australia. 33 In contrast, results from Japan showed that the most prevalent type was unilateral cleft lip and palate. 34 The discrepancy in these findings may have been affected by study design, such as conclusions drawn from studies in a single hospital. In such hospitals, complex cases are referred for treatment by a multidisciplinary team, while less complex cases, such as cleft palates, can be treated locally. However, ethnic variations cannot be ruled out.
In this study, unilateral cases were predominantly on the left side, agreeing with study findings worldwide, including China, 35 Saudi Arabia, 18 and Estonia. 36 Although many attempts were made to explain the left-side dominance in craniofacial anomalies, this phenomenon remains poorly understood. On a molecular genetic level, Matern et al. hypothesized that left-sided clefts are caused by dysfunction of the expression of nodal, lefty-1/2, and Pitx2 genes repressed on the right side. 37 The right-sided clefts are a consequence of insufficient repression, while bilateral clefts result from gene polymorphisms not associated with laterality.37,38
Our findings illustrated that the most common cleft type in females was cleft palate; in males, it was unilateral cleft lip with or without alveolus. This is similar to findings from Japan, 34 Thailand, 39 Estonia, 36 and Yemen. 28 One explanation could be that the female sex hormone could delay the palatine process fusion, as the fusion occurs earlier in males. Speculations have also been made about differential timings in the development of male and female embryos and the influence of teratogens and other environmental factors in a certain gestational age. 40 An analysis of variance in the prevalence of cleft lip with or without palate and isolated cleft palate found no differences in paternal age. However, the age of the fathers of female patients was higher than that of males. The theory was that females may have a higher threshold of resistance to factors associated with cleft lip and palate. 41
Seasonal variation was significant, in agreement with the findings of Sofianos et al. 42 and Chung et al. 9 but different from those of Jahanbin. 8 The prevalence of OFC was significantly higher during summer when the first trimester could have occurred in October–April. Further ecological and animal studies are vital to identify the association between seasonal variation and OFC in Kuwait.
A statistically significant trend was observed for the birth prevalence over 23 years (1997–2019); the highest birth prevalence was during 2005 (2.55/1000 live births), and the lowest recorded was 0.75/1000 live births during 2003. Increased birth defects associated with environmental factors, such as post wars,43–46 and periods of exposure to air/water pollution 8 have been reported. Further studies might provide a better insight into understanding this trend.
Collecting non-standardized data from multiple sources is a limitation of this study. The possibility of incomplete data collection is also another limitation. In 2020, MOH records showed significantly fewer reported cases than in previous years and thus excluded from this study. The SARS-CoV-2 pandemic had affected the MOH operational power, and “elective” surgeries were suspended. Consequently, many families opted to receive treatment in the private sector, resulting in a lack of documentation in MOH records. In addition, in 2019, 49% of births occurred in the governmental sector, while 51% were in the private. 5 However, most post-natal care for patients with oral clefts is received in government healthcare facilities, where the medical team enters the codes into the NCHI database. A national-based registry system will ensure that patients from the private and public sectors are recorded directly into the registry system.
In conclusion, the study outcome is an indicator to improve patient care and customize healthcare infrastructure in the Ministry of Health. It can also provide insight for better projections of future needs. Comparing a highly homogenous group (Kuwaitis) to another from different backgrounds (non-Kuwaitis) can provide a unique epigenetic insight into a multifactorial congenital anomaly like OFC. Continuing this work is vital; it should be expanded to the Gulf Cooperation Council (GCC) countries and the region.
Footnotes
Acknowledgment
We would like to thank Dr. Ahmed M. Okasha, Head of vital and health statistics division in the National Center for Health Information, Ministry of Health, Kuwait, for valuable data and statistics that has been used in this study. This work had been funded by Kuwait Foundation for the Advancement of Sciences (Grant #17PR-13DS-01).
Data Availability Statement
The data that support the findings of this study are openly available in Central Statistical Bureau of Kuwait at [ https://www.csb.gov.kw/Pages/Statistics?ID = 6&ParentCatID = 1 ]. in Addition, other raw data were generated at National Center for Health Information. Derived data supporting the findings of this study are available from the corresponding author [LK} on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Kuwait Foundation for the Advancement of Sciences, (grant number PR17-13DS-01)