
Abstract
Objective
To investigate condylar bone density (BD) in children with craniofacial microsomia (CFM) and identify factors that contribute to early stage condylar resorption (CR) after mandibular distraction osteogenesis (MDO).
Design
Retrospective study.
Setting
Craniofacial department of a plastic surgery hospital.
Patients
Fifty-one children with CFM classified as Pruzansky IIa based on complete pre-(T0) and post-MDO (T1) computed tomography (CT) data.
Intervention and Main outcome measurements
Mimic 21.0 (Materialise Inc., Belgium) was used to measure bilateral BD and condylar height (CH) and volume (CV) of affected side. Children were split into groups based on either affected side BD or the distraction length (DL,25 mm as cutoff) .Bilateral BD was compared using a paired t-test in each group. The CH and CV of affected side at T0 and T1 were compared. The relative values of the CH and CV (CH ratio) and the volume (CV ratio) of the affected side were compared across the groups.
Results
The BD was lower on affected side than on unaffected side. Regarding BD, CH and CV decreased after MDO in group I, while the CH ratio and CV ratio of group I was lower than that of groups II and III. Regarding DL, the CV ratio was lower in Group L than Group S.
Conclusions
The condylar bone quality on affected side is compromised in type IIa CFM. A low BD in combination with a larger distraction distance may increase the risk of CR; therefore, MDO in patients with such characteristics should be postponed.
Introduction
Craniofacial microsomia (CFM) refers to a group of congenital deformities characterized by malformation or absence of structures that arise from the first and second pharyngeal arches, including the mandible, soft tissues such as masticatory muscles, orbit and ears, and craniofacial nerves. The incidence of CFM is estimated to range from 1/5000 to 1/3000 live births. CFM was classified into three types by Pruzansky and Kaban based on the severity of the malformation of the mandible and temporomandibular joint (TMJ). Previous studies have evaluated the morphology of the condyle in patients with CFM 1 ; however, its bone quality has not been well-studied.2,3
To date, only one study has focused on the bone density (BD) of the mandible in patients with CFM using cone-beam computed tomography (CBCT) from an orthodontic perspective. 3 Bone mineral density describes bone quality as the mineral content in the specific volume of bone tissue with all its structures, 4 and is widely used to diagnose general bone conditions such as osteoporosis as well as locational lesions such as TMJ disease5,6,7 Hounsfield units (HU) of multislice computed tomography (MSCT) can be used for BMD measurements.2,8 Having a more profound understanding of bone quality in CFM may deepen our understanding of this disease and assist in its diagnosis.
Mandible distraction osteogenesis (MDO) has been applied to lengthening the mandibular ramus in patients with CFM. 9 Long-term effect of MDO in children is unclear, and second-stage orthognathic at maturity is required to correct the recurring asymmetry due to insufficient growth of the affected side after MDO. The psychosocial benefits provided by the MDO make some parents opt for early MDO, despite its non-permanent effect in the long run. In clinical practice, we noticed significant condylar resorption (CR) related to the early relapse of the occlusal plane on the affected side during the consolidation phase in some patients after MDO. early-stage relapse. Condylar remodeling after MDO has not been well studied,10,11,12,13,14 and the results of experimental studies cannot be translated into the scenario in patients with deficient soft tissue and abnormal TMJ before distraction like CFM.15,16 Unlike orthognathic surgery, the risk factors for CR after MDO are poorly evaluated. Based on previous clinical studies on orthognathic surgery, 17 we hypothesize that condylar bone quality and distraction length (DL) might be causative factors related to post-MDO condylar resorption.
This study aimed to compare the bilateral condylar BD and to optimize patient selection for early MDO by discerning the risk factors for CR in patients with type IIa CFM.
Methods
Patient Selection
This study included patients admitted to our hospital between 2017 and 2022. The inclusion criteria were as follows: (1) A diagnosis of unilateral CFM, classified as Pruzansky IIa, in patients between 5 and 10 years of age. (2) Patients who received MDO treatment and had no surgical intervention of bony structure or orthodontic treatment before MDO. (3) Patients with no clinical signs or symptoms of temporomandibular joint disorder, and who had never been diagnosed with any systematic disease that could influence BD, such as hyperparathyroidism. (4) Patients without metallic artifact adjacent to the region of interest (ROI) of BD measurement. (5) Patients without moderate or severe incidents occurring after MDO. A total of 51 patients who met the aforementioned criteria were included in this study.
Surgery and Distraction Procedure
MDO was performed in patients between January 2015 and December 2022, with 6–12 months of follow-up.
Preoperative Surgical Design
All patients underwent preoperative evaluation and preparation, including facial and oral photographs, cephalometric and panoramic radiographs, computed tomography scans, three-dimensional reconstruction, and computer-aided design. A modified osteotomy line parallel to the occlusal plane was designed for each patient to avoid damaging the tooth germs and the inferior alveolar nerve, and the distraction vector was perpendicular to the occlusal plane. A unidirectional and internal distraction device (Cibei Ningbo Inc., China) was selected and placed on the mandible in a three-dimensional model. A surgical guide plate was manufactured using a three-dimensional printer with a rapid prototyping technique.
Anesthesia and Operation
The operations were performed under general anesthesia. Subsequently, distraction osteogenesis surgery was performed using a surgical guide plate. All the distractors were placed through a submandibular incision.
Distraction was initiated at a rate of 1 mm/day, 4–7 days after the first operation (latency period). The distraction phase continued until the occlusal plane was levelled by clinical evaluation and no overcorrection was performed. The overall distraction distances ranged from 13 to 40 mm according to the preoperative design. Afterwards, the distractors were left in place for 6–12 months (consolidation period). An occlusal plate designed by orthodontists was used to guide the downward growth of the maxilla. Subsequently, a second-stage operation was performed to remove the distraction device. Craniofacial MSCT was performed before surgery (T0) and before distractor removal (T1).
Treatment Outcome
Before the removal of the distractor, clinical examination imaging studies (panoramic radiography and MSCT) of the patients were performed to evaluate the treatment outcome. The newly formed bone between the distraction gap was opaque on panoramic radiographs, which indicated its good quality, and the open bite was closed or reduced compared with that at the end of the distraction phase. Facial symmetry improved after MDO. No moderate or severe complications occurred during treatment according to Verlinden’ classification. 18 Patients encountering mouth-opening limitation after distraction were instructed to perform active open-mouth training routinely, and mouth opening recovered after training.
Measurements of Variables
All patients were scanned using a PHILIPS Brilliance Nano 64-row helical computed tomography (CT) machine according to the standard scanning method. The scanning parameters were as follows: scanning voltage 120 kV, 213–298 mA, slice thickness/slice distance, 1 mm/0. 626 mm. The CT image data with a pixel matrix of 512 × 512 pixels were obtained and saved.
BD of Condylar Cancellous Bone
The BD of the condyle at a spherical region of interest (ROI) was measured using the following steps: (1) After the CT data were imported to MIMICS 21.0 (Materialise Inc., Belgium),500–2000 HU was chosen as the threshold for the bony structure mask. The holes inside the condyle were filled manually so that the mask could include all voxels of the condyle, and then a 3-dimensional model of the craniofacial bone was calculated. A cut function was used to obtain a separate mandibular model. (2) Point S was the most inferior point of the sigmoid notch, and point C was the midpoint between the internal and external poles of the reconstructed condyle. Point P was located at the posterior border of the condylar head such that a line passing through P and S was perpendicular to the posterior border of the condylar head. An oblique sagittal plane formed by S, C, and P was created and used to reconstruct the original CT image. (3) On the oblique sagittal plane, the highest point of the condyle was defined as Co (condylion), a spherical region (ROI for BD measurement) with a radius of 2 mm containing no cortical bone was placed 4 mm below the Co using Create Primitives within the software. The mean HU value of the mask of the ROI represents the density of the cancellous bone of the condyle process (Figure 1).
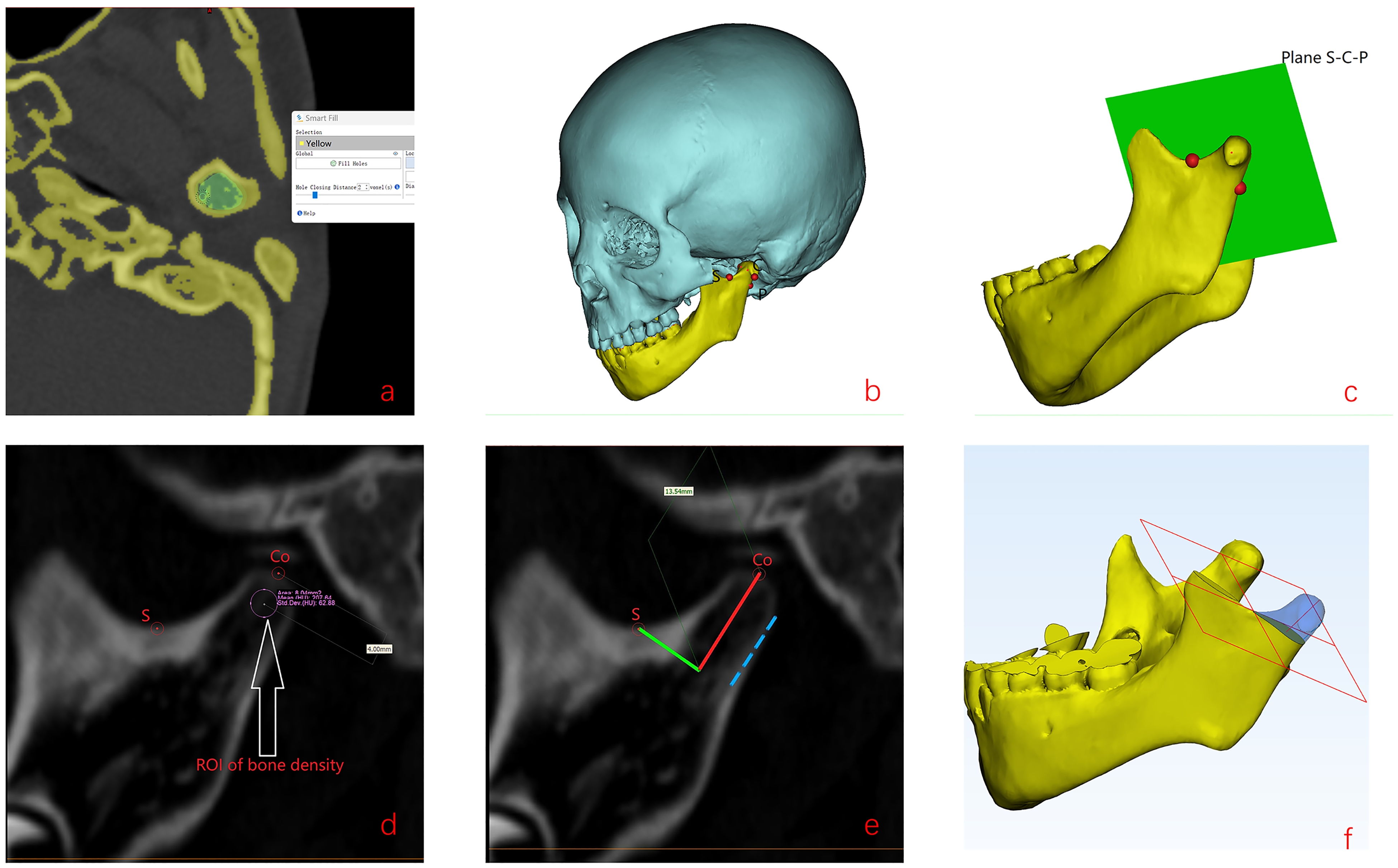
Condylar Height (CH), Volume (CV), and Ramus Height
Condylar height measurement was performed in the reconstructed plane (S-C-P, described above). A line passing Co and parallel to the posterior border (blue) of the condyle was defined as line A (red), a second line passing S and perpendicular to line A was defined as line B (green), and the distance between Co and the intersection of Line A and Line B was defined as the condylar height (CH) (Figure 1). CH was measured for both CT data at T0 and T1. A plane passing through S with line A as its normal vector was defined as the inferior border of the condyle, and cutting with this plane was used to isolate the condyle for the volume calculation. The ramus height was measured from the Condylion to Gonion in 3-dimensional mandible models, and the ratio between the affected side and unaffected side reflected the severity of mandibular ramus hypoplasia.
Grouping of Patients
By Density
The patients were divided into three groups according to preoperative BD on the affected side tertiles to investigate whether lower bone quality will predispose patients to CFM CR: Group I (the first tertile, lower bone quality), Group II (middle bone quality), and Group III (higher bone quality). A comparison of the participants’ baseline characteristics (sex ratio, age, and ramus height ratio) and treatment (distraction length) are shown in Supplemental Table 1.
By Treatment
Considering that the DL may also influence the mechanical environment of the condyle, patients were divided into a Group with DL shorter than 25 mm (Group S) and a Group with DL longer than 25 mm (Group L) to investigate the effect of DL.
Statistical Analysis
The CT data of randomly chosen 15 patients were remeasured by the first author 2 weeks after the first measurement, and the intra-class correlation coefficients (ICCs) of bilateral BD, CH, and CV were calculated to verify the repeatability of the measurement. (1) Bone density was compared between the affected and unaffected sides using a paired t-test in each group. Bone density was compared between groups using one-way ANOVA and post-hoc LSD t-test. (2) The height and volume at T0 and T1 of the condyle of the affected side were compared using a paired t-test. (3) The indices reflecting the change in condylar height (CH ratio, ratio of CH at T1 and T0) and volume (CV ratio, ratio of CV at T1 and T0) of the affected side were compared between different groups using one-way ANOVA and post-hoc LSD t-test. CH and CV were compared for both groups using density and DL. (4) To describe clinically significant CR
Results
The ICCs show excellent repeatability of the variables measured (0.898–0.959).
Baseline Comparison among Density Groups
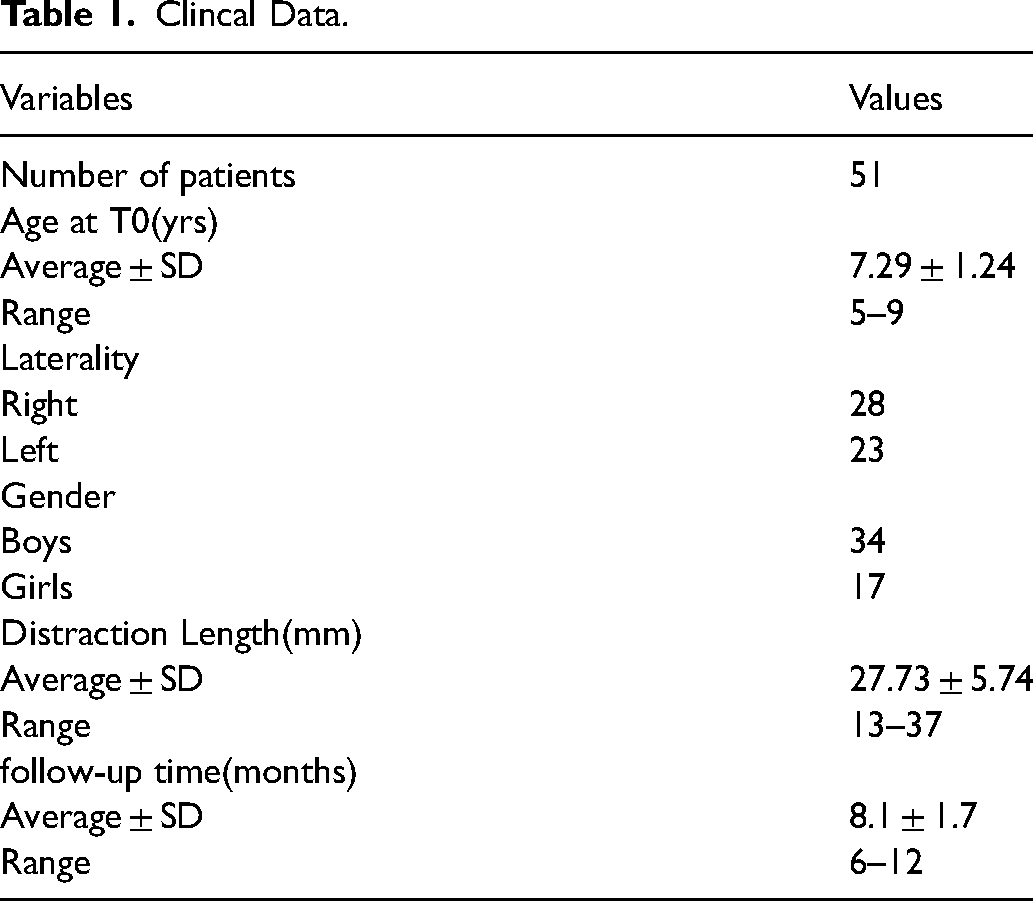
The basic information of the 51 patients is listed in Table 1. The patients were divided into Group I (n = 17, 30 HU ≤ BD ≤ 133 HU), Group II (n = 17, 134 HU ≤ BD ≤ 208 HU), and Group III (n = 17, 212 HU ≤ BD ≤398 HU). The patients in Group I had smaller ramus height ratios than those in groups B and C, while the difference between groups B and C was not statistically significant (Supplemental table 1). A negative relationship between BD and DL was found, but this did not reach statistical significance (p = 0.085).
Clincal Data.
Comparison According to Density Groups
(1) The BD was lower on the affected side than on the unaffected side in all three groups; however, the differences in BD on the unaffected side between three groups were not significant (381.29 ± 80.61 HU vs. 413.47 ± 58.12 HU vs. 420.53 ± 75.66 HU p = 0.249) (Table 2). (2) The CH and CV decreased from T0 to T1 in group I (p = 0.000, p = 0.000); however, the differences were not significant in Groups II and III (Table 3). (3) Intergroup multiple comparisons using one-way ANOVA and LSD t-test showed that the CH ratio of group I was lower than that of groups II and III (p = 0.000, p = 0.000, respectively), and the CV ratio of group I was lower than that of groups II and III (p = 0.000 and p = 0.000, respectively). However, the differences in CH and CV between groups II and III were not significant (p = 0.262 and p = 0.111, respectively). Illustrations of typical condyles at T0 and T1 for the different groups are presented in Figure 2.

Bone density of condyle in different groups.
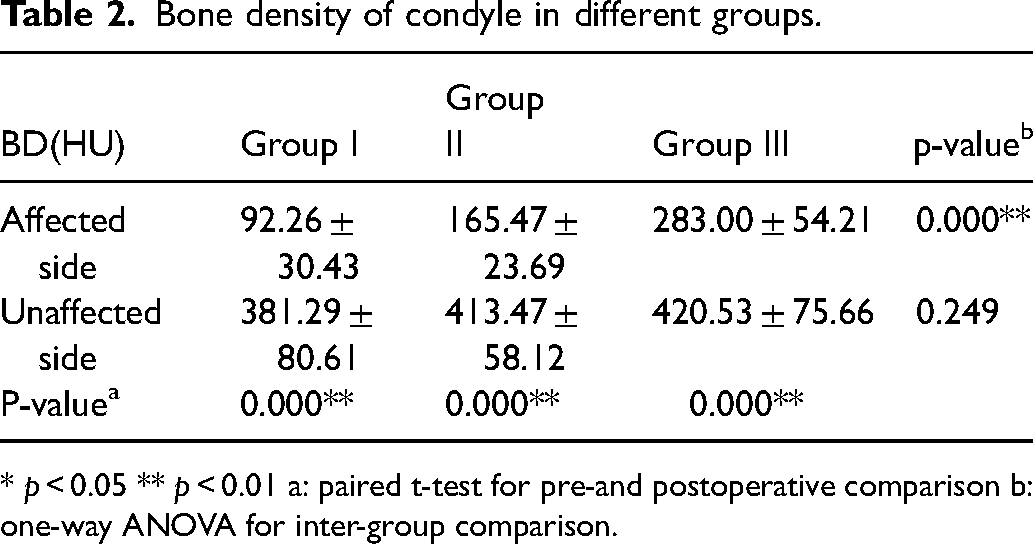
* p < 0.05 ** p < 0.01 a: paired t-test for pre-and postoperative comparison b: one-way ANOVA for inter-group comparison.
Height and volume of condyle before and after MDO in different BD groups.
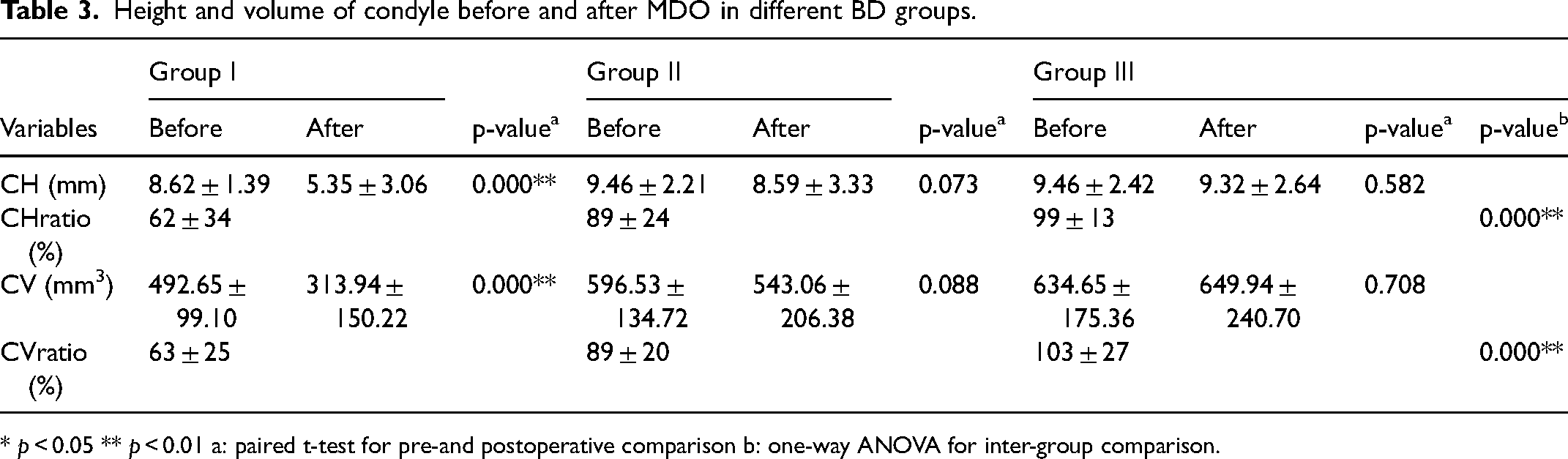
* p < 0.05 ** p < 0.01 a: paired t-test for pre-and postoperative comparison b: one-way ANOVA for inter-group comparison.
Comparison According to DL Groups: (Supplemental Table 2)
(2) the CH and CV decreased after MDO in Group L (p = 0.000 and p = 0.000, respectively). (3) The CH ratio was lower in Group L than in Group S; however, the difference was not statistically significant (p = 0.1). The CV ratio was also lower in Group L than in Group S (p = 0.001).
Incidence of SCR Across Groups (Supplemental Table 3)
Six patients met the SCR criteria. All six patients were in the group with the lowest density (Group I); one patient was in Group S, and five were in Group L in terms of DL.
Discussion
A deformed condyle on the affected side in CFM characterized by decreased height and volume has been previously reported. 1 The BD of the condyle may be related to sagittal and vertical mandible skeletal patterns, 4 and an asymmetric mandible is related to asymmetric distribution of the BD of the condyle according to a previous study. 19 There are limited studies on the BD of the condyle in patients with CFM. However, elucidation of condyle bone quality will allow us to better understand CFM.
Multislice computed tomography (MSCT) is an established clinical modality for evaluating bone quality at implantation sites. Hounsfield units obtained from MSCT represent the relative density of body tissue according to a calibrated gray-level scale. 20 In our study, we chose a spherical region below the condylar articular surface as the ROI, which is believed to be more susceptible to alterations in the mechanical environment. Our pilot test indicated that a sphere 4 mm below the condylion with a radius of 2 mm did not include the cortical bone of the condyle; therefore, we chose this spherical region as the ROI for BD measurement. Both condylar height and volume were evaluated to comprehensively reflect the morphology of the condyle.
This study only included patients who were classified as IIa. However, MDO was also performed in our center for patients classified as IIb; moreover, CR was also observed in this group of patient. The scarcity of cancellous bone in the affected condyle makes the measurement of BD difficult; therefore, patients classified as IIb were excluded from this study.
A previous study using computerized skeletal scintigraphy demonstrated that the condylar bone-seeking radiopharmaceutical uptake (BSRU) ratio on the unaffected side of patients with CFM was higher than that on the affected side. 21 Therefore, we postulated that such abnormal bone metabolism would lead to inferior condylar bone quality in patients with CFM. In this study, we found that the BD of the condyle on the affected side was inferior to that on the unaffected side in CFM, as reported by Hirschfelder. 3 However, Hirschfelder's study did not examine the Pruznaksky classification of all 16 patients, and these patients were older (7–23 years); therefore, our study aimed to evaluate the condyle BD of type IIa children. BD on the unaffected side in our study is comparable to Hirschfelder’ study (381–410HU vs. 408HU); however, the BD on the affected side in our study decreases by larger factors (4.14, 2.50, and 1.48 in group I, II, and III, respectively) compared to that in their study (1.33). The differences may mainly be explained by the different regions of BD measurement, because our study chose cancellous bone located at the head of the condyle, rather than the whole condyle in Hirschfelder's study, which is more influenced by the local mechanical environment.
Decreased Bone trabeculae and increased adipose tissues in the affected condyle should be the histological basis of the decrease in HU value in our study. The compromised condylar bone quality may be caused by genetically determined bone malformation and exacerbated by the lack of physiologic stimulation of occlusion forces and delayed dental development.22,23,24,25
The absolute indication of early DO is confined to life-threatening airway problems; however, DO has also been applied to lengthening the hypoplastic mandible in patients with CFM who seek psychological benefit. Studies have shown that MDO could fail to change the intrinsic growth pattern and should not be regarded as a permanent treatment for growing patients. 26 Our philosophy is that the benefit of psychological development must be balanced against the risk 27 and stability of MDO, that is, whether patients are prone to rapid relapse, especially those occurring during the consolidation phase. A better understanding of the relationship between preoperative characteristics and MDO outcomes is conducive to clinicians making appropriate choices. Patients with some preoperative conditions (more retrognathic mandible, smaller ramus height, larger gonial angle, and more inward ramus inclination of the affected side) may have unsatisfactory outcomes during follow-up. 28 In our practice, we found that some patients treated with early MDO had a significant relapse of the occlusal plane (> 4 °) before the removal of the distractor, remarkably expediting the recurrence of the titling occlusal plane, which will otherwise gradually regress to the original growth pattern. 29 The three sites of early relapse are shown in Supplemental Figure 1. Among these three sites, bone segment sliding and alveolar bone growth are more physiologic adaptations usually seen after MDO and can be alleviated to some extent via orthodontic treatment. However, condylar resorption is more pathological or degenerative, and SCR is uncommon after MDO (approximately 10% by estimate). Unusually high BD is found for severely resorbed condyle after MDO, suggesting potential destruction to the condyle (Figure 3), whose upward and backward adaptive growth occurring by endochondral ossification serves to increase ramus height. 30
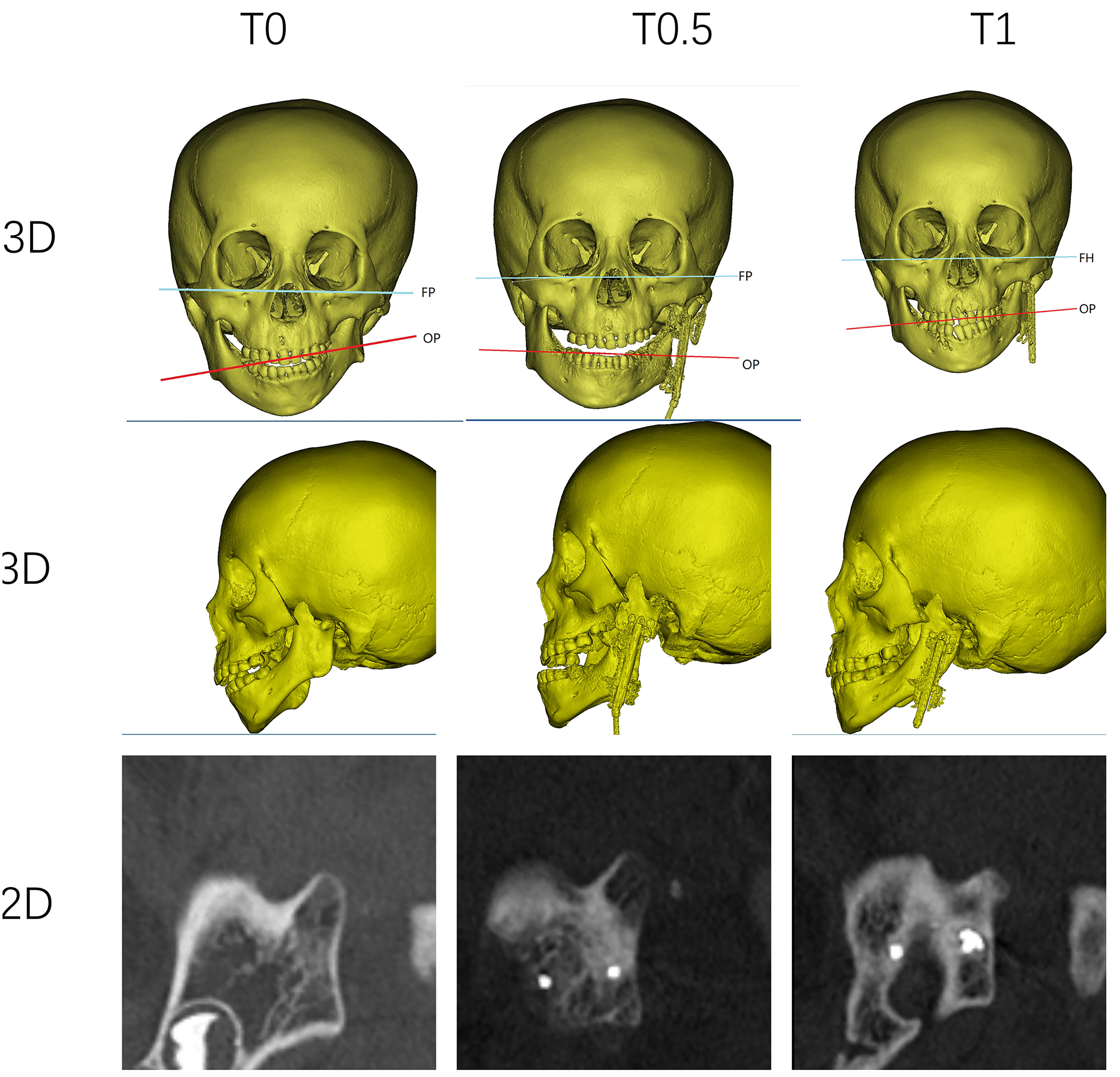
Two-dimensional views and three-dimensional images of the mandible of one patient at different stages of treatment. As shown, the condyle on the affected side becomes denser and smaller at T1. T0, preoperative, T0. 5: completion of distraction, T1: before the removal of the distractor; FP: Frankfort plane; OP: occlusal plane.
In this studyUnlike CR after orthognathic surgery, CR after MDO is rarely reported in clinical studies. Van Strijen et al. reported that the high-angle Class II patients are at higher risk of relapsing than normal or low-angle patients after bilateral mandibular distraction osteogenesis; however, this study proposed that reasons for relapse in the high-angle patient group are related to other factors (myoskeletal balance, habitual mouth posture, etc) rather than CR, 14 only one patient who sustained facial trauma developed CR after MDO.
Our study shows that as the bone quality becomes worse, the patients in Group I encountered a large amount of volume and height decrease (about 40%) after MDO, in contrast, in patients with relatively higher condylar BD, the condyle sizes remain stable or grow to some extent (99% of condylar height and 103% of condylar volume at T0). Intergroup comparison indicated that group I failed to preserve as much condylar height and volume as groups II and III, which was caused by an imbalance in bone resorption/formation influenced by multiple factors. Similar to experimental studies, we identified BD as a factor contributing to TMJ degenerative change. 31 Previous studies have demonstrated that preoperative TMJ conditions may influence the outcomes of MDO or orthognathic surgery. Fan et al. reported that syndromic micrognathia patients who suffered from more abnormalities before treatment were prone to condylar pathology and TMJ ankylosis. 13 Kobayashi et al. reported that erosions or deformities of the condyles, or both, were seen in ICR patients on three-dimensional CT performed before mandibular advancement. 32
A larger amount of distraction may increase the tension on the surrounding soft tissue and lead to greater compressive loads on the condyle; therefore, it is necessary to discern its role in CR after MDO in CFM. Our results showed that Group L lost more of its volume than those in Group S. Preoperative comparison among the groups according to BD demonstrated that the mandible was somewhat more hypoplastic in patients in Group I and consequential a larger distraction length will be required; therefore, both DL and BD are cofounders for CR, and their actual effect can only be distinguished by conducting a multivariate analysis with larger samples in the future. Some researchers support overcorrection of MDO to compensate for insufficient growth of the affected side in CFM to delay long term-relapse 33 ; however, our study suggests that it can be counterproductive by accelerating the degenerative change of condyles, especially in patients with lower condyle quality before treatment.
By defining significant condylar resorption (SCR), we aim to help clinicians focus on patients who are likely to have the worst short-term outcomes for MDO. For patients with an intercondylar distance of 100 mm, a reduction of the typical condylar height (10 mm) by 50% alone can be translated into occlusal plane relapse by 3 °(arctan (5/100)), close to the threshold for recognition of facial asymmetry (4 °). 34 Such a drastic relapse will negate the correction of MDO, and long-term stability may also be compromised, considering the deleterious effect on the condyle of MDO. The results showed that among six patients with SCR, six had a BD in the lowest tertile, five had a DL of over 25 mm, and one was less than 25 mm. Although no multivariate analysis was performed in this study, the distribution of SCR among groups suggests that lower BD in combination with longer DL is more likely to experience SCR, while higher BD allows the condyle to withstand larger distraction distance without significant resorption.
Orthognathic surgery is another treatment modality for the correction of bone deformation in patients with CFM. 35 Bilateral sagittal split osteotomy (BSSO), in combination with Lefort I (or genioplasty), is performed as the sole treatment or secondary surgery after MDO. Condylar resorption is seen after mono- or bi-maxillary operation and is related to the stability of the operation.36,17 Compared to BSSO, lengthening the mandible by distraction osteogenesis may provide some protection to the condyle by producing less force from the surrounding soft tissue. 37 Although the effectiveness of orthognathic surgery in patients with CFM was reported to be relatively stable in previous studies,38,39 it is still recommended that enough attention should be given to those who have preoperative compromised condyle bone quality and are planned for greater advancement or counterclockwise rotation, because their condyle may not tolerate the even greater stress caused by orthognathic surgery.
This study has some limitations. Our research focused on the relative short-term change of the condyle after MDO, and whether CR is progressive or self-limited requires longer follow-up. Second, many factors, such as soft tissue condition and orthodontic treatment also contribute to CR, and some of these factors are difficult to quantify, such as the compliance of patients during MDO and orthodontic treatment. Our research warns clinicians of possible compromised short-term outcomes due to condylar resorption in children with more hypoplastic ramus and lower BD; however, for children whose BD is relatively higher (>200 HU), the risk may not increase when a larger DL is planned. Thus, further studies with larger sample sizes are warranted for multifactorial analyses to comprehensively evaluate the risk factors for CR.
Conclusions
The condylar BD of the affected side was lower than that of the unaffected side in children with Pruzansky -Kaban IIa CFM. Lower BD in the affected condyle and longer distraction length in patients with Pruzansky -Kaban IIa CFM are potential factors for CR after MDO. We suggest that when preoperative evaluation indicates the need for a longer distance for children with inferior condylar BD, surgeons should defer definitive surgery until maturity or at least take the possible significant condylar resorption after MDO very seriously.
Supplemental Material
sj-docx-2-cpc-10.1177_10556656231163725 - Supplemental material for Bone Density of the Condyle of Children with Craniofacial Microsomia and its Correlation with Condylar Resorption After Mandible Distraction Osteogenesis
Supplemental material, sj-docx-2-cpc-10.1177_10556656231163725 for Bone Density of the Condyle of Children with Craniofacial Microsomia and its Correlation with Condylar Resorption After Mandible Distraction Osteogenesis by Xiyuan Li, Zhiyong Zhang, Xiaojun Tang, Chuan Li and Wei Liu in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656231163725 - Supplemental material for Bone Density of the Condyle of Children with Craniofacial Microsomia and its Correlation with Condylar Resorption After Mandible Distraction Osteogenesis
Supplemental material, sj-docx-3-cpc-10.1177_10556656231163725 for Bone Density of the Condyle of Children with Craniofacial Microsomia and its Correlation with Condylar Resorption After Mandible Distraction Osteogenesis by Xiyuan Li, Zhiyong Zhang, Xiaojun Tang, Chuan Li and Wei Liu in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-4-cpc-10.1177_10556656231163725 - Supplemental material for Bone Density of the Condyle of Children with Craniofacial Microsomia and its Correlation with Condylar Resorption After Mandible Distraction Osteogenesis
Supplemental material, sj-docx-4-cpc-10.1177_10556656231163725 for Bone Density of the Condyle of Children with Craniofacial Microsomia and its Correlation with Condylar Resorption After Mandible Distraction Osteogenesis by Xiyuan Li, Zhiyong Zhang, Xiaojun Tang, Chuan Li and Wei Liu in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-5-cpc-10.1177_10556656231163725 - Supplemental material for Bone Density of the Condyle of Children with Craniofacial Microsomia and its Correlation with Condylar Resorption After Mandible Distraction Osteogenesis
Supplemental material, sj-docx-5-cpc-10.1177_10556656231163725 for Bone Density of the Condyle of Children with Craniofacial Microsomia and its Correlation with Condylar Resorption After Mandible Distraction Osteogenesis by Xiyuan Li, Zhiyong Zhang, Xiaojun Tang, Chuan Li and Wei Liu in The Cleft Palate Craniofacial Journal
Footnotes
Ethical statement
This retrospective research was approved by the Peking Union Medical College Review Board and the Chinese Academy of Medical Sciences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the CAMS Innovation Fund for Medical Sciences (grant number 2021-I2M-1-068).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.