
Abstract
Objective
Superior Semicircular Canal Dehiscence (SSCD) is a recently-defined developmental defect may be associated with several craniofacial anomalies such as Cleft Lip/Palate (CLP). The present study aimed to compare subjects with unilateral and bilateral CLP and normal controls in terms of Superior Semicircular Canal (SSC) bone thickness and pattern.
Subjects and Methods
A total of 238 Cone Beam Computed Tomography (CBCT) images were collected from 52 unilateral Cleft Lip and Palate (UCLP) subjects (104 temporal bones) and 38 Bilateral Cleft Lip and Palate (BCLP) (76 temporal bones) subjects and 148 healthy controls (296 temporal bones). The SSC bone thickness was measured twice and validated by a maxillofacial radiologist. The samples were then classified into five categories based on bone thickness: papyraceous or thin, normal, thick, pneumatized, and dehiscence. After all, the UCLP, BCLP, and normal control groups were compared concerning the SSC pattern and thickness.
Results
The results revealed no significant difference among the three groups regarding the SSC pattern and thickness based on gender. The SSC patterns (P value = .001) and SSC thickness (0.01) were strongly correlated to the cleft type. The thinnest bone thickness and the highest incidence of SSCD were observed among the subjects with BCLP.
Conclusions
The results showed a significant association between the SSC patterns and SSC thickness and the study groups.
Keywords
Introduction
With a global prevalence of 1 in every 800 live births, 1 Cleft Lip/Palate (CLP) is the most common type of craniofacial anomaly occurring in three major forms, including medial, unilateral, and bilateral, with the last two accounting for over 99% of all cases. 2 Nevertheless, CLP is not an isolated anomaly, as it is often associated with other facial or even cerebral anomalies, leading to significant disruptions throughout the growth and development of the affected newborn. 3 CLP is associated with problems like speech disorders, dental abnormalities, eating difficulties, underdevelopment of craniofacial structures, aesthetic issues, hearing loss, psychological problems, and defects in cardiac, nervous, and ocular systems.4,5,6
Minor et al defined Superior Semicircular Canal Dehiscence (SSCD) and its complications in 1998 for the first time. 7 SSCD occurs when the bony roof of the Superior Semicircular Canal (SSC), interfacing with the floor of the middle cranial fossa, fails to thicken properly as the newborn ages. 8 Approximately 1%-2% of the general population have been predisposed to SSCD in their childhood, manifesting in the form of nystagmus, vertigo, tinnitus, and disequilibrium. 8 Furthermore, Oscillopsia, hyperacusis, aural fullness, autophony, change in the middle ear, and middle cranial pressure are the other symptoms of SSCD.9,10,11,12 In addition to vestibular and cochlear complications of SSCD, it may facilitate the spread of middle ear infections to the cranial fossa, predisposing individuals to central nervous system infections. 13
The bone complex of the maxillofacial can be affected by CLP; The facial structures near the cleft side develop later than other areas of the face, which require surgical intervention for their normal growth.14,15 The embryologic origin of orofacial structure and ear is the same; they originated from the first pharyngeal arches and pouches. 16 Therefore, this is probably the reason those hearing problems, especially conductive hearing loss related to otitis media with effusion and SSCD prevalent among CLP patients.17,18 Therefore, it is essential to assess SSCD in CLP patients.
Cisneros et al 19 proposed a classification system for the pattern of the bone based on the thickness of the SSCcanal. This classification system contains a “normal pattern” when the thickness of the bone wall that separates the SSCC from the middle cranial fossa is between 0.6 and 1.7 mm, “Papyraceous pattern” which is featured by fine thin bone covering the SSC roof where the thickness of the bone that separates the SSCC from the middle fossa is ≤0.5, “Thick pattern” where is featured by compact bone layer overlying SSCC roof was ≥1.8 mm in thickness; and “Pneumatized pattern” when the roof of the canal characterized multiple supralabyrinthine cells, exhibiting as a woven structure.
Diagnosis of SSCD is based on the presence of vestibular or auditory symptoms. Because of the complexity of the anatomical structure of the temporal bone, the exact radiological investigation is essential in the diagnosis of SSCD. Key components of the clinical diagnosis are confirmed by radiologic examination. 20 Currently, CT is an acceptable imaging technique for assessing SSCD, but it isn't a perfect one. CT cannot recognize bone thickness <0.1. Sequeira et al 12 showed that routine CT could not be the best method, especially when SSCD is correlated with low-level dehiscence. Cloutier et al 21 showed that CT over diagnosed SSCD. Tavassolie et al 22 indicated that CT overestimates the extent of SSCD. Besides, Masaki 23 concluded that 80% of SSCD diagnoses via helical CT might be false-positive. Cone Beam Computed Tomography (CBCT) is a new radiological method. Still, small voxel size, low radiation dose, high spatial resolution, rapid interoperation and display, low radiation dose, acquisition of three-dimensional (3D) data, and good quality of imaging make CBCT the method of choice for evaluating individuals suspected of SSC. 24
The prevalence of hearing problems is high among CLP subjects. 18 SSCD is the major cause of hearing diseases like otitis media with effusion. 25 Clinical manifestations and symptoms of SSCD can imitate the symptoms of other diseases, such as cerebrovascular diseases, trauma, and other otologic pathologies.10,26,27,28 Besides taking and evaluating history, and clinical and physical examination, it is essential to take radiography to differential diagnosis among numbered diseases among CLP subjects and confirm the SSCD. 29 Differential diagnosis is critical in determining the treatment plan and cause of the symptoms. Many studies suggest that the disease has advanced over the years.30,31,32
To the best of our knowledge, SSCD is a relatively newly defined type of developmental defect, and only one study has investigated its epidemiology in subjects with CLP. 33 We hypothesized that the prevalence of SSCD was higher among CLP subjects, which correlates with the cleft's severity. Therefore, the present study aimed to compare the SSC bone thickness and pattern in subjects with Unilateral CLP (UCLP) and Bilateral CLP (BCLP) and normal controls using CBCT.
Subjects and Methods
The Ethics Committee approved this study of the University of Medical Sciences (IR.SUMS.DENTAL.REC.1400.138). The study was carried out on patients’ records and CBCT images selected from the archives of a private radiology center. It should be noted that the CBCT images were not taken for this study. The CBCT images in the control group were taken for other reasons such as the dental implant, tooth impaction, the third molar extraction, etc. The randomly chosen control and case groups were selected according to inclusion and exclusion criteria. Inclusion criteria were CBCT images with a large field of view, high-quality images, the possibility of visualization of SSC bilaterally in the scanning area, and no previous history of trauma and surgery. CBCT images with low quality and small field of view, subjects with congenital syndromes, bone pathologies that may affect the craniofacial structures, and subjects using drugs that may alter bone metabolism were excluded from the study. The mean age of the participants was 21.3 + 2.6 years (age range: 20-30 years). The subjects were divided into three groups as follows: 148 subjects without CLP who served as controls (80 male, 68 female), 52 subjects with UCLP (23 male, 29 female), and 38 subjects with BCLP (16 male, 12 female). The mean age of the control group was 21.3 + 2.6 years (age range: 20-30 years). The mean age of the UCLP group was 23.1 + 1.6 years (age range: 22-31 years). The mean age of the BCLP was 24.3 ± 3.6 years (age range: 23-32 years) (Table 1). The control and the case groups were age and sex-matched.
Mean age of the Groups According to Gender.
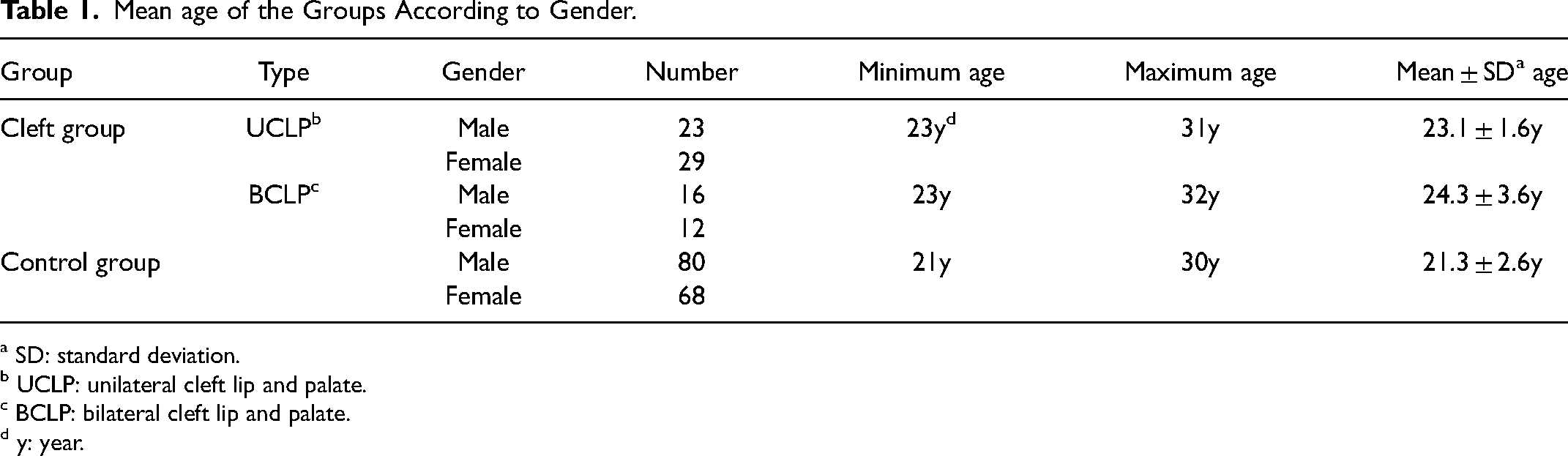
a SD: standard deviation.
b UCLP: unilateral cleft lip and palate.
c BCLP: bilateral cleft lip and palate.
d y: year.
The characteristics of CBCT were as follows: a) scanning time: 14–18 s, b) field of view: 15 × 12, c) exposure time: 5 s, d) voltage: 110 kVp, e) current: 3 mA, and f) voxel size: 0.3 mm. The images were taken using a NewTom VGi device (QR-SRL, Venora, Italy). To ensure the consistent orientation of the sagittal images, the head was placed perpendicular to the floor with the Frankfort horizontal plane. All images were analyzed using Quantitative Radiology (QR) NNT imaging software, version 2.21.
Analysis of CBCT Images
Similar to the Altun et al study, 33 the CBCT images were first taken in the axial plane. Using these images, the Pöschl plane was reformatted. The Pöschl plane ran at approximately a 45 angle to both the coronal and sagittal planes. It was specifically drawn parallel to the SSC (Figure 1A). In this plane, the SSC appears as an intact ring.
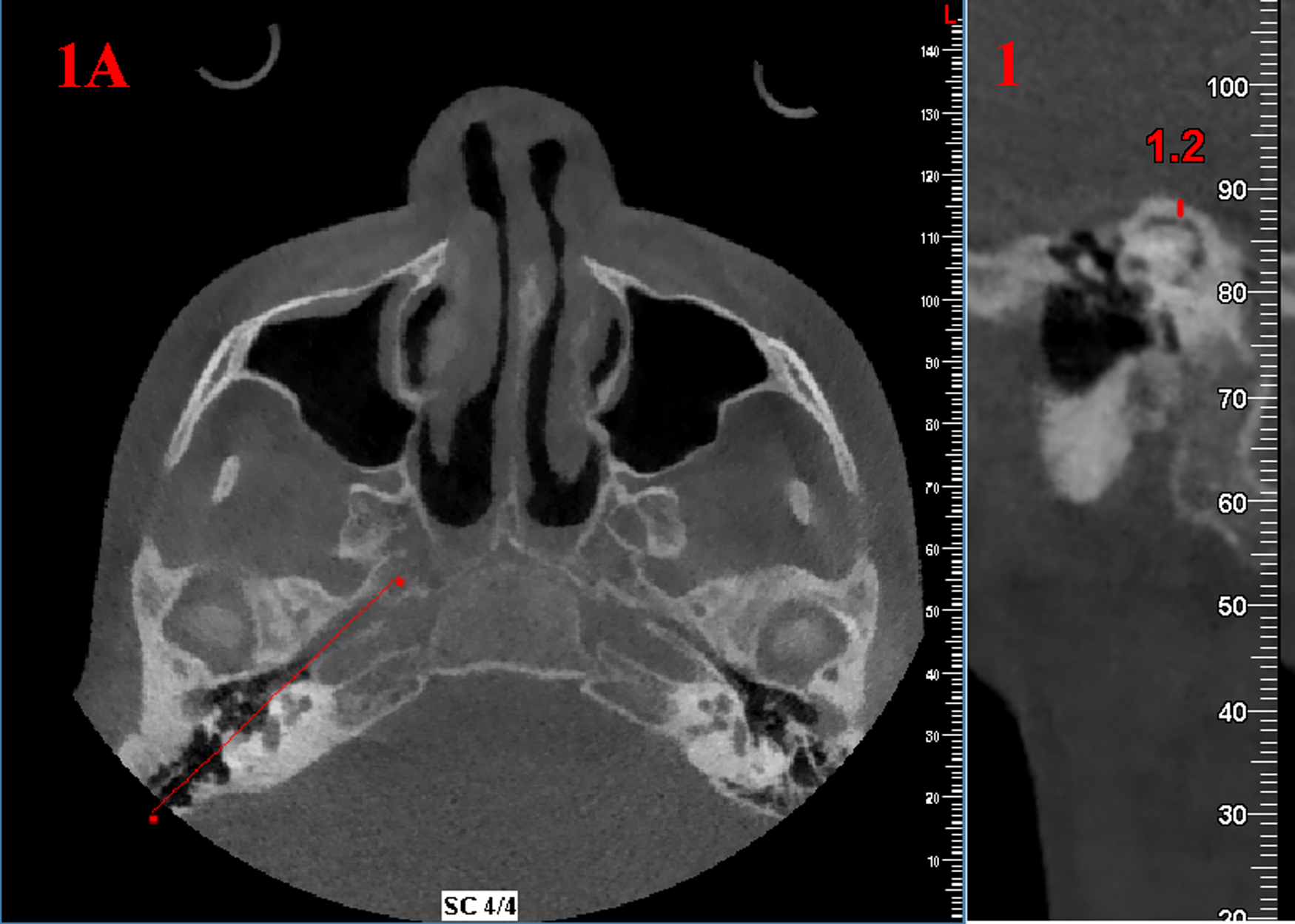
Measurement of SCC thickness in a sample patient: (A) Axial view shows the Pöschl plane. (B) Reformatted sagittal view shows the SCC thickness.
The bone thickness of SSC was measured for each CBCT image in the Pöschl plane twice with a seven-day interval by the same oral and maxillofacial radiologist with ten years of experience. The CBCT images of 50 participants were processed again by another oral and maxillofacial radiologist with nine years of experience. To determine the significance of any errors during measurements, inter and intra-observer reliability was assessed using the kappa coefficient test. The bone thickness interspersing the outer surface of SSC and the surface interfacing the middle cranial fossa were defined as the thinnest point of SSC (Figure 1B). The SSC pattern was classified into five categories as proposed by Cisneros et al 19 in 2014; ie, (a) papyraceous or thin (≤0.5 mm), (b) normal (0.6–1.7 mm), (c) thick (≥1.8 mm), (d) pneumatized, and (e) dehiscent (Figure 2).
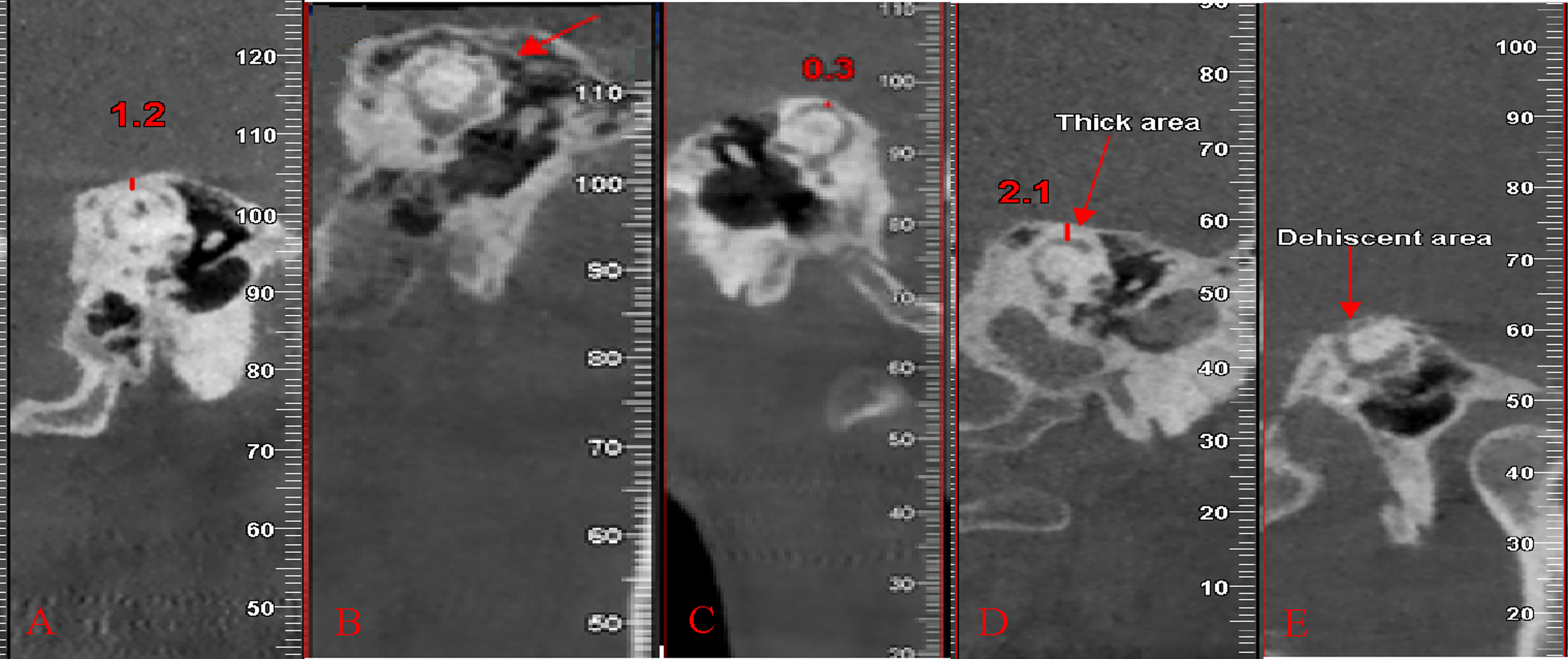
Cone beam computed tomography images indicate different radiologic features of the superior semicircular canal. (A) Normal. (B) Pneumatized (the arrowhead). (C) Papyraceous. (D) Thick. (E) Dehiscent.
Data analysis was conducted using the SPSS software, version 20. T-test was used to compare males and females concerning the thickness of SSC. Tukey's range test was also used to determine the possible significant differences among the three groups (UCLP, BCLP, and control) according to the SSC bone thickness. Moreover, the Chi-square test was employed to compare the three groups regarding the patterns of SCC. The data were also categorized into two groups, including dehiscent and non-dehiscent SSC. Fisher's exact test was used to compare the UCLP, BCLP, and normal control groups concerning the prevalence of dehiscence. Fisher's exact test was also used to compare the SSCD in the CLP and the control groups. In UCLP subjects, the cleft and non-cleft sides were compared according to pattern and thickness using Fisher's exact test and independent t-test. P < .05 was considered statistically significant.
Results
No statistically significant differences between the data obtained by double measurements were found. Therefore, the mean of the twice measurements was assessed and used for further analysis. The Intraclass Correlation Coefficient (ICC) of the two evaluations was >0.9, which proved the strong reliability of the measurements. In addition, ICC indicated strong agreement between the two observers.
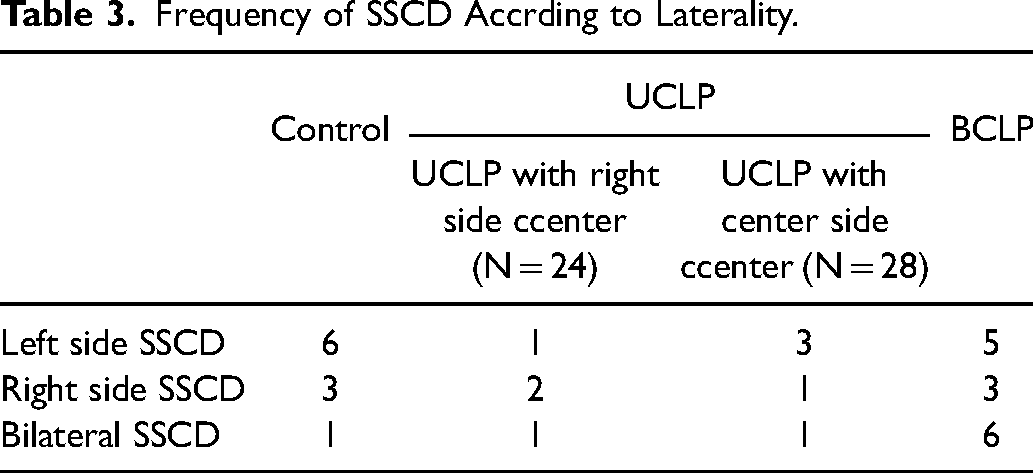
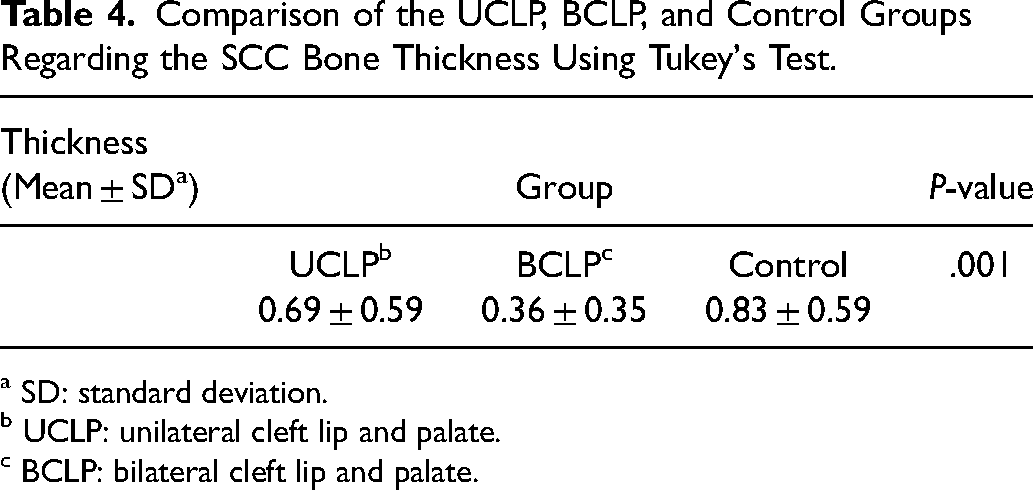
The results revealed no significant difference between males and females regarding the SSC thickness (P = .115) and pattern (P = .848) (Table 2). Unilateral SSCD was significantly higher than bilateral SSCD in the CLP groups. (P-value = .002). Furthermore, in the patients with unilateral SSCD, left-sided SSCD was significantly higher than right-sided SSCD (P value = .032). In UCLP group, the the SSCD was more prevalent in the cleft side (Table 3). The mean bone thickness was significantly lower in the subjects with CLP (0.55 ± 0.53) compared to the controls (0.83 ± 0.59). As a predictor of disease severity, the mean bone thickness was considerably lower in the subjects with bilateral CLP compared to the other two groups. Nonetheless, the mean difference between the unilateral cases and the controls was not statistically significant (Table 4).
The Comparison of Males and Females Regarding the SSC Thickness Using T-Test.
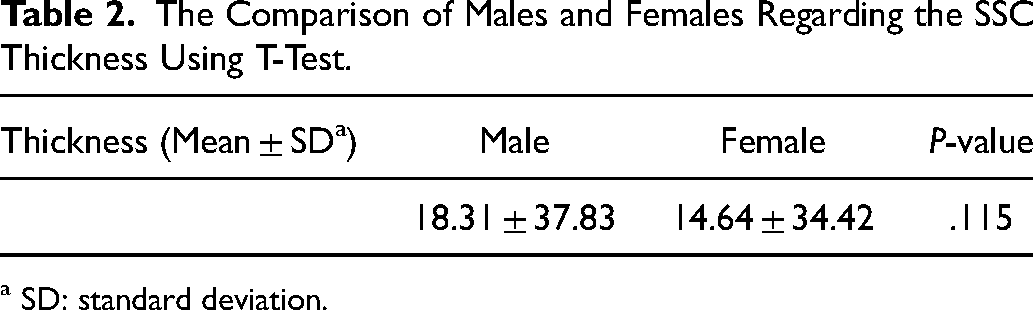
a SD: standard deviation.
Frequency of SSCD Accrding to Laterality.
Comparison of the UCLP, BCLP, and Control Groups Regarding the SCC Bone Thickness Using Tukey's Test.
a SD: standard deviation.
b UCLP: unilateral cleft lip and palate.
c BCLP: bilateral cleft lip and palate.
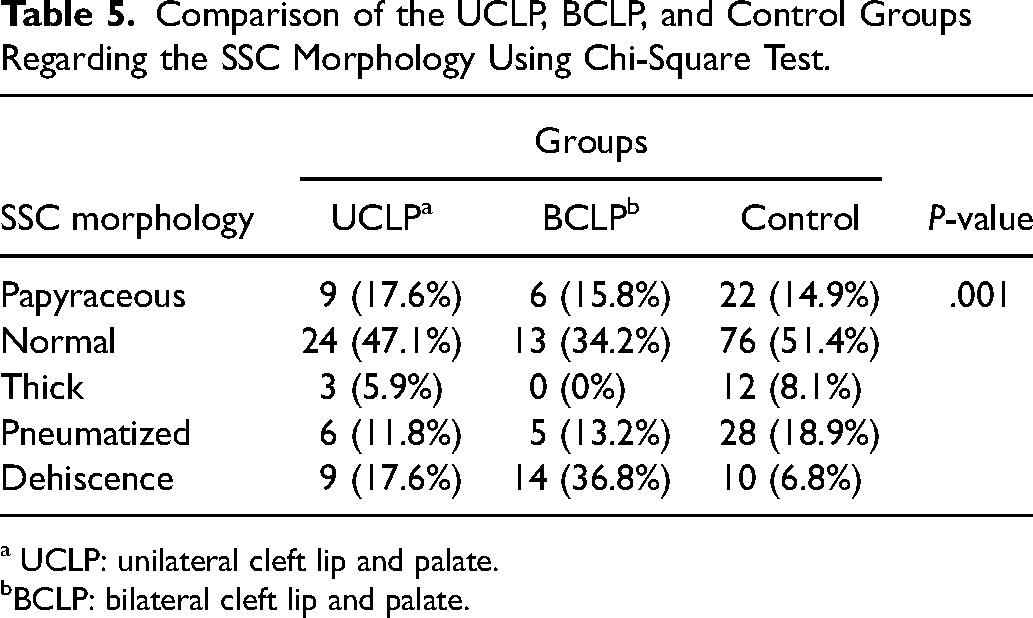
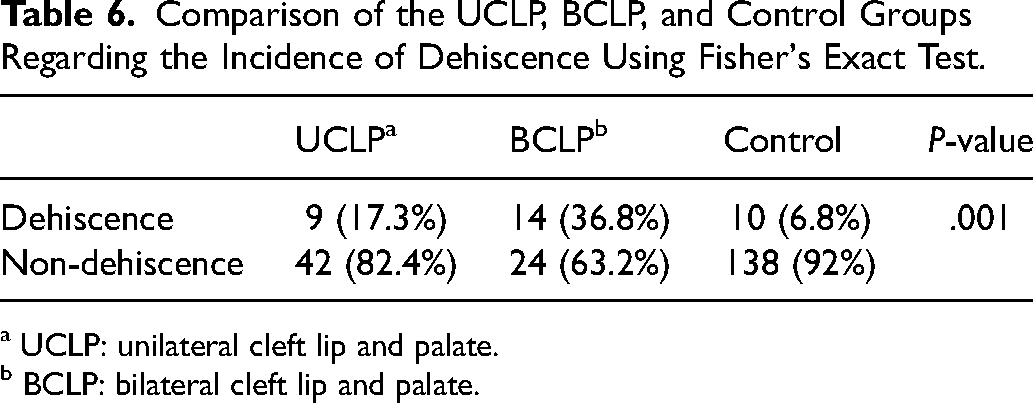
The findings showed a significant association between the SSC pattern and the study groups. In other words, a significant difference was found among the three groups regarding the SSC pattern (Table 5). Dehiscence was also significantly higher in the BCLP and UCLP groups than in the control group (P = .001 and P = .0299, respectively). However, no significant difference was observed between the UCLP and BCLP groups in this regard (P = .052) (Table 6). In subjects with UCLP, there was no significant differences between clef side and non cleft side according pattern (P-value = .175) and thickness (P-value = .976).
Comparison of the UCLP, BCLP, and Control Groups Regarding the SSC Morphology Using Chi-Square Test.
a UCLP: unilateral cleft lip and palate.
bBCLP: bilateral cleft lip and palate.
Comparison of the UCLP, BCLP, and Control Groups Regarding the Incidence of Dehiscence Using Fisher's Exact Test.
a UCLP: unilateral cleft lip and palate.
b BCLP: bilateral cleft lip and palate.
Discussion
Many diseases, such as vestibular diseases, cerebrovascular diseases, trauma, and tumors, may cause symptoms seen in SSCDS. When these symptoms occur, the patient should be evaluated with anamnesis, physical examination, and radiological examinations should be performed if necessary. Differential diagnosis is essential in understanding the cause of the symptoms and planning the treatment. Studies argue that the syndrome and symptoms do not show progression, but other studies propose that the disease progresses over the years30,31,32 Complaints may be prevented by surgical or symptomatic treatment (tympanostomy tube, diuretic therapy) in patients diagnosed with SSCD. The present study aimed to compare the SSC bone thickness and patterns in subjects with UCLP and BCLP and normal controls using CBCT. Evlice et al 34 also used CBCT images and reported that the SSC bone thickness was 1.079 ± 0.8 mm in females and 0.952 ± 0.6 mm in males. The mean SSC thickness was also found to be 1.25 mm in the research carried out by T.kaur et al 35 Similarly, the median bone thickness was 0.71 mm in the study by Mahul et al 36 In the present study, the mean bone thickness of SCC was 0.83 ± 0.59 mm in the healthy controls, which was close to the values reported in the previous studies.
The current study showed that gender was not significantly related to the SSC bone thickness and pattern. Similarly, some previous studies revealed no significant differences in the SSCD thickness based on gender.34,35,36,37 For instance, Evlice et al 34 and Altun et al 33 reported no significant differences between males and females regarding the SSCD patterns. However, Crovetto et al 38 and Karimnejad et al 39 referred to a significant female predominance for semicircular canal dehiscence. They stated that this sexual dimorphism might be attributed to women's predisposition to seek more medical care and temporal variances in growth and sex hormones.
Previous studies showed different rates of SSCD ranging from 3.3% to 16.5%9,33,34,40,41,42,43,44 The differences in the incidence of SSCD might be related to the differences in slice thickness and imaging modality. Many studies used CT imaging to analyze SSC characteristics.9,21,38,45,46,47 However, CT scans cannot detect bone layers with lower than-0.1 mm thicknesses. Masaki et al 23 revealed a high rate of false positive SSCD cases when CT alone was utilized in diagnosis. Sequeira et al 12 consistently indicated that a CT scan could not be used as a gold standard when SSCD was related to low-level dehiscence. CBCT has been widely accepted as the appropriate diagnostic technique for SSCD because of its smaller voxel size and high spatial resolution. 42 CBCT technique facilitates image-taking in standing and sitting positions.48,49 It diminishes time and dose of exposure in addition to approving three-dimensional (3D) image interpretation and reconstruction.50,51 Bremke et al 52 disclosed that CBCT was better than CT in identifying the thin bone layer of the SCC roof in the temporal bone. CBCT has a higher spatial resolution in comparing CT. Therefore, CBCT was used in the present study to evaluate the SCC thickness and pattern. Previous studies suggested that CT imaging might overestimate the SSCD prevalence.21,22,23,45 The studies that applied CT for the incidence of SSCD demonstrated a higher incidence of SSCD than those that used CBCT. In the research conducted by Kurt et al, the incidence of SSCD was approximately 6.28% in CBCT images, which was in agreement with the findings of the present investigation in the control group (6.8%).
The present study showed a significant difference between the CLP and the control groups concerning the SSC thickness and SSCD patterns. In the same line, Altun et al 33 reported significant differences between the CLP and control groups regarding the SSC pattern. Orofacial structure originates from the first pharyngeal arch. Similarly, the external and middle ear are derived from the first and second arches and pouches. 16 Therefore, there may be abnormalities involving the face and ears simultaneously because of their similar embryonic origin. According to a study by Kuo et al, developmental anomalies in the craniofacial skeleton of children with CLP could predispose them to otitis media and hearing loss. 53 Moreover, one of the most important causes of hearing loss is SSCD, which occurs more in CLP subjects than in normal individuals. 33
Unilateral SSCD was significantly higher than bilateral SSCD in the CLP groups. Furthermore, in the patients with unilateral SSCD, left-sided SSCD was significantly higher than right-sided SSCD. In the same line, Sugihara et al 54 indicated that the incidence of unilateral SCCD was 71.0% and bilateral SSCD was 29.0%. Similarly, Karimnejad et al 39 reportd that left-sided SSCD was most prevalent, followed by right-sided then bilateral. They proposed this hypothsis that these signicant diffrences among SSCD laterality may be because of gross morphological size differences between the right and left cerebral hemispheres.Increasing in the brain size result in amplification of intercranial brain pressure which cuases erosion in bony tegmen in the dehiscence area.A study conducted by Goldberg et al 55 showed that lateral superior temporal gyrus in left hemisphere was larger in compared to right side. Therefore, the mrhological diffrences may be the reason of higher incidence of left- sided SSCD.
This study had some limitations. The FOV of the images used in this study was high. Therefore, the resolution decreases and creates problems in SSC dehiscence analysis. Furthermore, this investigation was a retrospective study, so we did not have access to the subjects’ clinical manifestations and symptoms of SSCD. Yet, future studies are recommended to confirm the present study results.
Conclusions
The present investigation delivers considerable insights into the association between CLP and SSCD thickness and the distribution of different patterns of SSC among subjects with CLP and healthy individuals, which was related to cleft type.
Footnotes
Acknowledgments
The authors would like to thank Ms. A. Keivanshekouh at the Research Consultation Center (RCC) of Shiraz University of Medical Sciences for her invaluable assistance in editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.