
Abstract
Objective
To identify characteristics of malpractice litigations involving skull deformity in infants (craniosynostosis and deformational plagiocephaly).
Design
Retrospective review of all lawsuits with jury verdicts or settlements involving infant skull deformity as the primary diagnosis using the Westlaw Legal Database.
Setting
United States.
Patients, Participants
Plaintiffs with skull deformity as the primary diagnosis.
Main Outcome Measures
Litigation outcome and indemnity payment amount.
Results
From 1990 to 2019, 9 cases involving infant skull deformity met our inclusion/exclusion criteria. Among these cases, 8 (88.9%) cases resulted in indemnity payments to plaintiffs, totaling $30,430,000. Failure to diagnose (n = 4, 44.4%) and surgical negligence (n = 3, 33.3%) were the most common reasons for litigations.
Conclusions
There were a small number of malpractice lawsuits involving infant skull deformity over three decades. When cases go to court, physicians and hospitals have a high likelihood of judgment against them, frequently resulting in high indemnity payments.
Introduction
According to recent data, physicians in the United States face a 7.4% annual risk of medical malpractice litigation. 1 Due to the relative complexity of the United States legal system, health care providers are often unaware of the logistics of malpractice lawsuits until faced with litigation. 2 In medical malpractice claims, plaintiffs (ie, patients or their families) must demonstrate that defendants (ie, healthcare providers, hospitals) failed to adhere to their legal duty of providing the standard of care, resulting in injuries and damages to the plaintiffs.2,3 Malpractice litigations are financially and psychologically burdensome to physicians regardless of outcomes and may negatively affect well-being and clinical practice, including a tendency to practice defensive medicine.4,5 Unfortunately, defensive medical practice shifts the physician's focus away from the patient and promotes unnecessary utilization of healthcare resources, 6 costing up to $46 billion annually in the United States. 7 Thus, understanding factors associated with malpractice lawsuits is imperative.
Malpractice suits related to early pediatric pathologies may involve medical providers (eg, pediatricians, primary care physicians) or surgical providers (eg, craniofacial surgeons, neurosurgeons, pediatric surgeons). Among these, nearly 80% of litigations posed against medical providers are due to delayed or missed diagnoses, while nearly half against surgeons are due to surgical complications. 8 Across medical disciplines, the majority of malpractice cases (78%) are ruled in favor of defendants, while remaining cases require indemnity payments to plaintiffs. 1 However, craniofacial surgeries have reportedly been associated with lower rates of defendant verdicts and higher amounts of indemnity payments when compared to the overall medical malpractice landscape. 9 Historically, fewer than half of litigations involving craniofacial surgeries were ruled in favor of defendants, and the median payment to pediatric plaintiffs was $1.2 million, 9 which far exceeded the mean indemnity payment of $365,503 across all medical specialties in 2015. 10
In the craniofacial surgery literature, factors specific to outcomes of infant cranial deformity lawsuits have not yet been reported. Early diagnosis of skull deformity and subsequent treatment are critical to minimizing sequelae, which may include developmental delay, visual disturbances, or neurologic deficits. 11 In turn, failure to manage such deformities in a timely manner could contribute to litigation risk for physicians treating pediatric patients. In this study, we aimed to describe the outcomes, indemnity payments, and characteristics of malpractice litigations involving synostotic and non-synostotic skull deformity.
Methods
Study Design and Patient Population
We utilized the Westlaw Legal Database (Thomson Reuters, NY), an online legal research service compiling the results from over 40,000 legal databases, which is widely used to study malpractice litigations across various fields of medicine.12,13 Because the Westlaw dataset is publicly available upon subscription, this study met criteria for Institutional Review Board exemption, and the ethical/consent statement was not applicable and not needed. We queried the database using Stedman's Medical Dictionary Codes of infant skull deformity and its subclasses to identify lawsuits with jury verdicts or settlements (
Search Terms for Malpractice Litigations Involving Infant Synostotic and Non-Synostotic Skull Deformity.
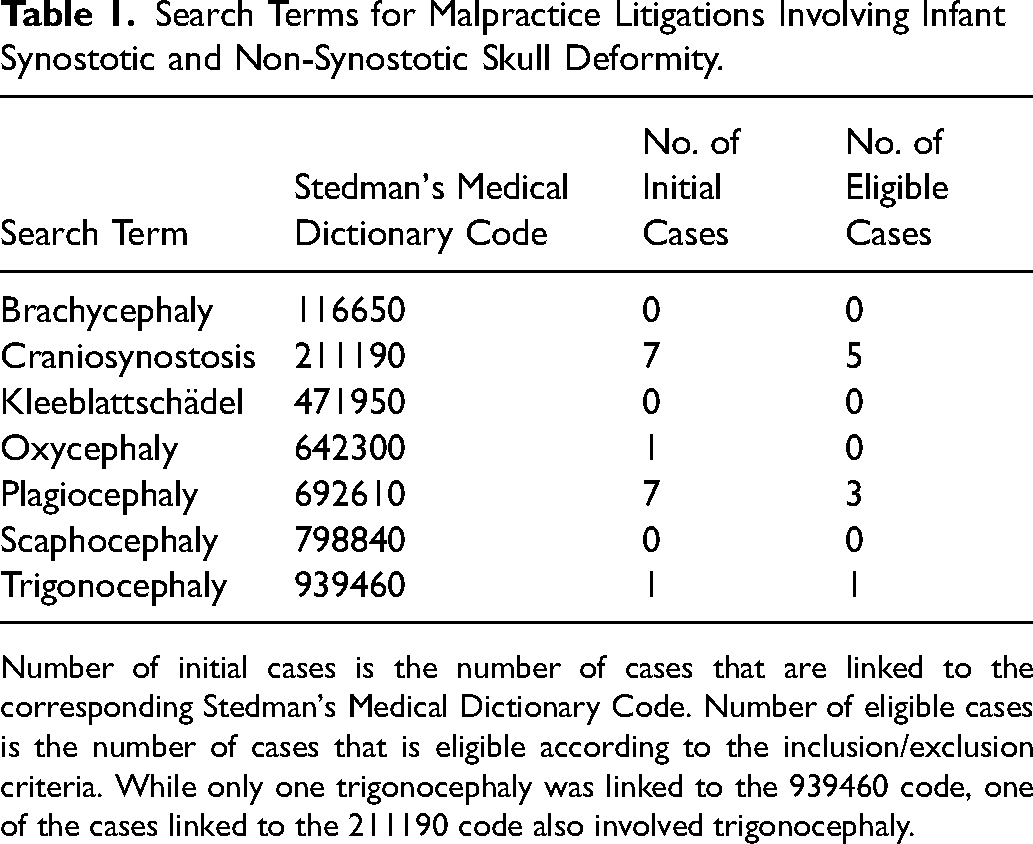
Number of initial cases is the number of cases that are linked to the corresponding Stedman's Medical Dictionary Code. Number of eligible cases is the number of cases that is eligible according to the inclusion/exclusion criteria. While only one trigonocephaly was linked to the 939460 code, one of the cases linked to the 211190 code also involved trigonocephaly.
Variables and Statistical Analysis
We collected plaintiff demographic and clinical characteristics (age, sex, type of deformity), litigation characteristics (year of trial or settlement, state of jurisdiction, court level, presence of expert witnesses), defendant types (physician and/or hospital), trial outcomes (defendant or plaintiff verdict versus settlement), and indemnity payments to plaintiffs. We also identified alleged reasons for litigation and plaintiff reported injuries. To characterize descriptive data, we calculated frequencies and proportions for categorical variables, as well as median and range for continuous variables. For cases that resulted in indemnity payments, we categorized the cases by the primary alleged reasons (eg, delayed diagnosis, surgical negligence) for litigation. For each alleged reason, we described the type of skull deformity, outcome (plaintiff verdict vs. settlement), defendant type, and indemnity payment. We also identified the associated primary injury and secondary reasons for litigation.
Results
We identified 15 litigations spanning 7 Stedman's Medical Dictionary Codes related to infant skull deformity (
Characteristics of Malpractice Litigations Involving Infant Synostotic and Non-Synostotic Skull Deformity.
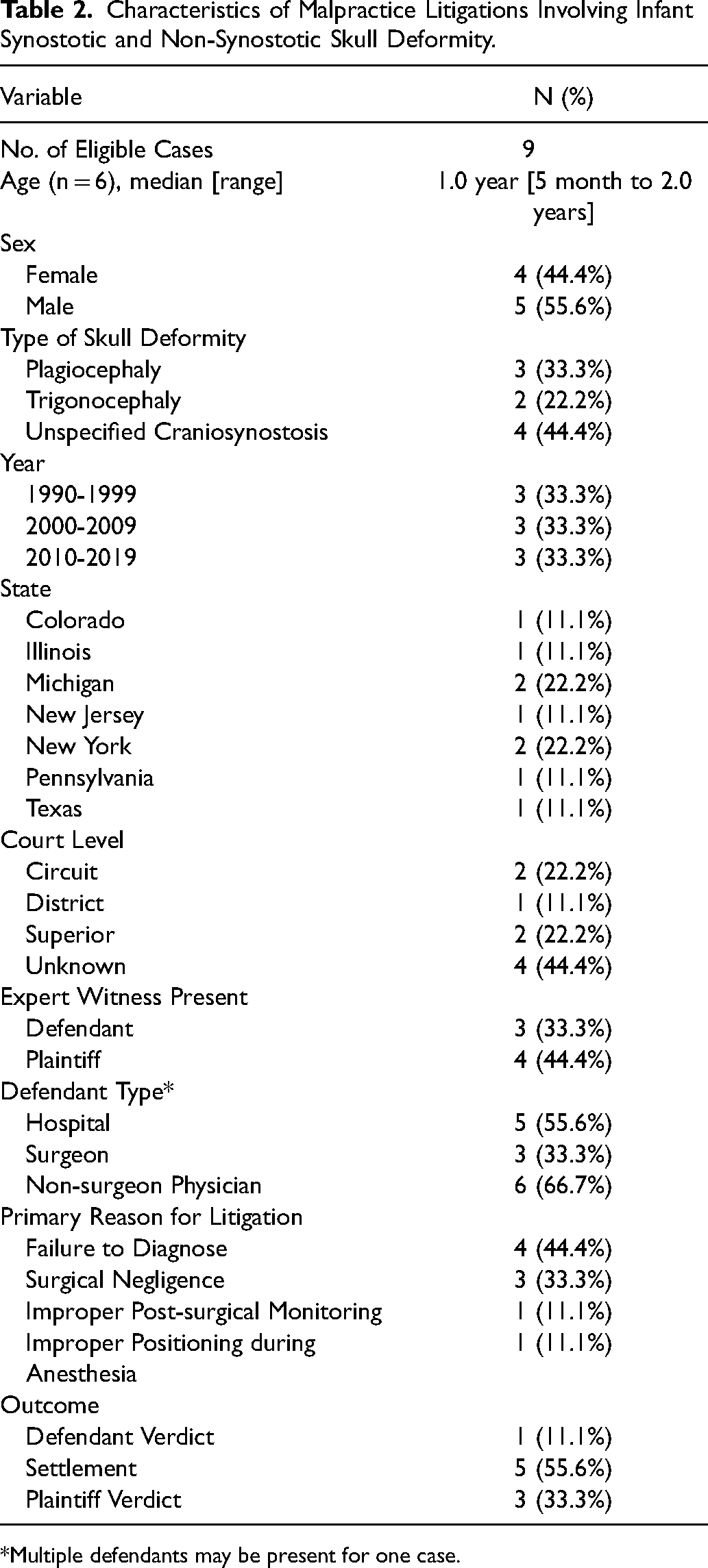
*Multiple defendants may be present for one case.
Among malpractice litigations relating to skull deformity, 1 (11.1%) case resulted in defendant verdict, 3 (33.3%) cases were ruled in favor of plaintiffs, and 5 (55.6%) cases resulted in settlement. The total amount of indemnity payments for the 8 cases was $30,430,000 (range: $25,000 to $16,300,000) (
Indemnity Payments Across Primary Alleged Reasons for Litigation.
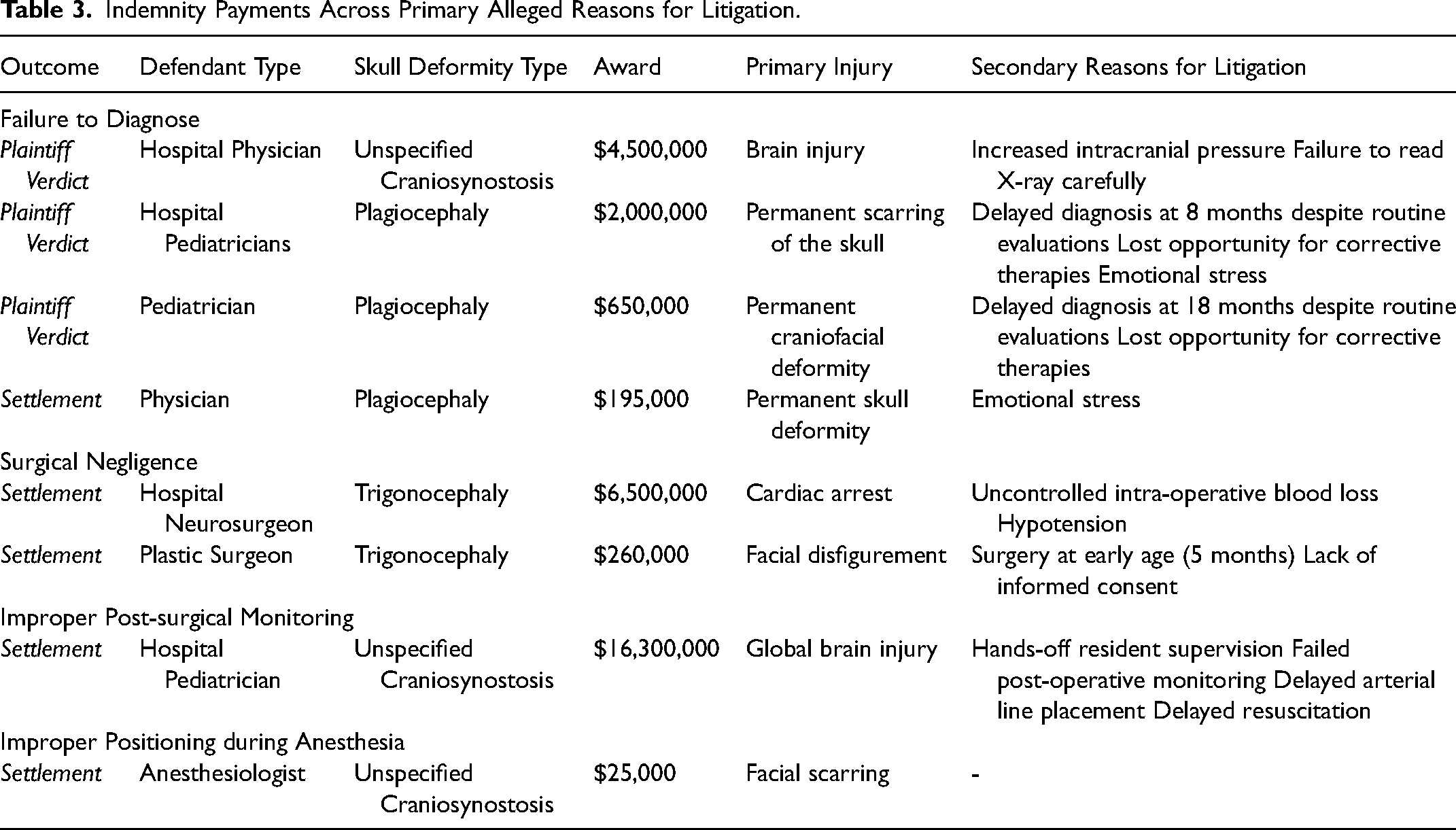
Rates of indemnity payments were 100% (n = 3) for plagiocephaly cases and 83.3% (n = 5) for craniosynostosis cases. Awards for plagiocephaly cases ranged from $195,000 to $2,000,000 (median: $650,000). Awards for craniosynostosis cases ranged from $25,000 to $16,300,000 (median: $4,500,000). Rates of indemnity payments were 66.7% (n = 2) for cases involving surgeons as defendants and 100% (n = 6) for cases without surgeons as defendants. Payments for cases involving surgeon defendants ranged from $260,000 to $6,500,000 (median: $3,380,000). Payments for cases involving non-surgeon defendants ranged from $25,000 to $16,300,000 (median: $2,325,000).
The highest indemnity payment of $16,300,000 was issued as a settlement for an alleged case of improper post-surgical monitoring. After the plaintiff underwent operative management for craniosynostosis, the defendant physician failed to properly supervise resident physicians and monitor post-operative laboratory values. This led to delayed placement of an arterial line and resuscitation, resulting in avoidable global anoxic brain injury. The case with the second highest indemnity payment of $6,500,000 involved failure to control intra-operative blood loss, hypotension, and eventual cardiac arrest during an anterior cranial vault reconstruction with bandeau advancement for metopic synostosis. In this case, the plaintiff counsel alleged that surgical negligence led to intraoperative complications and an increase in operative time of two hours.
Among litigations due to failure to diagnose, one case with a $4,500,000 indemnity fee involved brain injury and resultant cognitive and behavioral deficits. In this case, the defendant physician inadequately evaluated the plaintiff's imaging and, therefore, failed to consider a diagnosis of craniosynostosis. The plaintiff team alleged that failure to diagnose led to delayed operative intervention, resulting in consequent brain injury. In another case with a $2,000,000 award, four pediatricians evaluated the plaintiff in the first eight months of life. The first pediatrician (plaintiff age, 4 months) raised suspicion for deformational plagiocephaly and recommended altering sleeping position without initiating further management (eg, orthotic helmet). The second and third pediatricians (plaintiff age, 5-8 months) failed to diagnose plagiocephaly during seven well-child visits. The last pediatrician (plaintiff age, 7 months) evaluated the plaintiff for ear infection, but failed to address plagiocephaly until follow-up visit (plaintiff age, 8 months). During this visit, the pediatrician determined that the plaintiff had a severe skull shape deformity. Surgery for this condition eventually resulted in permanent scarring of the scalp and emotional distress. The plaintiff team alleged that such an outcome could have been avoided with appropriate diagnosis and timely intervention.
Discussion
Our retrospective review of 9 medical malpractice litigations involving synostotic and non-synostotic infant cranial deformity identifies several key findings. First, cases involving deformational plagiocephaly are exceedingly rare, and few resulted for surgical negligence. Second, while most cases of medical malpractice result in a defendant verdict in general, the inverse is found in skull deformity cases. Indeed, nearly all legal suits undergoing litigation (88.9%) required indemnity payments due to settlement or plaintiff verdict. Third, despite the small number of cases, malpractice lawsuits involving skull deformity, on average, resulted in indemnity payments which are significantly higher than in other areas of medical practice. Finally, failure to diagnose and surgical negligence were the most common primary reasons for lawsuits.
In the United States, the estimated incidence of craniosynostosis ranges from 4110 to 6155 live births per year. 15 Using the Healthcare Cost and Utilization Project's National Inpatient Sample, a large nationwide database of inpatient services, Wu et al. reported that 22,916 patients underwent open cranial vault surgeries for craniosynostosis from January 2007 to December 2014, resulting in nearly 2900 cranial vault surgeries performed annually. 16 Compared to the incidence of craniosynostosis and estimated surgical volume, there were an exceedingly small number of reported malpractice litigations. While 29,000 cranial vault surgeries are estimated to be performed each decade, we identified three cases of litigation (0.01%) involving infant cranial deformity every ten years. Among these cases, only three lawsuits over the study period (0.003%) had a surgeon as defendant. Thus, the risk of undergoing litigation among physicians, especially surgeons, who care for this patient population remains extremely low.
There are several possible explanations for the low allegation risk. First, there are notable physical exam findings (eg, abnormally shaped skull, palpable bony ridge at the prematurely fused suture) and other syndromic features (eg, congenital abnormalities in hands and feet observed in Pfeiffer and Apert syndromes) which quickly raise clinical suspicion for craniosynostosis.17–19 Further, health care providers can often definitively diagnose craniosynostosis with imaging (eg, computed tomography, X-ray films, and ultrasound). 20 Importantly, parents and caregivers play a central role in prevention and early diagnosis of non-synostotic skull deformities. Parents can identify abnormal head shapes of their children and raise concerns during well-child visits. Furthermore, parent education regarding infant positioning is a simple, cost-effective primary prevention method to avoid positional skull deformity.21,22
The defendant verdict rate in skull deformity lawsuits was significantly lower than established rates across other fields of medicine. While previous studies report that 78% of all medical malpractice cases 1 and 39% of cases involving pediatric surgical conditions 8 were ruled in favor of defendants, we found that only 11% of litigations involving infant skull deformity were ruled in favor of defendants. Thus, although the risk of lawsuits involving infant cranial deformity is extremely low, once legal action has been undertaken, physicians or organizations are much more likely to pay substantial sums of indemnity payment.
Failure to diagnose was a common allegation (44.4%) among skull deformity lawsuits. Importantly, a previous study reported that 46.9% of litigations relating to pediatric surgical conditions more generally involved delayed or missed diagnosis as the primary reason for lawsuit. 8 In cases with failure to diagnose, cranial deformity was not diagnosed despite routine evaluation, missing the window of conservative management for deformational plagiocephaly (ie, orthotic helmet) or ideal times for surgical intervention. One of these cases eventually required surgical intervention for deformational plagiocephaly due to late presentation. This could have been avoided with timely institution of helmet therapy. Currently, surgery is not recommended for positional plagiocephaly except in cases of severe cranial deformity refractory to non-operative management. 23 Litigations involving infant skull deformity could be avoided with efforts for early diagnosis at the provider level. When pediatric providers detect physical exam findings concerning for isolated or syndromic craniosynostosis, they should immediately refer patients to a center with a craniofacial team for further radiographic evaluation and subsequent treatment.11,24 At the organizational level, primary and secondary care sectors are recommended by the Working Group on Craniosynostosis to implement guidelines with illustrations of skull deformities so that healthcare workers across different training backgrounds are able to recognize craniosynostosis. 24 Providing a structured education program to infant care team members (eg, midwives, obstetricians) regarding craniosynostosis is also recommended. 24 These implementations could facilitate the workflow of diagnosis and referral of craniosynostosis and minimize the risk of legal indemnity.
Surgical negligence was another reason for litigation and has been widely cited as a key risk factor for surgical malpractice in medicolegal literature.4,9,12,13 Given that nearly 2900 cranial vault surgeries are performed each year, 16 a surgeon's risk of being sued remains extremely low. However, those who face legal action for surgeries for infant skull deformity are likely subjected to a substantial financial burden. Surgeons, in particular, must be vigilant to optimize safety both during and after an operative procedure. Failures in appropriate monitoring of intraoperative blood loss and resuscitation were particularly notable among the reasons for the initiation of lawsuits against surgeons. As an aside, prior studies have reported a decrease in malpractice claims and resolution of medical error events after implementing institution-level medical error disclosure programs.25–27 Therefore, if surgical error does occur, institutional guidelines for disclosing these errors ought to be followed.
Our study had several limitations. First, we were constrained by a small sample size. For this reason, our study is descriptive in nature. In the plastic surgery literature, 93% of plastic surgery malpractice cases are dismissed or settled before filing. This trend in the malpractice industry could have contributed to the small sample size in our study. 4 Regardless, as our search included both synostotic and non-synostotic skull deformities, our query was comprehensive of all the relevant cases. Second, certain case descriptions did not clearly differentiate whether plagiocephaly was due to craniosynostosis or positional deformity. Thus, these two diagnoses are not easy to tease apart, based upon available legal documentation. Regardless of pathophysiology, early diagnosis and involvement of a multidisciplinary team is important to achieve the greatest possible patient outcome and avoid lawsuits. When surgical intervention is indicated, appropriate cardiovascular monitoring and resuscitation appear paramount to patient safety and the avoidance of litigation.
Conclusions
In our review of all medical malpractice litigations with synostotic and non-synostotic deformities in infants as a primary diagnosis, most cases resulted in indemnity payments to the plaintiff side, as high as $16.3 million. Failure to diagnose and surgical negligence were the two most common reasons for allegation. Implementation of craniosynostosis-specific diagnostic and referral guidelines, aggressive intraoperative monitoring and resuscitation during surgery, and transparency in medical error disclosure may help minimize the risk of malpractice claims.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical/Consent Statement
Not applicable and not needed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Prior Presentations
None.