
Abstract
Objective
Posterior cranial distraction (PCD) is a surgical technique to address craniosynostosis, especially in syndromic patients. The technique has the ability to significantly expand the cranium, while requiring minimal dural dissection, compared to cranial remodeling. Our goals were to determine the patient characteristics and surgical outcomes of PCD. The two questions that we sought to answer were: 1) What is the average published complication rate and the most common complications of PCD? and 2) How much intracranial volume expansion can one expect with PCD?
Design
A PubMed database search of articles on PCD was performed. Case reports and articles with overlapping patients were excluded. A systematic review was performed using the remaining articles.
Main Outcome Measures
Patient data were extracted in order to determine the total number of patients, patients with a syndrome, types of syndromes, mean age at surgery, mean distraction distance, mean increase in intracranial volume, and complications.
Results
18 articles representing 325 patients were analyzed. A syndrome was present in 68.6% of patients. The mean age at time of surgery was 22.1 months. Mean distraction amount was 24.7 mm. Mean increase in intracranial volume was 253.2 cm3. The overall complication rate was 32.2%, with the most common complications being surgical-site infection, hardware-related complications and delayed wound healing.
Conclusions
PCD is a powerful technique in the management of syndromic craniosynostosis, although complication rates are significantly higher than traditional remodeling techniques. Future studies should compare the effects of supratorcular and infratorcular osteotomies on intracranial volume, cosmesis and complications.
Keywords
Introduction
Craniosynostosis is the premature fusion of one or more cranial sutures. The incidence of nonsyndromic craniosynostosis is 1/1000 births, while the incidence of syndromic craniosynostosis is 1/2500 births. 1
Surgery has been the established treatment for craniosynostosis since the late nineteenth century. 2 The surgical treatment of craniosynostosis has evolved over the past century, and now includes open remodeling, minimally-invasive suturectomies with spring placement or postoperative helmet therapy, and distraction osteogenesis.
First described in 2009 by White et al., 3 posterior cranial distraction (PCD) affords the ability to progressively expand the posterior cranial fossa, thereby stretching the soft tissue and minimizing the risk of relapse. PCD involves limited epidural dissection, thus allowing shorter surgery and decreased blood loss compared to cranial remodeling. 4
Despite its significant advantages, PCD requires a second operation to explant the hardware. In addition, PCD has relatively high complication rates.5-7 Our goal in this study was to perform a systematic review of the literature, in order to describe the characteristics of patients undergoing PCD, and measure the surgical outcomes of PCD, including gain in intracranial volume and complications. The study aimed to answer two main questions:
What is the average complication rate and the most common complications of PCD? How much intracranial volume expansion can one expect with PCD?
Methods
Ethics/Consent Declaration
Due to this study being a systematic review of published articles, institutional review board approval and subject consent were not applicable and not needed.
Literature Search
PubMed database searches for “cranial distraction” and “posterior distraction” in May 2022 yielded 114 results. Articles that were not in English, and those that were not related to posterior cranial distraction were excluded. The full text of the remaining articles was then reviewed. Additional articles were identified from the references and reviewed. Case reports, articles that did not involve posterior cranial distraction, reviews of the literature, and articles that did not provide extractable clinical data were excluded. In addition, articles that may include duplicate patients were excluded. Articles with potentially duplicate patients were defined as those published from the same institution with overlapping study periods.
Data Extraction and Analysis
For each article, clinical data were extracted, including the number of patients who underwent posterior cranial distraction, the number of patients with a syndrome, the average age at time of surgery (in months), presence of cerebellar tonsillar descent, hydrocephalus, average amount of distraction (in millimeters), and average intracranial volume gain from preoperative CT scan to postoperative CT scan (in cm3). Additional data on type of osteotomy (supratorcular versus infratorcular) and postoperative complications were extracted.
Results
Literature Review and Articles Included
As shown in Figure 1, the initial PubMed (using the terms “posterior” AND “distraction” AND “cranial” OR “calvarial”) search yielded 114 articles. After manually excluding articles that were clearly not related to posterior distraction, and articles that were not in the English language, 75 articles remained. After review of the full text of the remaining articles and their references, 18 articles were included in the systematic review. Details of the included articles are shown in Table 1. Two of the articles were published by the same institution,10,23 but the date ranges of patient recruitment did not overlap.
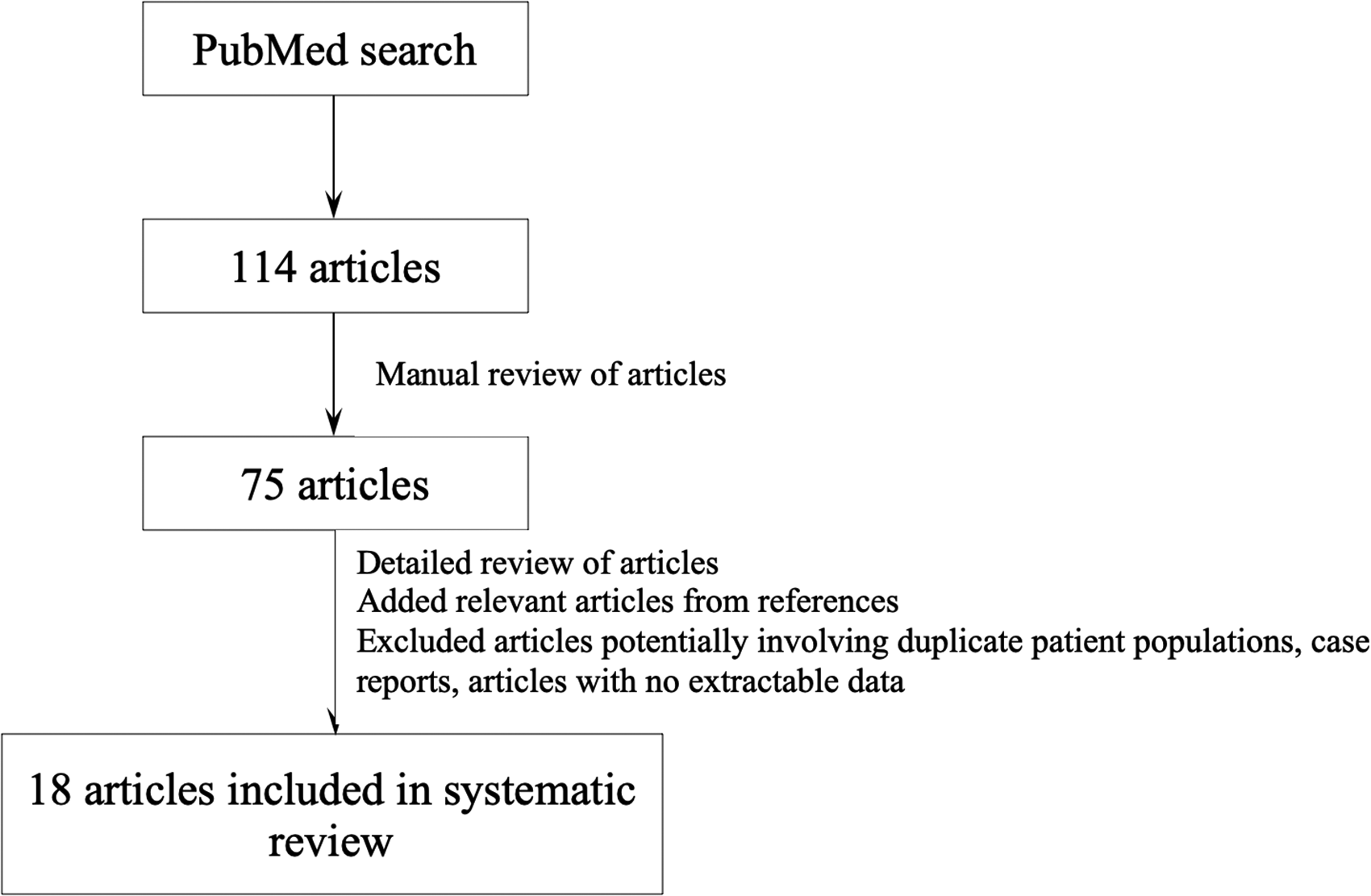
Extraction of articles included in the systematic review.
Details of Articles Included in the Systematic Review.
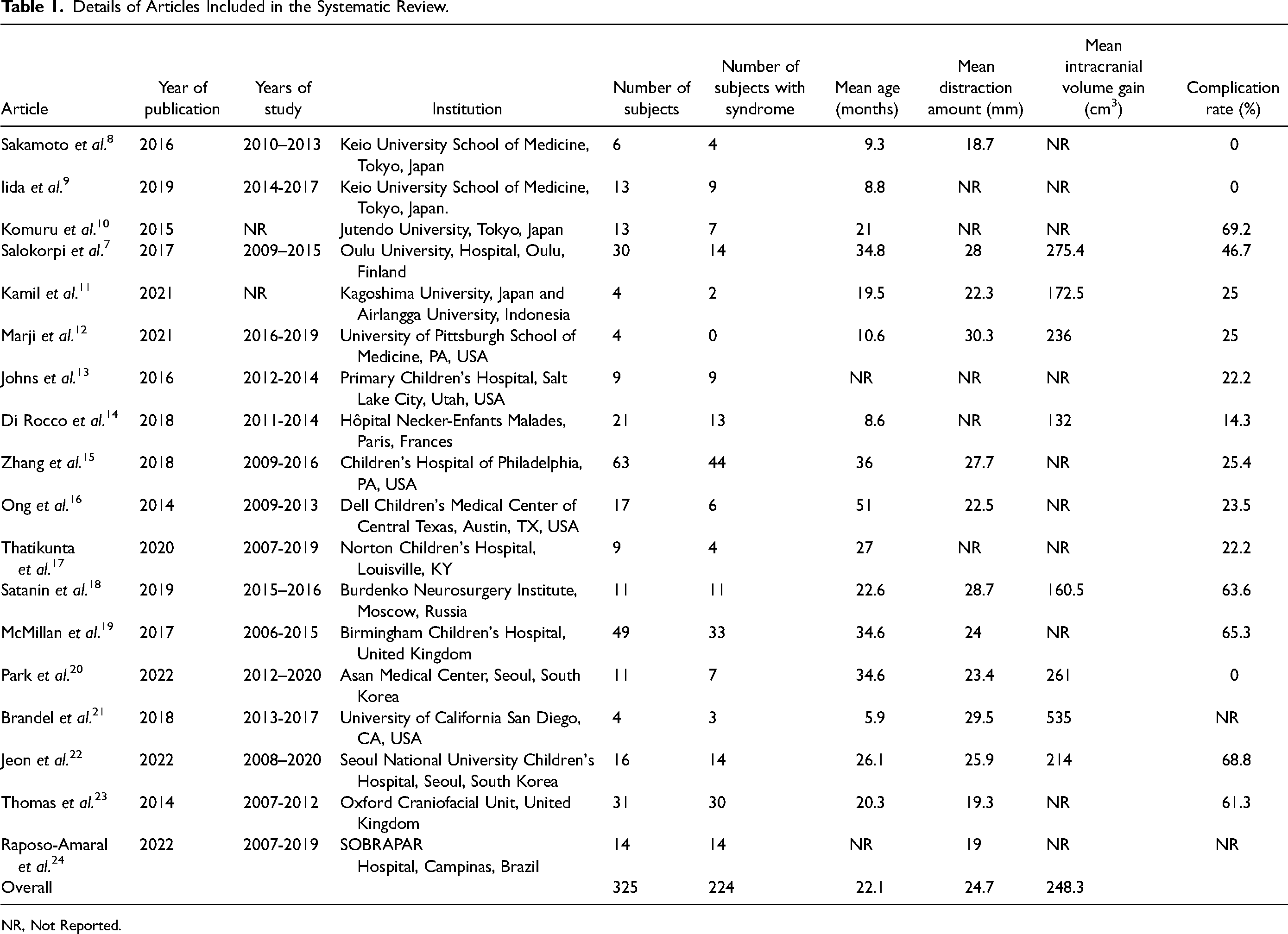
NR, Not Reported.
Patient Population
The 18 articles included 325 distinct patients, of whom 224 (68.9%) had been diagnosed with a syndrome. Of the 224 patients with a syndrome, the type of syndrome was provided in 174 patients. Apert syndrome was most common (62 patients, 35.6%), followed by Crouzon (36 patients, 20.7%), Muenke (17 patients, 9.8%), Saethre-Chotzen (17 patients, 9.8%), and Pfeiffer (16 patients, 9.2%) syndromes. Patients with other syndromes or unknown syndromes represented 11.7% of those with a syndrome. The average age at the time of surgery was 22.1 months.
Surgical Outcomes
The average length of distraction was 24.7 mm, ranging from 18.7 mm to 30.3 mm.10,11 Eight studies computed the average intracranial volume gain using preoperative and postoperative computed tomography scans.8,11,12,14,18,20-22 In those studies, the average volume gain was 253.2 cm3. The average volume gain per mm of distraction was 9.8 cm3.
Sixteen studies representing 307 subjects detailed postoperative complications.8-21,23,25 The overall complication rate in those studies was 32.2% (Figure 2). The most common complication was surgical-site infection (10.7%), followed by hardware failure/fracture/dislodgement (8.5%), delayed wound healing (6.2%), persistent cerebrospinal fluid leak (5.5%), significant hemorrhage (0.7%), meningitis (0.3%) and death (0.3%). The two cases of significant hemorrhage included one postoperative epidural hematoma, 16 and one case of severe intraoperative hemorrhage that required abandoning the procedure and returning to complete in a several days. 9 The death was due to postoperative respiratory failure in a patient with Crouzon syndrome. 13
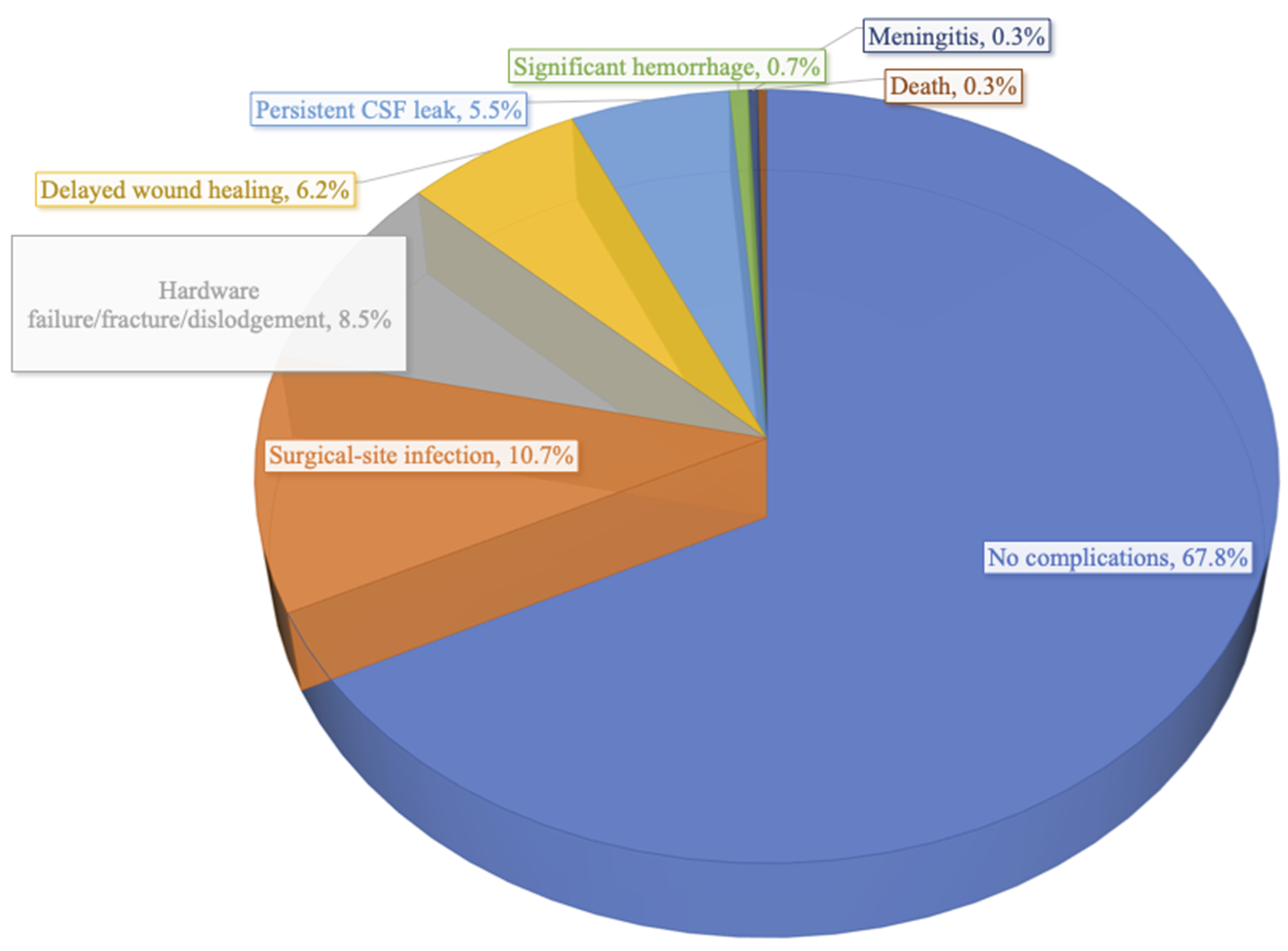
Complications of posterior cranial distraction.
Four studies included 35 patients with pre-existing cerebellar tonsillar herniation.13,20,21,25 After posterior cranial distraction, tonsillar herniation improved radiologically in 26 patients (74.3%).
Two studies included 40 patients with pre-existing signs of increased intracranial pressure.9,20 Those studies found that 37 patients (92.5%) had improvement in their intracranial hypertension, based on clinical, ophthalmologic or radiologic criteria.
Discussion
Posterior cranial distraction has gained significant popularity in the management of multisuture and syndromic craniosynostosis, due to its ability to significantly increase intracranial volume. On average, in the included studies, PCD increased intracranial volume by 253.2 cm3, which represents an increase in intracranial volume of approximately 25%. 12 Several studies have demonstrated that PCD is more effective at increasing intracranial volume than fronto-orbital advancement,26,27 which only provides approximately 8% of volume increase. 18 In the 40 patients with pre-existing signs of intracranial hypertension, 92.5% improved after PCD. These advantages, in addition to the fact that PCD has been found to improve turribrachycephaly 28 and fronto-orbital contour,24,29 have changed the paradigm for the treatment of multisuture and syndromic craniosynostosis,26,30 allowing the delay of fronto-orbital advancement until an older age when relapse is less likely. 30
In addition to increasing intracranial volume and attenuating intracranial hypertension, posterior cranial distraction has the potential to treat cerebellar tonsillar herniation, with improvement in up to 75% of patients, as noted above, thereby potentially obviating the need for posterior fossa decompression.31,32 In addition, Lin et al. found that patients who underwent PCD were significantly less likely than those who underwent posterior cranial remodeling to develop new-onset cerebellar tonsillar descent postoperatively. 33 Despite the benefits of PCD, there remain a significant proportion of patients whose tonsillar herniation does not improve postoperatively. It remains difficult to predict when PCD will be insufficient at preventing or improving tonsillar herniation. Therefore, where there is significant concern by the neurologic surgeon (significant tonsillar descent, very restricted foramen magnum), in-continuity posterior fossa decompression can usually be safely performed concurrently with PCD. 34
CSF leakage remains a relatively common complication of PCD, occurring in approximately 5.9% of cases. The dural laceration and subsequent CSF leak are believed to be due to the screw tips lacerating the dura during the activation phase of distraction. Various strategies have been employed to decrease this risk, including using resorbable material in the epidural space to act as a barrier between the dura and the screws,5,35 using self-drilling screws, 17 using the shortest screws possible, 6 and using resorbable pins instead of titanium screws. 14 No comparative study has been published to establish the effectiveness of any of these maneuvers. Overall, we found that PCD has a complication rate of 32.2%, which is higher than calvarial vault remodeling (5-11%), 36 spring-assisted cranioplasty (7.4%) 37 and minimally-invasive suturectomy and helmet therapy (3.5%). 38
Another important variable with PCD is the craniocaudal level of the occipital osteotomy. This osteotomy may be performed cranial or caudal to the level of the torcula. Some authors describe only performing supratorcular osteotomies.26,28,33 Other choose the level of the osteotomy based on preoperative imaging. 20 It is unclear whether an infratorcular osteotomy is more effective at improving tonsillar descent, 20 or increasing intracranial volume, 12 than supratorcular osteotomy. Zapatero et al. found that patients with a supratorcular osteotomy had a higher risk of developing an occipital step-off deformity. 39 Several authors have attempted to minimize that deformity by performing a supratorcular osteotomy and adding barrel staves to the bone caudal to the osteotomy,13,28,40 although evidence suggests that these barrel stave osteotomies do not help improve the step-off deformity.17,34 In addition, infratorcular osteotomies may minimize the risk of injury to the torcula and bleeding,3,9 although there is limited data to support that.
Since this is a systematic review of retrospective studies, this study has similar limitations to the underlying studies, namely small number of patients and lack of randomization. In addition, certain factors, such as the craniocaudal level of the osteotomy (supratorcular versus infratorcular), were only analyzed by a small number of studies, thereby making extraction of useful data difficult. The volumetric measurements may suffer from heterogeneity due to lack of standard interval between surgery and follow-up CT scan, ranging from a few months to over a year. Our study focused on posterior cranial distraction, and did not include other types of cranial distraction, such as anterior distraction for coronal craniosynostosis, and spring-assisted cranioplasty.
Conclusion
Posterior cranial distraction is a powerful technique in the initial treatment of multisuture or syndromic craniosynostosis, although the complication rates are significantly higher than traditional remodeling techniques. Despite its relatively high complication rates, the procedure allows significant increase in intracranial volume, decreasing intracranial pressure, and potentially alleviating cerebellar tonsillar descent. Further studies are needed to better evaluate the optimal craniocaudal level of the occipital osteotomy, and techniques to minimize the risk of CSF leakage.
Footnotes
Conflicts of Interest and Source of Funding
None of the authors have any relevant financial conflicts of interest. This study was not funded.
Ethics/consent declaration
Due to this study being a systematic review of published articles, institutional review board approval and subject consent were not applicable and not needed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Level of Evidence
IV