
Abstract
Objective
The purpose of this study is to assess cleft rhinoplasty terminology across phases of growth.
Design/Setting
A systematic review was performed on cleft rhinoplasty publications over 20 years.
Interventions
Studies were categorized by age at surgical intervention: infant (<1 year); immature (1 to 14 years); mature (>15 years).
Main Outcome Measures
Collected data included terminology used and surgical techniques.
Results
The 288 studies included demonstrated a wide range of terminology. In the infant group, 51/54 studies used the term “primary.” In the immature group, 7/18 studies used the term “primary,” 3/18 used “secondary.” In the mature group, 2/33 studies used the term “primary,” 16/33 used “secondary,” 2/33 used “definitive,” 5/33 used terms such as “mature,” “adult,” and “late,” and 8/33 did not use terminology.
Surgical technique assessment demonstrated
cleft rhinoplasty at infancy used nostril rim or no nasal incision, immature rhinoplasty used closed and open rhinoplasty incisions; and mature rhinoplasty used a majority of open rhinoplasty. Infant and immature cleft rhinoplasty incorporated septal harvest or spur removal in <10% of cases, whereas these procedures were common in mature rhinoplasty. No studies in infants or immature patients used osteotomies or septal grafts, common techniques in mature rhinoplasty.
Conclusions
Current terminology for cleft rhinoplasty is varied and inconsistently applied across stages of facial development. However, cleft rhinoplasty performed at infancy, childhood, and facial maturity are surgically distinct procedures. The authors recommend the terminology “infant,” “immature,” and “mature” cleft rhinoplasty to accurately describe this procedure within the context of skeletal growth.
Introduction
Cleft rhinoplasty aims to correct the nasal deformity associated with cleft lip, hallmarks of which include malposition of the lower lateral cartilage, soft tissue deficiency of the nasal floor, septal deviation, and lateralization the alar base. 1 This can lead to a broad, flat nasal tip, wide alar base, and short columella, especially in bilateral cleft lip. 2
Due to previous concerns over negative effects on facial growth and excessive scarring, cleft rhinoplasty was initially performed at a delayed stage, in late adolescence or after skeletal maturity. However, long term studies have largely addressed this concern, and primary cleft rhinoplasty has become more routine since its initial conception in the late twentieth century.3‐8
Despite this evolution of cleft rhinoplasty, the literature is varied in how the procedure is described across the infant and adult population. Cleft rhinoplasty technique is commonly surgeon-dependent, and reported literature is largely based on single-surgeon outcomes. This heterogeneity is compounded by the following observations: 1) not all surgeons elect to perform cleft rhinoplasty at time of primary cleft lip repair, and 2) the timing, technique and decision to perform revision rhinoplasties is highly variable.
The wide variety of techniques reported in the literature has been associated with a similarly wide range of terminology used to describe cleft rhinoplasty. Terms such as “primary”, “secondary”, “late”, “definitive” and others are commonly used, sometimes with unclear association with any specific type of technique. We hypothesize that current terminology does not consistently reflect stages of facial development, and that these growth stages greatly influence the surgical techniques used in the cleft rhinoplasty procedure. Therefore, the purpose of this study is to systematically evaluate the terminology used in cleft rhinoplasty across phases of skeletal growth.
Methods
Search Criteria
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 9 Institutional review board approval and patient consent was not applicable and not needed for this study. Three electronic databases (PubMed, Cochrane CENTRAL, and Embase) were queried through December 2021 for keywords and subject headings pertaining to cleft rhinoplasty. An example of the search strategy and concepts as applied to PubMed is available in Figure 1. This search strategy was adapted for each database.
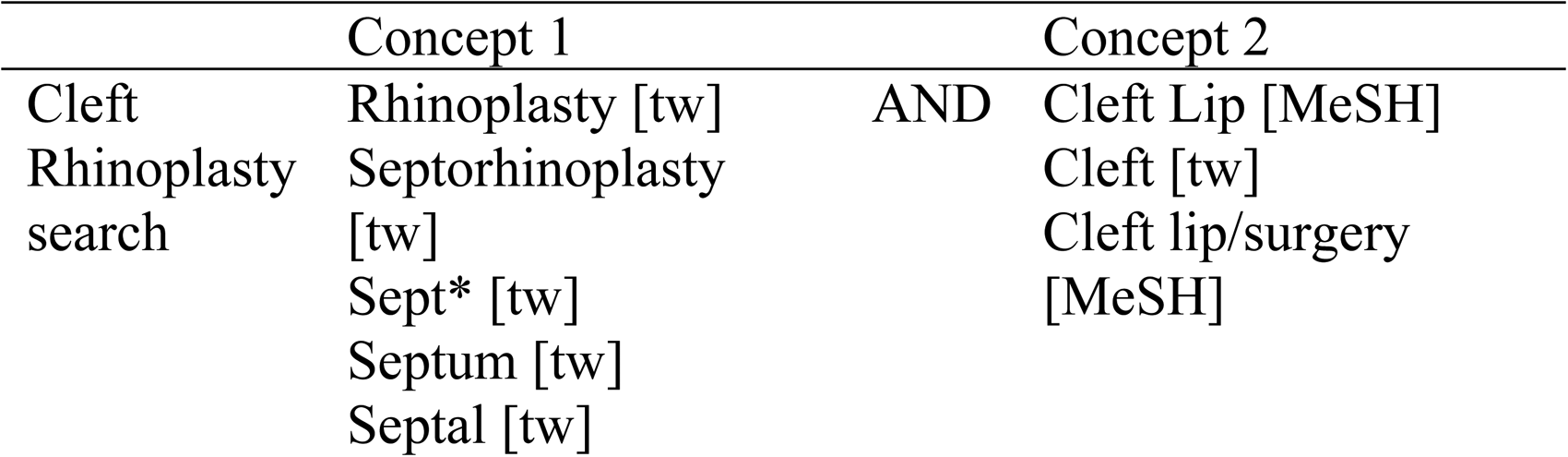
Systematic review search strategy example using PubMed.
Selection Criteria
All resulting articles were compiled, and duplicate titles were removed using Endnote X9. Of five independent reviewers (JJP, RRC, FDA, ML, BFC), each remaining title and abstract was screened by two reviewers in Covidence (www.covidence.org). Screening was equally divided amongst reviewers. Inclusion criteria during screening included mention of cleft rhinoplasty. Articles describing rhinoplasty in patients without a cleft, rhinoplasty in patients with syndromic facial cleft, those with non-human subjects, cadaveric studies, and non-English language articles were excluded. Conflicts were resolved by a third voting member.
Final inclusion criteria in full text review were based on clinical studies that included description of cleft rhinoplasty. Articles that discussed cleft rhinoplasty morphology without surgical intervention, rhinoplasty in patients without a cleft, rhinoplasty in patients with syndromic facial clefts, systematic or narrative reviews, abstracts, correspondence, and editorials were excluded from analysis. Each article was screened by two independent reviewers from the reviewer pool (JJP, RRC, FDA, ML, BFC) with articles equally distributed among reviewers.
Data Collection
A tool for data collection was prospectively developed in Covidence (www.covidence.org) and completed for the following data points as available by the reviewers: year of publication, study population, age at surgery, primary vs secondary vs revision cleft rhinoplasty, terminology used, and described surgical technique.
Identified articles were grouped by the following stages of growth: infancy (< 1 year), skeletal immaturity (2–14 years), and skeletal maturity (>15 years). Descriptive terms to categorize cleft rhinoplasty (primary, secondary, etc) were collected. Described surgical techniques, including type of incision used, exposure of anatomic structures, septal work, nasal dorsum manipulation, nasal tip work, and alar base resection were collected.
Results
Cleft Rhinoplasty Search
A total of 1068 unique articles were identified (Figure 2). The title and abstract screen excluded 489 articles, resulting in 524 articles for full text screening. Following full text review, 236 articles were excluded, with a total of 288 articles included for data collection (
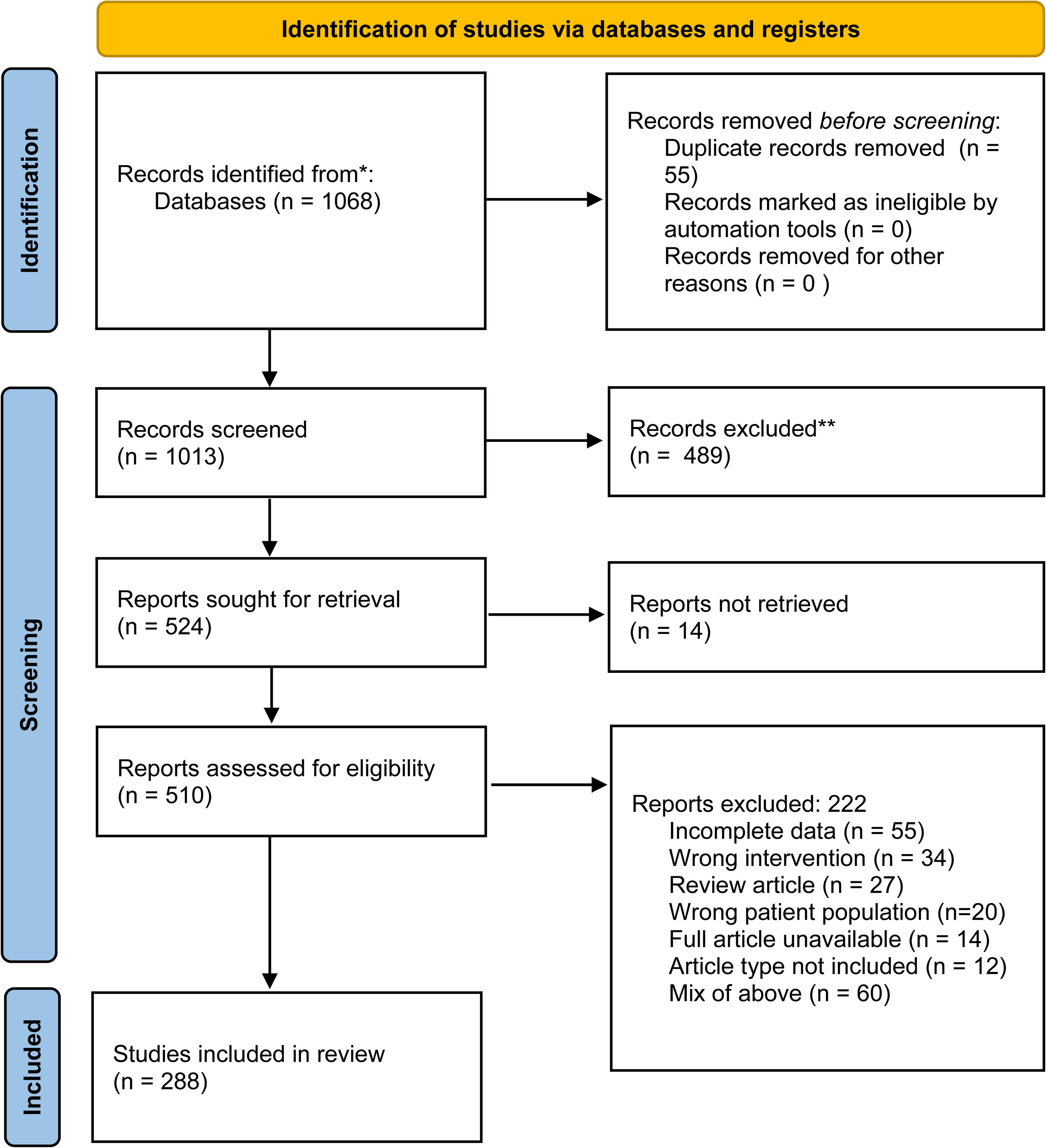
PRISMA diagram.
First Cleft Rhinoplasty
Of the 139 studies describing first cleft rhinoplasty, 97 studies described rhinoplasty in patients with a unilateral cleft lip and nose, 26 studies described rhinoplasty in patients with bilateral cleft lip and nose, and 16 studies described rhinoplasty as applicable to patients with both unilateral and bilateral clefts (Table 1).
First Cleft Rhinoplasty by Terminology.
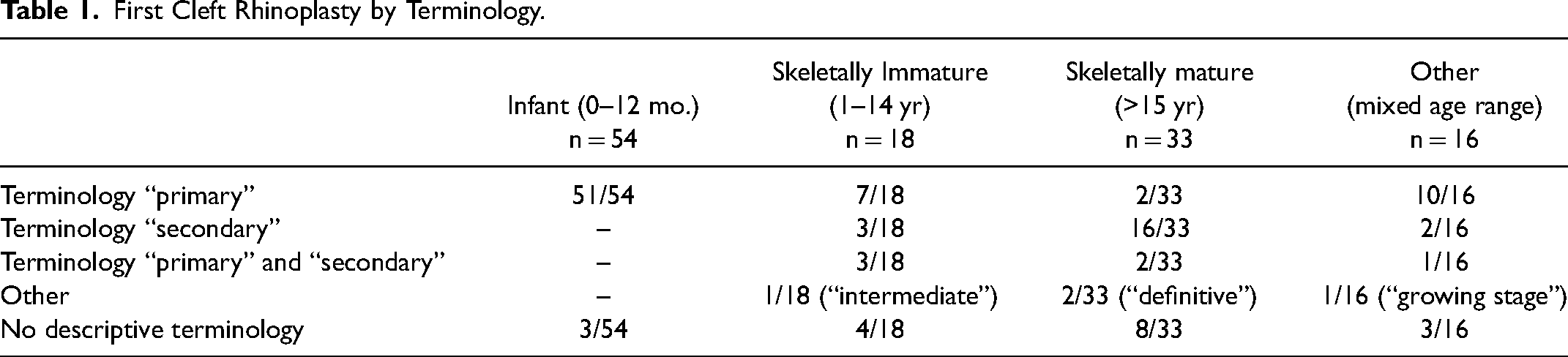
There were 54 studies describing first cleft rhinoplasty in infants 12 months old or younger; 51/54 (94.4%) used the term “primary” to describe the cleft rhinoplasty and 3/54 did not use descriptive terminology. The average reported age of the patients in these studies was 4.7 months.
There were 18 studies describing first cleft rhinoplasty in a skeletally immature population (1–14 years old); 7/18 (38.9%) used the term “primary,” 3/18 (16.7%) used the term “secondary,” 3/18 (16.7%) used a mix of primary and secondary descriptive terms, 1/18 (5.6%) used the term “intermediate,” and 4/18 (22.2%) did not use any descriptive terminology.
There were 33 studies describing first cleft rhinoplasty in a skeletally mature population (>15 years old). Of these studies, 2/33 (6.1%) used the term “primary,” 16/33 (48.5%) used the term “secondary,” 2/33 (6.1%) used a mix of “primary” and “secondary,” 2/33 (6.1%) used the term “definitive,” 3/33 (9.1%) studies used terms “mature,” “adult,” and “late,” and 8/33 (24.2%) did not use any descriptive terminology.
There were 16 studies that described first cleft rhinoplasty in a wide age range of patients that did not fall into the aforementioned categories. There were 7 studies that did not note the age range of patients undergoing first cleft rhinoplasty.
Revision Cleft Rhinoplasty
There were 114 studies describing a revision cleft rhinoplasty procedure (Table 2). Of these studies, 18 described revision rhinoplasty in a skeletally immature (1–14 years old) population. The average reported age of the patients in these studies were 10.4 years. In this skeletally immature group, 17/18 (94.4%) used the term “secondary,” and 1/18 (5.6%) did not use descriptive terminology.
Revision Cleft Rhinoplasty by Terminology.
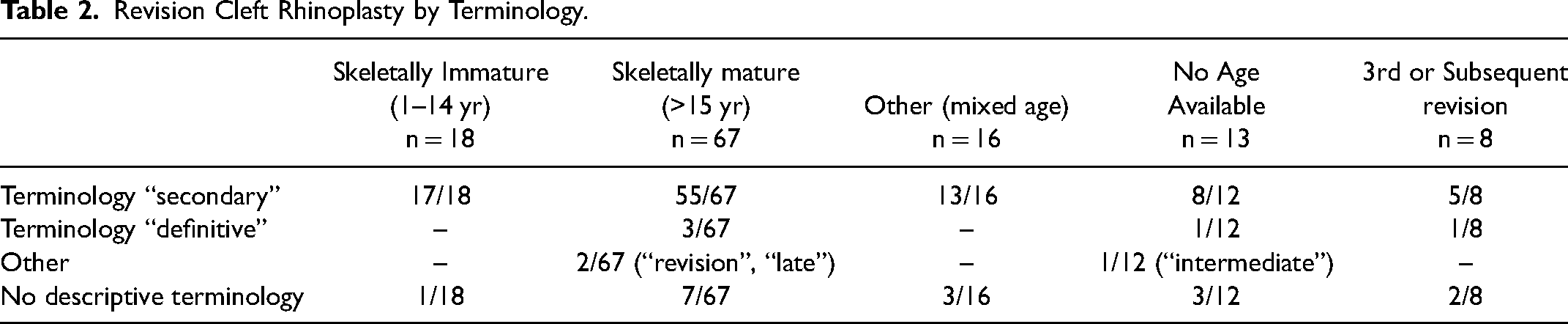
There were 67 studies describing revision cleft rhinoplasty in skeletally mature patients (>15 years old). The average reported age of patients in these studies was 21.6 years. In this skeletally mature group, 55/67 (82.1%) used the term “secondary,” 3/67 (4.5%) used the term “definitive”, 2/67 (2.9%) used terms “revision,” and “late,” and 7/67 (10.4%) did not provide descriptive terminology.
There were 16 studies describing revision cleft rhinoplasty in a wide age range of patients that did not fall into the categories of skeletally immature or mature; 13/16 (81.3%) studies used the term “secondary,” and 3/16 (18.8%) did not provide descriptive terminology. There were 13 studies that described secondary rhinoplasty without specifying the age range of included patients.
There were 8 studies describing a 3rd or subsequent revision cleft rhinoplasty. Of these studies, 5/8 (62.5%) used the term “secondary,” 1/8 (12.5%) used the term “definitive,” and 2/8 (25.0%) did not use descriptive terminology.
Surgical Techniques in First Cleft Rhinoplasty
Incision
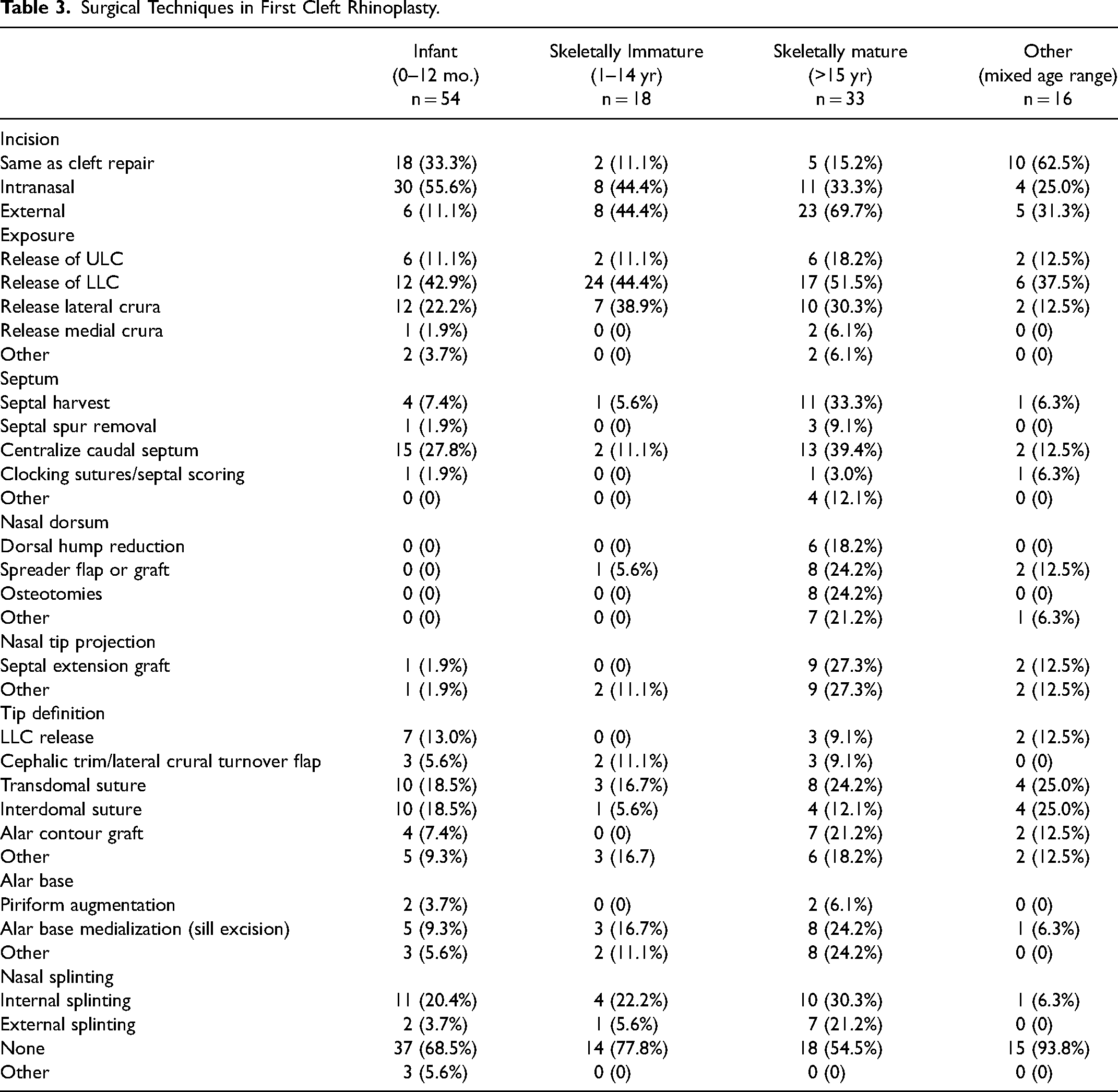
Among the articles describing first cleft rhinoplasty in the infant population, most articles described use of a closed rhinoplasty with nostril rim incision (30/54, 55.6%) or utilizing the cleft repair incision (18/54, 33.3%) compared to use of an external columella incision (6/54, 11.1%) (Table 3). In the skeletally immature population, there was equal distribution of articles describing closed (8/18, 44.4%) and open rhinoplasty incision use (8/18, 44.4%). In the skeletally mature population, the majority of articles described use of open rhinoplasty (23/33, 69.7%).
Surgical Techniques in First Cleft Rhinoplasty.
Septum
In articles describing first cleft rhinoplasty in the infant population, most commonly described technique was centralization of the caudal septum (15/54, 27.8%). Few articles described septal spur removal (1/54, 1.9%) or septal harvest (4/54, 7.4%). In the skeletally immature population, few articles described septum centralization (2/18, 11.1%), harvest (1/18, 5.6%), or septal spur removal (0/18, 0%). In the skeletally mature population, commonly described techniques included centralization of the caudal septum (13/33, 39.4%), septal harvest (11/33, 33.3%), septal spur removal (3/33, 9.1%) and septal extension grafts (9/33, 27.3%).
Nasal Dorsum
In the infant and skeletally immature population, no articles described dorsal hump reduction or osteotomies. In the skeletally mature population, nasal dorsum manipulation techniques of dorsal hump reduction (6/33, 18.2%), spreader flap or graft (8/33, 24.2%), osteotomies (8/33, 24.2%), or other surgical manipulation (7/33, 21.2%) were described.
Nasal Tip
In the infant and skeletally immature population, commonly described techniques included transdomal (10/54, 18.5%) and interdomal (10/54, 18.5%) sutures. Few articles described use of alar contour grafting (4/54, 7.4%) or cephalic trim/lateral crural turnover flaps (3/54, 5.6%). In the skeletally immature population, described techniques included transdomal sutures (3/18, 16.7%), interdomal sutures (1/18, 5.6%), and cephalic trim (2/18, 11.1%). In the skeletally mature population, most commonly described techniques included transdomal sutures (8/33, 24.2%), alar contour graft (7/33, 21.2%) and interdomal sutures (4/33, 12.1%).
Alar Base
Alar base medialization (sill excision) was described in 5/54 (9.3%) articles in the infant population, 3/18 (16.7%) articles in the skeletally immature population, and 8/33 (24.2%) articles in the skeletally mature population.
Surgical Techniques in Revision Cleft Rhinoplasty
Incision
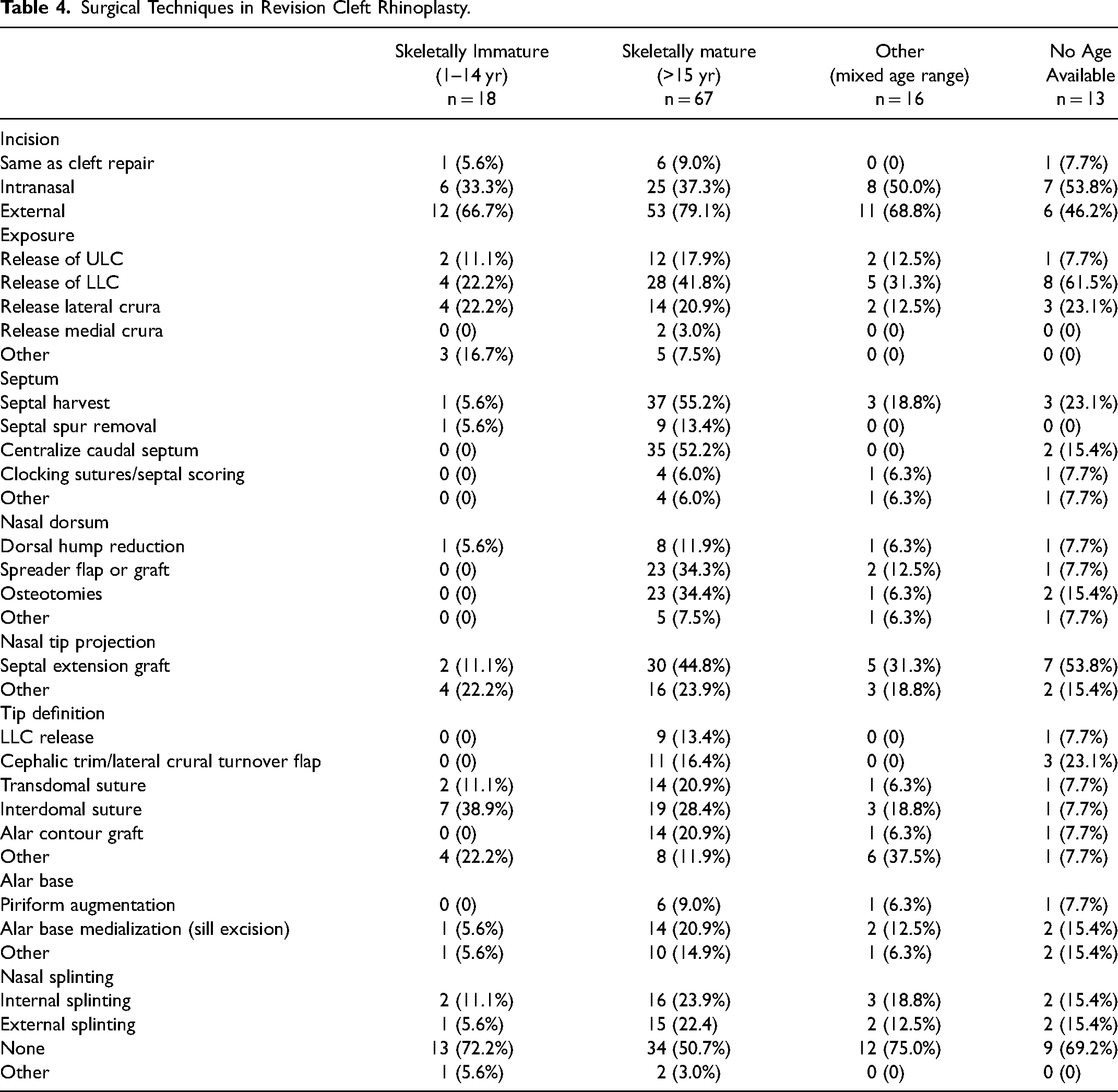
In articles describing a revision cleft rhinoplasty procedure, external incisions were most commonly described in both skeletally immature (12/18, 66.7%) and skeletally mature (53/67, 79.1%) groups (Table 4).
Surgical Techniques in Revision Cleft Rhinoplasty.
Septum
In articles describing septal work during revision cleft rhinoplasty in the skeletally immature population, one article (1/18, 5.6%) described septal harvest and one article (1/18, 5.6%) described septal spur removal in the skeletally immature population; two articles described use of septal extension grafts (2/18, 11.1%). In the skeletally mature population, commonly described techniques included septal harvest (37/67, 55.2%), septal spur removal (9/67, 13.4%), and centralization of the caudal septum (35/67, 52.2%). Septal extension graft use was described in 30 (30/67, 44.8%) articles.
Nasal Dorsum
In the skeletally immature population, one article described dorsal hump reduction (1/18, 5.6%); no articles described use of spreader flaps, grafts, or osteotomies. In the skeletally mature population, most commonly described techniques included osteotomies (23/67, 34.3%) and spreader flap or graft (23/67, 34.3%) followed by dorsal hump reduction (8/67, 11.9%).
Nasal Tip
In the skeletally immature population, described techniques for nasal tip included interdomal sutures (7/18, 38.9%) and transdomal sutures (2/18, 11.1%). There were no articles describing cephalic trim, lateral crural turnover flaps, or alar contour grafts. In the skeletally mature population, described techniques included transdomal (14/67, 20.9%) and interdomal (19/67, 28.4%) sutures, alar contour graft (14/67, 20.9%), and cephalic trim/lateral crural turnover flaps (11/67, 16.4%).
Alar Base
Alar base medialization (sill excision) was described in 1/18 (5.6%) articles in the skeletally immature population and 10/67 (14.9%) articles in the skeletally mature population.
Discussion
The results of this systematic review identify inconsistencies in the nomenclature used to describe cleft rhinoplasty. The term “primary rhinoplasty,” while predominantly used to describe first cleft rhinoplasty procedure in infants, is also used to describe the first cleft rhinoplasty surgery in skeletally immature and mature patients, despite the finding that the techniques used in cleft rhinoplasty vary significantly dependent on the stage of facial development. Therefore, current use of the term “primary rhinoplasty” can infer different types of operations depending on the age of the patient. Furthermore, the term “secondary rhinoplasty” is also used to describe first cleft rhinoplasty procedure in skeletally immature and mature patients, as well as revision cleft rhinoplasty in skeletally immature and mature patients. Therefore, there is a confusion of terminology in the literature as the term “secondary” appears to be interchangeably used to denote the timing of rhinoplasty or a revision rhinoplasty. Furthermore, it also appears that “secondary” rhinoplasty has been used to denote any revision rhinoplasty (tertiary, quaternary, etc) creating additional inaccuracies in the literature. This study demonstrates that the descriptive terms “primary” and “secondary” are used interchangeably in the literature, and do not accurately denote the age or skeletal maturity of the patient nor the stage of surgical repair.
Review of cleft rhinoplasty technique shows that there are significant differences in techniques used for patients undergoing reconstruction in infancy, skeletal immaturity, and skeletal maturity. Based on frequency of reporting in the literature, first cleft rhinoplasty in infancy and at skeletal immaturity primarily used an internal nostril rim or cleft lip repair incision with centralization of the caudal septum but rare septum harvest, graft use, osteotomies, or dorsal hump reduction. Conversely, first cleft rhinoplasty in skeletally mature patients more commonly utilizes an open rhinoplasty incision with incorporation of more invasive techniques such as septal harvest, septal/cartilage grafts, osteotomies, and nasal dorsum manipulation. This distinction is critical, as the relatively limited surgical dissection seen in cleft rhinoplasty in infancy and skeletal immaturity aims to limit iatrogenic damage to facial growth while providing a level of early correction to the cleft nasal deformity. Rhinoplasty at the time of facial maturity, in contrast, can incorporate the entire repertoire of osteotomies, septal manipulation and other rhinoplasty techniques available within the armamentarium. Therefore, the techniques used in cleft rhinoplasty are more influenced by the stage of facial development than by the fact that it is the patient's first nasal surgery.
This distinction in cleft rhinoplasty techniques influenced by stage of skeletal maturity is also present in revision cleft rhinoplasty. This study demonstrates that revision cleft rhinoplasty at skeletal immaturity rarely utilizes septal harvest, grafting, osteotomies, or dorsal hump reduction, whereas these techniques are commonly used in revision cleft rhinoplasty at skeletal maturity. This suggests that revision rhinoplasty procedures have distinct surgical hallmarks based on the skeletal maturity of the patient, not by the number of previous operations, a detail that is not conveyed through the nomenclature currently used in the literature. There can be a significant range of what is surgically indicated at revision rhinoplasty, based on status of previous rhinoplasties and considerations of skeletal maturity.10,11 A recent study investigating secondary cleft rhinoplasty practices through query of a national database supports this idea, showing that even within secondary cleft rhinoplasty, there are distinct surgical procedures based on patient age, with patients 10 and under typically receiving a “tip only” secondary rhinoplasty and patients 14 and over receiving more extensive rhinoplasty with septal work and osteotomies. 12
Cleft rhinoplasty has seen significant evolution over the past decade. The most significant change in the field has been increasing performance of cleft rhinoplasty at infancy, which was previously discouraged due to concern for effects on facial growth.5,6,13 However, with increasing evidence that a limited surgical dissection can provide early correction of the cleft nasal deformity while preserving facial growth centers, large-scale database studies now report that 33–50% of patients undergo primary cleft rhinoplasty at infancy, especially in urban settings and academic teaching hospitals. 14
In the literature, there has been increasing investigation into this evolution of cleft rhinoplasty, both on a large scale nation-wide as well as individual practice trends.14‐16 In understanding the history of this evolution, it is possible to see how the nomenclature used in the literature has not evolved to the pace of practice. The most commonly used descriptive terms “primary” and “secondary,” while adequate at a time when cleft rhinoplasty was solely performed in late adolescence or after skeletal maturity, no longer provide sufficient distinction between the variations of cleft rhinoplasty procedures that occur throughout the stages of skeletal growth. Furthermore, when considering cleft surgery in low-to middle-income countries, where the majority of cleft surgery is performed, “primary” rhinoplasty can commonly occur after infancy and well into skeletal maturity, resulting in conflation of a wide range of surgical technique under one umbrella term. Therefore, the importance of reliable nomenclature is critical considering the inaccuracies that “primary” and “secondary” rhinoplasty pose in different parts of the world.
The presented study has identified several other terms used to describe cleft rhinoplasty performed after the time of infancy such as: “intermediate,” “definitive,” “adult,” “mature,” and “late.” Although these terms lend some insight into either the stage or type of operation, they are ultimately vague and lack clarity. A “definitive” operation is one that completes reconstructive and aesthetic goals. This can be performed at the time of the first operation at infancy or a minor revision surgery at the time of growth. Although one could posit that the rhinoplasty performed at the time of skeletal maturity can be considered definitive, the significant re-operation rate associated with cleft rhinoplasty calls to questions the accuracy of this term. “Late” rhinoplasty as a term also suffers from limitations, as different practices and different parts of the world vary in the parameters of when a rhinoplasty is considered “late.” Furthermore, the term implies that there is an “early” rhinoplasty or at least one that is “on time”, two definitions for which there is an unlikely consensus. The authors believe there is need for a simplified set of descriptive terminology that clearly and succinctly relays the category of cleft rhinoplasty performed on the patient.
Therefore, based on the results of this study, the authors suggest a nomenclature of “infant,” “immature,” and “mature” cleft rhinoplasty to describe this surgery within the context of skeletal maturity. This categorization will allow accurate depiction of the cleft rhinoplasty as applicable to skeletal stage, which is more predictive of the types of techniques used compared to the number of previous surgeries. This study has found that the term “primary” rhinoplasty does not accurately reflect the type of surgery performed and “secondary” rhinoplasty has been interchangeably used to describe either rhinoplasty performed after infancy or some type of revision rhinoplasty. Therefore, the authors discourage the use of these terms as they lack clarity and promote confusion in the literature.
Using standard terminology to convey precise and unambiguous information is important both for scientific assessment as well as patient counseling and education. 17 Reported outcomes on practice patterns and surgical techniques, especially through large database studies, increasingly relies on appropriate capture via search terms; this is evidenced by the increasing number of systematic reviews and Current Procedural Terminology (CPT)-code based studies.18‐20
Furthermore, standardized key words in online patient education materials is crucial to successful dissemination of information, by way of promoting appropriate retrieval by search engines, providing understandable information for non-medical communities, and allowing for cross-comparison across sources. As patients and families increasingly rely on online education materials and social media both prior to and during care, establishing consistency helps maintain readability and achieve the benefits of online platforms and social media.21‐23
Though this study aims to provide a current characterization of cleft rhinoplasty performed at infancy, skeletal immaturity, and skeletal maturity as reported in the literature, there are several limitations. The ability to categorize and tabulate surgical technique is dependent on reporting in the published literature, and the heterogeneity in the level of detail provided across studies precludes comprehensive analysis of how frequently surgical techniques are utilized. Furthermore, although there are broad categorizations made on how surgical techniques are used in cleft rhinoplasty at different stages, ultimately the surgical techniques used in a given surgery are dependent on anatomic and physiologic needs. Additionally, surgeons themselves evolve in use of specific techniques, and what is currently available in the literature may not accurately reflect current practice. 24 Furthermore, the studies captured by this systematic review likely skew towards academic, research-heavy surgeons and practices and likely under-represent community-based surgeons that do not regularly publish on cleft rhinoplasty.
Conclusions
Current terminology for cleft rhinoplasty is varied and inconsistently applied across stages of facial development. However, cleft rhinoplasty performed at infancy, childhood, and facial maturity are distinct procedures. The authors recommend the terminology “infant,” “immature,” and “mature” cleft rhinoplasty to accurately describe this procedure within the context of skeletal growth.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231169479 - Supplemental material for Characterizing Cleft Rhinoplasty Across Skeletal Maturity: A Systematic Review of Terminology and Surgical Techniques
Supplemental material, sj-docx-1-cpc-10.1177_10556656231169479 for Characterizing Cleft Rhinoplasty Across Skeletal Maturity: A Systematic Review of Terminology and Surgical Techniques by Jenn J. Park, Matteo Laspro, Fernando D. Arias, Ricardo Rodriguez Colon, Bachar F. Chaya, Danielle H. Rochlin, David A. Staffenberg and Roberto L. Flores in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.