
Abstract
Objective
The addition of a uvular flap (PFU) was hypothesized to improve outcomes over standard pharyngeal flap (PF) for correction of velopharyngeal dysfunction. We report differences in outcomes of PF vs PFU at our institution.
Design
Retrospective cohort study.
Setting
Tertiary children's hospital.
Patients
Children who underwent PF or PFU with the three highest-volume surgeons at our institution in 2004-2017.
Outcome measures
We examined differences in complications between groups, frequency and type of revision surgery, and speech-related measures including nasometry, pressure-flow testing (PFT) and perceptual speech analysis (PSA).
Results
160 patients were included, 41 PF and 119 PFU (including 18 with Hogan technique). Patients undergoing PFU were older (7.6 yr vs 6.0 yr; p = 0.037) and more likely to have cleft palate (63/119 vs 14/41; p = 0.047). There was no significant difference in complications. With PFU, a decrease in airspace contracting revision surgeries was noted, (4/119 vs 8/41; p = 0.002) which drove a reduction in revision surgery of all types (7/119 vs 13/41; p = 0.033). However, patients that did undergo revision surgery after PFU underwent more revision procedures (p = 0.032). PSA scores were found to be lower (less hypernasal) after PFU (p = 0.009) compared to PF. Objective speech measures had varying results, with nasometry demonstrating a significant difference between groups (p = 0.001), while PFT (p = 0.525) did not demonstrate a statistical difference.
Conclusion
The use of a uvular lining flap in pharyngeal flap surgery may be associated with improved long term surgical outcomes, including both improvements in subjective and objective testing and a lower rate of revision surgery, without increased complications.
Introduction
Velopharyngeal dysfunction (VPD) is a speech disorder characterized by incomplete closure of the nasopharynx during speech, leading to inappropriate hypernasal resonance and nasal air emission. Symptoms of VPD can significantly impact quality of life. 1 VPD may persist after primary repair of a cleft palate (CP) in up to 20% of patients depending on the technique utilized.2,3 It may also be the presenting symptom of an unrepaired submucous CP, 4 and is frequently present in patients with 22q11 deletion regardless of the presence of CP. 5 VPD may also be associated with neurofibromatosis type 1 6 and other disease processes or syndromes. Occasionally, VPD is also found after adenotonsillectomy, but rarely persists beyond a few months. 7
Velopharyngeal insufficiency (VPI) is a common subtype of VPD characterized by an anatomical deficit leading to incomplete closure of the velopharyngeal port. One surgical treatment for VPI is the pharyngeal flap.8–10 In this procedure, a myomucosal flap is raised from the posterior pharyngeal wall and is left pedicled superiorly. An incision is made in the posterior soft palate and a pocket is created for insertion of the flap, which is sutured into place (see Figs 1a-1d). The procedure is straightforward and has demonstrated good results in a variety of patient groups including those with repaired CP, 11 non-cleft VPD 12 and 22q11 deletion. 13 It has even been shown to improve articulation scores in younger patients that have both articulation errors and VPD. 10 The procedure is often successful at reducing unwanted hypernasality, but risks of surgery include hyponasality or obstructive sleep apnea (OSA) from overcorrection of the anatomic gap. Alternatively, persistent VPI may also occur if there is undercorrection of the gap. Either case (overcorrection or undercorrection) may require revision surgery.
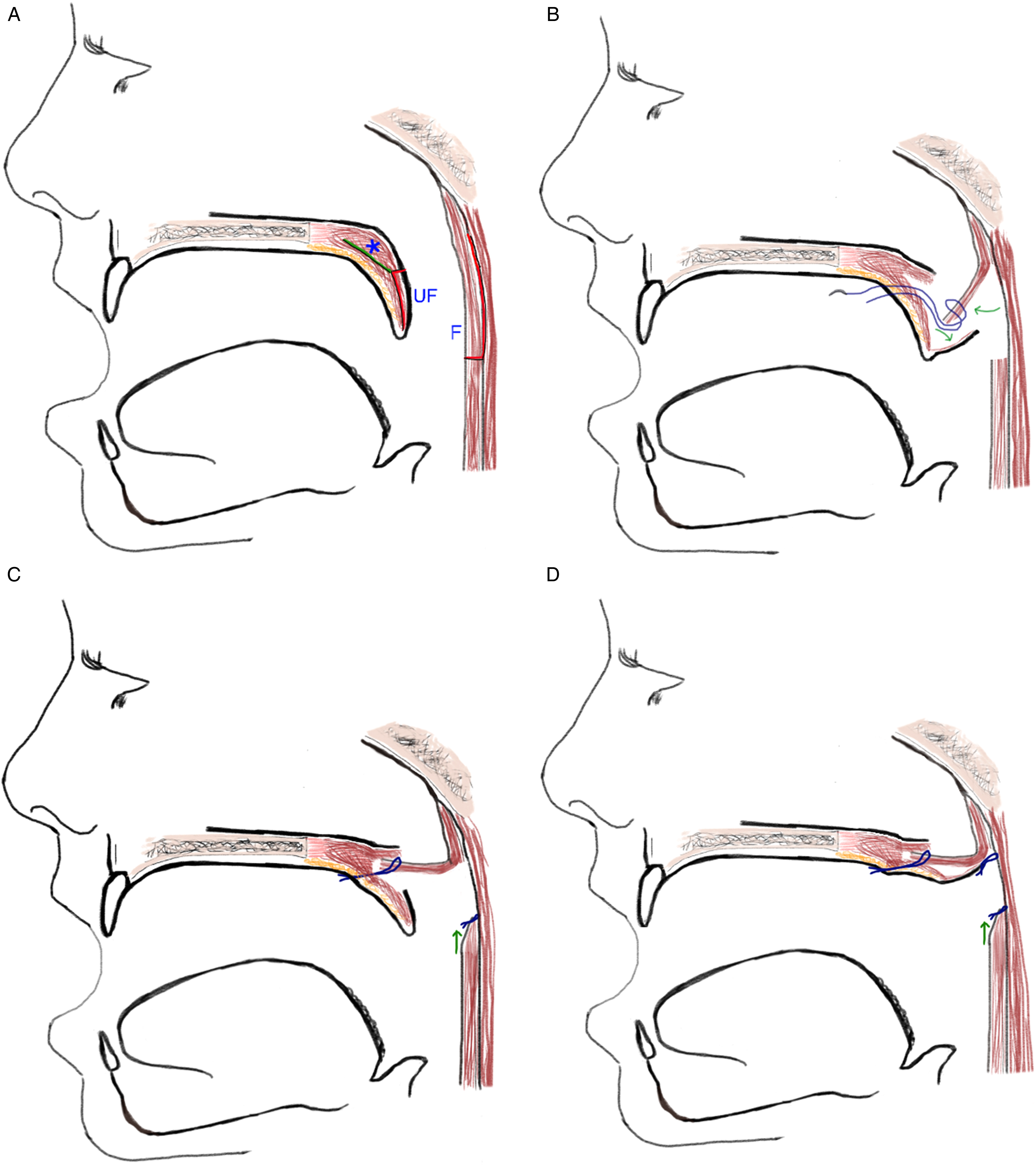
Pharyngeal Flap Techniques.
The raised pharyngeal flap is mucosalized on its superior surface after being inset. However, the inferior surface of the flap has exposed raw tissue unless additional action is taken. We hypothesized that the healing of this raw surface through secondary intention could lead to changes in the size and shape of the flap tissue with time, which may cause unpredictable results and increase the need for revision surgery.
Our institution's VPI team shifted from the use of a standard, “unlined” pharyngeal flap (PF) to the additional use of a uvular lining flap (PFU) to theroretically reduce healing by secondary intention and better maintain the intended width of the flap. This technique is further described in the methods section below. Some have advocated for the use of the Hogan flap technique (HF), also known as the lateral port control technique, which is similar to PFU but involves additional steps including a full thickness division of the soft palate in the midline prior to the creation of the uvular and nasal mucosal flaps that are also used for lining the undersurface of the PF. 14
This retrospective study describes our outcomes using both of the above techniques that cover, or “line,” the pharyngeal flap (using either the PFU or HF techniques), compared with the standard PF.
Methods
Patient Population
This retrospective cohort study was approved by the University of Arkansas for Medical Sciences Institutional Review Board. We created a database to analyze demographics, VPI-related testing, and outcomes in patients undergoing primary pharyngeal flap for VPI at our institution from 2004 to 2017. The timeframe was selected as the beginning and end points of our institution's prior electronic health records system which also allowed for sufficient follow-up time (at least 4 years) for analysis of the most recent surgical patients in the cohort. Institutional billing records were used to obtain a list of all patients who had undergone any version of a pharyngeal flap (inclusive of PF, PFU and HF) using the current procedural terminology code (42225). Surgical and clinic records were then reviewed. Patients were excluded if: over 18 years of age at the time of primary surgery; less than 6 months of follow-up; history of prior surgery for VPI; history of radiation therapy or partial pharyngectomy as a cause for VPD.
Assessments
Patients found to have significant VPD at our institution (regardless of prior history of CP) are evaluated routinely in a multi-disciplinary VPD clinic. The evaluation includes: 1) flexible nasopharyngoscopy, 2) perceptual speech analysis (PSA), 3) nasometry, and 4) pressure-flow testing (PFT) when able.
Resonance is perceptually rated by a licensed speech language pathologist (SLP) on a scale from −3 (severely hyponasal) to + 3 (severely hypernasal). This assessment was made by a single SLP at each visit, and each assessment was made by one of three SLPs who participated in the VPD clinic during the study period. A nasometer (Nasometer II: 6200, 6400, or 6450) uses microphones near the upper lip (mouth) and nose separated by a sound shield to capture the ratio of nasal to nasal-plus-oral acoustic energy (multiplied by 100, represented as a percentage) during speech production, referred to as nasalance. Data is gathered during repetition of the “Zoo Passage,” a sample of all oral consonants void of any nasal productions, and the “Nasal Sentences Passage,” a series of sentences with a high load of nasal consonants. Alternatively, abridged samples can be used to gather valid nasalance data for patients who cannot fully participate or who have invalid Zoo Passage Scores due to known productions with a volitional open velopharyngeal port (eg, phoneme-specific nasal air emission; glottal stops). 15 Each nasometry passage and corresponding model has its own established normative range.15,16
Pressure Flow Testing (PFT) is a less commonly utilized test which yields an estimated size of the gap in the velopharyngeal port during phonation. As outlined in procedures described by Dobois, 17 patients produce repeated sounds including: /pa, pa, pa/, /pi, pi, pi/, and /hamper, hamper, hamper/, allowing for the potential gap in the velopharyngeal port to be measured during production of bilabial stop consonants in non-tensed vowel context, tensed vowel context, and adjacent to a nasal phoneme. Patients’ nasal pressure data are then captured via a nasal plug connected to a pressure transducer. Nasal flow data are also captured via a nasal mask connected to a pneumotachometer, and oral pressure data are captured via an oral catheter connected to a pressure transducer. The PERCI-SARS (Speech-Aeromechanics Research System) for Aerodynamic Assessment of Speech uses the hydrokinetic equation to yield the area of the velopharyngeal gap in millimeters squared in the various speech contexts. These are then averaged to obtain a single value for each phoneme.
Postoperative subjective and objective speech testing are performed routinely during the second postoperative visit at 6 to 12 months. This may also include nasopharyngoscopy. Over the study period, our team also transitioned to include this testing battery at the initial postoperative visit (3–6 weeks postoperatively). Additional evaluations are repeated at the surgeon's discretion, which in most cases takes place on a yearly basis until adulthood either within the VPD clinic or as a component of the cleft lip and palate multidisciplinary team evaluation.
Surgical Interventions
Multiple factors determine which surgery is recommended for each patient. These include: palatal mobility, length, muscle position and continuity, and the size and shape of the velopharyngeal gap as evaluated on nasopharyngoscopy. For this series of patients, larger defects and those with a sagittal orientation are usually managed with pharyngeal flap while smaller defects or those with a coronal orientation undergo other procedures such as injection pharyngoplasty, sphincter pharyngoplasty or Furlow palatoplasty, which are not included in this study. During the timeframe of this study, pharyngeal flap surgical technique variants included PFU, HF and PF.
At our institution, prior to performing PF or PFU surgery, an adenoidectomy is always performed at least 3 months before. Tonsillectomy may also be performed prior to VPI surgery if found to be enlarged and/or symptomatic, or by surgeon preference. To perform PFU, all of the initial steps of a traditional PF are performed. 18 (Figs 1a-1c) Then, the nasal surface of the uvular and distal soft palate mucosa is incised in the midline and unfurled. A tacking suture is then placed, through one side of the uvular flap, through the midline at the base of the pharyngeal flap, and then through the opposite side of the uvular flap. The suture is used to stretch the uvular flap to achieve maximum coverage. Additional tacking sutures may be placed when needed. Ideally, the uvular flap reaches the base of the pharyngeal flap where it meets the posterior pharyngeal wall. (Figure 1d) The technique is similar to that described by Winters et al. 19
Data Extraction and Outcome Measurements
Pertinent clinical data for the study were collected and managed using Research Electronic Data Capture (REDCap) tools hosted at the University of Arkansas for Medical Sciences.20,21 The data included: sex, age at time of surgery, date of surgery, type of PF surgery variant performed, performing surgeon, history and type of palatal cleft (CP, submucous CP, or no CP), presence or absence of 22q11 deletion, and preoperative speech and resonance measures. Outcomes included: post-operative speech and resonance measures, incidence of postoperative complications, incidence of OSA by polysomnogram (PSG), and incidence and type of revision surgeries. All patients were routinely screened for signs and symptoms of OSA in post-operative visits which was documented, and PSG was obtained when deemed appropriate by the clinician.
Although we planned to analyze differences between groups by PSA, PFT, and nasometry by both Zoo passage and Nasal Sentences passage testing, pre-operative Nasal Sentences testing data was absent for nearly all of the study subjects in one of the groups. Although a model could be constructed from the remaining data, the lack of pre-operative data in one group severely limited the value of model-based comparisons of this measure, and so the data for Nasal Sentences nasometry was later excluded.
Revision surgeries were subclassified into those that were intended for expansion of the nasopharyngeal airway (which included takedown of the pharyngeal flap and port dilation) and those intended for contraction of the airway (including port tightening by hemisphincteroplasty or injection using fillers such as hyodroxyapetite, and complete revision including flap takedown and replacement). When complete takedown and replacement was performed, this was tallied as a single revision, rather than two.
Visits where post-operative speech data were obtained were classified as early (4–18 months), and late (more than 18 months). Speech data collection was stopped after any patients underwent revision surgery. When multiple visits fell into any above category, the visit with the most available data was used, and if all visits were similar in this respect, the last visit in the timeframe was used for analysis.
Statistical Analysis
Statistical analysis was performed to compare surgical groups in terms of pre-operative demographic characteristics as detailed above, using chi-square test or Fisher's exact test as appropriate for dichotomous variables, and Wilcoxon-Rank-Sum test or Kruskal-Wallis as appropriate for continuous variables.
Post-operative dichotomous outcomes were analyzed using chi-square test and Fisher's exact as appropriate.
The effect of surgical technique on continuous objective speech related outcomes (nasometry and PFT) was performed using a mixed effect model for repeated measurements, with compound symmetry covariance structured for constant correlation, and Satterthwaite approximation to account for non-constant denominator degrees of freedom across mean differences. Comparisons across surgical techniques was performed by adding an interaction term to the model between technique and time. PSA was evaluated with a generalized linear mixed model for multinomial distribution and cumulative logit link to accommodate for the ordinal nature of the outcome.
The model was constructed using data from pre-operative, early and late data points.
Analyses were performed considering HF as a subtype of PFU, as both techniques represented lined flaps, compared to the PF alone. All statistical analyses were performed using SAS Enterprise Guide v7.1 (SAS Institute, Cary, NC) with a significance level set at p < 0.05.
Results
A total of 224 pediatric patients underwent either PFU (including HF) or PF during the study timeframe. 39 patients underwent surgery with a surgeon other than the three highest-volume surgeons, and were excluded. Four patients were excluded for iatrogenic causes of VPI including history of partial pharyngectomy or radiation therapy to the nasopharynx, and 21 were excluded due to follow-up <6 months. 160 patients met inclusion criteria for this study and underwent PFU (N = 119, including 18 HFs) or PF (N = 41).
There were several significant pre-operative differences between PFU and PF groups (Table 1) though no speech-related measures demonstrated any significant differences. Patients undergoing PF were significantly older (7.6 yrs vs 6.0 yrs, p = 0.037) and were less likely to have history of cleft lip (34% vs 53%, p = 0.047) or cleft palate (54% vs 73%, p = 0.048). The PF procedure was also used mostly by surgeon 1 (93% of total PF patients and 100% of surgeon 1's patients in this cohort).
Pre-Operative and Demographic Variables Between Groups.
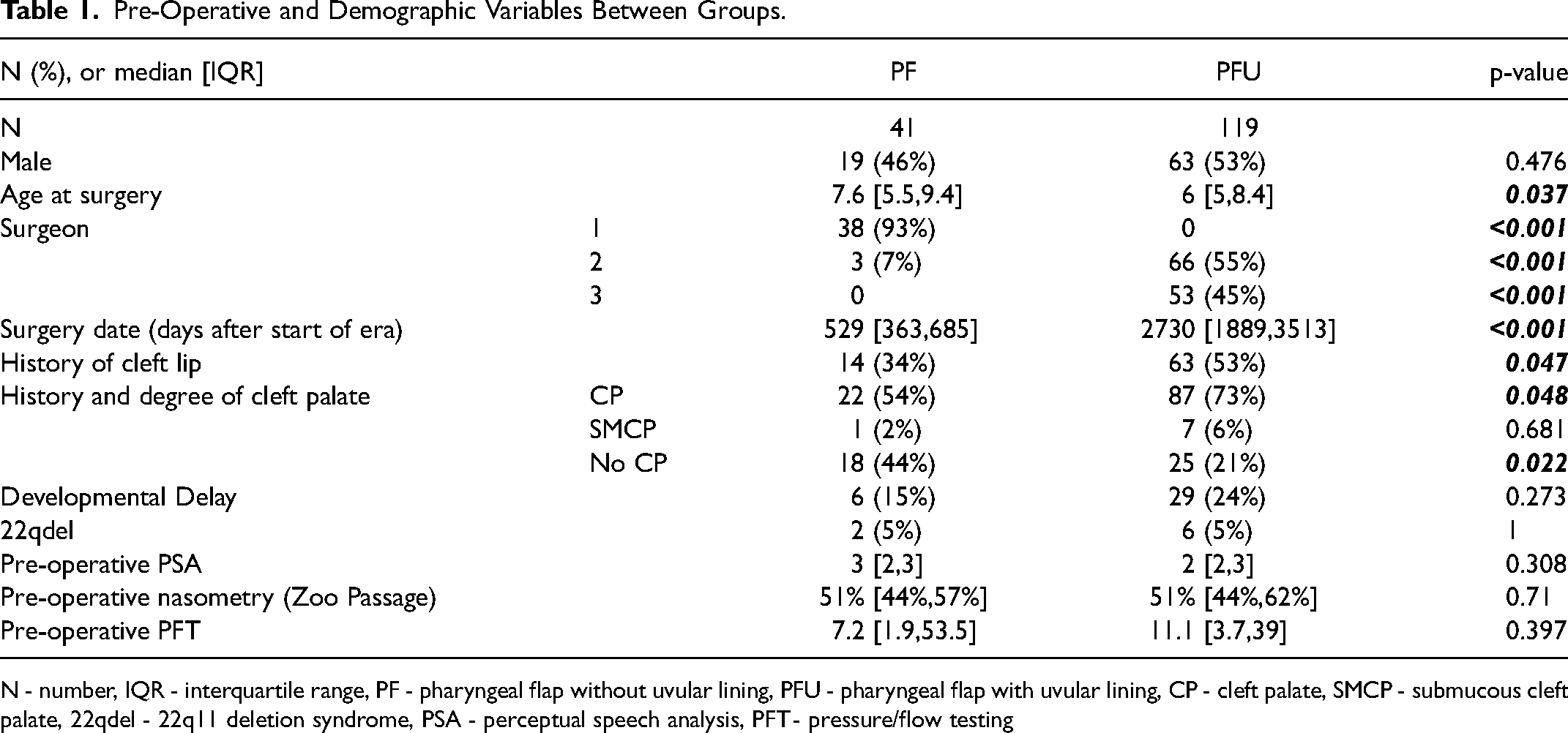
N - number, IQR - interquartile range, PF - pharyngeal flap without uvular lining, PFU - pharyngeal flap with uvular lining, CP - cleft palate, SMCP - submucous cleft palate, 22qdel - 22q11 deletion syndrome, PSA - perceptual speech analysis, PFT - pressure/flow testing
Post-operative outcomes showed OSA in 19 patients in the overall cohort, with no significant difference between PF and PFU groups (Table 2), although a trend toward significance was demonstrated in the different frequency of sleep studies obtained, with more PSGs obtained in the PF group (27% after PF, 13% after PFU, p = 0.056). There was no significant difference in complication rate (including incidence of OSA) between groups. Airspace expanding revision surgery was performed at similar rates between surgical groups (12% after PF vs 4.2% after PFU, p = 0.126), but airspace contracting revision surgery was significantly more common after PF compared to PFU (20% after PF vs 3.4% after PFU, p = 0.002). This contributed to a significant difference in number of patients undergoing at least one revision surgery of any kind (32% after PF vs 6% after PFU, p < 0.001). However, among those patients who had revision surgery, the PFU group had more revision surgeries per patient when compared to the PF group (median 1, interquartile range (IQR) [1,2] for PF vs. median 3, IQR [1,4] for PFU p = 0.032). Notably all five patients with PFU who underwent airspace expanding surgery underwent at least two balloon-assisted port dilation procedures. One patient in the PFU group and two patients in the PF group had developmental delay, and one patient in each group had 22q11 deletion.
Post-Operative Outcomes Between Groups.
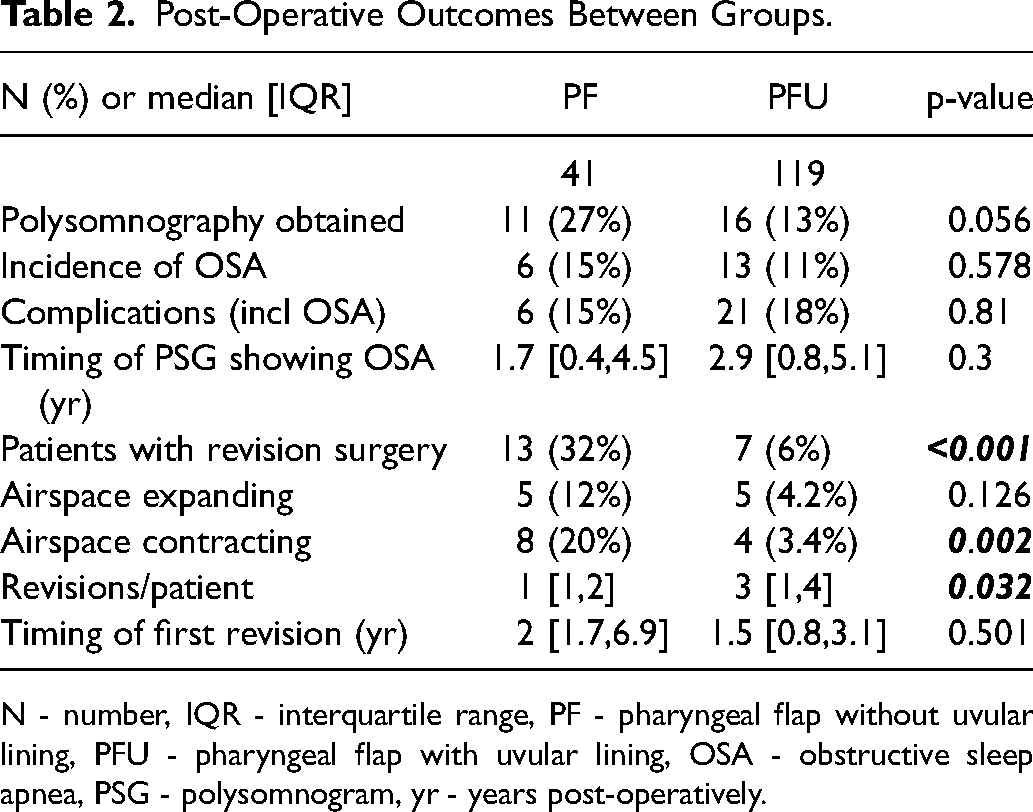
N - number, IQR - interquartile range, PF - pharyngeal flap without uvular lining, PFU - pharyngeal flap with uvular lining, OSA - obstructive sleep apnea, PSG - polysomnogram, yr - years post-operatively.
Two patients in the PFU group underwent both airspace expanding and contracting revision surgeries. In both cases an airspace contracting revision was performed first, followed by an airspace expanding revision.
There was no significant difference between PF and PFU groups with regard to the amount of speech-related data pre-operatively. However, significantly more speech-related testing data were available at the early timepoint (23/41, 56% vs 105/119, 88%, p < 0.001) in the PFU group. (Table 3) Significantly more data were available in the PF group in the late period (31/41, 76% vs 64/119, 54%, p = 0.017).
Pre- and Post-operative speech data.
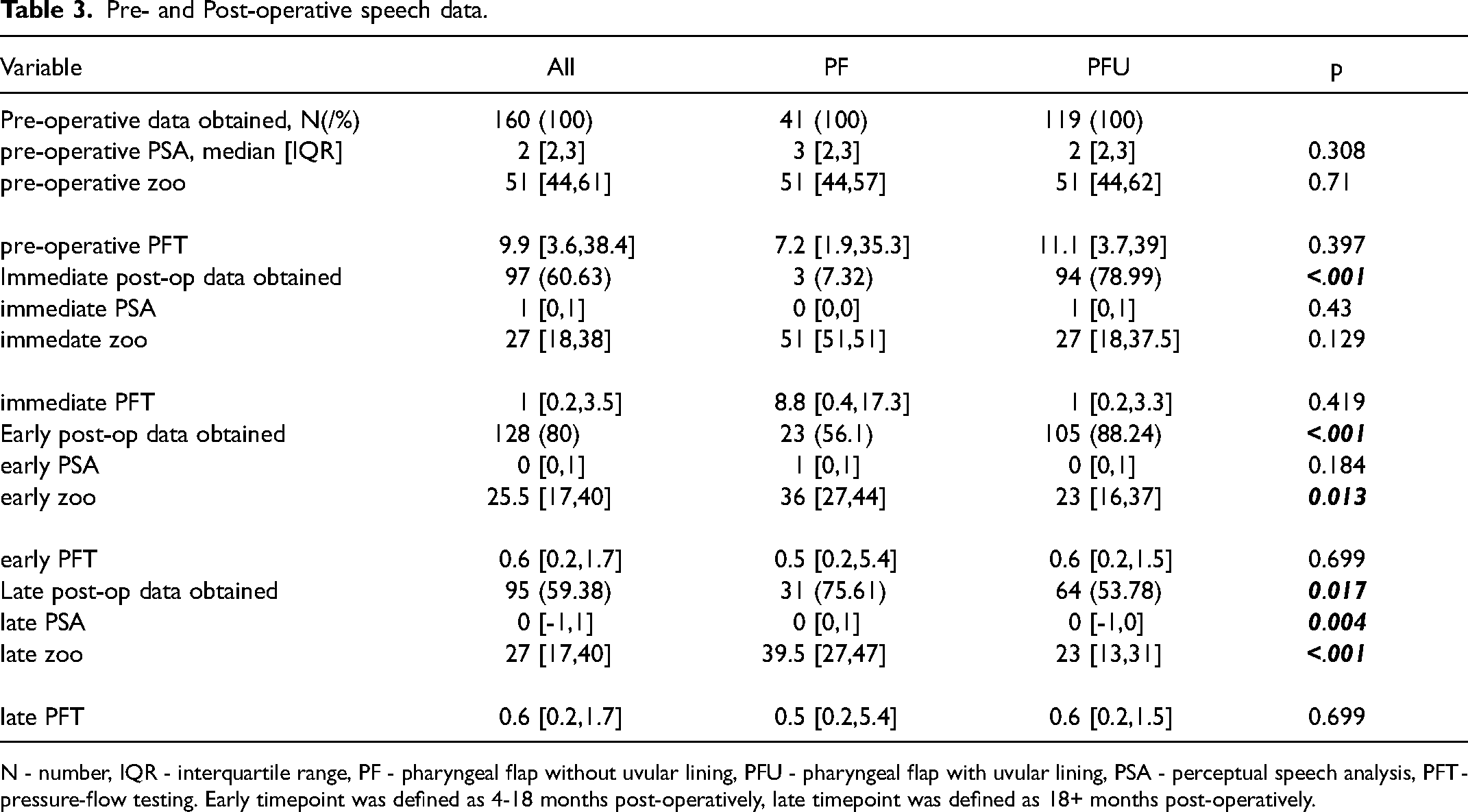
N - number, IQR - interquartile range, PF - pharyngeal flap without uvular lining, PFU - pharyngeal flap with uvular lining, PSA - perceptual speech analysis, PFT - pressure-flow testing. Early timepoint was defined as 4-18 months post-operatively, late timepoint was defined as 18+ months post-operatively.
Although post-operative data was plentiful, just a single pre-operative data point for Nasal Sentences nasometry was recorded for the PF group. As mentioned previously, Nasal Sentences nasometry data was thus excluded from the analysis.
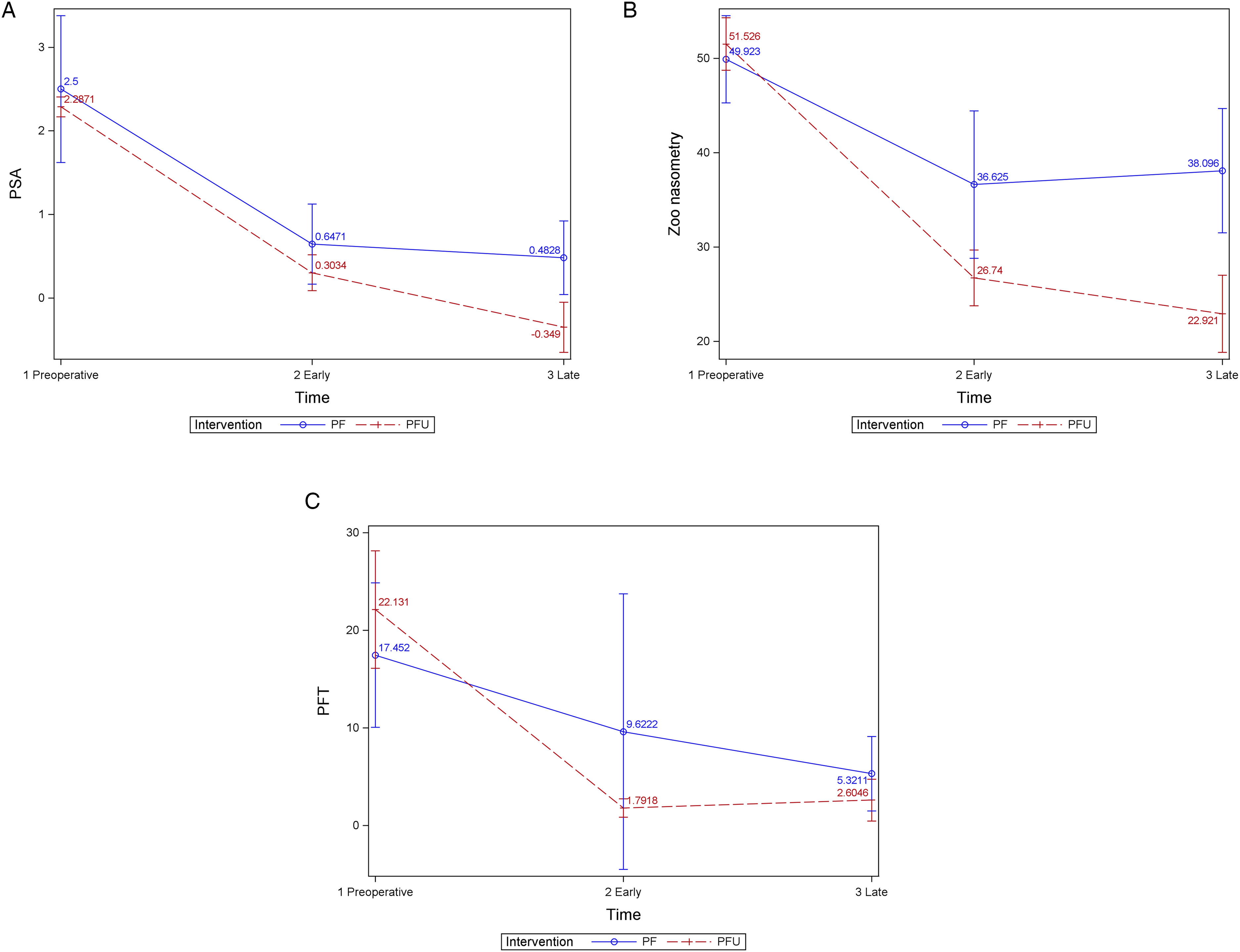
However, the mixed effects model showed significant improvement in PSA, zoo passage nasometry and PFT for all groups over time (p < 0.001). (Table 4a, Figures 2a-2c) There were significant differences found between the two surgical groups in PSA (p = 0.009) and zoo passage nasometry (p = 0.001), with bigger changes in both in the PFU group according to the mixed effects model.
Differences based on repeated measures model.
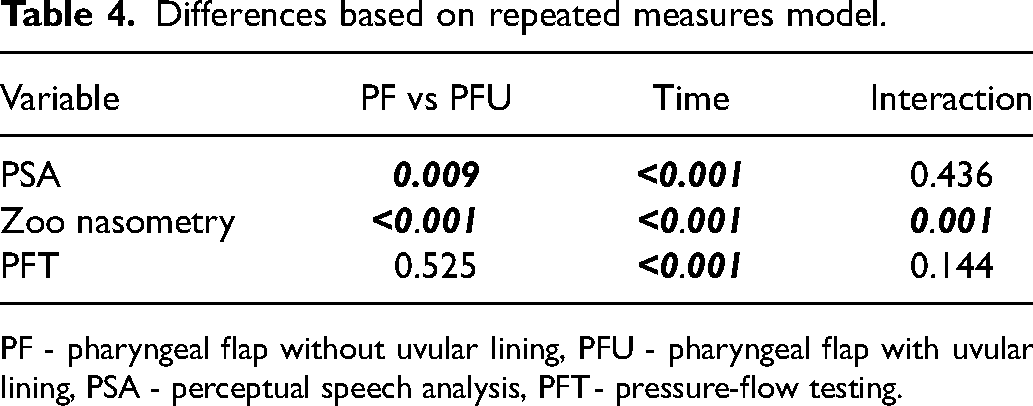
PF - pharyngeal flap without uvular lining, PFU - pharyngeal flap with uvular lining, PSA - perceptual speech analysis, PFT - pressure-flow testing.
The difference between surgical groups for zoo passage nasometry however was not independent of time (p = 0.001). In the context of the model, the significant interaction between surgical group variable and the time variable weakens the impact of surgical group on the difference in outcome.
Discussion
Pharyngeal flap surgery is a valuable surgical technique in the management of VPD. However, secondary intention healing of the raw undersurface of the pharyngeal flap has been suggested to lead to unstable preservation of flap width over time, which historically prompted exploration of the HF technique. 14 Other surgeons have explored the use of a uvular lining flap with the idea that “lining” the flap will reduce flap contracture. 19 However, prior to the present study, outcome comparisons have not been performed to evaluate whether these techniques achieve the desired stabilization of surgical results.
The present study reveals a lower rate of revision surgery in the lined flap (PFU) group compared to the unlined group (PF), driven in part by a four-fold difference in the rate of patients undergoing airspace contracting revision surgery, which is higher after PF. This supports the hypothesis that secondary intention healing and flap contracture may be contributing factors to poor outcomes after unlined pharyngeal flap surgery. These data also suggest that this problem is likely ameliorated by the addition of a uvular/mucosal flap coverage of the pharyngeal flap. Patients also had lower (less hypernasal) PSA scores after PFU, although the same difference was not consistently found for more objective speech measures according to the mixed effects model: PFT showed an improvement over time that was not different between surgical groups; and the differences between groups in zoo passage nasometry were impacted by significant interaction with the time variable.
Although risk of needing revision was lower after PFU, among patients with revisions, the PFU patients underwent a larger number of revision procedures per patient. In this group, there was a higher proportion of airspace expanding procedures performed, all of whom underwent at least two balloon-assissted port dilations (usually combined with steroid injection). Although this might indicate that balloon dilation was unsuccessful, in some cases these procedures were planned as a series, similar to balloon dilations for other types of airway stenoses. 22
We recognize that due to the retrospective nature of this study the patients were not randomized. SLPs performing pre- and post-operative assessments were also not blinded to surgical group, and inter- and intra-rater reliability for PSA was not evaluated. Small but significant differences were also noted in the groups’ pre-operative characteristics, including age, history of cleft lip, history of cleft palate, and surgeon. (see Table 1) The reasons that these groups would be different with regard to variables other than surgeon are not readily apparent to the authors.
The differences between groups with regard to surgeon, with surgeon 1 performing only PF and accounting for 93% of all PF procedures, reflects the progressive adoption of PFU at our institution over time. While the potential impact of different surgeons on the ultimate outcome should not be understated, some of this is somewhat mitigated by similar training pedigree and technique from all three high-volume surgeons. Both surgeons 1 and 3 trained in VPI surgical technique under surgeon 2, and the only documented consistent difference in surgical technique between operators was the use of uvular lining techniques. A multivariate analysis was attempted to assess the different impacts of surgical group and surgeon on surgical outcome. However, the degree of overlap between these two factors was too high to produce any meaningful results. It could therefore be argued that the differences shown in this study primarily demonstrate differences in outcome by surgeon rather than by technique. Unfortunately, gathering further data on this question is hampered moving forward at our institution due to our essentially-exclusive use of the PFU technique since it was initially adopted.
Cleft palate was more common in the PFU group
One statistical limitation of the of the fixed-effects model with repeated measures is that the time component was modeled as an ordinal variable. Categorizing our post-operative data points as early and late was an improvement over simple pre- and post-operative values, but greater granularity might have been achieved with a continuous variable model. It is notable that with other surgical techniques for VPI24,25 there can be considerable change in resonance over time post-operatively. Our cohort of patients could have experienced similar changes in resonance within the time periods we arbitrarily defined (4–18 months, > 18 months).
Younger age at the time of PF surgery has been associated with better improvements in articulation outcomes in one previous study. 10 However, intergroup comparisons in the study were only significant when comparing groups younger that 10 years to patients older than 21 years, and the authors did not comment on revision rate. Our data includes only patients under 18, and the difference in mean age between groups was just 1.6 years. However, this difference could have improved PFU group outcomes, as this group was younger on average at the time of surgery.
We primarly accredit the differences in surgical outcomes and revision rate to the utilization of the uvular lining techniques. The additional elevation and suturing of the uvular mucosal flap to line the raw surface of the PF does not require much additional operating room time (we roughly estimate 10–15 min for PFU and 20–25 min for HF, although this was not measured in this study and impossible to determine retrospectively with available data or possible to determine with our data). The additional step more importantly does not increase the risk of complications in this study. We feel these data validate our institutional preference for the uvular lining flap as a way to reduce hypothesized unwanted secondary intention healing and narrowing that can contribute to persistent or recurrent VPI
OSA is a potential complication of pharyngeal flap surgery. A meta-analysis of retrospective data demonstrated OSA in 5.1% of post-operative patients (de Blacam 2018) after PF, though studies varied widely in this incidence from 0–43%. It is notable that the above overall rate of OSA is not drastically higher than the estimated 1–4% prevalence in the general pediatric population, 26 and it is lower than the 8.5% prevalence in those with history of repaired cleft palate. 27 In our cohort, the incidence of PSG-confirmed OSA was 12%. Although an otolaryngologist routinely screened each patient post-operatively for signs and symptoms of OSA, a PSG was not performed for all patients. The reasons for a higher rate of OSA than other studies is not clear, but all of our surgeons in this study are otolaryngologists that treat OSA in other settings, which may have led to a higher index of suspicion for this disease at baseline and thus more sleep studies performed.
This study incorporated the HF technique into the PFU group, but further study comparing these two techniques may be warranted to investigate whether the gains from the use of uvular lining are further amplified by the more aggressive HF technique.
Conclusion
The application of a uvular lining flap technique may improve subjective (and some objective) speech outcomes while reducing the necessity for revision surgery after pharyngeal flap. Pharyngeal flap with uvular lining is a safe procedure with fairly low rates of postoperative complications with no differences in complication rate found between lined and unlined flaps.
Footnotes
Acknowledgements
Elizabeth Cottrill, MD; Maria Melguizo-Castro, MS.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article