
Abstract
Objective
Measuring disability as a concept of impaired global function enables beneficiaries of treatment, the impact of treatment, and targets of health system investment to be rigorously assessed. Measures of disability are not well established for cleft lip and palate. This study aims to systematically review disability weight (DW) studies pertaining to orofacial clefts (OFCs) and identify methodological strengths and shortcomings of each approach.
Design
Systematic literature review of studies that met the following criteria: (1) peer-reviewed publication, (2) focus on disability valuation, (3) mention orofacial clefts, and (4) publication January 2001-December 2021.
Setting
None.
Patients/Participants
None.
Interventions
None.
Main Outcome Measure(s)
Disability weight method of valuation and the value itself.
Results
The final search strategy yielded 1,067 studies. Seven manuscripts were ultimately included for data extraction. The disability weights used in our studies, including those newly generated or taken from the Global Burden of Disease Studies (GBD), ranged widely for isolated cleft lip (0.0–0.100) and cleft palate with or without cleft lip (0.0−0.269). The GBD studies limited their consideration of cleft sequelae informing disability weights to impact on appearance and speech-related concerns, while other studies accounted for comorbidities such as pain and social stigma.
Conclusions
Current measures of cleft disability are sparse, inadequately reflect the comprehensive impact of an OFC on function and socialization, and are limited in detail or supporting evidence. Use of a comprehensive health state description in evaluating disability weights offers a realistic means of accurately representing the diverse sequelae of an OFC.
Keywords
Introduction
Multidisciplinary cleft care strives to provide longitudinal surgical and non-surgical support aimed at optimizing the quality of life for children born with cleft lip/palate. Modern interdisciplinary cleft teams are thought to often achieve this aim with high degrees of success. 1 Nevertheless, cleft care specialists are acutely aware of the disability associated with unrepaired or inadequately repaired clefts and suboptimal team care. In settings where cleft care is not accessible, a cleft lip or palate imparts devastating stigmatization due to an altered appearance as well as speech, hearing, breathing, nutritional, and other forms of orofacial dysfunction. Furthermore, cleft-related mortality, abandonment, and infanticide is widely reported across 27 countries and multiple world regions.2,3
Variable outcomes following surgical treatment of orofacial clefts (OFCs) can have multifactorial causes, with elements such as patient selection and preparation, surgical proficiency, postoperative follow-up, and access to additional services (eg, specialized pediatric medical care, nutritional counseling, dental education, and disease prevention, audiologic care, speech pathology and therapy) all contributing to the ultimate result. For instance, the burden of post-operative fistulae is reported at rates of up to 23% in high income countries (HICs) and 57% in low-middle income countries (LMICs),4,5 with potentially profound associated functional and psychosocial sequelae. Patient-reported outcomes have become increasingly important in evaluating cleft care,6–9 yet their findings have not yet been translated into terms that can quantify disability in a standardized fashion. Moreover, despite the large volume of cleft care that occurs on an international scale, there is a paucity of comparable data capturing treatment outcomes and quality of life (QoL) among patients with clefts. Valuable efforts are being made by organizations such as EuroCleft, ScandCleft, AmeriCleft, Cleft Collective, and CORNET to audit cleft outcomes, although through different approaches.
Disability is increasingly used in public health and medical system spheres as the key metric for quantifying mental and physical barriers attributable to a medical condition and the resultant limitations of patient capability. Quantification of disability directs prioritization of health care funding and is the basis for valuing impact vis-à-vis investments. Accurate valuation of disability is particularly important for congenital and pediatric conditions as disability is amortized across an entire lifetime. Thus, the burden of suffering—and opportunity for improvement—is proportionally greater for pediatric conditions. However, the concept of disability does not seem well-established for cleft lip/palate conditions. To be sure, clinicians tend to focus on enabling “ability” rather than emphasizing or enumerating “disability” for their patients. Questions in this discourse that remain unanswered include, “what aspects of treated or untreated cleft/lip palate conditions constitute disability?”, and “what are the most effective surgical or non-surgical methods of alleviating disability?”
An internationally accepted metric for quantifying disability due to a given cause is the Disability Adjusted Life Year (DALY), which represents the loss of the equivalent of one year of full health. This is calculated as the sum of the years of life lost due to premature mortality (YLLs) from that cause and the years of healthy life lost due to disability (YLDs). Disability weight (DW) is a weighting factor for YLDs that reflects the severity of a disease on a scale of 0 to 1, with 0 representing a state of perfect health and 1 representing a state equivalent to death.
The Global Burden of Disease (GBD) employs the aforementioned terms to quantify health loss from hundreds of diseases, injuries, and risk factors, including OFCs, so that health systems can be improved, and disparities can be eliminated. The GBD's efforts are aimed at helping policymakers understand the true nature of their country's health challenges and intentionally direct their efforts; therefore, their methodology has significant global health implications.
Delineating the concept and degree of disability experienced by patients with cleft lip/palate is critical for informing patient-level care and global health policy, including allocation of resources to cleft care. A clearer understanding of the impact of cleft disability has implications for global cleft care, including prioritization of efforts for future clinical and research work. Thus, this study aims to systematically review DW studies pertaining to OFCs and critically identify methodological strengths and shortcomings of each approach. Our hypotheses are that (1) the concept of disability and disability weights have not been robustly developed for cleft conditions, (2) nascent efforts at disability weighting are likely highly variable, and (3) cleft conditions may be underestimated by broader attempts at disability weighting across healthcare.
Methods
In accordance with guidelines from the Cochrane Collaboration 10 and PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analyses; Figure 1) a PubMed revised search strategy was developed with an accredited librarian to query all manuscripts describing quantification of cleft lip/palate disability. Eligibility criteria included (1) peer-reviewed publication in English, (2) focus on disability valuation, (3) mention of orofacial clefts (eg, cleft lip and palate, isolated cleft lip, isolated cleft palate, rare facial clefts), and (4) publication between January 2001 and December 2021.
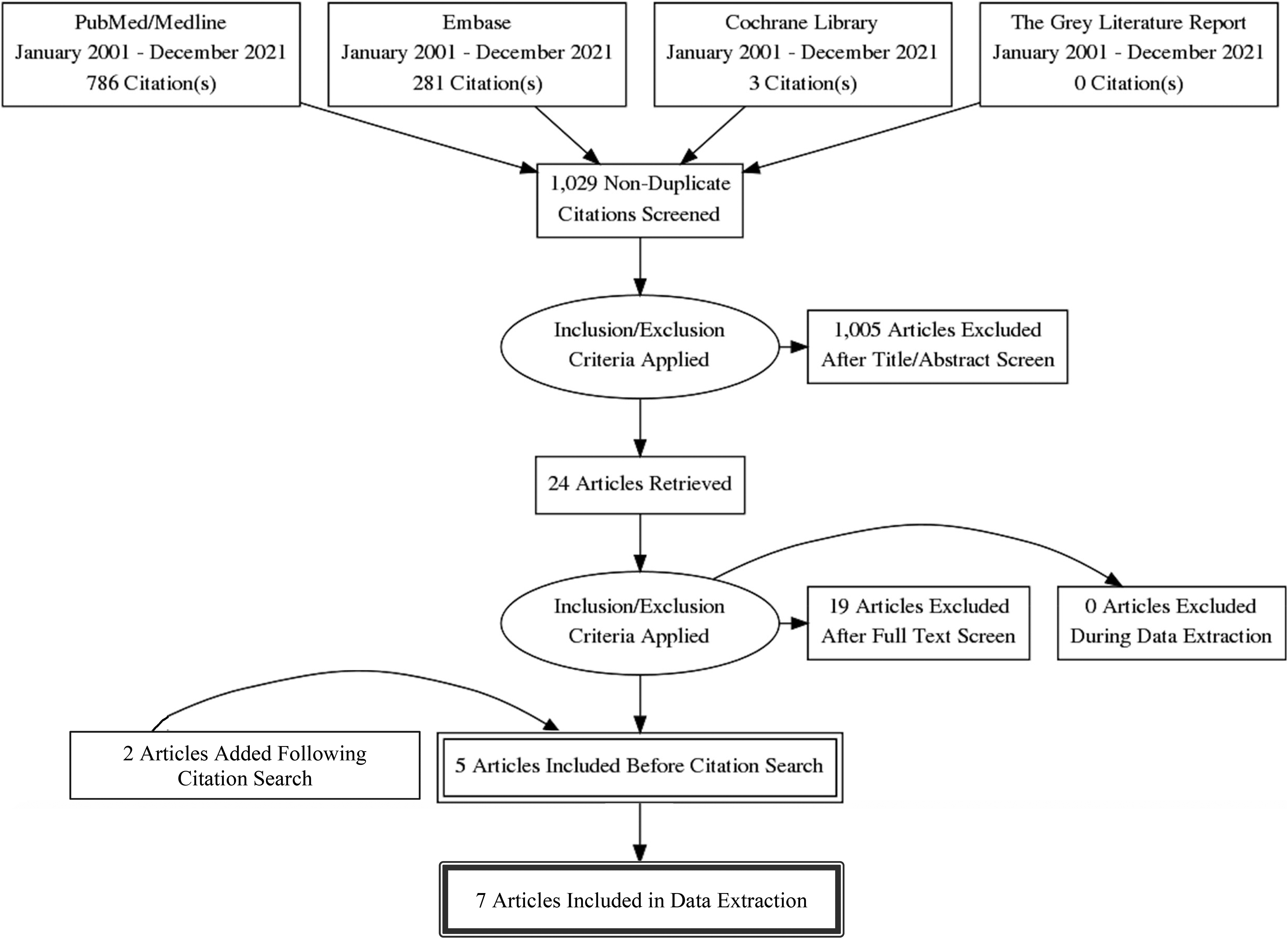
Cleft disability PRISMA flow diagram.
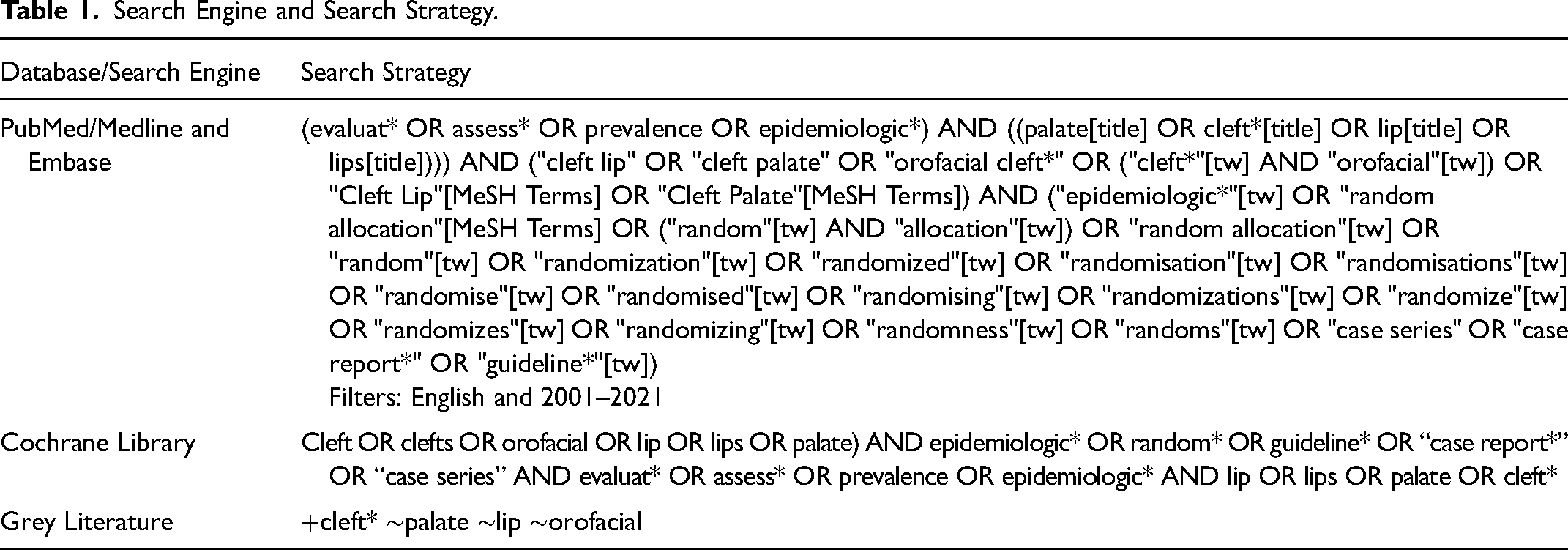
Studies were identified through electronic searches using PubMed/Medline, Embase, Cochrane Library, and The Gray Literature. The constructed search strategies can be viewed in Table 1.
Search Engine and Search Strategy.
The final search strategies were run on December 8, 2021. Covidence, a web based systematic review manager for text screening and data extraction, was used by two independent reviewers to screen abstracts and full texts. Any disagreement between reviewers was reconciled by re-evaluation of the full text and discussion until a consensus was reached.
Cohen's Kappa coefficients were calculated to determine interrater reliability. Studies describing specific elements of disability related to OFCs (eg, speech disorder) outside the context of DWs and DALYs were excluded.
Extracted data included publication year, authors, country, OFC disability weight, disability assessment methodology, source of DW, aim, methodology, results, and conclusion.
Additionally, the GBD Study Data Resources for the years 2010 through 2019 were reviewed to assess iterative DW valuations, case definitions, and associated health states for OFCs, and the modeling strategy and model settings.11–17
Analyses were conducted using SPSS Version 27.0 (IBM Corp, Armonk, NY) and Microsoft Excel 2019.This study was exempt from Institutional Review Board review at the Children's Hospital of Philadelphia.
Results
Systematic Review
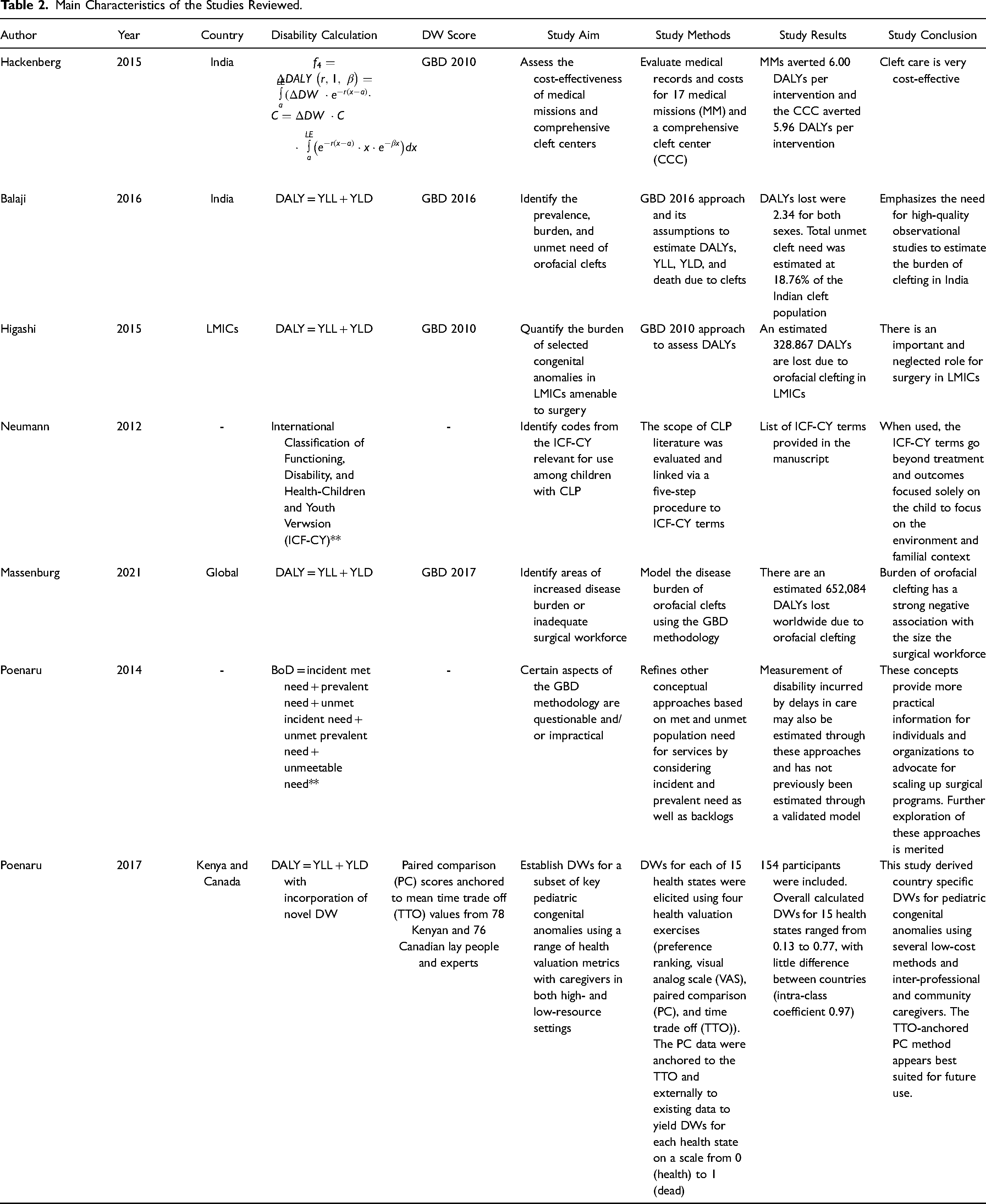
The final search strategy yielded 1067 studies on December 8, 2021. Covidence systematic review manager automatically removed 38 duplicates. One thousand and twenty-nine abstracts were screened by reviewers and 1,005 were excluded that did not pertain to cleft disability weights. Reviewers were dedicated craniofacial researchers with a background in global health. Twenty-four full texts were evaluated, of which 19 were excluded (all full manuscripts that did not mention DWs or DALYs). Our search strategy yielded five manuscripts that met inclusion criteria, and an additional two manuscripts were added following citation search (Table 2).
Main Characteristics of the Studies Reviewed.
Proportionate rater agreement was 91.4% for abstract screening and 100.0% for full text screening. Cohen's Kappa coefficient for interrater reliability was 0.90 for abstract screening and 1.00 for full text screening, demonstrating sufficient interrater reliability. 18
Studies
All studies spanned the past decade (2012–2021) and were published following the original GBD study in 1996. 19 One study described a series of standardized codes that can be used to describe cleft-related disability. 20 Two studies (28.6%) were purely conceptual, without quantitative measurement of DWs or DALYs for a specific country or region.20,21 Another two studies (28.6%) evaluated DALYs in India, with one assessing the cost effectiveness of medical missions 22 and another identifying the prevalence, burden, and unmet need of OFCs. 23 The remaining three studies assessed the global burden of unmet OFC care, 24 the burden of OFC care requiring surgical treatment in low- and middle-income countries (LMICs), 25 and the process for generating novel DWs in Kenya and Canada. 26
Methodological Design Choices to Render the Disability Weights and DALYs
Three studies calculated DALYs using the traditional equation of DALY = years of life lost (YLL) + years lived with disability (YLD). For DWs, each of these three studies used values from a different year of the GBD study, including 2010, 2016 and 2017. Of note, the DWs reported in 2010 did not change in any iteration until 2013 and then again in 2019 (see Results).
The study by Hackenberg et al. suggested an alternative integral equation for DALY calculation using DWs from the GBD 2010 study (Table 2) and adapting the original equation from Murray and Alkire.22,27,28 The variables of interest in the latter equation were age of participant at the time of surgery, medical diagnosis for which intervention was provided, and procedure received. 22 Life expectancy was based on the 2009 country-specific World Health Organization (WHO) life tables for India.
Two studies were published by Poenaru et al., the first in 2014 and the second in 2017.21,26 The first of these studies proposed a new conceptualization of burden of disease (BoD) which breaks “need” down into incident met need, prevalent need, unmet incident need, unmet prevalent need, and unmeetable need. 21 The more recent Poenaru study generated new DWs for pediatric congenital anomalies which the GBD had not addressed as of 2017 (eg, hypospadias and Hirschsprung's disease before and after colostomy). 26 This study essentially replicated the GBD approach to DW assessment, relying on paired comparison (PC) scores anchored to mean time trade off (TTO) values from Kenyan and Canadian lay people and experts. Furthermore, case descriptions of cleft lip and palate were provided to respondents (Appendix 1), similarly to the GBD model. OFCs were amongst the diagnoses measured by both the GBD and Poenaru studies, allowing for anchoring and comparison between outcomes.
Lastly, the study by Neumann et al. in 2012 describes the application of the International Classification of Functioning, Disability, and Health-Children and Youth Version (ICF-CY) to cleft lip and palate, outlining codes which can be used to standardize communication between interprofessional teams treating OFCs. 20
Disability Weight Valuation
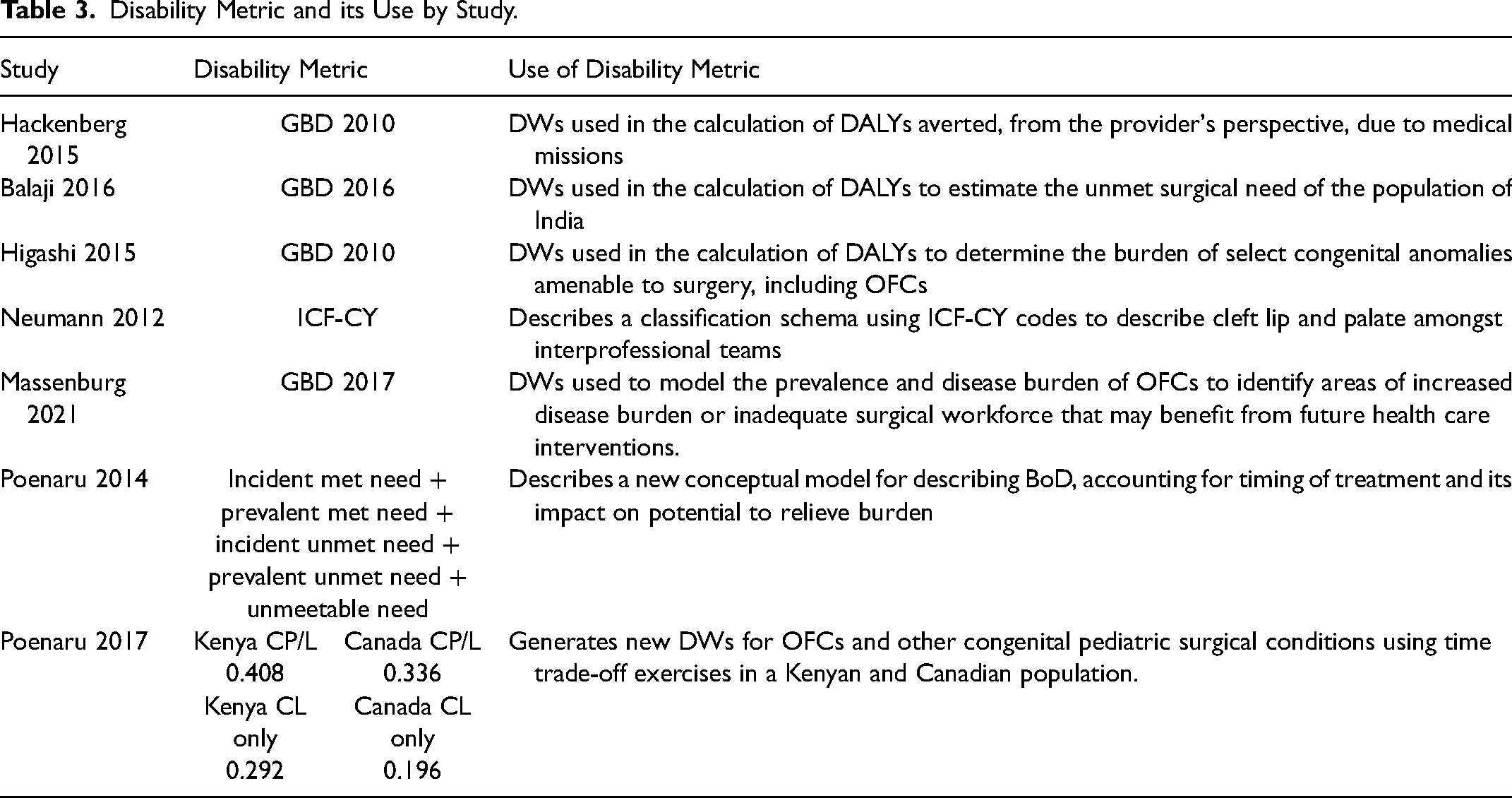
The most common sources for DWs were cited as the GBD 2010 (n = 2), 2016 (n = 1), and 2017 (n = 1) studies (Table 3). DWs are calculated by the GBD based on the valuation of different health states through a global survey of lay people and experts using paired comparisons (PCs) and scaled from 0 (perfect health) to 1 (death). This methodology was adapted following previous criticism of their original approach which only incorporated expert opinion. 29 The terms used by the GBD to describe and stratify OFCs are as follows:
Disability Metric and its Use by Study.
In the literature applying these DWs, disfigurement level 1 has been described as a “repaired or incomplete OFC with lasting sequelae of an OFC”. Disfigurement level 2 has been equated to an “unrepaired, symptomatic OFC”, whereas an asymptomatic OFC is one with “no sequelae”. 24
Note: all values are on a scale of 0 (perfect health) to 1(death):
The DWs described in Disfigurement level 1 (DW: 0.013, range 0.006–0.025) Disfigurement level 2 (DW: 0.072, range 0.048–0.103) Disfigurement level 1 due to OFCs (DW: 0.011, range 0.005–0.021) Disfigurement level 2 due to OFCs (DW: 0.067, range 0.044–0.096) Asymptomatic OFCs (DW: 0.0) Disfigurement level 2 and speech problems due to orofacial clefts (combined DW: 0.051, range 0.032–0.078). Disfigurement level 1 due to OFCs (DW: 0.011, range 0.005–0.021) Disfigurement level 2 due to OFCs (DW: 0.067, range 0.044–0.096) Disfigurement level 2 and speech problems due to OFCs (combined DW: 0.115, range 0.076–0.164)
Between
The 2013–2018 DWs were used consistently until the publication of new DWs published in the GBD
The DWs used in these studies, including those newly generated or taken from the GBD, ranged widely for isolated cleft lip (0.0–0.100) and cleft palate with or without cleft lip (0.0–0.269) (Table 3).24,26 Average DWs were greater for both cleft lip (0.100) and cleft palate (0.269) using the method described by Poenaru et al. in 2017, compared to the GBD method (minimum 0.0 for an asymptomatic cleft and maximum 0.164 for an unrepaired cleft with speech difficulties).15,17,26
Thinking about the components of a DW, the GBD studies limited their consideration to general impact on appearance and speech-related concerns, while Neumann et al. accounted for body structures, body functions, activities and participation, environmental factors, and personal factors. 20 Furthermore, Poenaru et al. 2017 accounted for issues with movement, self-care, activities of daily living (eg, eating, pain and discomfort, anxiety or depression, social stigma, cognitive problems, and evacuation problems). 26
Lastly, it is important to clarify that objective appearance and body image/adjustment are not linearly related. The term “disfigurement” is not clearly defined by the GBD which creates a space for misinterpretation and conflation of appearance with function. 30
Discussion
Several key findings emerged from this systematic analysis of disability valuation in cleft lip/palate. First, there is an overall paucity of disability data for cleft lip/palate conditions, despite it being one of the most common congenital anomalies, with functional limitations affecting patients of all ages. 31 Second, there is high variability in the disability weights that are reported. There are very few primary studies or examples of transparent, reproducible research supporting the disability weights that do exist. Third, there tends to be underrepresentation of the multifaceted ways in which disability is associated with orofacial clefts – including a myriad of aspects of psychological distress for affected patients. This is particularly true in the GBD reports, which dominate this discourse.
Disability Weights
Comparing studies that incorporate DWs and DALYs showed variation in OFC categorization, assessment, and valuation. This review illustrates that there are a range of methods used to derive disability weights; however, most studies rely on a simplified disease-specific description of the health state, using values obtained from one of the iterative GBD studies. The valuation of DWs has continued to evolve over time, incorporating additional disease states and modifying the panel of evaluators from exclusively health experts to a broader audience. The values of DWs provided by the GBD are lower than those described using alternative methods of DW valuation and account for a limited number of disease sequelae (impact on appearance and speech problems) compared to other studies in our review.20,22,26
Contextualizing DWs is essential to appreciating the extent of under- or overestimation in its valuation. For this purpose, the GBD 2019 DWs provide a useful reference. The value for level 1 disfigurement, essentially describing a repaired or incomplete OFC with lasting sequelae, is cited as 0.011 out of 1, equivalent to a 1.1% reduction from full health. This value is identical to that of “borderline intellectual disability with congenital heart disease due to other chromosomal abnormalities,” “recurrent urinary tract infections or other abdominal issues due to congenital anomalies of the urinary tract,” and “chronic abdominal pain due to congenital diaphragmatic hernia,” amongst others. The DW for disfigurement level 2 or an “unrepaired, symptomatic OFC,” is cited as 0.067, which is equivalent to the value of “symptomatic, benign prostatic hyperplasia,” “severe alopecia areata,” and “severe viral warts,” to name a few.
Methodological Issues in Disability Weighting
Reproducibility of what can be a subjective appraisal, balancing simple versus comprehensive assessment tools, and varying social constructs of disability are all challenges in disability weighting. Commentary in The Lancet Global Health described uncertainties in disability valuation, citing GBD contributor Joshua Solomon's observation that “in some cases, responses are evidently highly sensitive to particular details in these descriptions,” with “these descriptions” referring to the provided health state description. An example of this is illustrated by the 2010 GBD study for which deafness was assigned the weight of 0.03 and being in a wheelchair with a spinal cord lesion below the neck was assigned the weight of 0.05. These implausibly low ratings were attributed to respondents thinking that these individuals had disability rather than poor health. The descriptions were revised for the 2013 study and weights then became 0.22 for deafness and 0.30 for being in a wheelchair with a spinal cord lesion. 32 While subjectiveness in value judgments is inherent to the disability weighting process, ten-fold fluctuations in weightings as seen here attest to the limited internal consistency and reliability of current measurement methods.
Although an “expert panel” and lay people were consulted in the generation of most DWs, insufficient granularity is provided by the GBD to know whether any experts in cleft and craniofacial care or patients with OFCs were involved. Nevertheless, we would be remiss not to acknowledge that the GBD's inclusion of lay people in the valuation process is a tremendous strength, capturing a presumably less biased perspective on a condition's associated disability. However, a thorough description, delineating the nuances of cleft lip and palate and associated comorbidities, is essential to accurately evaluate the resultant disability. If evaluators conceptualize OFCs as a quick-fix, straightforward surgical repair without considering its broad clinical and psychosocial implications, we will continue to underestimate its severity.
Poenaru et al. provides a health state description that begins to capture the complexity of OFCs: “All children with cleft lip and palate need surgery. Some will be fine after one surgery, but most will need more surgeries to fix not only the lip or palate, but also the teeth, nose, and ears”. 26 Nevertheless, there is no reference in this description to the speech disorders or the psychosocial burden of OFCs, which has been associated with increased behavioral problems, depression, and anxiety, each which possesses its own disability weight (Figure 2). 33 Although the majority of patients with an OFC will not have a DSM-5 diagnosable mental illness, it is critical to account for the broader psychosocial impact of an OFC on the patient and their community (eg, bullying, frequent trips to a specialist, time missed from school for the patient, time missed from work for the caregiver, family adjustment to diagnosis, stigmatization based on appearance and speech differences). Incorporating these psychosocial considerations into DW valuation could be easily accomplished by a more comprehensive health state description that situates OFCs as more than just a surgical disease.
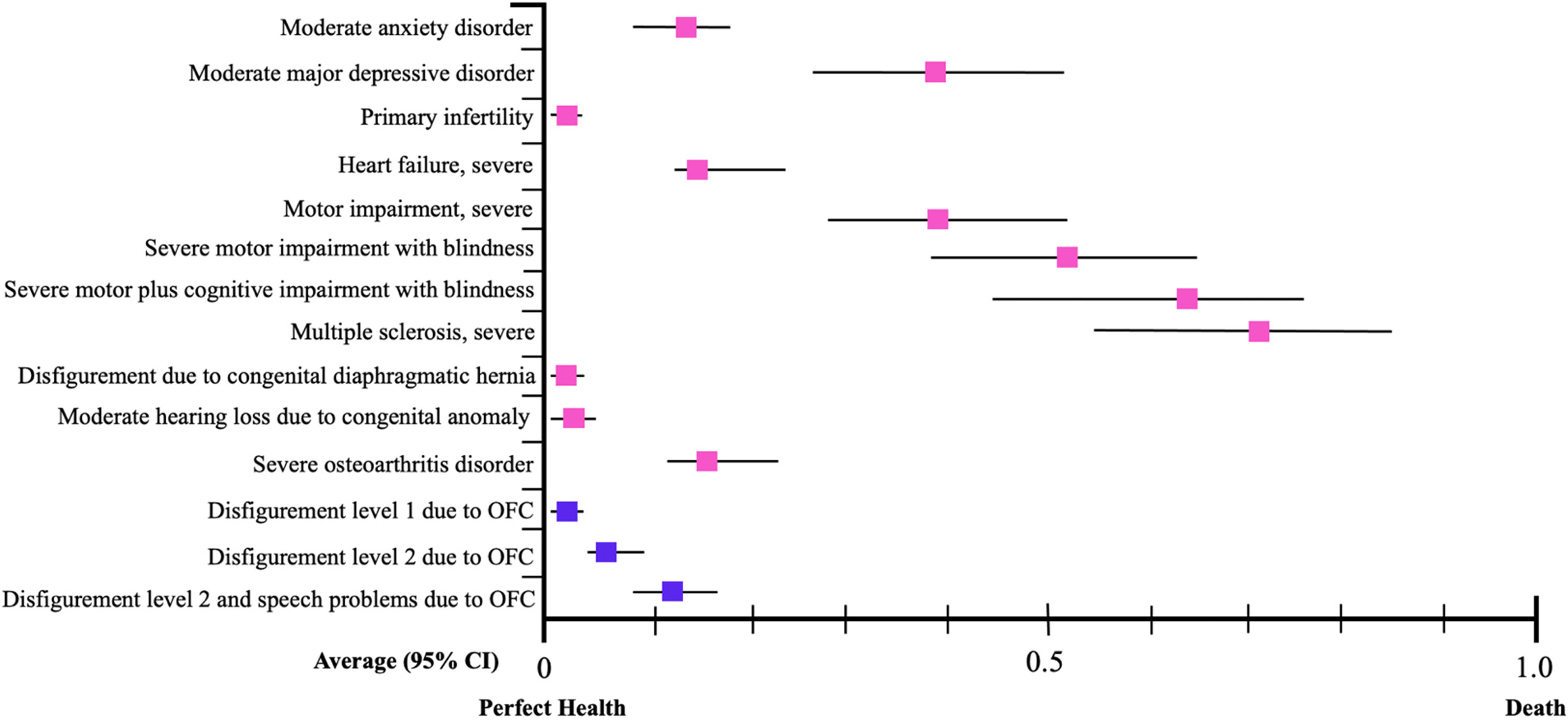
GBD Disability weights by disease including OFC (purple) and non-OFC (pink) health states.
An additional shortcoming of the use of DWs is the lack of distinction of quality of surgical repair. Although there is no formal definition for what constitutes “adequate” repair, at a minimum, there should be anatomic re-creation of the normal lip and/or palate elements with good velopharyngeal function and harmony of the central philtral element. 34 Inadequate repair of a cleft lip or palate threatens aesthetic outcomes and inadequate oronasal function, which may leave the patient in a similar or worse state than prior to surgery. Considering non-negligible complication rates (between 2 and 16%)34–38 that are considerably higher in low resource settings, 35 the prevalence of inadequately repaired OFCs and resultant disability must be considered when calculating the overall BoD.
Furthermore, the spectrum of morbidity that may result from a cleft lip and/or palate is extremely varied depending on phenotypic severity (eg, Veau classification, laterality), 3 syndromic status, 39 quality of the repair, 3 as well as personal and environmental factors. 40 Beyond the measurable outcomes of surgical repair, access to comprehensive cleft care galvanizes the functional potential of the individual with an orofacial cleft. An inadequate initial repair or poor post-operative management can result in complications such as palatal fistulae, which are often difficult to repair and can have a notable impact on quality of life. 4 As is suggested by Hackenberg et al.'s methodology, the timing of repair is also a critical consideration, requiring a delicate balance between optimization of speech development without unnecessary sacrifice of midfacial growth potential. 41 Furthermore, addressing complications related to feeding difficulties, hearing loss, poor dentition, and psychosocial well-being is essential to providing the gold-standard, comprehensive cleft care that all patients deserve. 42
Cleft-Related Disability and Low-Resource Settings
Due to advancements in public health and medicine, many previously fatal conditions are now characteristically chronic (eg, HIV, some cancers). With this shift toward increased longevity with long-term illness, we can expect the YLD (years lived with disability) component of the DALY equation (DALY = YLL + YLD) to become a proportionally larger contributor than YLL (years of life lost). However, for OFCs, failure to account for associated comorbidities will underestimate the YLD factor of the DALY equation, negatively impacting domestic and international efforts to treat OFCs.
This underestimation of OFC-related disability will have a greater impact on LMICs. For context, the prevalence of orofacial clefting was estimated to be 10.8 million people in 2017, representing a disease burden of 652,084 DALYs, with 91.4% of this disease experienced by low- and middle-income countries. 24 The countries with the highest disease burden measured via DALYs per 100,000 population include Burundi (89.14), Central African Republic (71.90), and Sierra Leone (57.44), despite having the lowest disease prevalence of any other region (sub-Saharan Africa: 1.03 cases per 1000 population). This discrepancy between disease burden and available resources is at the core of the argument for appropriate disability valuation given its importance in informing resource allocation and prioritization on an international level.
Our ability to conceptualize the impact of a cleft diagnosis more accurately could provide support for the medical necessity of cleft surgical, orthodontic/dental, speech, and other components of multidisciplinary care. Even well-resourced families can struggle to access interventions due to insurance limitations, and this impact is likely much greater in lower resourced areas. We must emphasize that a cleft is not a cosmetic condition, but one that can have a significant and lasting impact on a patient's quality of life.
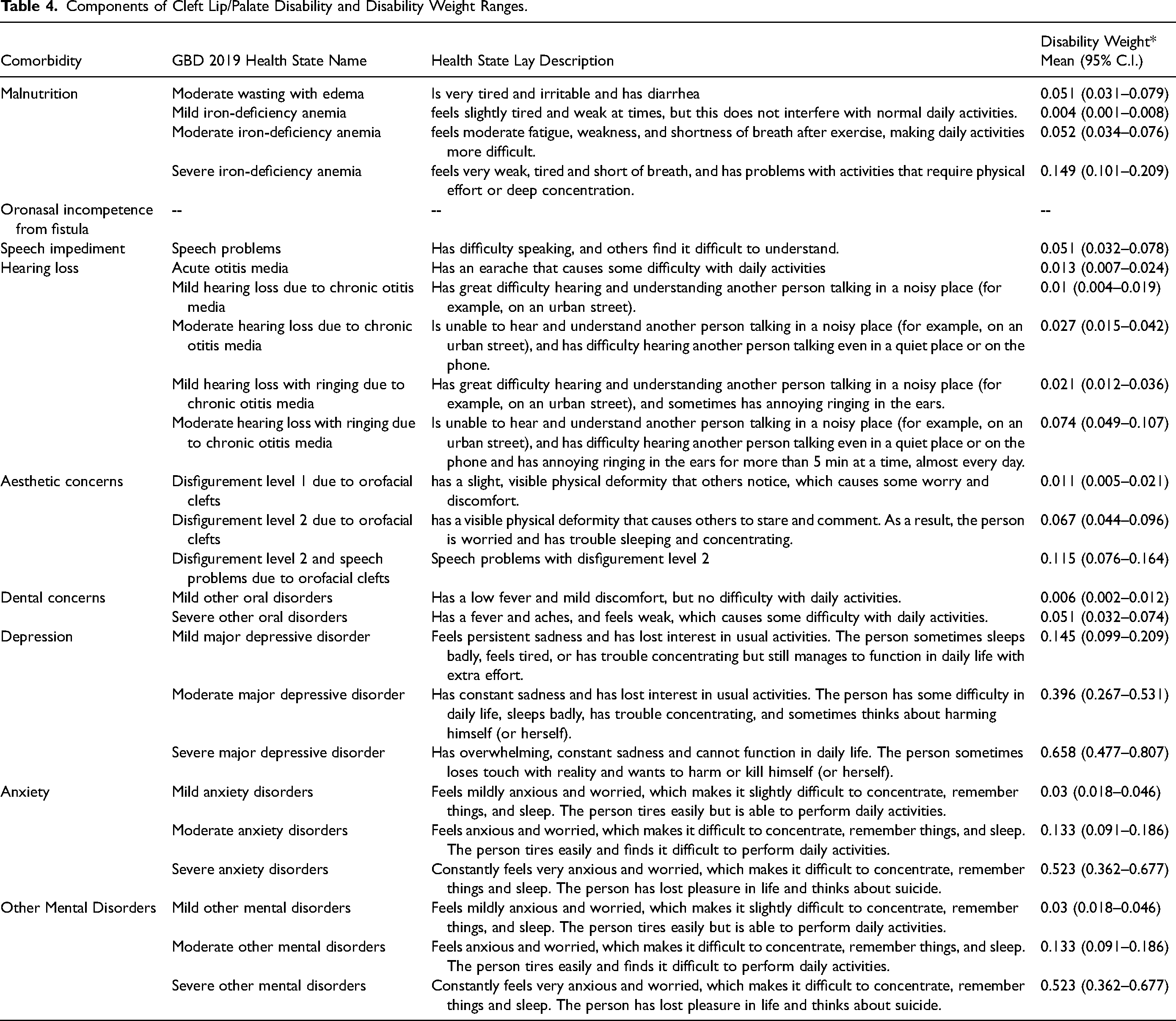
We propose two potential approaches to address the shortcomings of the current DW valuation, both of which are modifications of the current GBD approach and include 1) modifying the health state description for OFCs to include the breadth of associated comorbidities, and 2) approaching cleft-related disability by accounting for each component of coexisting disabilities in summative fashion. Table 4 proposes categories of cleft-related disability, and the range of potential disability weights for each component based on GBD methodology. Despite the shortcomings of the GBD DWs, which are shared amongst several of the studies presented herein, the GBD methodology still provides the most comprehensive, standardized approach for estimating incidence, prevalence, morbidity, and mortality of disease. 24 When these individual components are tabulated, reflecting the breadth of impact of cleft lip/palate, the total may approximate or even exceed some of the studies with a larger mean estimated DW for CL/P (eg, Poenaru 2017). 26 Mental health-related components appear to play a disproportionally large relative impact. Future work could help apply this methodology to by accounting for the prevalence of different comorbid components in the cleft population, thereby improving the accuracy of disability weights for patients with cleft lip/palate and for this population as a whole.
Components of Cleft Lip/Palate Disability and Disability Weight Ranges.
Limitations
This study is limited by the paucity of papers on this topic, preventing compilation of data or robust comparison across studies. Similarly, the aim of included papers was variable, with some focused on the conceptualization and valuation of DWs while others were focused on cleft BoD in a specific country or prevalence of disease amenable to surgical treatment. Furthermore, we added two papers that our search strategy did not pick-up. Although we do not anticipate any additional missed articles, any review is susceptible to unintentionally excluding articles that may have otherwise met inclusion criteria. To mitigate the potential impact of this limitation, this search strategy was developed through an iterative process with input from a biomedical librarian.
Conclusions
Current measures of cleft disability are sparse, limited in detail or supporting evidence, and appear to inadequately reflect the comprehensive impact of an orofacial cleft on function and socialization. Disability incurred during delays in care, inadequate repair, or due to secondary morbidity is not captured through this model. Working within the current GBD/DALY system to generate a more accurate representation of the impact of OFCs offers the most straightforward path to improving cleft disability valuation on an international scale. Approaches to this could take the form of a more comprehensive health state description or a summative combination of relevant comorbidities. Alternative methods to evaluate cleft disability exist but would likely pose a significant barrier to adaptation. Although the cleft burden of disease is down trending, the countries with the greatest proportional burden are those with the fewest resources to address it. It is our hope that more accurate estimation of cleft disability will garner more resources and capital to strengthen healthcare infrastructure and provide comprehensive care to all patients with clefts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB
This study was IRB exempt according to the Children's Hospital of Philadelphia Institutional Review Board.
Appendix 1 Health State Descriptions from Poenaru et al. 2017 . Cleft lip/palate 1
Cleft lip is a separation of the upper lip, either on one side or on both sides. It is sometimes only a small separation or may go all the way into the nose. Cleft palate is a separation in the tissues that make the roof of the mouth on the inside, above the tongue. It can also be either a small or a complete separation. Each of them can happen alone or together with the other one—some children have only cleft lip, others only cleft palate, and others have both.
Children with only a cleft lip problem will look disfigured and may have problems in life with their teeth. Children who also have a cleft palate may have feeding problems as babies, then will have serious problems with speech, hearing and teeth later on.
All children with cleft lip and palate need surgery. Some will be fine after one surgery, but most will need more surgeries to fix not only the lip or palate, but also the teeth, nose, and ears.
Cleft lip / palate is divided into the following states:
Cleft lip without cleft palate Cleft palate with or without cleft lip - No problems with moving about - No problems with washing and dressing self - Mild problems with performing usual activities (eating) - No pain and discomfort - Mild or severe anxiety or depression - Severe social stigma - No thinking problems - No bowel/urine problems
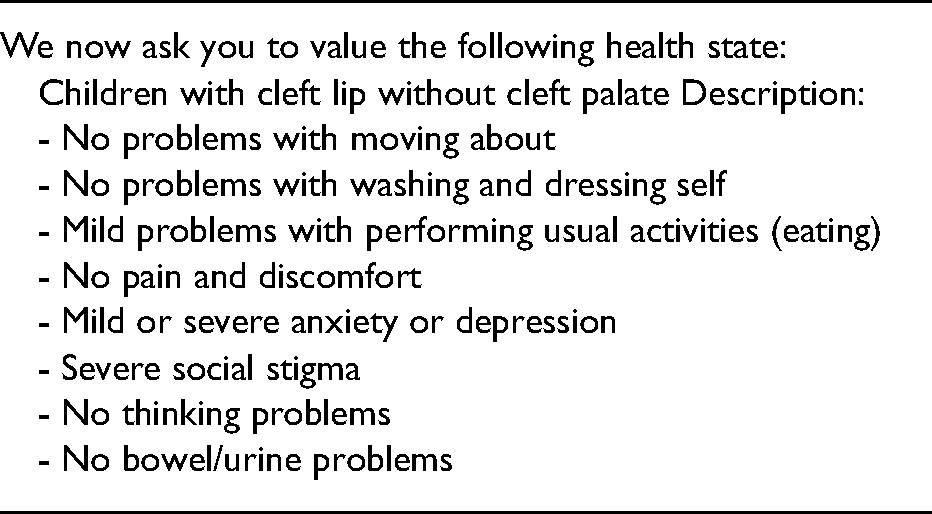
We now ask you to value the following health state:
Children with cleft lip without cleft palate Description: