
Abstract
Objective
To determine whether performing tonsillectomy at the time of Furlow palatoplasty for the treatment of cleft palate related velopharyngeal insufficiency (VPI) incurs increased surgical complications or compromises speech outcomes.
Design
A retrospective review of patients who had Furlow palatoplasty and the outcomes of surgery in the treatment of cleft palate related VPI.
Setting
A single academic center between January 2015 and January 2022.
Participants
Patients with submucous cleft (SMC) palate or patients with prior straight line primary palatoplasty presenting with VPI.
Interventions
Simultaneous conversion Furlow palatoplasty and tonsillectomy.
Main Outcome Measure(s)
Primary outcome measures include preoperative and postoperative Modified Pittsburgh Weighted Speech Scale (mPWSS), and postoperative surgical complications.
Results
Eight patients (25%) underwent Furlow palatoplasty and concomitant tonsillectomy, while 24 patients (75%) underwent Furlow palatoplasty alone. A significantly lower median postoperative mPWSS score, corresponding to better velopharyngeal function, was reported for patients in the Furlow-tonsillectomy group (0, IQR 0-0) compared to the Furlow only group (1, IQR 0–9, p = 0.046). No surgical complications were encountered in either group. Five patients (20.8%) in the Furlow only group required subsequent surgery for persistent VPI. No patients in the Furlow-tonsillectomy group required additional surgical treatment for VPI (0%, p = 0.16).
Conclusions
Tonsillectomy at time of Furlow palatoplasty is utilized in patients with both VPI and baseline tonsillar hypertrophy to lessen the risk of postoperative obstructive breathing. Tonsillectomy performed concurrently with Furlow palatoplasty is safe, without increased risk of surgical complications, and does not compromise post-Furlow palatoplasty speech outcomes
Introduction
Cleft lip and cleft palate, which can occur both sporadically and syndromically, are among the most common congenital craniofacial anomalies worldwide and require multiple operative interventions throughout a child's development beginning in the first year of life and continuing on through adolescence. 1 Surgical management of these deformities can prevent premature death, and improve the patient's ability to feed, speak, hear, and proceed comfortably in social interactions.2,3 The timing of cleft palate repair is typically performed between 10 and 18 months of age. This decision is a careful balance between intervening late enough to allow for maximal uninhibited maxillary growth, and intervening early enough to correct the aberrant anatomic and physiologic function of the palate to permit normal speech development in the young patient.1,4,5 Maxillary growth and palatal length are important contributory factors for velopharyngeal competence yet surgical intervention for cleft palate often results in growth restriction. 6
Reduced sagittal length of the hard and soft palate can lead to cleft palate-related velopharyngeal insufficiency (VPI). Patients with VPI may develop maladaptive articulations to compensate for speech difficulties caused by an incompetent VP port, which highlights the importance of the involvement of speech therapy in diagnosis and treatment of VPI. 7 The Pittsburgh Weighted Speech Scale (PWSS) is the most widely utilized clinical tool assessing nasality, nasal emission, facial grimace, phonatory characteristics, and compensatory misarticulations. 8 With the goal of cleft surgery being the establishment of normal palatal anatomy and reconstruction of a mechanism capable of producing normal speech, speech outcomes data is a critical measure for success.9,10 Although there is no standardized perceptual acoustic evaluation used universally by speech-language pathologists, the Pittsburg Weighted Speech Scale (PWSS) is a well-established and widely utilized clinical tool for evaluation velopharyngeal function.8,10 Besides the obvious challenge of listener reliability for resonance, nasal emission, and oral pressure differences, consonant compensatory errors are often unique to cleft palate speech and confound interpretation.11–13 This problem was evident in an early speech evaluation standardization effort by McWilliams and Phillips (1979). 14 The PWSS provided a framework for clinicians to qualify resonance, nasal emission, and oral pressure. This scale includes categories of velopharyngeal function: competent, borderline competent, borderline incompetent, and incompetent.
Unfortunately, these categories can be falsely influenced by abnormal compensatory speech errors and vocal hoarseness points. Many speech pathologists continue to use the PWSS today, though most will modify its use to eliminate misinterpretation of results. Theoretically, a score over 7 (the cutoff point for VPI) could be present in a child who has normal resonance and pressure but most or all points represent lingering compensatory errors. Thus, in our clinic we utilize a modified PWSS (mPWSS) in the evaluation of all our patients. This tool assesses only those parameters that reflect VP function and not learned or compensatory speech errors, since these errors are generally resolved with proper speech therapy and would not require surgery. We reported the mPWSS as cumulative points related solely to resonance, pressure and nasal emission.
While treatment is multimodal, surgeries to lengthen the palate are often required to improve velopharyngeal closure competence. Furlow palatoplasty is commonly employed for this purpose and has been shown to have good results at decreasing small gap sizes in the VP port in patients post-cleft repair suffering from VPI. 15 Other common surgeries utilized in the treatment of VPI include posterior pharyngeal flap, sphincter palatoplasty, and posterior pharyngeal augmentation with fat grafting. 16
The presence or absence of tonsillar pillars, as well as their size, can also affect the competence of the VP port. 6 Adenotonsillar hypertrophy has also been reported to impair velopharyngeal function following palate repair, and tonsillectomy may subsequently improve the velopharyngeal closure and speech resonance in such patients. 17 There has been some debate as to the appropriate management of cleft patients with concurrent VPI and adenotonsillar hypertrophy 18 with some suggesting that a subset of patients with hypernasal speech could be appropriately treated with tonsillectomy alone, 19 thus avoiding a more involved surgical operation, or postponing it for safer management. 20 Others have advocated that a combined surgery where tonsillectomy is performed concomitantly with cleft palate repair, posterior pharyngeal flap or pharyngoplasty yields comparable speech and airway results while reducing anesthesia time and subsequent surgical interventions.21–23
Due to the conflicting data in the literature, we aimed to present a comparative study evaluating speech outcome data and postoperative complications in a series of patients undergoing concurrent Furlow palatoplasty and tonsillectomy for the treatment of VPI. We hypothesized that patients undergoing tonsillectomy at the time of Furlow palatoplasty would have no difference in speech, surgical and airway outcomes compared to patients undergoing Furlow palatoplasty alone for the treatment of cleft palate-related VPI.
Materials and Methods
After institutional review board approval, a retrospective review of patient records at a large academic medical center from January 2015 to January 2022 was conducted. Patients with submucous cleft (SMC) palate who underwent primary Furlow palatoplasty for treatment of VPI and patients with prior intravelar veloplasty (straight-line) primary palatoplasty who underwent conversion Furlow palatoplasty for treatment of VPI were included. Patients were divided into two cohorts: (i) patients who underwent Furlow palatoplasty alone for treatment of VPI and (ii) patients who underwent simultaneous tonsillectomy for treatment of symptomatic airway obstruction and Furlow palatoplasty for treatment of VPI. Patients who had tonsillectomy, adenoidectomy, or other VPI surgery, including posterior pharyngeal flap or sphincter palatoplasty, prior to Furlow palatoplasty were excluded from the study. Postoperative speech evaluation was performed no earlier than 6 months after the operation. Our protocol for formal speech evaluation after speech surgery is to perform evaluation at 6 months postoperatively. The intention is to avoid making early decisions about successes or failures that may not hold up with time. This does not mean that speech surgery patients are not being evaluated and followed/treated by our speech language pathologist earlier in the postoperative course, but rather that definitive evaluation of success/failure is performed at a longer incremental time frame. Patients with syndromic cleft palates were not excluded.
Data points included patient demographics, Veau classification, postoperative surgical or airway complications, and preoperative and postoperative modified Pittsburgh Weighted Speech Scale (mPWSS) scores. Surgical complications evaluated included infection, postoperative bleeding, incisional dehiscence, delayed wound healing, fistula, ICU admission, or return to operating room (RTOR) for all reasons. Airway complications included respiratory distress or worsening of obstructive breathing requiring intervention. Patients were not routinely admitted to the ICU.
As PWSS has been widely utilized for evaluating speech in patients being treated for VPI we utilized the modified PWSS, which quantitatively assesses only those parameters that reflect VP function and not learned or compensatory speech errors, since these errors are generally resolved with proper speech therapy and not surgery.24,25 (Figure 1) Evaluations were conducted by our experienced cleft team speech therapist during routine clinic visits.

Modified pittsburg weighted speech scale.
Surgical Procedure
In patients who underwent simultaneous tonsillectomy and palatoplasty, tonsillectomy was performed with electrocautery, dissecting superior to inferior along the tonsillar capsule. Following tonsillectomy a Furlow double opposing Z-plasty was performed, which included dissection and reorientation of the levator musculature.
Statistical Analysis
The Fisher's exact or Chi-square test were implemented to analyze categorical data. The Shapiro–Wilk test for normality was applied to evaluate the distribution of data. Non-normal data were presented as median and interquartile range [IQR]. Normally distributed data were presented as mean ± standard deviation. The t-test or Mann-Whitney test were conducted to study continuous data according to its distribution. All analyses were performed using R statistical software, version 4.0.0 (R Core Team, 2020). 26 A p < .05 was considered statistically significant.
Results
Thirty-two patients met inclusion criteria. Eight patients (25%) underwent simultaneous Furlow palatoplasty and tonsillectomy, while 24 patients (75%) underwent Furlow palatoplasty alone. The median age at time of surgery for the Furlow-tonsillectomy group was 6 years [IQR, 4.5–8.5] compared to 4 years [IQR, 2.75–5, p = 0.039] for the Furlow-only group. Twelve patients (37.5%) had a Veau III or IV cleft palate, 11 patients (34.4%) had a SMC palate, and 9 patients (28.1%) had a Veau I or II cleft palate. There was no significant difference in cleft palate type between groups (p = 0.431). There was a higher proportion of patients with syndromic cleft palates in the Furlow-Tonsillectomy group (n = 2, 25%) compared to the Furlow-only group (n = 0, 0%, p = 0.01) (Table 1). The minimum follow-up time was 7 months, and the longest follow-up time was 42 months. The average length of follow up was 21.50 months with a standard deviation of 15.88 months.
Demographic Data.
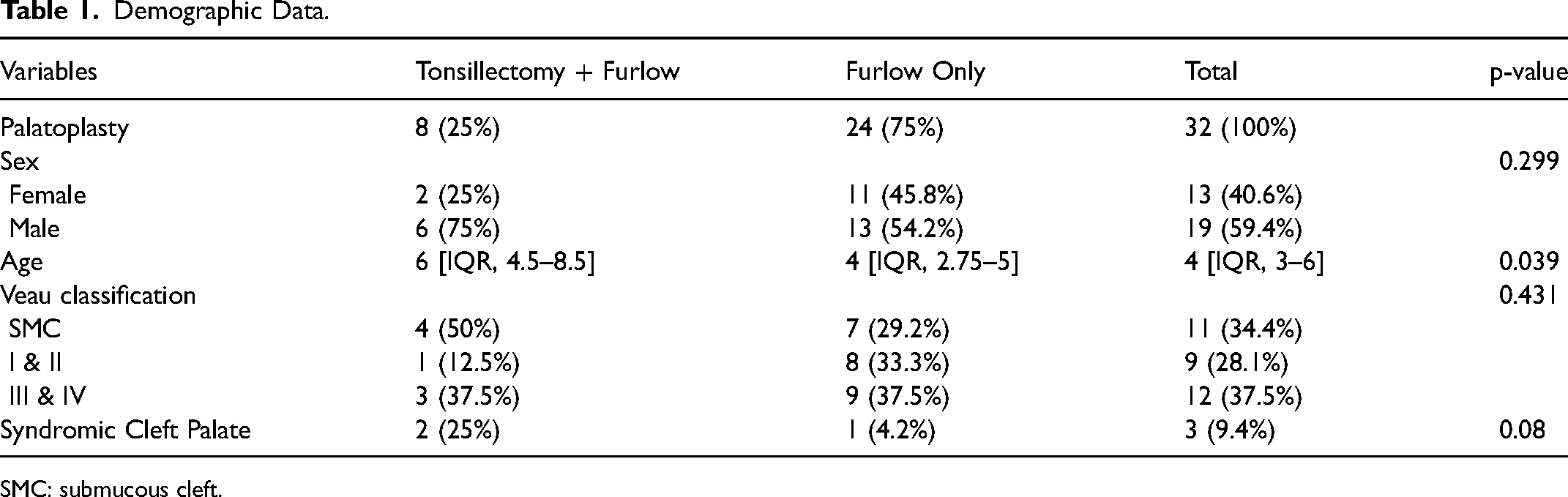
SMC: submucous cleft.
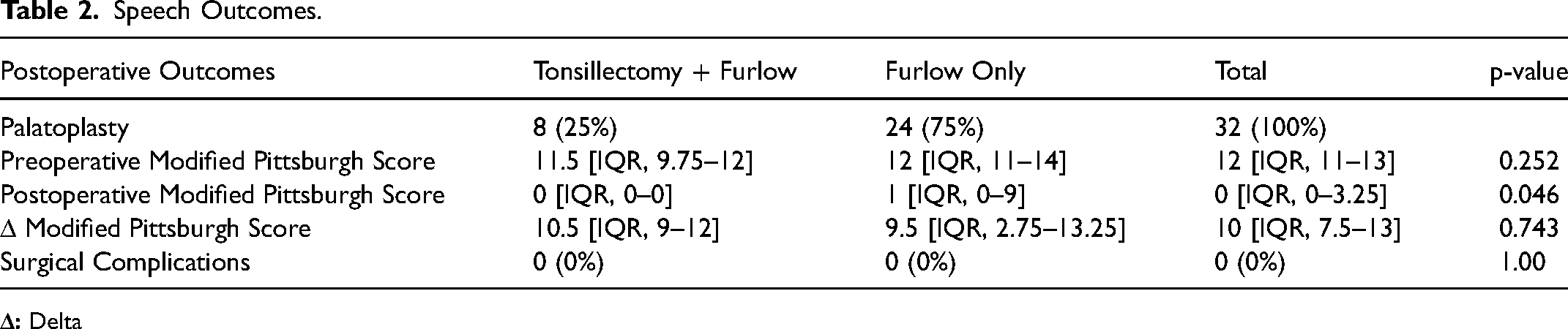
There was no significant difference in preoperative mPWSS scores for patients in the Furlow-tonsillectomy (11.5, IQR 9.75–12) versus Furlow-only (12, IQR 11–14, p = 0.252) groups. A significantly lower median postoperative mPWSS score, corresponding to better velopharyngeal function, was reported for patients in the Furlow-tonsillectomy group (0, IQR 0-0) compared to the Furlow-only group (1, IQR 0–9, p = 0.046). Nonetheless, the median delta between pre- and postoperative mPWSS scores was not significantly different between groups (p = 0.743) (Table 2). No surgical complications were encountered in either group. Five patients (20.8%) in the Furlow-only group required an additional surgical procedure, pharyngeal flap or sphincter pharyngoplasty, for persistent VPI post-Furlow palatoplasty (Table 3). No patients in the Furlow-tonsillectomy group required additional surgical treatment for VPI (0%, p = 0.16).
Speech Outcomes.
Surgical Outcomes.

On a sub-group analysis of only patients with SMC undergoing primary repair for VPI, a significant difference in the delta between pre- or post-operative mPWSS was not identified. Similarly, an analysis of non-SMC patients only, no significant difference was found (Table 4).
Subgroup Analysis.

Discussion
Regarding velopharyngeal function, a history of cleft palate with or without repair is the most common cause of VPI,27,28 and the most common cause of VPI in patients who have undergone straight line repair of the palate is inadequate length of the velum, poor levator function, or palatal scar contracture.15,29 In recent years Conversion Furlow Palatoplasty has been reported as an effective surgical approach for correcting VPI in patients with cleft palate-related VPI, especially in those with a previous straight-line repair since it effectively lengthens the palate, reestablishes proper orientation of the levator sling, and narrows the velopharyngeal aperture.9,29–34 Patients with kinetic palates and evidence of anteriorly oriented levator veli palatini muscle fibers are typically considered to be good candidates for secondary Furlow palatoplasty. 6 Patients with large postoperative palatopharyngeal gaps of 1 cm in depth or greater, or with a residual gap of greater than 20% from the original deficit, may benefit from other surgical options for repair, including posterior pharyngeal flap or sphincter palatoplasty.6,35,36 In our practice, patients who are considered for Furlow Palatoplasty are those found to have good lateral wall motion, but poor anterior-posterior closure of the VP port as seen on video endoscopy. In our cohort who underwent Conversion Furlow Palatoplasty we achieved significant improvement in mPWSS scores in all patients.
With regard to velar length following Furlow Palatoplasty, Guneren, et al. demonstrated significant and lasting velar lengthening from this operation. 37 Randall, et al. reported that if the uvula reaches the posterior pharyngeal wall under tension, the patient is likely to achieve VP competence with Furlow Palatoplasty, but if it does not reach the adenoid pad, the patient may be better served with a pharyngeal flap. 38 D’Antonio, et al. showed that the length and thickness of a reconstructed palate correlate to the achievement of VP competence. 36 Although we do not have pre- or postoperative measurements of palatal length provided for the patients in our series, the universal improvements in speech scores indicate appropriate and adequate lengthening of the palate to achieve VP competence. While sagittal length is the goal of Furlow palatoplasty, the ultimate outcome desired is improvement in speech, which is measured with the mPWSS. Improvement in speech performance is the ultimate measure of a successful palatal-lengthening operation.
Maxillary growth and palatal length are important contributory factors for velopharyngeal competence yet surgical intervention for cleft palate often results in growth restriction and a history of cleft palate with or without repair is the most common cause of VPI. This means that non-SMC patients who received prior primary repair via intravelar veloplasty are more likely to have a reduced sagittal length of the soft and hard palate than SMC patients who did not receive primary cleft palate repair, and they are more likely to have palatopharyngeal insufficiency (VPI) associated with cleft palate. In our cohorts, patients with SMC (who had not previously undergone primary straight-line cleft palate repair) accounted for 50% of the Tonsillectomy + Furlow group and 29.2% of the Furlow Only group. Although not statistically significant, this represented a possible confounder in our data. Subsequent sub-group analysis (Table 4) did not demonstrate a statistically significant difference in delta-mPWSS between groups. Although the small sample size limits conclusions to be drawn from this analysis, this suggests that patients benefit similarly from Furlow palatoplasty performed for primary SMC or revision surgeries for palates previously repaired.
In a recent query of NSQIP data of nearly five thousand patients who underwent primary palatal repair, Mets et al. identified a low complication rate of only 6.4%. Most of these patients who experienced postoperative complications, had wound dehiscence with a reoperation rate of less than 1%. 39 Furlow palatoplasty is increasingly used for primary palatal repair and there is data that suggests that when performed for the treatment of cleft palate-related VPI, it carries a lower risk of obstructive airway symptoms when compared to pharyngeal flaps and sphincter palatoplasty.6,40
Tonsillar hypertrophy or scarred tonsillar pillars is a possible cause for VPI as they can prevent adequate closure of the velum against the posterior pharyngeal wall.6,17,19,41,42 Adenotonsillectomy has been shown to affect VP competence, 18 and some have advocated for a staged approach for tonsillectomy followed by palatoplasty.19,20 Past studies have evaluated the surgical safety of simultaneous palatoplasty and tonsillectomy but these studies lack significant power and fail to evaluate the effect that combining these procedures has on speech and airway outcomes.21–23 Hu, et al. presented a series of 11 patients who underwent velopharyngeal surgery with simultaneous tonsillectomy, and outcomes were compared between several other groups, including a group who had tonsillectomy prior to a velopharyngeal surgery, a group which had tonsillectomy after velopharyngeal surgery, and a group who had tonsillectomy performed alone for a total of 30 patients. They found that tonsillectomy had only a mild effect on velopharyngeal function and that simultaneous tonsillectomy and velopharyngeal surgery had an efficacy and complication rate comparable to staged operations. The results of our study adds to the findings of this group to provide strong evidence that simultaneous tonsillectomy and palatoplasty is safe and effective for the treatment of VPI. Although tonsillectomy is rarely considered a “major surgery”, combining these surgeries is impactful for patients who must undergo a long series of operations in their youth. We feel that eliminating the burden of one minor surgery is not insignificant for this population.
Limitations
Limitations for this study include its retrospective nature and small sample size. Additionally, while airway outcomes were assessed objectively by evaluating rates of required postoperative airway intervention, formal postoperative sleep studies were not routinely obtained in this population unless postoperative symptoms justified polysomnography. There are many different considerations a surgeon must make when performing surgery for the correction of VPI, including striking a balance between airway safety and adequate lengthening of the palate to maintain VP port competence. Another important factor of consideration, is the importance of minimizing the number of surgeries these patients must undergo. Despite a somewhat smaller sample size, this study demonstrates convincing evidence that tonsillectomy can be performed safely at the time of Furlow palatoplasty without increased risk of complication or negative impact on speech outcomes, and in doing so helps lessen the lifetime surgical burden for patients with oral clefts. Further studies are required to better validate the PWSS, however it's widespread use makes it one of the best tools for assessing speech in patients evaluated for VPI. Future studies with a larger patient population would likely further support this conclusion.
Conclusion
Tonsillectomy at time of Furlow palatoplasty is utilized in patients with both VPI and baseline tonsillar hypertrophy to lessen the risk of postoperative obstructive breathing. Despite demucosalizing the pharynx and altering the size of the VP port, tonsillectomy performed concurrently with Furlow palatoplasty is safe, without increased risk of surgical complications, and does not compromise post-Furlow palatoplasty speech outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.