
Abstract
Objective
Craniofacial microsomia (CFM) is a broad clinical term used to describe a congenital condition most commonly involving the underdevelopment of the external ear, mandible, soft tissues, and facial nerve. Despite medical advances, understanding of the psychological health and healthcare experiences of individuals with CFM and their caregivers remains limited. This article describes a research program designed to address these knowledge gaps, and identify opportunities for psychosocial intervention and improved healthcare provision.
Design
The Craniofacial microsomia: Accelerating Research and Education (CARE) research program aims to:
Results
Teams in the USA and UK have been established, alongside an international, interdisciplinary Advisory Committee. Data analysis for Aim 1 is ongoing and informing the delivery of Aims 2-3. Aim 4 is also in development. A dedicated website serves as a recruitment tool, educational resource, and mechanism for engaging with the CFM community.
Conclusions
The CARE program provides a comprehensive approach to understanding the experiences of individuals with CFM and their caregivers. Challenges encountered and lessons learned are shared for the benefit of the community.
Introduction
Craniofacial microsomia (CFM) is a term used to describe a congenital condition with a broad phenotypic presentation most commonly involving the underdevelopment of facial structures, such as the mandible, maxilla, ear, orbit, facial soft tissue and muscles, and the facial nerve.1,2 CFM is the third most common congenital craniofacial condition after cleft lip and/or palate (CL/P) and craniosynostosis, affecting approximately 1 in 5000 to 26,300 live births depending on the study inclusion criteria.3–6 CFM can affect facial appearance and impair function, such as hearing, feeding, breathing, facial movement, speech, and vision. In addition to craniofacial differences, many individuals with CFM have extracranial anomalies, which may involve the spine, cardiac, renal, pulmonary, gastrointestinal and central nervous systems.7,8 Long-term treatment plans, developed in collaboration with a specialized, interdisciplinary craniofacial team, are often required. 2
The Importance of Psychosocial Health for Individuals Born with CFM
Recent advances in techniques for interventions such as hearing amplification, distraction osteogenesis, and ear reconstruction have the potential to improve aspects of health important to individuals with CFM.9–11 However, knowledge about holistic outcomes, including the psychosocial impacts of CFM and burden of care, remains relatively limited. 12 Available literature suggests that having an atypical appearance can make children vulnerable to staring, comments, and questions, 13 with indications that rates of teasing and bullying among those with CFM may be higher than in the general population.14,15 Hearing loss, hearing amplification,16,17 as well as speech disorders may also impair communication and affect the quality of social interactions.18,19 In studies with microtia and CFM populations, teasing has been reported starting around the age of five for 41% to 100% of individuals and coincides with negative public perception ratings of social characteristics and cognitive functioning.20,21 These negative social experiences can lead to low self-confidence, depressive symptoms, social anxiety, internalising/externalising behaviors, appearance dissatisfaction, and reduced life engagement.22,23 This was reflected in a large multisite study of children with CFM in which teachers reported higher internalizing concerns and lower social competence and adolescents self-reported more social concerns compared to their peers.24,25 Some female adolescents and young adults with CFM reported covering their ears with their hair and a group of UK adults noted continued anxiety about their ears being seen.18,26 Young adults may shy away from romantic relationships due to a fear of rejection, and the possibility of having a child with a craniofacial condition may evoke distress around starting a family.27,28 Mental health services were reported for 14% of children with CFM in a large multisite study 23 and adults with craniofacial conditions may also experience a higher rate of mental health difficulties.27,29
Studies have demonstrated that overall cognitive functioning in young children with CFM is in the average range; however, an area of delay was identified in 39% at 36–42 months with relatively lower language, reading, and writing scores in school-age and adolescent samples.17,19,30,31 Studies of US children with microtia and/or CFM reported special education support for 20% to 48% of students.32–35 Additional intervention services such as speech therapy are also common and received by 60% to 79% of children with CFM.19,31,33 If the individual's cognitive development is affected by their condition, they may perform more poorly at school, potentially limiting educational and vocational opportunities. 36 For example, children with CFM have been found to have lower school and community activities participation and to spend less time with peers.23,33 As the individual grows older, they may become more involved in complex decisions about care, which can be difficult to manage. 37 While many individuals endorse a benefit of interventions such as use of hearing amplification and ear reconstruction,38–41 overall quality of life may also be impacted by the burden of ongoing such treatment, 42 in addition to various challenges in the home, school, and community settings. 43 Psychological adjustment to craniofacial conditions and adequate support throughout the healthcare journey is therefore vital for long-term psychological health, as well as physical health, vocational stability, and overall life engagement.
The Importance of Psychosocial Health for Caregivers
Caregivers of individuals born with craniofacial conditions also often experience impacts on psychosocial health. Following a diagnosis of CFM in their infant, caregivers report a range of emotions, which can include anxiety, shock, grief, guilt, confusion, and concern for the future.12,32,44–46 Families must learn about the implications of their child's condition, process a wealth of new medical information, and manage the potentially negative reactions of family members and members of the public.32,43 Preparing for surgery may be particularly distressing for caregivers, who may report conflicting emotions and symptoms of traumatic stress.47,48 As the child grows older, caregivers may also struggle to talk with their child about their condition and appearance. 49 Parental adjustment to these demands is crucial for their own long-term psychological health, as well as the emotional, social and cognitive development of the child, and family functioning as a whole. 50
Current State of Healthcare in CFM for Individuals with Craniofacial Microsomia
Although treatment guidelines have been proposed for healthcare screening and interventions for children with microtia and CFM,51–53 we lack widespread consensus among healthcare providers regarding clinical standards. As a result, healthcare for children with CFM remains highly variable, both between and within craniofacial teams. This is further complicated by the variety and complexity of clinical needs, the availability of treatments, and patient/caregiver preferences. Care coordination and the integration of psychosocial support is crucial, but without a standardized, centralized service, is often challenging to achieve. 43
In turn, access to reliable medical information for patients and families is sparse, and caregivers have voiced a desire for more information about medical specialties involved in care, surgery options, genetics, hearing, development, psychological adjustment, treatment steps, and financial support options.32,46,54 This can make the task of navigating healthcare services particularly daunting for patients and caregivers,42,43 especially when relying on this information to make surgical decisions. 26 Decisions made early on in the child's life can also affect future treatment options, make certain treatments impossible later in life, or provide a suboptimal situation for performing further treatments. 55 For example, the choice to perform certain types of ear reconstructive procedures early in life may interfere with later surgical options to improve the symmetry of the face, while poor planning in bone-anchored hearing aid placement may make a future optimal ear reconstruction impossible. While craniofacial teams and advocacy groups provide information for a variety of craniofacial conditions, publicly accessible information about CFM specifically tends to be generalized or focused on specific topic areas (eg, options for ear reconstruction). Families often turn to social media for medical information, which was illustrated in one study finding that half of posts in online CFM and microtia groups were seeking guidance on medical care. 54 The lack of a central source of vetted, evidence-based information for families and individuals thus provides another barrier to patient-centred care in CFM.
Current State of Psychological Research in CFM
To date, most of craniofacial research has been conducted in the field of CL/P, the most common congenital craniofacial condition. Significant progress has been made in understanding the psychological impact of CL/P on those affected and their families, understanding individuals’ and families’ support needs, and moving toward evidence-based psychological screening and intervention. 56 Qualitative research has provided unique insight into what it is like to live with CL/P, patients’ and caregivers’ experiences of healthcare, and the adequacy of current service provision in addressing psychological concerns. 57 Methodological advances, including consensus on the use of patient- and parent-reported outcome measures and the establishment of interdisciplinary and international networks has allowed for large-scale, international data collection. 57 As a result of this research, CL/P care in some countries has become more patient-centred, with defined treatment protocols that integrate psychological support into routine practice. In contrast, far less psychosocial research has been conducted with the CFM population, with a recent review identifying only 64 studies since 2000. 12 The review noted that studies tended to be cross-sectional, from European and North American populations, and with sample sizes generally smaller than 100 participants. While the research showed that many participants benefitted from medical and surgical interventions and had generally average range neurocognitive and psychosocial functioning, results also demonstrated that the population was at an increased risk for language and social concerns and significant stress associated with diagnosis and complex care. The review highlighted the need for effective screening and interventions for psychosocial concerns as well as more global representation in qualitative and quantitative research with both diagnosis-specific and general population measures in the context of well-described sociodemographic and medical histories.
Aims of this Article
Given the long-term and multifaceted nature of treatment for CFM and the anticipated impact on the quality of life of those affected and their families, more knowledge of holistic outcomes and a thorough understanding of the healthcare experience is needed. In recognition of this need, the National Institute for Dental and Craniofacial Research (NIDCR) at the National Institutes for Health (NIH) have funded a 5-year program of research into the psychological and healthcare needs of the CFM population, entitled “Craniofacial microsomia: Accelerating Research and Education (CARE)”. The aim of the present article is to describe the steps involved in the CARE program, designed to investigate the psychological and healthcare impacts of CFM, assess the adequacy of existing healthcare guidelines to meet these needs, address methodological limitations of prior studies, and work toward the identification of appropriate psychosocial screening tools and interventions for the CFM population. Additionally, this article aims to share the approach taken and the lessons learned for the benefit of the scientific community, as well as encouraging international engagement and collaboration.
Methods
Developing the Aims of the Grant
In response to the gaps in the literature and current challenges within healthcare settings, we sought funding for a new program of work (Figure 1) to investigate the psychosocial impact and healthcare burden of CFM. A core team of researchers with expertise in various aspects of CFM-related clinical care and research was established, and initial literature reviews and exploratory studies12,42,43 were performed.
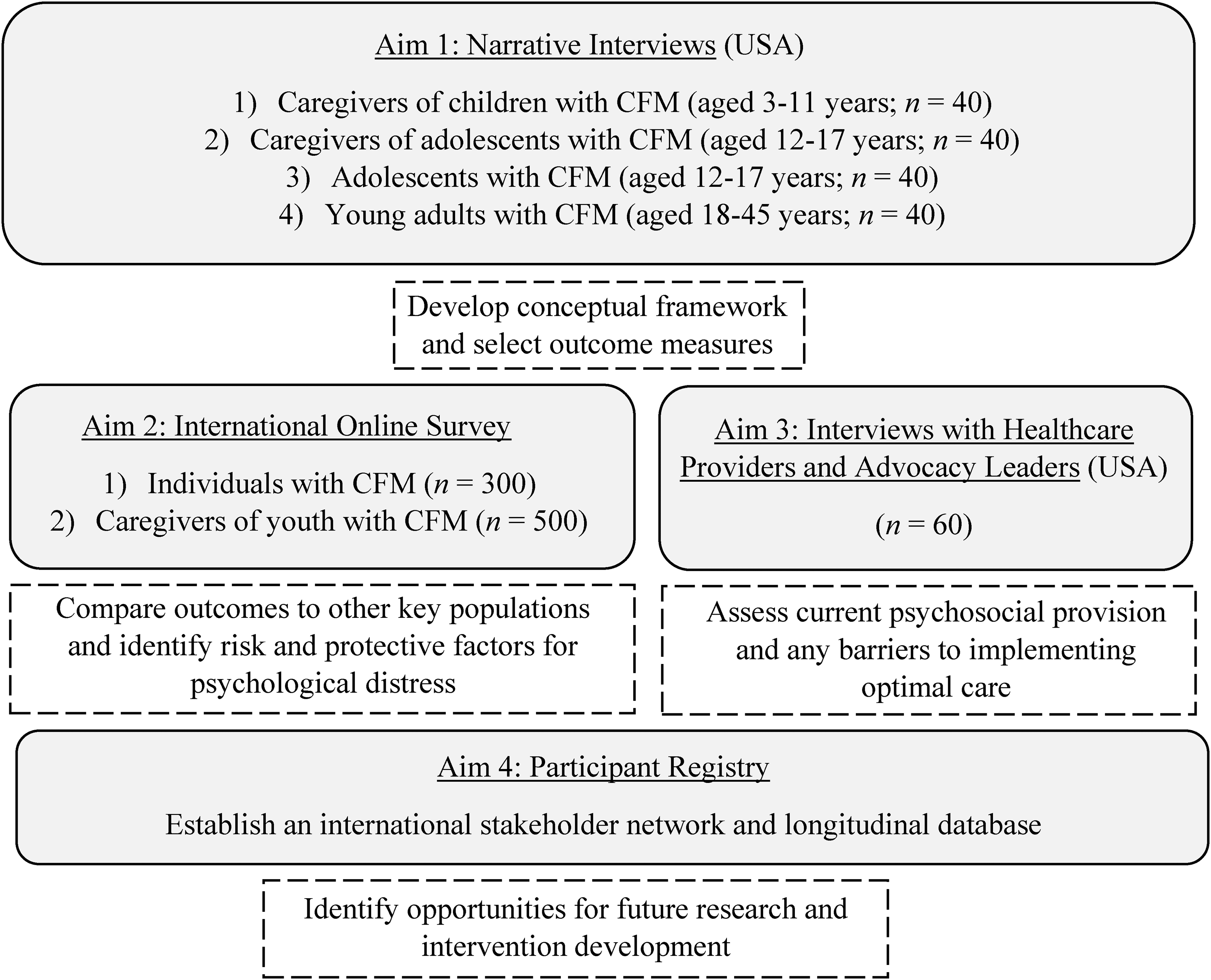
Primary aims of the CARE research program.
Aim 1: Validate a Conceptual Framework for CFM
Particular insight from the related field of CL/P and other areas of healthcare highlighted the importance of a conceptual framework to drive methodological decisions and provide a foundation for further work.57,58 Such a framework could encompass all areas of potential psychosocial distress and demonstrate how these areas might integrate with the CFM treatment pathway and other significant life stages and events. Due to the relative lack of inclusion of the patient perspective in CFM research and the success of qualitative approaches in advancing research in other craniofacial conditions,59,60 we took a qualitatively driven approach to the first aim of the research program. A large-scale qualitative study was perceived to be necessary in order to capture the wide variability in individual healthcare needs and anticipated spectrum of medical experiences.
An ambitious target of up to 160 individual qualitative interviews was set. Interviews were conducted using a narrative methodology through telephone and/or videoconference platforms. Four distinct groups affected by CFM living in the USA were enrolled: caregivers of children with CFM aged 3–11 years (n = 29), caregivers of adolescents with CFM aged 12–17 years (n = 21), adolescents with CFM aged 12–17 years (n = 20), and young adults with CFM aged 18–45 years (n = 20). Up to 20 additional interviews are also being completed with Spanish-speaking participants to represent US demographics of CFM. Participants were invited to divide their stories into ‘chapters’ which they define themselves, describe each chapter in detail, and identify the most poignant ‘high’ and ‘low’ points throughout their journey to date. Alternatively, interviewers conducted semi-structured interviews for those participants (eg, young children, participants with complex needs) who prefered a more structured approach. The interviews have allowed the research team to validate a conceptual framework based on the common challenges experienced by caregivers and individuals with CFM, as well as targeted areas for future intervention. Participation in this study also included reporting on sociodemographic variables and engaging in a medical history interview. Finally, participants provided photographs, which are stored separately to all other data and which are used primarily to assist in describing clinical characteristics and ensuring representation from the broad CFM community.
Aim 2: Identify Predictors of Psychological Distress in an International Population Affected by CFM
For Aim 2, a quantitative approach was developed, to examine the generalisability of the qualitative findings on a broader scale. Such an approach will allow for the exploration of risk and protective factors that may influence psychological outcomes in CFM; knowledge which is essential for future development of interventions aimed at improving these outcomes. Data will be collected internationally to allow for the acquisition of a large sample, to expand the overall reach of the research programme, and to strive for more global representation in CFM research. In light of recent studies demonstrating the validity of online approaches, 61 the survey will be conducted online.
An online, multiple methods survey will be distributed to an international population of individuals with CFM (n = up to 300) and caregivers (n = up to 500) in five English-speaking countries initially (USA, UK, Canada, Australia, New Zealand). Up to 300 Spanish-speaking participants will also be sought. Mean scores on standardized measures will be compared to general population norms where available to assess relative adjustment, in addition to exploring condition-specific impacts. Higher level analyses will also be conducted to examine associations between variables of interest and potential risk and protective factors for psychological distress.
Aim 3: Examine the Extent to Which Current Healthcare Provisions Address the Areas of Medical and Psychological Need Identified
The third component of the research programme recognizes the complexity and spectrum of CFM, and the need for a coordinated, interdisciplinary approach to management, 1 which has also been identified as important by caregivers. 43 Further, community-based advocacy groups and their online forums 54 play a key role in the facilitation of holistic support for the CFM community. The perspectives of health providers and advocacy groups can be overlooked in health research; yet, these stakeholders are at the forefront of care provision for the CFM population. 62 The involvement of all stakeholders, particularly those responsible for the delivery of healthcare, is essential in overcoming the research-practice gap and progressing toward implementation and real change.
Individual qualitative interviews will be conducted with USA healthcare providers who specialize in craniofacial care (n = up to 50), in addition to USA craniofacial advocacy group leaders (n = up to 10). Qualitative analyses will examine current psychosocial provision, the feasibility of addressing psychological needs in practice, and any barriers to implementing change.
Aim 4: Establish an International Community Registry in CFM
Finally, discussions focused on the need for a broader and long-term network of individuals with CFM and caregivers, as well as patient and family resources to support decision-making and understanding, particularly as medical information is increasingly sought online. This patient and family network could support ongoing data collection, which could surpass the initial funding period and offer a unique opportunity for longitudinal analysis. 63 The primary aims of the registry are to engage the CFM community in research and to address priority questions generated by caregivers and individuals with CFM, healthcare professionals, and advocates. The registry has been developed with extensive input from advocacy partners, and a range of clinicians and researchers representing multidisciplinary team care. The CARE registry will enroll caregivers of children with CFM, adults with CFM, and adolescents with CFM (with parental consent). Participants will complete a baseline survey, alongside annual follow-up surveys. A variety of information will be collected in the following areas: 1) pregnancy; 2) birth and neonatal history; 3) family history; 4) diagnosis; 5) specialists seen and therapies received; 6) surgeries by feature; 7) care-coordination and shared decision-making; 8) scholastic experiences; 9) teasing; 10) the impact on the family; and 11) demographics. The registry will offer a relatively inexpensive and sustainable solution to longitudinal data collection, by leveraging resources such as REDCap and building on existing models, including the National Organization for Rare Disorders. The registry website will also ‘give back’ to the CFM community by including advocacy-driven resources, including a glossary of providers and healthcare terms, and plain language summaries of research findings.
All of the work carried out as part of the CARE program is conducted according to the World Medical Association Declaration of Helsinki and is subject to Institutional Review Board approval in the USA and UK. Verbal and/or written informed consent is sought from all participants prior to their participation in the study.
Building an Interdisciplinary Research Team
To achieve the four aims, an international research team contributing a wide range of expertise was required. The two primary sites are led by Dr Carrie Heike (Seattle Children's Hospital, USA) and Dr Nicola Stock (Center for Appearance Research, UK). Both PIs provide oversight regarding the development of and compliance with all policies and procedures, and the implementation of the scientific agenda and the leadership plan, utilizing their complementary areas of expertise. The PIs are also responsible for the overall governance of the team and oversee data collection and analysis. In addition, we developed an international Advisory Committee consisting of leading specialist researchers and clinicians in the areas of craniofacial surgery, otolaryngology, psychology, and epidemiology, as well as a parent and community advocates.
Results
Team Science
Launching a large programme of work with a new team composed of individuals with diverse backgrounds and internationally located poses significant challenges. To mitigate this and to maximize the opportunities of working with this unique team, methods aimed at optimizing true team science have been introduced. Initially, this included a series of online ‘retreats’ for all members of the Advisory Committee, hosted by an expert in the Institute of Translational Health Sciences at the University of Washington, USA. Retreat activities focused on identifying each members’ motivations for becoming involved in the CARE program, and their hopes for what the program could achieve, both in the short- and long-term. In addition, all members completed ‘Personal Style Inventories’, to better understand each other's preferred communication styles and information needs. Facilitated group discussions aligned members’ expectations about each person's role(s) within, and capacity to contribute to the CARE program (eg, Co-Investigator versus voluntary consultant).
The group worked together to plan the mission, vision, and values for the CARE program, to ensure a shared ethos. The interdisciplinary Advisory Committee developed the following vision: “A world in which all individuals born with CFM are able to reach their full potential, where the CFM community has access to high quality actionable information, and the overall wellbeing of the individual and their family is central to the care pathway”. This led to the development of the following mission for the research programme: “To serve the CFM community, which includes individuals born with CFM and their families, healthcare teams, researchers, advocacy groups, education systems, policy makers, and members of the public. Our team seeks to learn about the lived experiences of the CFM community to improve wellbeing and to make a lasting difference to the CFM journey both now and in the future”. Five key values were also chosen which underlie the team's collective efforts: Knowledge (valuing specialist expertise, including expertise by experience); Quality (having a shared standard of excellence), Integrity (ensuring aims and actions match), Collaboration (a strong cooperative team effort); and Meaningful Change (a commitment to making a lasting difference to care).
These retreats also gave all Advisory Committee members a chance to develop new and/or build upon existing relationships with one another. Later activities included input into the design of the CARE website and logo, trialing the interview protocol, completing surveys to highlight each member's specific areas of interest, and developing a clear policy for data access and authorship. These retreats, in addition to regular meetings and subgroup discussions, have been invaluable to instilling authentic ‘team science’ principles.
Diagnostic Criteria
Multiple terms are used to describe conditions with phenotypes that overlap with those associated with the CFM spectrum.64,65 Currently, there is a lack of consensus on diagnostic criteria within the CFM healthcare community. 1 In order to use consistent language throughout the CARE program, we use the term ‘CFM’ as a broad term that includes the following diagnoses: microtia, hemifacial microsomia, Goldenhar syndrome, and Oculo-Auriculo-Vertebral Spectrum. We have used the FACIAL inclusion criteria 65 for Aim 1, which includes a diagnosis of microtia or anotia and/or one of the following combinations of features: facial asymmetry and preauricular tag(s); facial asymmetry and facial tag(s); facial asymmetry and epibulbar dermoid; facial asymmetry and a lateral oral cleft (ie, macrostomia); preauricular tag(s) and epibulbar dermoid(s); preauricular tag and a lateral oral cleft; facial tag(s) and epibulbar dermoid; a lateral oral cleft and epibulbar dermoid(s). Individuals who meet the inclusion criteria and have not been diagnosed with a more specific syndrome such as Townes-Brocks, Treacher-Collins, Brachiootorenal, Nager, or Miller syndromes are eligible to participate. Participants are invited to take a screening survey and are also asked to submit photographs to confirm study eligibility.
Recruitment and Retention
The CARE program utilizes a range of recruitment strategies, including contacting participants from past studies, delivering information in clinic, sharing online advertisements, attending advocacy group events, and working with partners to widen the program's reach. Methods have been implemented to make participation as simple as possible. For example, the use of QR codes on all recruitment materials take the participant directly to the relevant information. Guidance is continually sought from participants, advocates, and colleagues to ensure advertisements are engaging, study content is relevant, and study methodology is accessible. Gift cards are provided to participants to thank them for the time they spend on the study. In addition, individuals and caregivers are invited to sign up to receive CARE updates, including newsletters, which inform the recipient of upcoming studies which they/their child may be eligible for, and how their contribution to the program has been utilized to progress knowledge and improve care.
At the time of writing, 90 narrative interviews (Aim 1) have been completed and enrollment has now concluded. Interviews with Spanish-speaking participants are now almost complete. Analysis of Aim 1 data is ongoing, and is informing the delivery of the international survey (Aim 2) and health provider/advocacy leader interviews (Aim 3). The participant registry (Aim 4) is also under development and will be launched in late 2022. Finally, a dedicated CARE website has been established (www.thecarestudy.org), in addition to a site specifically for the registry (www.craniofacialcare.org). These sites will act as a recruitment tool, an educational resource, and a way to share findings with the CFM community throughout (and potentially beyond) the research program.
Discussion
In the first two years of the program, a number of challenges were anticipated, and/or identified. These have included: how to attain broad representation of the CFM population, how to involve non-English-speaking participants, whether and how to acquire the perspectives of young children, and how to effectively work remotely within an international and interdisciplinary team. The grant also presents a variety of exciting opportunities for the broader CFM community, including: the chance to address several known methodological challenges, the potential to develop a sustainable interdisciplinary network, and the ability to create opportunities for academics and clinicians at all career levels.
Challenges Presented by the CARE Program
Attaining Broad Participant Representation
Given the wide range of clinical features captured by the term ‘CFM’ and our study eligibility criteria, it is expected that different individuals will embark on a variety of treatment pathways. The challenge is therefore to ensure inclusion of participants presenting with features that span the clinical spectrum, in order to capture the full range of healthcare experiences. Equally, a range of racial and ethnic backgrounds is desired, to ensure the relevance of the findings and resulting resources across cultures and countries. Researchers have also typically found it more challenging to recruit fathers into psychological studies, and males in general. 66 Other key demographic factors, such as insurance status, socioeconomic status, educational status, and marital status may also play a role in data representativeness, as has been the case with other large-scale studies and recommended in recent review.12,66 To promote inclusivity, the CARE team will track key demographic variables to regularly assess the representativeness of the sample, and will specifically target groups for which numbers are lacking. In support of this, we continue to seek advice from advocacy groups.
Inclusion of Non-English-Speaking Participants
Language is a critical gap in many existing studies, both in CFM research 12 and in healthcare studies more generally. The barriers to involving non-English-speaking participants are significant and require adequate resources to achieve meaningful engagement. Yet, not including non-English-speaking participants in research is likely to result in a narrow understanding of the population under study, and any subsequent interventions may not be as relevant to particular groups. To combat this, our team has sought additional funding to enable Spanish-speaking participants to participate in all four aims of the CARE program. There are also plans to expand the program to include other common languages, such as French and Mandarin, with a particular focus on the CARE registry.
Perspectives of Children Younger than Age 12
Due to ethical considerations and resource restrictions, children under the age of 12 years will not be enrolled in the main aims of the CARE program. Yet, the importance of this age group should not be overlooked. Although not yet able to take legal responsibility for their healthcare, children's involvement in healthcare decision-making is increasing. 67 Healthcare experiences during the formative years can have a considerable impact on procedural anxiety, future treatment adherence, and long-term physical and psychological health. 68 Research with this age group is also lacking, and thus specific efforts to elicit the views of children are needed. To mitigate this in the CARE program, parent-proxy data will be collected and supplementary sub-studies with young children will be pursued where possible.
Remote Working
The international nature of the CARE program, combined with the recent constraints of the COVID-19 pandemic, has resulted in a need to engage in remote work. Planned international travel for team meetings and conferences has not been possible for the first two years of the grant. Even for team members based at the same site, in-person meetings have only recently become feasible. Although the CARE team is familiar with conducting telephone and video interviews, interviewers and participants face additional hurdles associated with navigating international time zones and facilitating accessibility, particularly for those participants and team members who are hard of hearing. The team continues to explore ways of making interviews as accessible as possible, such as in-person interviews with American Sign Language interpreters in clinic. Positively, remote working also offers an opportunity to conduct research which is more cost-effective and population-based, rather than relying solely on clinic-based recruitment.
Opportunities Presented by the CARE Program
Addressing Methodological Challenges
Advances in patient-centred care delivery have previously been hampered by a range of methodological challenges, described by several reviews over the last two decades.57,58,69 To address these challenges, the team is engaging in extensive qualitative investigation, and ensuring the involvement of patient and parent representatives throughout the research process, both of which are essential components of gaining richer insight into healthcare experiences and the unanswered questions that matter to those affected.57,70 In order to guide research and practice in relation to key constructs of interest and interposing factors, the CARE program will validate a conceptual framework for psychological adjustment to CFM.57,58 Quantitative aspects will involve the use of outcome measures, carefully selected on their ability to collectively capture all aspects of the conceptual framework consistently over time, as well as their psychometric properties, the general population norm data available, and their previous use in cleft and craniofacial research.57,69 Both generic and condition-specific constructs will be included, in order to distinguish between normative levels of concern and the intricacies of the condition itself. 57 In addition, elements of positive growth and resiliency will be captured, as well as areas of difficulty. 71 The size and multi-site approach of the CARE program should allow for examination of the complexities within and between clinically important subgroups and international variation.69,72 The inclusion of healthcare professionals’ views on the current state of CFM care will identify potential barriers to creating an optimal service, and pragmatic methods of facilitating improvements. 62 Finally, CARE will examine adjustment across the lifespan, with the registry offering longitudinal data, which is ultimately needed to establish when and how particular issues become pertinent, and in the delivery of age-appropriate care.58,69
Building a Sustainable Interdisciplinary CFM Community
Given the level of investment in the CARE program and the collective reach of the partners, there is potential to build an international network of caregivers, individuals with CFM, and professionals, with sustainability beyond the current 5-year funding period. These efforts have already begun with the establishment of the CARE registry. The primary aims of the registry are to engage the CFM community in research, and address priority questions generated by this community. More broadly, the registry represents a crucial opportunity to bring the CFM community together in the long-term, through the sharing of research progress, patient driven resources, and opportunities for collaboration across stakeholder groups. Ideally, this international infrastructure will not only ensure the success of the CARE program, but also that of future research and resource development.
Creating Opportunities at all Career Levels
In addition to creating opportunities for established academics and clinicians to collaborate, the CARE program offers opportunities for early career stakeholders, including students and trainees from a broad range of disciplines to engage in the work. Interested stakeholders are invited to contact the CARE team via the website to discuss their ideas and requirements, and subsequently to complete an application. All sub-studies must be aligned with the CARE mission, vision, and values, and will be carefully monitored in relation to pre-agreed expectations and timelines. In the longer term, access to registry data will also be possible.
Conclusions
Research exploring the psychosocial impacts of CFM and related healthcare experiences remains relatively limited. Treatment protocols vary widely across centers and no standardised psychological assessments or support is currently available. The CARE program will increase international understanding of the prevalence of psychological concerns in the CFM population and improve identification of those who may be vulnerable to psychological distress. Determining the appropriateness of current care provisions in addressing psychosocial needs and identifying barriers to the delivery of optimal care will be vital in directing future research into interventions and improvements in clinical care.
Footnotes
Acknowledgments
This study was carried out as part of the “Craniofacial microsomia: Accelerating Research and Education (CARE)” research program, funded by the National Institutes of Health (1R01DE029510-01). The CARE research team includes: Kiley Bijlani, Dr Craig Birgfeld, Dr Linda Caron, Bruna Costa, Dr Canice Crerand, Kristen Daniels, Dr Amelia Drake, Dr Kelly Evans, Dr Kristin Billaud Feragen, Dr Carrie Heike (Co-PI), Dr Matthew Hotton, Albert Hsu, Dr Alexis Johns, Dr Maarten Koudstaal, Dr Leanne Magee, Dr Christy McKinney, Angela Mills, Muhammad Rahman, Amy Schefer, Dr Nicola Stock (Co-PI), Laura Stueckle, Erik Stuhaug, Melissa Tumblin, and Dr Paul White. The CARE team would like to thank the Institute of Translational Health Sciences for their guidance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was made possible by the following grant support: 1R01DE029510-01, UL1 TR002319, KL2 TR002317, and TL1 TR002318 from NCATS/NIH.
Prior Dissemination
The work contained in this manuscript was presented at: the 79th Annual Meeting of the American Cleft Palate-Craniofacial Association, Fort Worth, TX, and the 14th International Congress of Cleft Lip, Palate & Related Anomalies, Edinburgh, UK.