
Abstract
This case report demonstrates a rare finding of a pediatric patient with Morning Glory anomaly and Moyamoya Disease with a palatal meningeal hamartoma discovered as a mass within a previously repaired incomplete cleft of the alveolus. Oral meningeal hamartomas are exceedingly rare with only two palatal cases described and none within a cleft palate or alveolus. These findings prompt a review of oral hamartomas with meningeal subclassification. Further discussion describes the relationship of the proposed origins of meningeal hamartomas within the setting of cleft palate development.
Introduction
Hamartomas are benign, unencapsulated masses defined as a proliferation of disordered mature connective tissue. Within the connective tissue, there is a predominance of particular tissue subtypes native to the associated anatomical region. 1 These may occur spontaneously or be associated with chromosomal syndromes. Presenting either at birth or developing later in life, they have a limited growth after adolescence as they grow in concordance with the surrounding tissues.
With a preponderance for structures within the thoracic and abdominal cavities,1,2 head and neck hamartomas are considerably rarer, particularly within the oral cavity.2,3 The eclectic subtypes that have been reported in the oral cavity are in part due to the diversity of different tissues types within a small anatomic area, spanning from odontoid, vascular, to neural. 1 Fundamentally, each tissue type may conceivably be found within that region, in contrast to choristomas which are similar collections of disorganized tissue growth, however, contain tissue types that are unrelated to that anatomic area.
Those with meningothelial tissue are exceedingly rare upon review. If meningeal tissue is identified within the oral cavity specifically, the tongue historically is the primary location reported, 4 with a accompanying paucity of palatal reports. Meningothelial hamartoma origin is controversial despite first being described by Suster in 1990. 5 Proposed origins include abortive neural crest migration to meningoceles with eradicated communication intracranially.6–8 The Tekkeşin report 9 of prior oral cavity meningothelial hamartomas argues for meningothelial tissue to be categorized as a hamartoma designation, rather than that of the aforementioned choristoma. Meningeal tissue, it is argued, is one that may feasibly be found during development due to rests of ectopic tissue being displaced during cranial development.
Upon literature review, a published collection of only two palate cases is noted. 9 This case exhibits a multifaceted report of a meningeal hamartoma that developed within a previous alveolar cleft repair.
Case
Our patient originally presented as an infant with a midline cleft of the upper lip and alveolus (Figure 1), symptomatic submucous cleft palate exhibiting nasal regurgitation, overdeveloped labial frenulum (Kotlow Grade 4), and ankyloglossia. MRI was obtained at 3 weeks of age for central sleep apnea. This demonstrated no significant cerebral deformity or encephalocele. On radiologist's review, there was no cleft noted but on review, there was splaying of the soft tissues present at central maxillary alveolus. Initial surgical correction was carried out at six months of age due to continued difficulty feeding. Surgery included labial frenuloplasty, repair of the midline cleft of the lip and primary and soft palate cleft, and lingual frenectomy. Gingival tissue rearrangement was performed for the alveolar cleft without gingivoperiosteoplasty. Subsequently, he was diagnosed with Morning Glory anomaly of the left eye. Further workup revealed Moyamoya Disease of the left internal carotids and proximal middle cerebral artery treated with vascular bypass. Patient continued to be followed in craniofacial clinic and on exam, nearly 24 months after the original repair, a pink mass on the anterior mid hard palate adjacent the incisive foramen was identified, clinically appearing as excess mucosa or granuloma (Figure 2). This 0.5 cm tissue was pedunculated just posterior to the site of previous repair of the primary palate (Figure 3). The mass did not extend deeply nor was there apparent nasopalatine nerve involvement. The new mass was excised intraoperatively in its entirety with expectation of benign mucosal overgrowth.
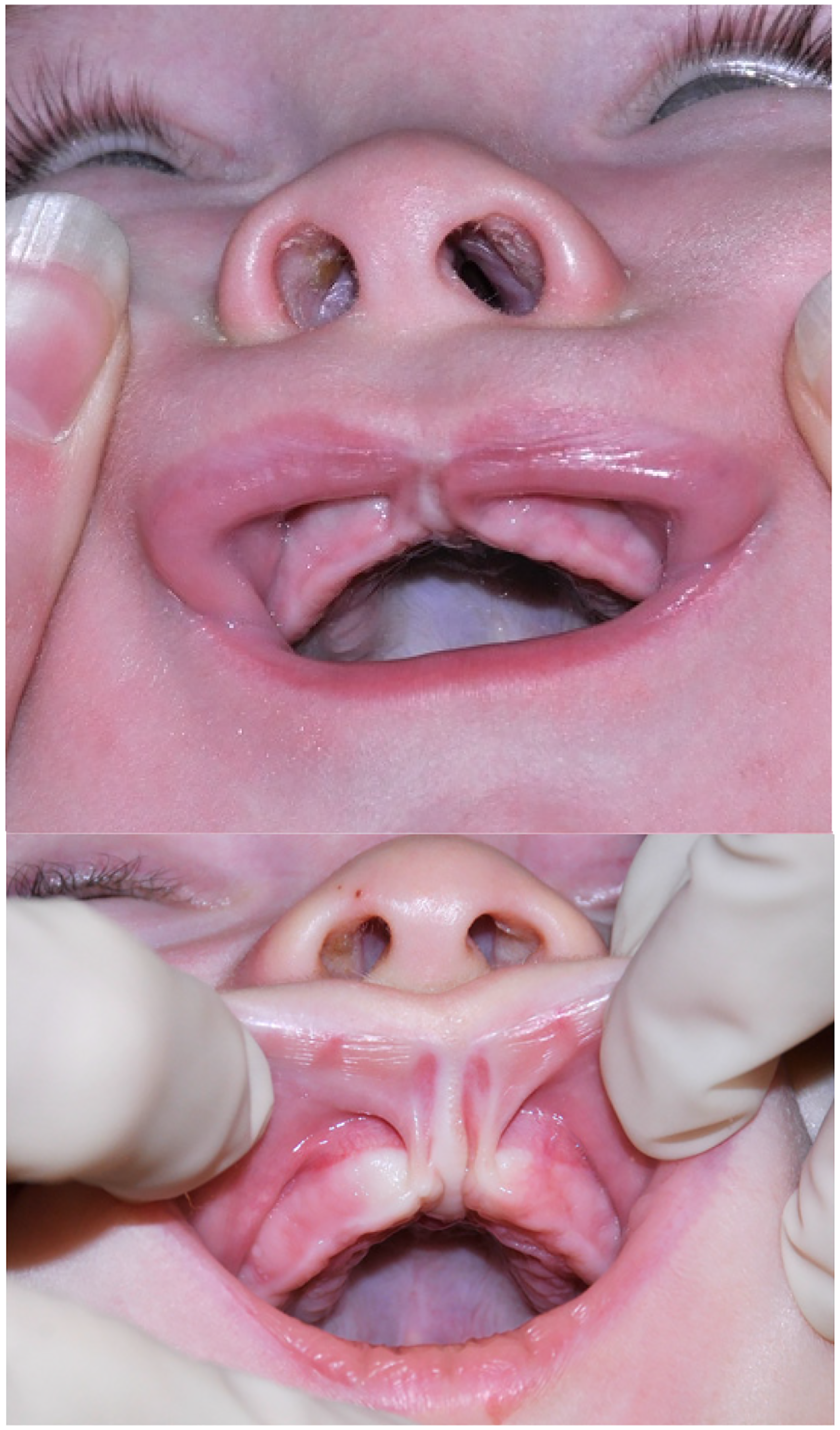
Demonstrates incomplete midline alveolar cleft and lip cleft and prominent frenulum.
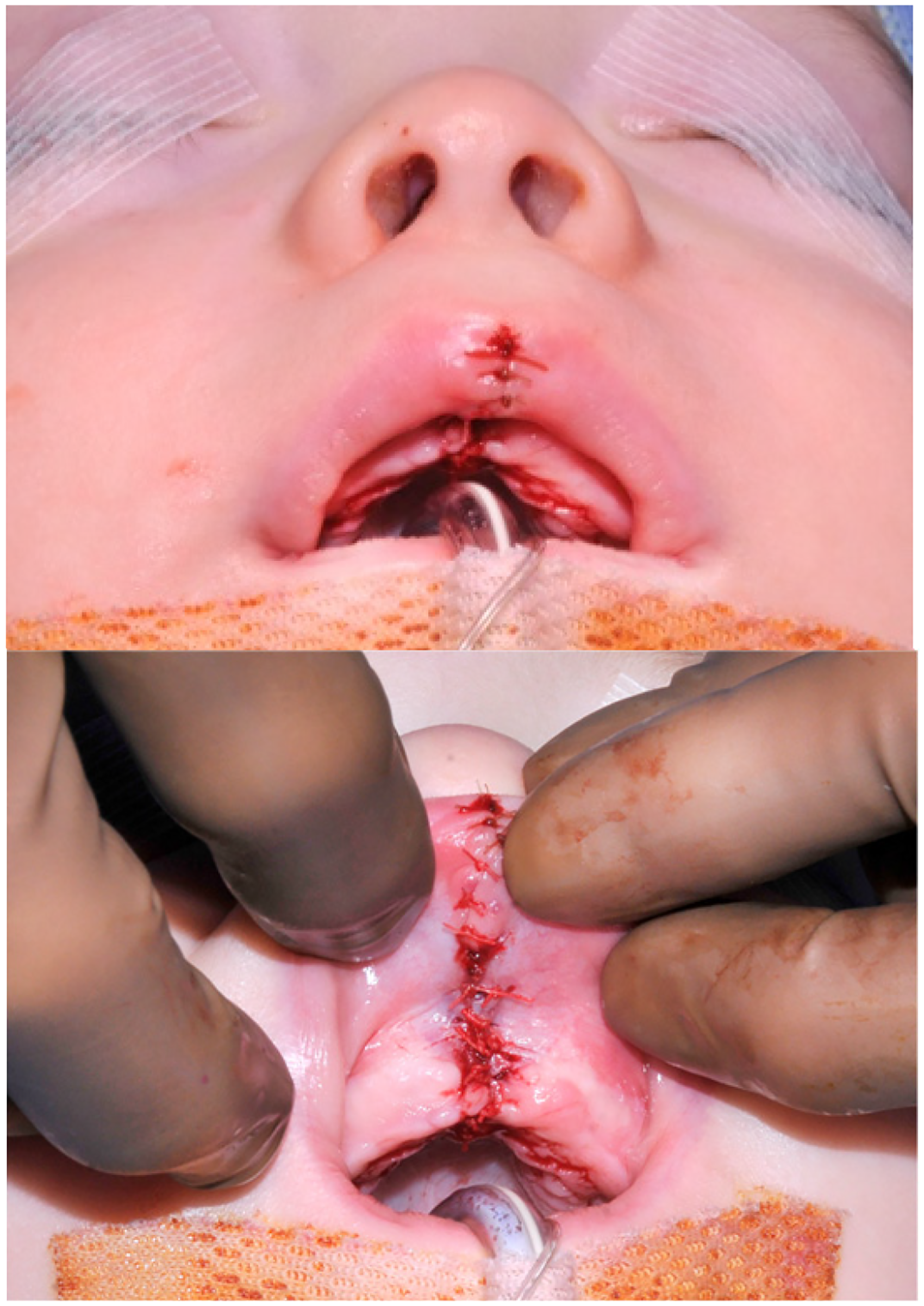
Post-operative frenulectomy and midline cleft lip and alveolar repair.
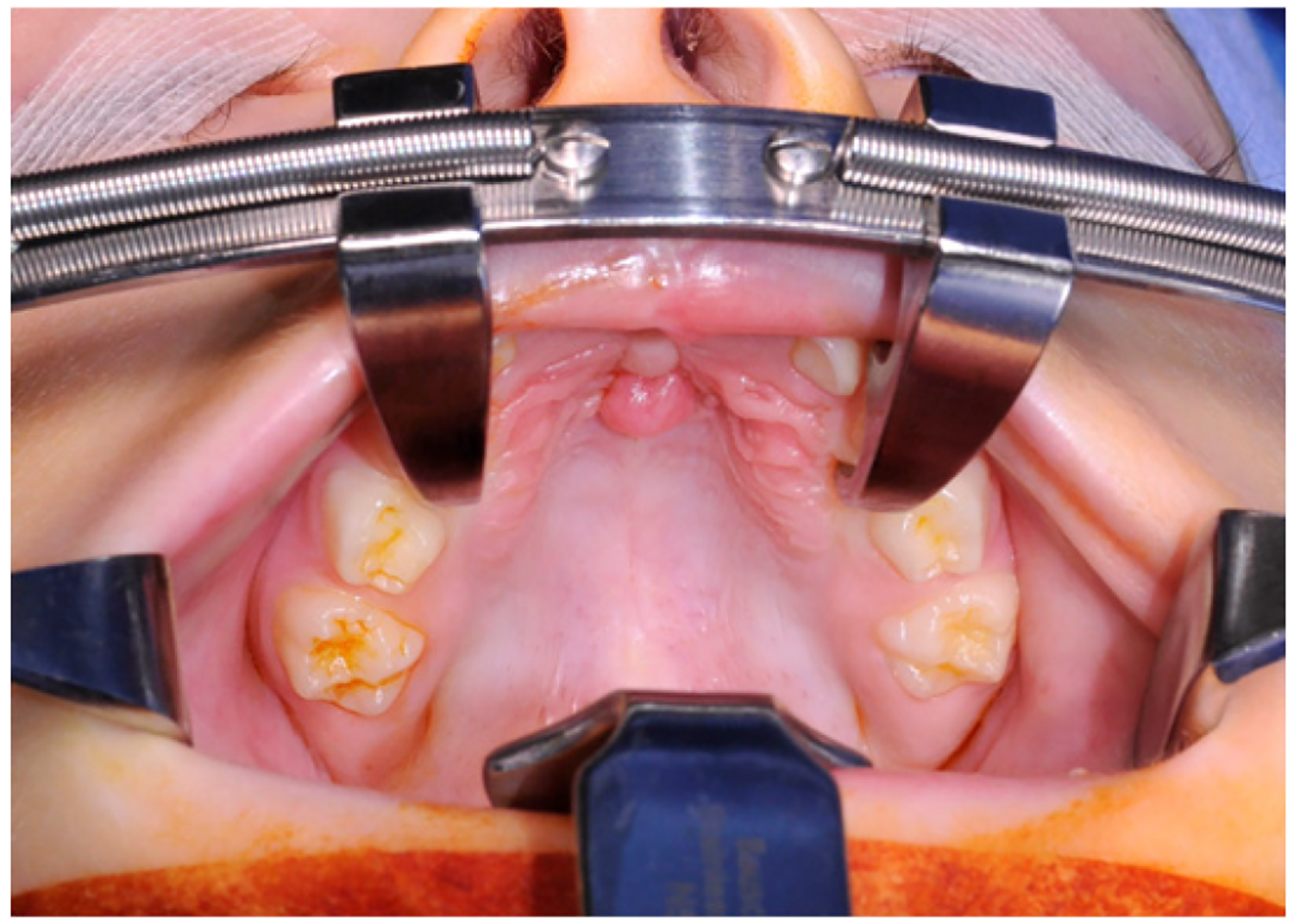
Pedunculated growth at juncture of primary and secondary palate, immediately posterior to prior repair.
Pathology
Reported by the pathology lab as a polypoid portion of tissue with meningothelial heterotopia, sections showed tissue lined by keratinizing squamous epithelium. In the underlying tissue there were a few cystically dilated spaces lacking a definitive lining (D < 40 non-1mmunoreactive) and cleft-like spaces. The cleft-like spaces were lined by bland round to spindled cells that show EMA immunoreactivity and no S-100 immunoreactivity. Admixed with these cleft-like spaces were thin strands and nodules of dense collagen.
Histology
Typically, hamartomas arise within the subcutaneous tissue or occasionally the dermis with a histologically normal epidermis. 10 The characterization of these lesions was defined in 1990 by Suster et al. with the meningothelial elements closely intermixed within haphazard connective tissue elements and freely anastomosing vascular channels. Immunohistochemistry demonstrates positive epithelial membrane antigen antibodies and Vimentin in epithelioid cells, indicating a meningothelial classification. Importantly, S-100 and HMB-45 are negative, providing rejection of melanocytic origin. 10 In Suster's original paper in 1990, the comparison to angiosarcoma was drawn given the prominent vascular channels, highlighting the importance of exclusion. Screening for this is via negative staining for Factor VIIII. 5
Discussion
The oral cavity has eclectic tissue types within a confined anatomical region allowing for a variety of hamartoma subtypes. The differing subtypes are classified by their predominate tissue types. These subtypes are only limited by the available tissue subtypes of the oral cavity. They can range from vascular, odontoid, to osseous. A meningeal hamartoma within the head and neck is a rare finding and exceptionally rare within the oral cavity. Historically, meningeal subtypes are more commonly encountered in the thoracic and abdominal cavities. Those previously reported in the head and neck have primarily been located within the scalp and occasionally the tongue.
Controversy exists regarding meningothelial hamartoma origin. The variable theories proposed range along a spectrum from cutaneous meningiomas, abortion of neural crest cell (NCC) migration, meningoceles with absent intracranial communication, to proliferation along existing nerve pathways. Given that definitive definition of its source has not been illuminated, discussion of these pathways is warranted, particularly in connection with that of a corresponding cleft palate as in this case.
Normal facial development is an intricate process, beginning externally between the 4th and 6th week of embryonic development. A palatal cleft hamartoma highlights how both appropriate palate closure and meningeal tissue location depend on neural crest formation and differentiation. Between the 6th and 8th week, the palate begins to develop. This development is reliant on mesenchymal tissue made from pluripotent neural crests which themselves develop from the neural ectoderm. 11 These then proceed to migrate and differentiate, entering the pharyngeal arches. The relationship of pharyngeal arches and the appropriate development and migration of neural crest cells is critical to facial development with the arches and their NCCs producing facial cartilage, bone, connective tissue, sensory neurons, and a multitude of other cell types. The neural crest cells migrate from the forebrain and midbrain into the frontonasal, palate, and periocular areas while the caudal midbrain NCC extend to the maxillary component. 12 These continue to contribute to development of the maxilla and palate mesenchyme. 11 Additionally, the same NCC forebrain regions provide the forebrain meninges. This shared origin provides further plausibility of extracranial meningeal tissue while not excluding persistent precursor migration along the cranial verves exiting from associated foramina during development.
Additionally, the paired pathways lends plausibility of native meningothelial tissue within the oral cavity, mitigating the classification of meningothelial hamartoma rather than that of a choristoma. 9
The specifics of palatal development in relation to NCCs is beyond the scope of this report, however, a general review is as follows; as the nose develops, the medial nasal prominences fuse, creating the intermaxillary segment. This segment will broaden and project posteriorly, giving rise to the primarily palate. The secondary palatal body is comprised of mesenchyme tissue, primarily from NCC. The associated palatal shelves develop from the maxillary prominence in a vertical fashion and grow inferiorly towards the tongue.13,14 As the mandible continues to mature, the tongue is shifted inferiorly. The tongue's displacement allows for the palatal shelf axis to rotate into a more horizontal plane, finally fusing with the primary palate anteriorly6,11,13,15 .This normal palatal development can be hindered by both sporadic extrinsic and congenital intrinsic factors. Spontaneous structural impedance may result from a congenital mass or as part of obstructive physiologic consequence as in the case of Pierre Robin Sequence in which the tongue is malpositioned due to micrognathia, preventing complete fusion.11,13
NCCs and neural crest-like stem cells (NCLSC) can maintain an amount of pluripotency postnatally. NCLCs have been identified within the palate, oral mucosa, and tongue. These have demonstrated the ability to demonstrate multilineage differentiation even if collected in adulthood. 16 These cells have been able to be manipulated in vitro and differentiate into a multitude of tissue types, ranging from odontoblasts to glial cells. Further research is necessary into ectopic meningeal tissue in its relation to this ongoing pluripotent activity.
For the discussed patient, a diagnosis of Morning Glory Anomaly was found. It is important to note that individuals with Morning Glory syndrome may have associated midline facial and brain anomalies Including agenesis of the corpus callosum, transsphenoidal encephalocele (which can result in a cleft of the soft palate) and midline upper lip cleft. 17 Our patient had a submucous cleft palate and midline cleft of the lip and primary palate but no encephalocele or midline brain anomalies as documented on MRI and nasal endoscopy.
When encountering a mass in the pediatric population, balancing diagnostic intervention and prudent observation is paramount. In the oral cavity, the ability for rapid progression and proximity of vital structures prioritizes the exclusion of neoplastic activity. Differentials are broad and clinical exam is nonspecific. Reactive tissue lesions, vascular lesions, meningiomas, or other hamartoma subtypes are all feasible with this presentation. Ectopic meningiomas are markedly similar on a histochemical and histopathologic analysis. Distinction is possible given hamartomas have a less defined border in comparison and the meningothelial tissue is more arbitrarily coalesced within the connective tissue. Histologic areas simulate freely anastomosing vascular channels which have a similar appearance to that malignant masses as they are lined by round to spindle-shaped slightly hyperchromatic epithelioid cells. 5 Distinction from specific etiologies of melanoma and angiosarcoma can be provided via immunohistochemistry. Pertinent findings are the absence of S-100, HMB-45, Ki-67 proliferation and negative Factor VIII for melanoma and angiosarcoma respectively. The epithelioid cells present will be positive for epithelial membrane antigen and vimentin, helping to further define the meningothelial component. 6
We present a case report as an interesting framework to discuss the complex nature of head and neck development while providing floor for discussion on the pathophysiology surround ectopic meningeal tissue. Pediatric head and neck masses, particularly of the oral cavity, can be exceptionally diverse and a broad differential and clinical acumen is paramount.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article