
Abstract
Objective
A protruded premaxilla has always been challenging to care for by cleft care professionals. This study aims to fortify the use of a single-stage premaxillary setback, with posterior vomerine ostectomy and primary cheiloplasty to achieve proper care for patients with bilateral cleft lip and palate (BCLP) and protruded premaxilla.
Design
Longitudinal retrospective analysis.
Setting
Twenty-three outreach programs to four countries (Ecuador, Lebanon, Peru, and El-Salvador) between 2016-2022.
Patients/Participants
Sixty-five patients between the ages of 3 months and 6 years and 5 months, with BCLP and severely protruded premaxilla underwent premaxillary setback via posterior vomerine ostectomy and primary cheiloplasty. Patients with diagnosed syndromes and inaccessible vomer bone due to fused palates were excluded from the study.
Interventions
Premaxillary setback with posterior vomerine ostectomy, bilateral gingivoperiosteoplasties (GPP), and primary cheiloplasty.
Main Outcome Measure(s)
Postoperative complications and aesthetic outcomes.
Results
The mean age at surgery was 13.17 ± 14.1 months, with an average follow-up time of 26 ± 17 months. Patients underwent their procedures in Ecuador (72%), Peru (9%), Lebanon (8%) and El-Salvador (1%). The majority of patients were aged 1 year or less (66.7%) and were males (58.5%). All patients were operated on successfully and had good aesthetic outcomes. Only one patient developed partial necrosis.
Conclusion
Patients with BCLP and severe premaxillary protrusion have always carried immense social, psychological, and financial burdens, especially in outreach settings. Our described single-stage technique has proven to be safe and effective with good aesthetic results. Further follow-up after primary repair should be done to document and ensure proper facial growth and normal nasolabial maturation.
Keywords
Introduction
Clefts of the lip and/or palate affect about 1 out of 700 live births. The prevalence varies significantly by geographical region and population. Early surgical repair can greatly improve aesthetic and functional outcomes, psychosocial well-being, and quality of life while decreasing the economic burden that accompanies this deformity.1,2 However, many patients lack proper access to healthcare and awareness, especially in underserved settings. Consequently, they can often have a late presentation, beyond the recommended age for cleft lip (3-6 months) and palate repair (9-12 months) or may not seek surgical treatment at all. 3
A prominent premaxilla is a prevalent feature of complete bilateral cleft lip and palate (BCLP). Cleft lip repair, without addressing the severely projected premaxilla, can result in weak muscle apposition and a distorted prolabium with a widened inter-alar distance and stretched labial scars. 4 Undesirable functional repercussions can include malocclusion, fistula formation, suboptimal oral hygiene, speech difficulties, and psychosocial distress. 5 Patients with poorly repaired lip often face social stigmatization and bullying, that can lead to poor quality of life, and difficulty integrating into the workforce. The parents of these patients also face their own challenges and are often being pulled away from the labor force to take care of their child.6,7 Therefore not having the right surgical training and know-how while trying to repair a BCLP with a projected premaxilla can often lead to more deleterious consequences than not repairing it at all. (Figure 1).
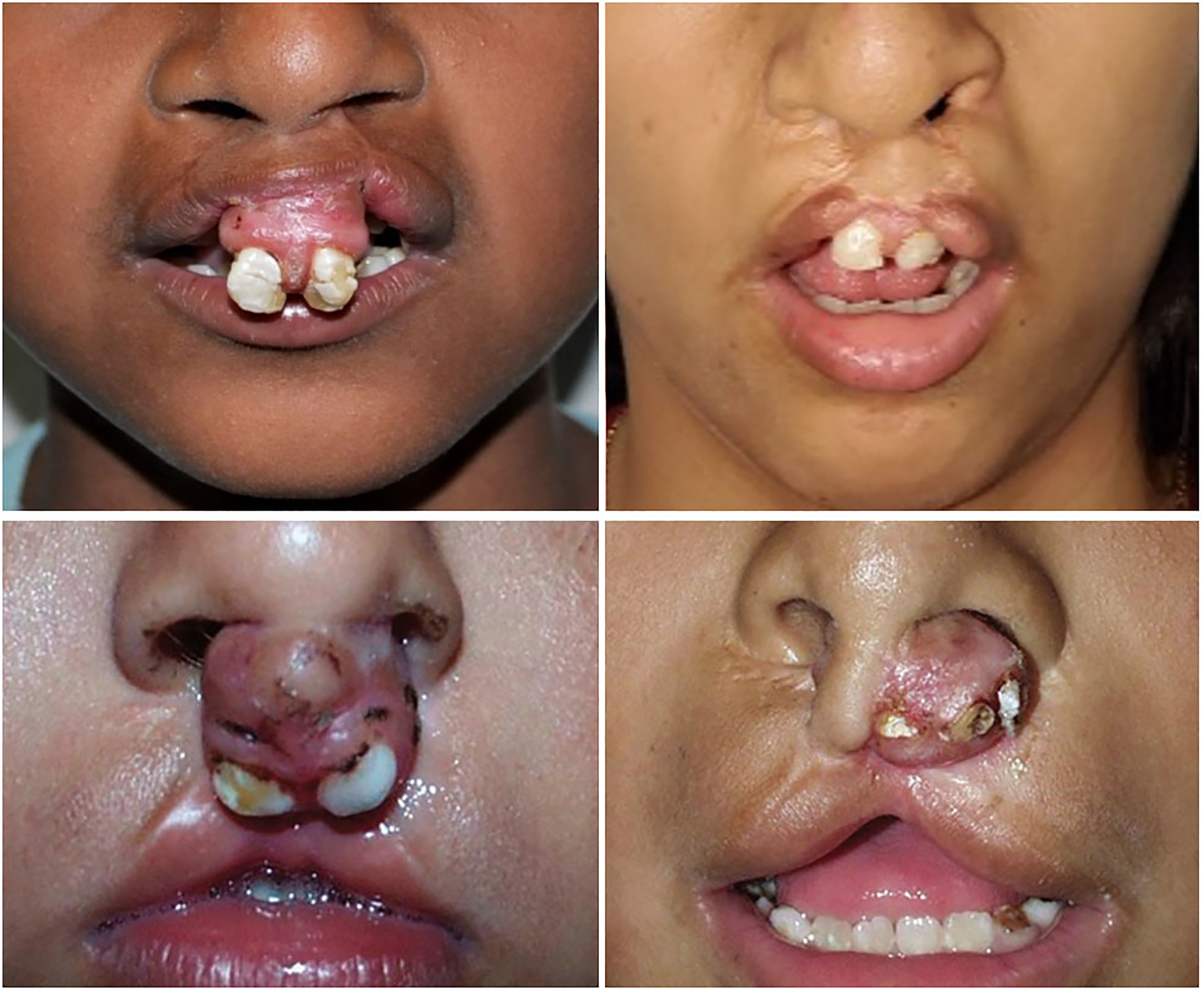
Failed outcomes at repair of bilateral cleft lip with protuberant premaxilla.
Extraoral and intraoral orthopedic appliances providing external compression such as nasoalveolar molding (NAM), Burston plates, and Latham appliances have been described and are commonly used to address the protruding premaxilla. 8 The use of presurgical orthodontic treatment can decrease the level of both nasal and lip deformities by narrowing the cleft and repositioning the nostrils. It also allows elongation of the columella, provides better aesthetic outcomes, and reduces the number of subsequent surgeries. 9 Even though these appliances have been successful, they require long-term, regular follow-up and are not readily available in low socio-economic settings. 10 Late patient presentation further complicates corrective surgery as it diminishes possible treatment options: vomer ossification with time prevents any applicable retrusion technique as it leads to locked-out premaxilla.
Lip adhesion has been proposed as an initial stage for repairing wide clefts. However, this method has been associated with wound dehiscence and necrosis due to increased tension on the lip, leaving patients with a scarred upper lip, scarred orbicularis oris muscle, or scarred prolabial flap. 8 Scarring also makes subsequent corrective surgeries more complex. Several approaches to surgical premaxillary setback have been described since the nineteenth century, but consensus has yet to be reached on the optimal technique, with practice differing significantly among surgeons and centers. 11 Vomerine ostectomy allows repositioning of the projected premaxilla. It decreases tension from the projected premaxilla on the repaired lip, decreasing the risk of wound dehiscence and infection. However, vomerine ostectomy during premaxillary setback anterior to the vomero-premaxillary suture (VPS) has been associated with higher risks of premaxilla necrosis due to damage of the blood supply, mainly from the dorsal nasal artery. 12 When paired with concomitant nasolabial repair and alveolar gingivoperiosteoplasties (GPP), this risk becomes even higher. 13 Staged repair has also been described to address the risks of premaxillary necrosis, especially in children older than one year of age. 14
This study presents the long-term outcomes of premaxillary setback using a posterior vomerine ostectomy. This is a single-stage surgical procedure that includes premaxillary setback with posterior vomerine ostectomy, bilateral GPP, and bilateral cleft lip repair with primary rhinoplasty while minimizing the risk of complications such as premaxillary necrosis. To date, this article represents the largest case series of premaxillary setback in patients with BCLP.
Material and Methods
This retrospective study evaluated patients who underwent primary bilateral cleft lip repair with premaxillary setback from September 2016 to May 2022 in Ecuador, El Salvador, Lebanon, and Peru. Patients with a BCLP deformity and a severely projected premaxilla of at least 10 mm were included in the study. Those who did not qualify for surgery were patients younger than 3 months, underweight patients less than the fifth percentile, those with fused palates due to inaccessibility of the vomer, and those with syndromic features or cardiovascular anomalies. Patients meeting inclusion criteria underwent single-stage premaxillary setback with posterior vomerine ostectomy, bilateral GPP, and bilateral cleft lip repair with primary rhinoplasty. Surgery was performed by six different surgeons throughout the study period. Follow-up was possible through local multidisciplinary cleft care centers and regular annual or biannual visits by a visiting cleft team that includes surgeons, pediatricians, anesthesiologists, dentists, nurses, psychosocial experts, and speech and language pathologists. The COVID-19 pandemic promoted the use of telehealth for patient follow-up which was quickly adopted to ensure continuity of care. Direct postoperative complications such as infection, dehiscence, and necrosis of the premaxilla were assessed for each patient 1-2 weeks post-surgery. Six months after primary surgery, pre-maxillary mobility was assessed. Patients’ aesthetic outcomes were evaluated by the visiting surgeons upon follow-up either bi-annually or annually. Several key features of the repaired lip and nose were taken into consideration by the examining surgeons and were noted to either be present or not:
Proper alignment of Cupid's bow Symmetry of Cupid's bow peaks respective to the nostril bases Orbicularis oris muscle continuity throughout the upper lip Philtral ridges symmetry and adequate fullness of philtral tubercles Proper support and projection of the top of the nose, with adequate columellar fullness Symmetrical out-flaring of the medial crural footplates, and symmetrical width and shape of the nostrils Adequate positioning of the premaxilla and its proper alignment with the secondary palatine shelves
Written informed consent for surgery, participation in study, as well as utilization of patient information and photographs, was obtained for all patients and signed by their legal guardians. This study was performed in concordance with the principles outlined in the Declaration of Helsinki. Institutional review board approval was obtained from the institution's ethics and research committee. Patient demographics and data were obtained by reviewing patients’ charts stored in the electronic medical records. Descriptive analysis was performed using SPSS v 28.0 (IBM).
Surgical Technique
The surgical technique has been previously described by the first author. 15 Indications for premaxillary setback include protrusion of the premaxilla of at least 10 mm, locked-out premaxilla, failed pre-surgical orthopedic and lack of alternative treatment option. Surgical planning is centered on the physical examination of the premaxilla: the size of the ostectomy correlates with the extent of protrusion of the premaxilla and aims for continuity of the premaxilla with the maxillary arch. Surgery is performed under general anesthesia. After positioning the patient in a supine position with the head extended and securing the endotracheal tube, marking of the lip is performed. Surgical marking for cleft lip repair follows the nasolabial marking described in the Interdisciplinary Cleft Care: Global Perspectives (ICCGP) textbook. 15 External nasal and infraorbital nerve blocks are then performed using an equal mixture of 0.25% lidocaine, and 0.125% bupivacaine with 1: 1 50 000 epinephrine with a max dose of 1 mg/kg for patients under 12 years of age. The same local mixture is injected under the vomerine mucoperiosteal flaps maximizing the vasoconstrictive effect and facilitating the elevation of the vomerine flaps. The GPP incision area, the medial edge of the secondary palatine shelves, the alar footplate, the prolabial flap, and the upper lip are also injected at this time. To optimize the vasoconstrictive effects of epinephrine, incision time is delayed until 12 min after injection. For patients over 12 years of age, an equal mixture of 0.5% lidocaine, 0.25% bupivacaine with 1: 1 50 000 epinephrine is used without exceeding 0.5 mg/kg per patient.
A “conjoint double-Y” marking is made with the anterior part being at least 5 mm posterior to the vomero-premaxillary suture
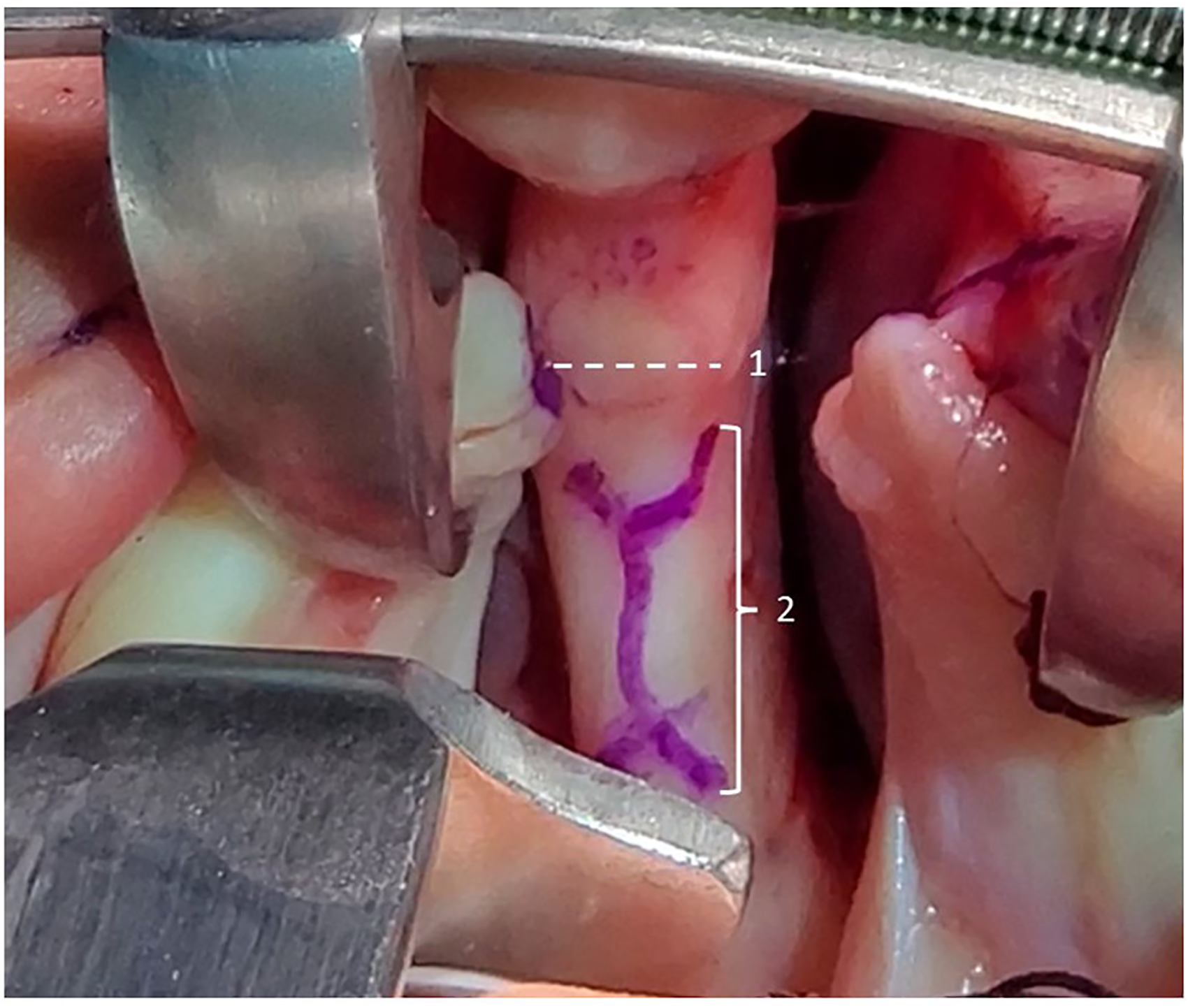
“Conjoint double-Y” marking with the anterior margin being at 5 mm posterior to the center of the VPS.
Premaxillary setback is performed by digital pushback and retropositioning making sure the maxilla is aligned with the secondary palatine shelves. The vomerine mucosa is closed over the ostectomy site with 5-0 Vicryl © on RB-1 needle.
Bilateral GPP are performed to stabilize the premaxilla in its new position, using an “8-point fixation system”. Four anchor sutures are placed on each side of the GPP, two on the palatal side and two on the buccal side. Constant pressure is applied during this suturing process to prevent the premaxilla from moving and creating a gap with the lateral palatal elements. The premaxilla is not released until all anchor sutures are tied.
Primary bilateral cleft lip repair is done following the steps described by the first author in the ICCGP reference textbook. 15 Cupid's bow symmetry and alignment, as well as philtral length and fullness, are essential to achieve successful outcomes. Cartilage sparing cleft lip rhinoplasty is performed through a columellar access with gentle separation of the overlying nasal skin from the underlying lower lateral cartilages to allow their medial repositioning and subsequent double dome suture application.
This is followed by meticulous repair and approximation of the orbicularis oris using the V-Cheiloplasty technique, enabling lip lengthening and medial mobilization of the alae, ensuring balanced and careful repair of the orbicularis oris muscle and the formation of the philtral tubercle.
Special attention should be given when aligning the prolabial flap with the cupid's bow. A short prolabial flap results in blunting of the nasal tip, a short- to non-existing columella, and a gap in height between the short prolabial flap and the newly reconstructed Cupid's bow, yielding potentially unappealing outcomes. This flap can be lengthened by creating relaxing incisions that extend from the lateral side of the columellar flaps into the membranous septum, allowing the flap's inferior mobilization towards the newly created Cupid's bow. The Stepdown Technique is another method that compensates for the height difference between the prolabial flap and the newly established Cupid's bow, by lengthening the available skin in the flap. 15 The first suture on the prolabial flap is placed 1 mm below the columellar-labial crease and angled 2-3 mm inferiorly towards the advancement flap. The second suture is placed 2 mm below the columellar-labial crease on the other side and is also angled 2-3 mm inferiorly. At this stage, the remaining non-sutured portion of the prolabial flap is well aligned with the upper edge of the vermilion border, resulting in tension-free approximation of the lip. Cleft palate repair is delayed to a second surgery.
Postop Care and Follow up
Patients are placed on a liquid diet until discharge (Post-op Day 1). Patients are then instructed to follow a mashed diet for at least two weeks, after which a regular diet can be resumed. Breastfeeding can be started on day 1 post-surgery. In low-middle income countries (LMIC) settings, given the inconsistent nature of post-operative care and follow-up, a successful approach has been to prescribe a five-day course of oral broad-spectrum antibiotics, and a seven-day course of topical antibiotics to begin after the Dermabond falls off. All patients are instructed to come back for in person follow-up 7 and 14 days after their surgery along with daily virtual visits via telehealth. In addition, guardians are also instructed to contact local cleft providers in case of any emergency prior to their scheduled follow-up. Legal guardians are instructed to begin circular massage of the upper lip, over the lip scar starting 6 weeks after surgery. Massages are ideally done five to six times a day for five to six months to prevent the development of a hypertrophied scar. Patients are also instructed to limit sun exposure and apply sunscreen to the scar for one year after surgery to decrease hyperpigmentation of the scar.
All patients are reassessed regularly by our onsite teams and aesthetic and functional outcomes are evaluated and documented every 6 months.
Results
Between May 2016 and May 2022, 65 patients underwent premaxillary setback with vomerine ostectomy. Patients underwent their procedures in Ecuador (72%), Peru (19%), Lebanon (8%), and Salvador (1%). Patient travel time ranged between 15 min and 10 h with an average of 2.4 h. Two-thirds of our patients were aged one year or less, while the remaining one-third ranged between 1 year and 6 years and 5 months with a mean age at surgery of 13.17 ± 14.1 months. Fifty-eight percent of our patients were males. Patients who were operated on mainly presented for a single stage bilateral cleft lip repair and premaxillary setback and were not previously operated on. Average operative and anesthetic times were 152 ± 61 min and 213 ± 95 min, respectively. Of our 65 patients, 8 patients were lost to follow up and the remaining 57 patients had an average follow-up time of 26 ± 17 months (ranging between 5 months and 71 months when followed up for aesthetic outcomes). Eight parameters for aesthetic outcomes were evaluated in all 57 patients and are notated in Figure 3. Figures 4 and 5 showcase the outcomes of two patients who underwent single-stage premaxillary setback with primary bilateral cleft lip repair, GPP, and primary rhinoplasty. Upon follow-up, 12 of our 57 patients exhibited minimal premaxillary mobility at or after 5 months postoperatively. In the case of a mobile premaxilla, a revisional GPP is performed at the same time of Alveolar Bone Grafting (ABG). Only 1 patient had partial premaxillary necrosis and no patients had dehiscence of the lip or severe wound infection postoperatively.
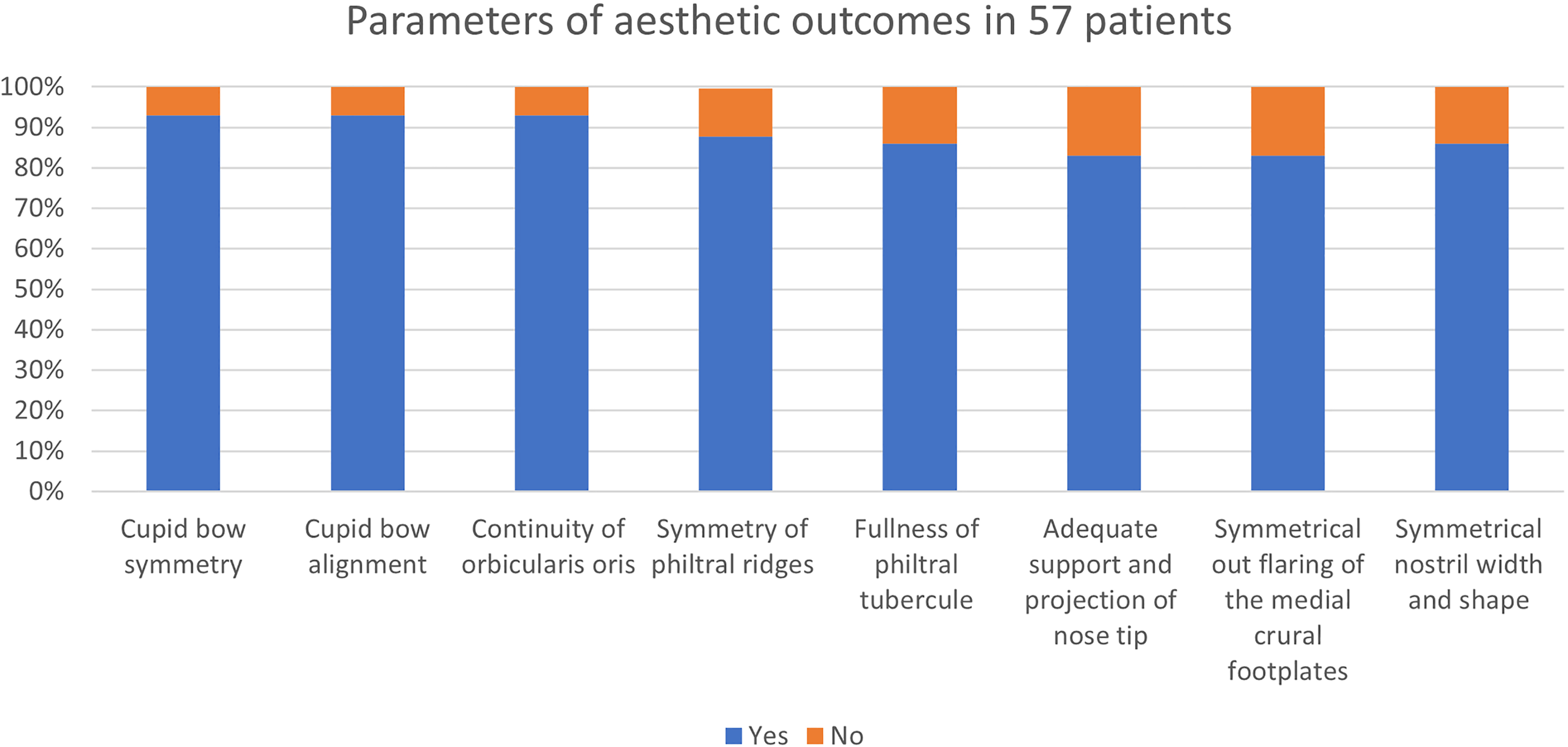
Parameters of aesthetic outcomes.

Postoperative outcome at 30-month follow-up.

Postoperative outcome at 36-month follow-up.
Discussion
Several different approaches are adopted for the treatment of patients with BCLP with premaxillary protrusion. These can often include presurgical orthopedics as well as surgical repair. Functional, anatomical, and aesthetic parameters should be taken into consideration when treating these patients. Surgeons seek to preserve functional integrity and anatomical growth of the midface in order to allow proper facial and orthognathic maturation. 10
Finding the proper treatment approach should be designed on a case-by-case basis. Patient age upon presentation, anatomical landmarks, availability of dentofacial appliances can all influence the surgical plan. Early repair provides advantages for proper wound healing and functional adaptation due to neonatal plasticity.2,13 Early planning and effective preventive management will therefore increase the likelihood of successful treatment with improved physical functioning and self-esteem found at a later age. 17 Economic and psychosocial burden on patients and their families are also decreased. In our outreach trips, the age of patients at the time of repair ranged between 3 months and 6.5 years. This greatly depended on the age of presentation and the need for presurgical interventions.
Due to the complex nature of the defect, patients with BCLP and a protruded premaxilla would require multiple surgeries throughout their lives in order to achieve functional adequacy. In an attempt to improve quality of care and quality of life, a single-stage surgical approach was devised. The approach involves using ostectomy to posteriorly reposition the premaxilla and align it with the secondary palatine shelves, allowing for symmetry, nose and lip continuity, and philtral ridge fullness.15,18
During the time of this study ranging between May 2016 and May 2022, 65 patients with BCLP and severe premaxillary protrusion received bilateral cleft lip repair with premaxillary setback, bilateral GPP and primary rhinoplasty during 23 outreach programs in four different countries (Ecuador, Lebanon, Peru, and Salvador). Fifty-seven patients had a continuous follow-up with our team and were therefore included in our analysis.
Twenty-eight percent of our patients received presurgical orthopedic appliances, mainly NAM, in preparation for surgical repair. This intervention can be helpful but requires skilled orthodontists with regular follow-up, typically available in well-developed cleft centers. 13 Therefore, their accessibility may be limited in LMIC, where compliance and follow-up can be more difficult to achieve. To attain maximum effectiveness, their implementation should be started early on, typically before 8-10 months of age, prior to ossification of the premaxillary-vomerine junction. 19 Moreover, the use of NAM has been debated, with some studies finding it beneficial and others suggesting it can cause problems such as premaxillary segment instability or over-rotation due to improper placement, excessive pressure leading to full necrosis, or facial profile concavity.20,21 We contend that the use of presurgical orthopedic appliances when suitable and accessible prior to premaxillary setback is beneficial in reducing the protrusion of the premaxilla thus facilitating nasolabial repair.15,22
Optimal time for cleft palate repair is still debatable, but it is advised for surgery to be performed between 9-18 months of age. Our patients typically receive cleft palate repair 6-12 months following single-stage vomerine ostectomy and bilateral cleft lip repair. Some of these cleft palate repairs were delayed during the COVID-19 pandemic in 2020 through 2021 due to the cancelation of several outreach trips. At the time of cleft palate repair, the vomer bone is exposed and assessed for healing. All patients who had previously undergone vomerine ostectomy were noted to have vomer bone fusion, indicating adequate bone healing capacity. Figure 6A and 6B depict two of our patients, 30 months and 36 months following BCLP repair and premaxillary setback, respectively, showing vomer bone repopulation with reformation of the cortex. A good vascular supply is essential for bone healing, indicating good preservation of vascularization of the vomer bone using premaxillary setback with ostectomy performed posterior to the VPS. 23

(A) Bone repopulation at 30-month post vomerine ostectomy. (B) Bone repopulation at 36-month post vomerine ostectomy.
Koh et al. found that premaxillary retropositioning did not lead to significant long-term midfacial hypoplasia but rather would correctly reposition the protruded premaxilla while maintaining harmony with the mandible. 24 This is further supported by Padwa and her colleagues who observed similar postoperative facial growth profiles between patients who received premaxillary setback at an early age and patients who did not require it. 4 On the other hand, Vinas et al. showed that patients with cleft palate are more likely to develop craniofacial alterations affecting the palate, maxilla, and mandible with any associated cleft lip deformity. This effect was most severe in patients with BCLP. 25 Furthermore, midfacial growth was found to be normal in patients with normal secondary palate receiving bilateral cleft lip repair in several studies.19,26 Palate repair is known to have an impact on mid face growth, but how much it affects patients with BCLP with a protruding premaxilla is not yet established. Study of the craniofacial growth profile of these patients is an area of great opportunity since the protruding premaxilla adds an additional growth element.
It is imperative to keep in mind that GPP does not eliminate the future need for ABG, but it helps reduce the existent wide space in the original defect. This ultimately facilitates the future ABG and reduces potential adverse events. Even though some patients have shown some bone repopulation and teeth regrowth, most patients will require bone grafting in the future. 27 According to Rochlin et al., GPP helps decrease the total number of cleft surgeries in patients with BCLP allowing proper fixation and positioning of the premaxilla. This might, in limited cases, obviate the need for ABG, but more prominently allow for the healthy growth of the premaxilla. 28
Complications of premaxillary setback can include premaxillary segment instability or over-rotation, pressure induced necrosis, and scarring which depend on surgeon's experience and patient compliance. 13 In our study, we found that the single-stage surgical approach described above was successful in achieving good aesthetic and functional outcomes for patients, with a low incidence of complications. This approach is especially beneficial in outreach settings where multiple surgeries and specialized care are often nonexistent or inaccessible. The psychosocial benefits and positive change in the quality of life for these patients and their respective families are significant, and although subjective and difficult to quantify, should be seen as a priority.
Limitations:
Measuring aesthetic outcomes after cleft lip repair can be difficult and there is no universally accepted tool for doing so. While there are many validated aesthetic tools available to measure the outcomes of cleft lip repair, not all of them are suitable for bilateral cleft lip repair. One such tool, the Asher-McDade scale, has been validated for bilateral cleft lip repair but does not consider a protruded premaxilla, and requires a high level of expertise and experience to use accurately, which can limit its applicability in our settings. 29 In this study, we used a simplified method that involved breaking down the desired outcomes into individual categories and determining their presence or absence objectively. Future efforts should focus on developing and validating a user-friendly measurement tool that can aid in the judgment of aesthetic outcomes for patients undergoing bilateral cleft lip repair with premaxillary setback.
Another limitation of this study is its retrospective nature, which makes it difficult to control variables and accurately assess the effects of the technique on facial growth. Additionally, there is no anthropometric confirmation of premaxillary stability or radiographic documentation of premaxillary position following the setback. A prospective, longitudinal study with a longer follow-up period would be useful in comparing premaxillary setback surgical repair outcomes among different surgeons and in analyzing anthropometric data on the evolution of facial growth post-premaxillary setback. This study could also include facial radiographic imaging to document the rate of growth and the size of the premaxilla in infants with BCLP, which could be used to predict subsequent craniofacial morphology.
Conclusion
Through the decades, management of cleft lip and palate has advanced greatly, encompassing numerous and diverse interdisciplinary approaches. The hardships of BCLP with premaxillary protrusion have prevented children in outreach settings to have a life free of social, psychological, and financial burdens. Our single-stage procedure has shown good aesthetic outcomes on nasolabial appearance allowing children to have an improved social and functional life. It also reduces the burden of the deformity on patients, especially those living in an underserved environment. Moreover, anthropometric studies should be done to properly evaluate facial growth after surgery. This can further fortify the validity of the procedure and validate its ability not to interfere with normal facial and nasolabial growth and maturation. The authors are committed to documenting continuous growth profiles of its patients and are currently conducting a study assessing the facial growth of patients who underwent premaxillary setback.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.