
Abstract
Objective
To characterize the epidemiology, identify trends in prevalence, seasonality, and risk factors for orofacial clefts (OFC), selecting the São Paulo state (SPS) population database.
Design
A population-based study to estimate the OFC prevalence trends in recent years, stratified by maternal age and SPS geographical clusters.
Setting
All live births (LB) with OFC in SPS from 2008-2019.
Patients
5342 cases of OFC among 7 301 636 LB.
Interventions
Not applicable.
Main outcome measures
OFC prevalence trends, annual percent change (APC) with a 95% confidence interval, and seasonality.
Results
We found an OFC prevalence of 7.3/10 000LB in SPS, Brazil. Among all the cases, the majority were male (57.1%), Caucasian (65.4%), 77.8% born at term, 75.8% weight >2500 g, 97.1% singleton, and 63.9% of births were by cesarean section. From 2008-2019, SPS presented a stationary OFC prevalence trend; in São Paulo city, the highest APC was observed (0.05%); the maternal age group with the highest OFC prevalence rate was ≥35 years (9.2/10 000LB). We identified the existence of seasonal variation based on the conception date in the final months of the year, corresponding to the spring season (P < .001).
Conclusion
OFC had a stationary prevalence trend in recent years, with the highest prevalence in the Central North Cluster and ≥35 years maternal age group. Seasonality was observed in the spring season, and congenital malformation of lips was the most common associated pathology. This population-based study is the first to summarize the current epidemiology of OFC in SPS.
Introduction
Orofacial clefts (OFC) can be considered one of the main congenital diseases. They result from a fusion failure in the developmental processes of morphogenesis of the facial structures and are associated with functional and aesthetic impairment that is difficult to treat. 1 Several genetic factors have been identified and are thought to be solely responsible for approximately 25 to 30% of cases; however, many cases result from an interaction of multiple risk factors and maternal habits during pregnancy.2,3
The worldwide prevalence of OFC, estimated by the World Health Organization, is 1.4/10 000 live births (LB). 4 In recent years, epidemiological studies have demonstrated different trends in the prevalence of OFC, which may be increasing,5-7 stationary8-10 or decreasing,11,12 depending on the region studied. The highest prevalence in Brazil has been identified in São Paulo state (SPS), 13 but we have no population-based studies that analyze the trend of this prevalence or its seasonality.
The aim of this study was to identify the prevalence trend, seasonality, risk factors and other associated congenital malformations in LB with congenital OFC, in SPS, Brazil, between 2008 and 2019.
Materials and Methods
Study Design & Participants
This is a population-based study, with time trend, 14 following Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) 15 guidelines, using official microdata of all cases of OFC identified by the Live Births Information System (SINASC – Sistema de Informação sobre Nascidos Vivos) The present study was conducted in São Paulo state, which is the most populous in Brazil, with a population of 41 262 199 (2010) 16 and birth rate of 610 000/year, 17 where the completeness of public data is more reliable.18,19 Birth data correspond from January 1, 2008, to December 31, 2019. We extract the data, by the maternal city of residence, from the Unified Health System Department of Informatics 17 (DATASUS – Departamento de Informática do Sistema Único de Saúde), maintained by the Ministry of Health of Brazil. The International Classification of Diseases 10th Edition, 20 (ICD-10 codes Q35.X, Q36.X, and Q37.X) was used to identify all the cases of orofacial clefts (cleft palate, cleft lip, or cleft palate with cleft lip) at the live birth declaration among all LBs in the period of study.
Ethical Statement
This is an audit survey study protocol that uses a secondary, anonymous, public, and open health database, and therefore does not need evaluation, authorization, or ethical approval, from the Human Research Ethics Committee; nevertheless, we followed the stipulated protocol by national and international standards. 21
Variables
Sociodemographic and clinical explanatory variables of LBs, such as gender, race/color, gestational age, birth weight, maternal age, maternal schooling, maternal occupation, type of gestation, type of delivery, and the number of prenatal consultations, were collected. We calculated OFC prevalence trends according to maternal age range (≤14 years, 15-19 years, 20-24 years, 25-29 years, 30-34 years, ≥35 years) and for territorial clusters (São Paulo Metropolitan Region – SPMR, São Paulo City – SPC, Baixada Santista Metropolitan Region – BSMR, Taubaté Administrative Area – TAR, Central South Cluster – CSC, Campinas Region Cluster – CRC, Central North Cluster – CNC, Northwest Cluster – NWE, São Paulo State – SPS), in São Paulo state, following Calderon et al. proposal. 22
Data Sources
We extracted the microdata from the file transfer service provided by DATASUS. The TABNET and TABWIN programs were used to extract the data. These tabs were developed to perform fast tabulations on DBF files, then we expanded the files to XLS version and classified the variables selected for this study in EXCEL®. To minimize possible discrepancies, two researchers collected data independently.
DATASUS developed the Live Birth Information System to gather epidemiological information on births reported throughout the country to subsidize interventions related to women's and children's health for all levels of the Unified Health System (SUS – Sistema Único de Saúde), such as actions of attention to the pregnant woman and to the newborn, as well as the monitoring of the evolution of the SINASC's historical series, which allows the identification of intervention priorities and contributes to the practical improvement of this information system. Through the Internet, DATASUS and the Health Surveillance Service (SVS – Sistema de Vigilância em Saúde) provide the primary information for tabulation on the SINASC's databases.
SINASC provides the number of LBs in SPS. To construct the rates, we collect data according to maternal age group and territorial clusters, year by year (for trend) and month by month (for seasonality).
This database has been validated and previously used for public health and perinatal epidemiologic research and surveillance.6,21,23
Statistical Analysis
We used only the population of LBs to obtain the prevalence rates to remove age bias. Therefore, it is unnecessary to standardize the rates since all the studied population (LB) had the same age. With this, the result obtained by the analysis can be used for comparison to other studies. OFC prevalence rates were calculated for 10 000 LB by territorial clusters and maternal age group in a global period (2008-2019) and two time intervals of 7 consecutive years (2008-2013 and 2014-2019).
We used the Prais-Winsten regression model for trends analysis, following Antunes and Cardoso's 14 methodological indications. The dependent variable was the logarithm of the rates, and the independent variable was the years of the historical series. The annual percent change (APC) of the rates was also calculated, as suggested by Antunes and Waldman. 24
The data modeling process includes transforming the standardized rates into a base 10 logarithmic function using the Durbin-Watson test to measure the existence of first-order autocorrelation of the time series composed of the annual coefficients (β), and to verify if the correlation was compatible with the random regression residuals hypothesis. According to geographic clusters and maternal age groups, annual rates of increase or decrease (APC) were then calculated, with the respective confidence intervals (95%CI). This procedure makes it possible to classify the OFC trend as increasing, decreasing, or stationary, considering to be stationary the trend whose coefficient was not significantly different from zero (P > .05). 14 To facilitate graphical visualization, we performed the 3rd order centered moving averages technique for trends and seasonality.24,25
To model the seasonality, we used monthly measures for births (96 months). The calendar months were numbered sequentially for monthly measurements; for the seasonality hypothesis test, Antunes and Waldman's
24
methodological indications were used. For seasonality analysis, we used the month of the conception date; in this case, the available data were from April 2011 to March 2019. We considered the seasonal variation significant if one or more of the coefficients of the seasonal term (B3 and B5 for Seno and B2 and B4 for Cosseno) were significantly different from zero (P < .05).
14
We used STATA 15.1
26
for all statistical analyses.
Results
The sociodemographic distribution of LBs with OFC in SPS, Brazil, from 2008-2019 is summarized in Table 1, including data on total births, type of birth, and maternal and infant characteristics. We identified a higher proportion of OFC in males (57.1%), white births (65.4%), born at term (37-41 weeks: 76.5%), and weighing >2500 g, (75.8%). Among maternal characteristics, a lower prevalence in adolescent mothers was identified, but there was no significant difference after adulthood (>20 years), and in the highest proportion of cases, mothers with education between 8-11 years were identified (60.3%). The most prevalent obstetric history was single pregnancy (97.1%), cesarean delivery, (63.9%), and ≥7 prenatal consultations (73.9%).
Maternal and Infant Sociodemographic Characteristics in São Paulo State, Brazil from 2008 to 2019.
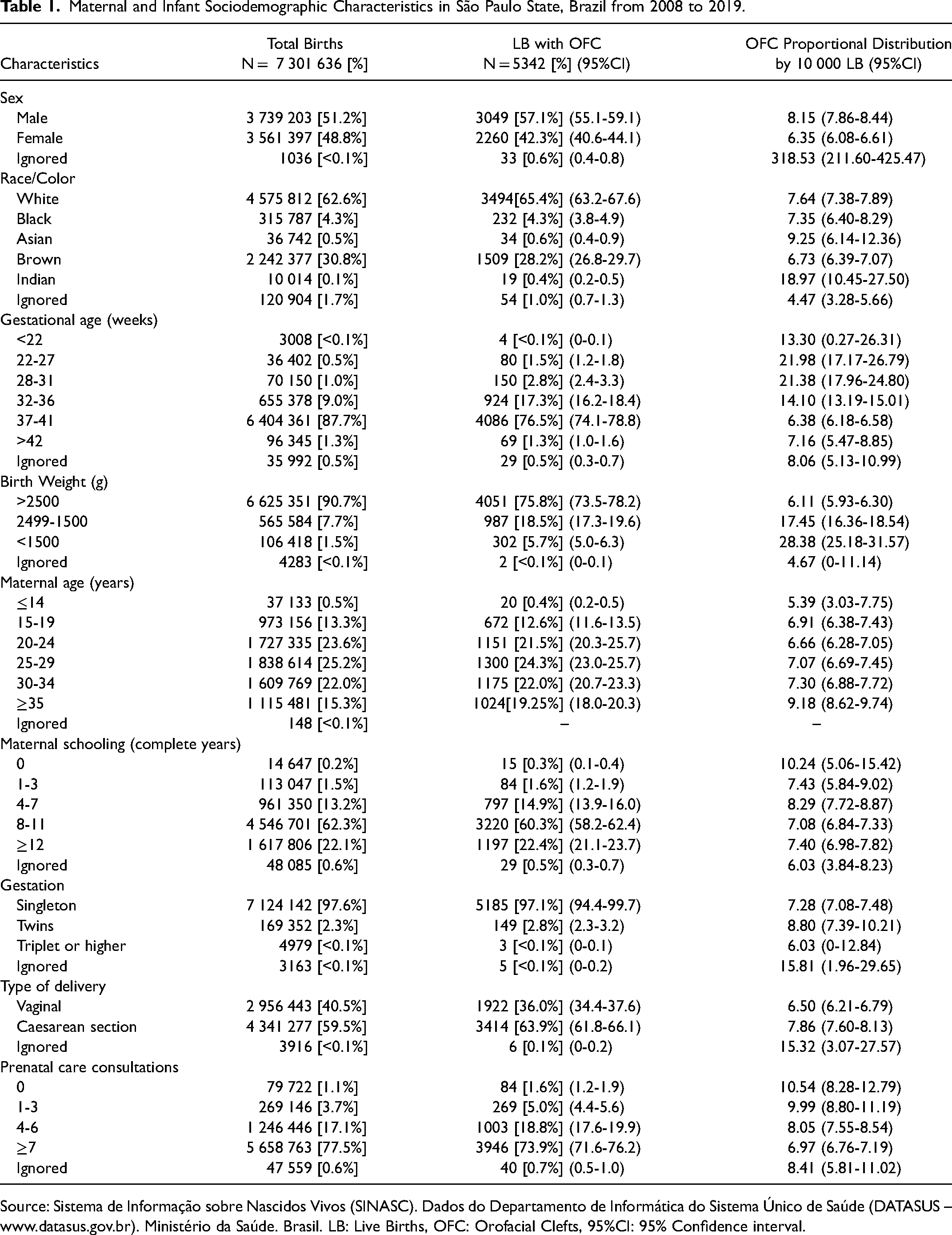
Source: Sistema de Informação sobre Nascidos Vivos (SINASC). Dados do Departamento de Informática do Sistema Único de Saúde (DATASUS – www.datasus.gov.br). Ministério da Saúde. Brasil. LB: Live Births, OFC: Orofacial Clefts, 95%CI: 95% Confidence interval.
The annual proportions and prevalence trends of OFC cases in LBs in all SPS clusters from 2008-2019 are summarized in eTable 1, and the significant results are shown in Figure 1. During this period, in SPS, both the highest number of cases (499) and the highest prevalence rate (8.3/10 000 LB) occurred in 2016. When we analyzed the district clusters, from 2008-2019, the NWE cluster showed the highest annual prevalence (2017, 11.4/10 000 LB), the CNC cluster showed the highest total prevalence (8.3/10 000 LB), the TAR cluster showed the lowest annual prevalence (2017, 3.0/10 000 LB), as well as the lowest total prevalence (5.3/10 000 LB); for the absolute number of cases, SPRM showed the highest amount (2.622), and BSMR showed the lowest number of cases (200). eFigure 1 shows the geographic distribution of OFC prevalence by clusters in São Paulo state from 2008 to 2019.
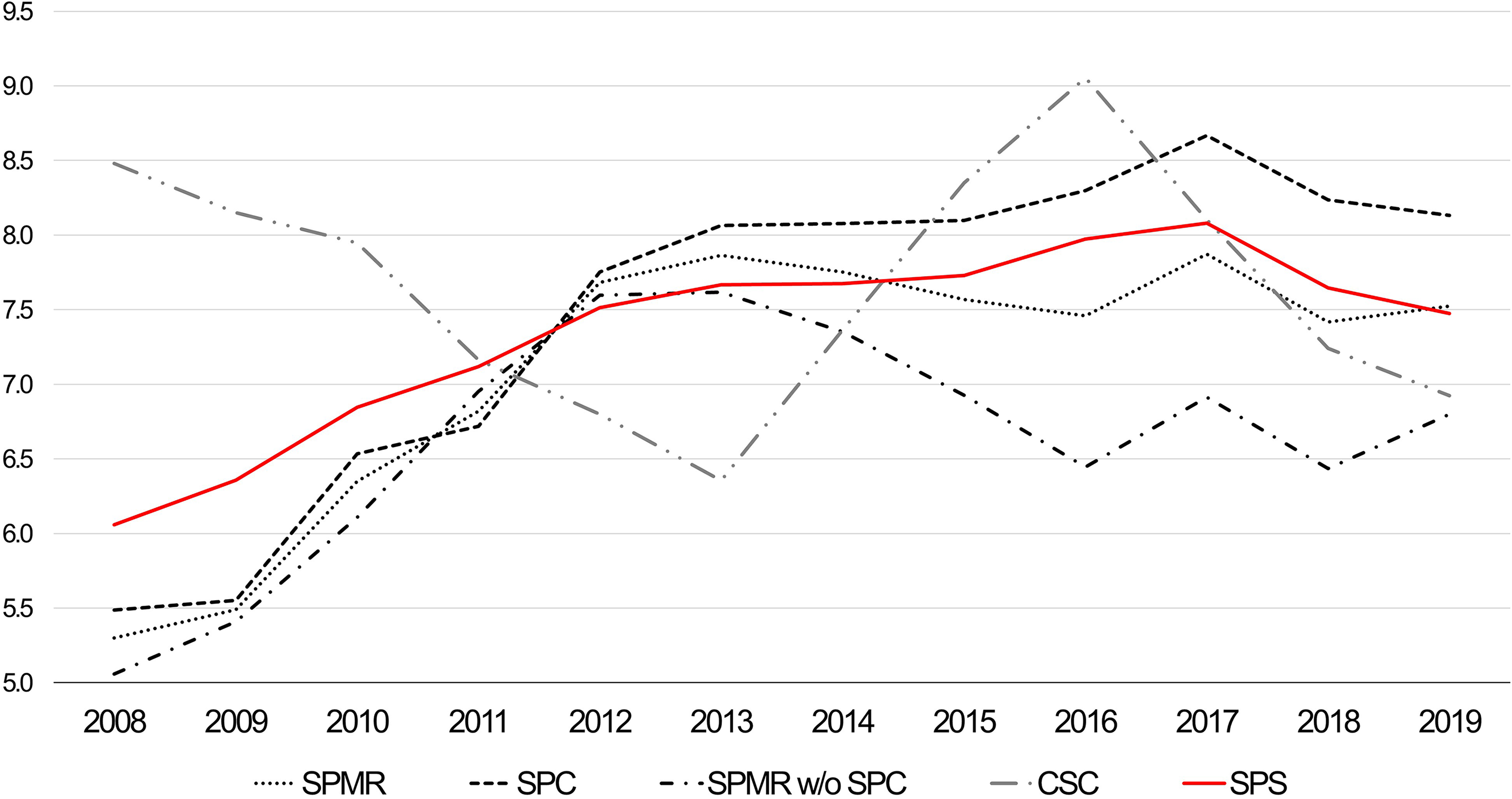
OFC prevalence trend (per 10 000 LB) by clusters in São Paulo state, Brazil from 2008 to 2019).
The OFC prevalence trend from 2008-2019, increased only in SPC, showing an annual growth rate of 0.05% (95% CI: 0.01-0.09), all other clusters showed stationary prevalence. In the first period studied (2008-2013), the prevalence trend of OFC was slightly increasing in SPMR, SPC, SPRM w/o SPC and SPS presenting, with APCs of 0.12%, 0.12%, 0.11% and 0.07%, respectively. We observed a decreasing prevalence trend in CSC, with an APC of −0.06% (95% CI: −0.09-0.02). In the second period (2014-2019), all clusters presented stationary trends (Table 2).
Prais-Winsten Regression Model for Trends in OFC Prevalence, by Clusters in São Paulo State, Brazil from 2008 to 2019.
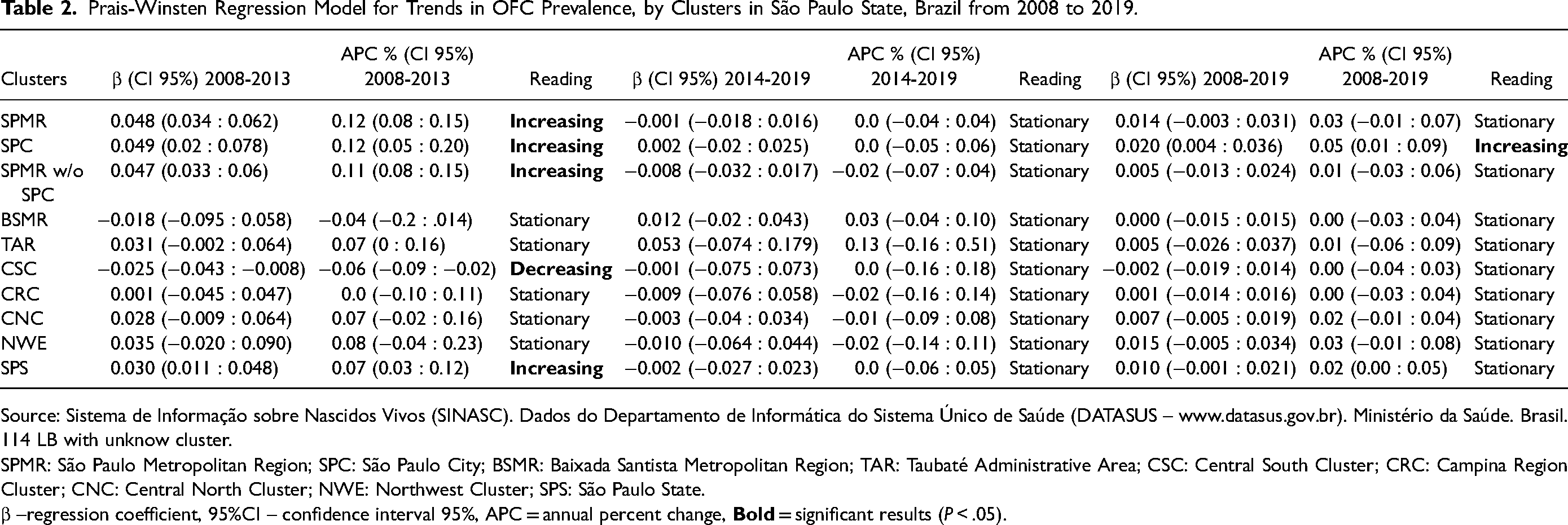
Source: Sistema de Informação sobre Nascidos Vivos (SINASC). Dados do Departamento de Informática do Sistema Único de Saúde (DATASUS – www.datasus.gov.br). Ministério da Saúde. Brasil. 114 LB with unknow cluster.
SPMR: São Paulo Metropolitan Region; SPC: São Paulo City; BSMR: Baixada Santista Metropolitan Region; TAR: Taubaté Administrative Area; CSC: Central South Cluster; CRC: Campina Region Cluster; CNC: Central North Cluster; NWE: Northwest Cluster; SPS: São Paulo State.
β –regression coefficient, 95%CI – confidence interval 95%, APC = annual percent change,
The annual OFC prevalence trends in different maternal age groups were also analyzed. The highest OFC prevalence rate occurred in the maternal age group of ≥35 years (9.2/10 000 LB) and the lowest was observed in the maternal age group of ≤14 years (5.4/10 000 LB) (eTable 2, Figure 2). From 2008-2019, the maternal age group 30-34 years was the only one that showed an increasing trend with an APC of 0.03% (95% CI: 0.01-0. 06). When separated by period, from 2008-2013, the maternal age group 15-29 years showed the highest increasing prevalence trend (APC = 0.09%; 95% CI: 0.03-0.16). From 2014-2019, the maternal age group ≥35 years showed a decreasing prevalence trend (APC = −0.02; 95% CI: −0.03-0), and all other maternal age groups showed stationary prevalence trends (Table 3).

OFC prevalence trend (per 10 000 LB) by maternal age group in São Paulo state, Brazil from 2008 to 2019.
Prais-Winsten Regression Model for Trends in OFC Prevalence, by Maternal age Group in São Paulo State, Brazil from 2008-2019.
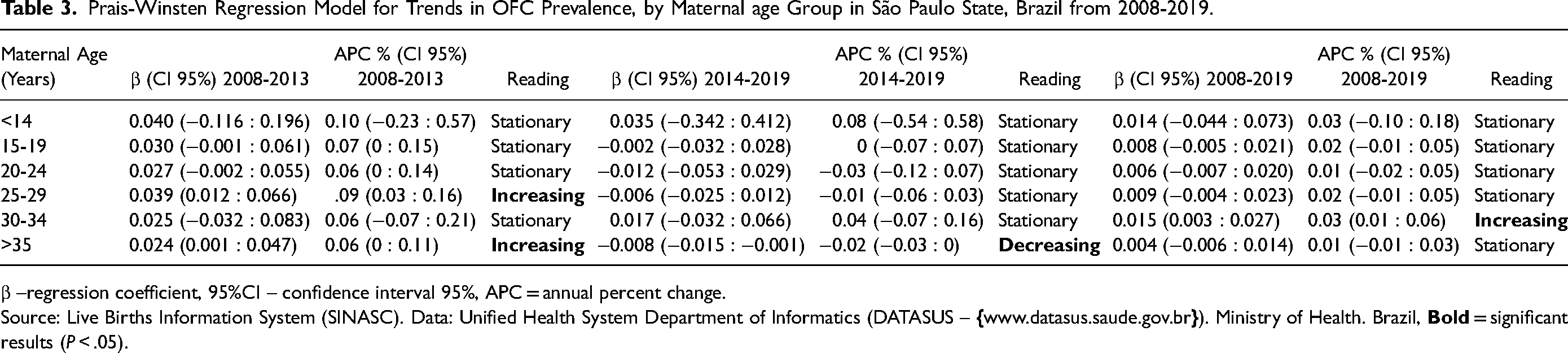
β –regression coefficient, 95%CI – confidence interval 95%, APC = annual percent change.
Source: Live Births Information System (SINASC). Data: Unified Health System Department of Informatics (DATASUS –
The OFC ICD-10 distribution and associated congenital pathologies are summarized in eTable 3. Cleft palate with cleft lip, is more frequent, 44.01% (95% CI: 42.00-46.02), compared to isolated cleft palate or isolated cleft lip. A total of 1388 cases of syndromic orofacial cleft (SOFC) were associated with 2236 other congenital pathologies. Congenital malformation of lips (IDC-10: Q380) was the most frequent (9.62%, 95% CI: 8.39 −10.84), and the various malformations found that corresponded to less than 2% (N ≤ 41) were grouped into a single set (71.02%, 95% CI: 69.14-72.90).
Figure 3 demonstrates the OFC monthly prevalence, based on the month of conception, in SPS from 2011-2019. This prevalence variation was, on average, 15.46% (95% CI: 8.08-23.36; P < .001) higher in the months in which conception occurred in the last quarter of the year (October, November, and December), corresponding to the spring months in the Southern Hemisphere, when compared to the months in which conception occurred in the second quarter of the year (April, May, June), corresponding to the fall period.
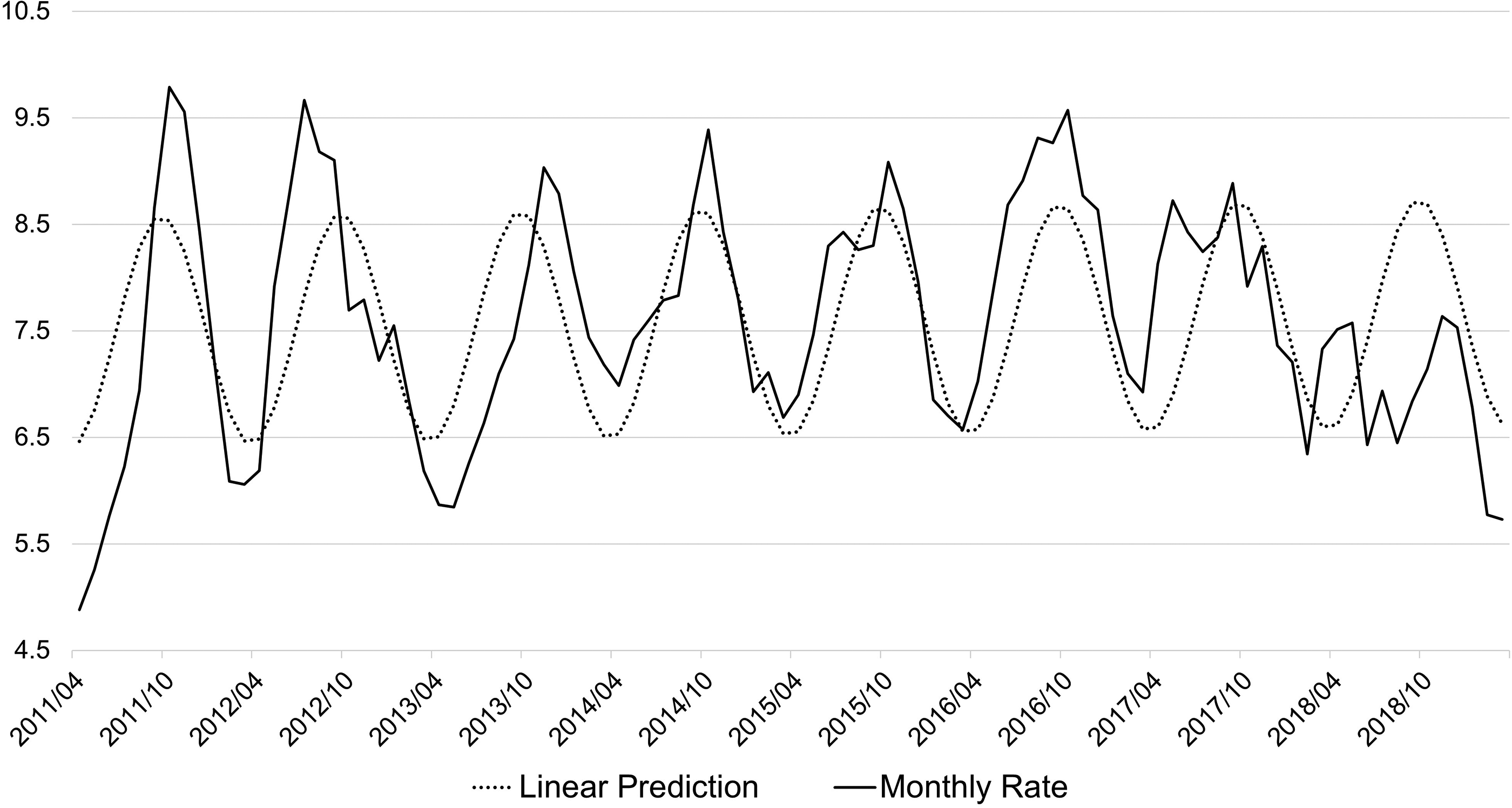
OFC monthly prevalence rate (per 10 000 LB) in São Paulo state, Brazil from 2011 to 2019.
Discussion
This population-based study describes the recent epidemiology, seasonality, and prevalence trend of LBs with OFC in SPS. Furthermore, this study adds essential information on OFC to the limited data in Brazil since this population has not been previously evaluated in detail concerning this malformation.
The strengths of this study are the large number of cases (n = 5342), the 12-year period, and information from a public, open and validated database21,22,27 used to describe and categorize the epidemiological data obtained from SPS.
Some limitations were identified inherent in recording public data, either in the data collection stages or in the quality of the information, where there are fields with ignored or unfilled content until the data transmission to the information systems in the Live Birth Declaration (LBD). Another limitation is the fact that the SINASC system only provides information up to the peripartum moment, which means that any conditions that are diagnosed later, such as submucous cleft palate or different related syndromes, may not be captured in this system. This can result in a high chance of bias, due to incomplete data, and thus impact the accuracy of health outcomes monitoring and resource allocation.
Since 1999, the Brazilian Ministry of Health has introduced a specific field in the LBD for congenital malformations and/or chromosomal abnormalities and their respective codes in the IDC-10, facilitating the search for data regarding the prevalence of congenital malformations. In Brazil, the notification of congenital anomalies, including OFC, is performed through SINASC, which extracts the information from LBD to compose its database. Congenital malformations became compulsory notification in Brazil from the implementation of federal law 13 685 in 2018, 28 being SINASC, a dedicated birth defects surveillance system.
The SINASC Procedures Manual advocates that the physician should fill the field related to the detected congenital malformation. However, Mello Jorge et al. 29 identified that 45.4% of LBDs are filled by administrative staff. Nunes et al. 30 observed that the data were extracted from the medical record, based on the physical examination performed by the pediatrician in the delivery room, without any contact with the physician to clarify any specific questions about the malformation of any LB. National studies published between 2010 and 2015 identified that there is a large amount of underreporting regarding OFC, ranging from 43.4% to 67.5%,31,32 and this may impact our results, because underreporting of cases leads to a lower prevalence. However, this is something that can be solved with a better training of the professionals who fill out the document or the creation of a sector dedicated to this filling out in hospitals and maternity hospitals.
In SPS, we identified an OFC prevalence of 7.3/10 000 LB, in which males were the most prevalent, with 3049 cases (57.1%). Studies in different regions of Brazil3,5,6,32 and several countries7,9-11,33-37 have identified a very wide prevalence, ranging from 3.6-21.8/10 000 LB. Other authors in different regions of Brazil identified results regarding sex distribution similar to ours, ranging from 56.6%-57.8% for males.1,31,38-41
We also found a predominance of the white race over the others, with 3494 cases (65.4%), followed by the brown race with 1509 cases (28.2%). In Brazil, depending on the region studied, cases are predominant in the brown race1,13,42 or the white race.5,39,43 Some authors have identified that race and ethnicity are the only demographic variables consistently associated with OFC. The highest prevalence is observed in populations of Amerindian, Asian, Caucasian, and African race/origin.5,9,44-48
The proportion of LB with low birth weight (24.2%), considered a risk factor for OFC,5,49 was lower than the proportion of LB cases with >2500 g; (75.8%). This situation of adequate birth weight is compatible with the finding of a large amount (total = 77.8%) of term pregnancies (≥37 weeks). This is due to an effective prenatal follow-up performed throughout the SPS, since 73.9% of mothers of LB with OFC had seven or more prenatal visits. Similar results regarding birth weight and gestational age have also been described by other authors.5,7,11,47 In addition, most pregnancies were single (97.1%) and were born through cesarean section(63.9%).
As identified by other authors,5,50 our results suggest that low education acts as a protective factor, since only 15.8% of the mothers have ≤7 years of education. However, low education has also been cited as a risk factor for the development of OFC.11,51 However, we believe that this information is more related to the low maternal age, rather than the complete years of schooling.
The rural region clusters of SPS (TAR, CSC, CRC, CNC, NWE) from 2008-2009, presented a 10% higher prevalence than metropolitan regions (SPMR, BSMR) (Rural: 7.7/10 000 LB x Metropolitan: 7.0/10 000 LB). The literature is not conclusive about the higher prevalence between urban and rural areas, as some authors have found higher prevalence in rural areas39,52 while others have identified it in urban areas. 11
It is known that the occurrence of OFC is related to genetic and environmental factors. Shaw & Gold identified a 3.8% increased risk for the occurrence of OFC in LB with mothers previously exposed to pesticides. 53 The meta-analysis by Romitti et al. 54 identified an increased risk (OR = 1.37) of OFC associated with pesticide exposure. However, we found that 52.83% of all cases occurred in metropolitan regions (SPMR, BSMR), which are exposed daily to pollution, mainly fine particulate matter (PM2.5) and ozone (O3), that are correlated to the occurrence of OFC.55,56
Although folic acid supplementation plays an uncertain role, 46 there are authors who have found that it represents one of the main protective factors against OFC occurrence.2,57 Since the national public health system distributes folic acid free of charge, it was expected that with the expansion and improvements of public health programs, the OFC prevalence trend would progressively decrease, but this was observed only in CSC from 2008-2013.
The stationary prevalence trend was observed by other authors,2,4,46 suggesting that genetic factors play a fundamental role in the development of OFC, 44 regardless of whether environmental risk factors are removed (maternal use of drugs and alcohol), vitamin supplementation is given, or maternal metabolism/nutrition conditions are improved (diabetes/obesity control). 58
We observed a lower prevalence in the BSMR and TAR regions, which also had the lowest number of cases overall. This may have occurred due to underreporting problems; since 2018, this congenital malformation was not considered compulsory notification, 28 and underreporting may interfere with the real prevalence of this pathology. Tosetto et al., 59 warn that many professionals do not realize the importance of notification as the main source of epidemiological surveillance. Alaguney et al. 60 relate underreporting to a lack of training and knowledge on how to perform a notification.
Maternal age is a significant topic in the occurrence of congenital malformations. We demonstrated that the maternal age range with the highest and lowest number of cases of OFC was between 25-29 years and ≤14 years, respectively. The highest prevalence of OFC occurred in the maternal age group of ≥35 years (9.2/10 000 LB) which showed an increase during the years analyzed, being 7.1/10 000 LB in 2008, and 8.3/10 000 LB in 2019. The lowest prevalence was observed in the maternal age group of ≤14 years (5.4/10 000 LB). This suggests that maternal age ≥35 years is a risk factor, and maternal age ≤14 years can be considered a protective factor for OFC occurrence.
Several authors have already associated advanced maternal age (≥35 years) as a risk factor for several chromosomal alterations as well as for OFC occurrence.61,62 This may be related to accumulative changes in gametes over the course of life because of environmental exposures or chromosomal alterations, as well as the low selectivity of the uterus for defective embryos and higher placental permeability to teratogenic agents. However, this is not a consensus in the literature, as other authors have reported divergent results.1,50
Maternal age ≤14 years is often associated with adverse outcomes, but not for the above reasons, which occur in older mothers. Young mothers also have a lower risk of metabolic disorders such as diabetes, lower likelihood of using recreational or prescription drugs, smoking, drinking alcohol excessively, and being exposed to stressful situations, compared to older mothers. These conditions have been implicated in the occurrence of OFC. 2 However, it is essential to note that teenage pregnancy still carries several risks and challenges for both the mother and the child.
Although the majority of cases were nonsyndromic (74.02%), we observed a significant amount (25.98%) of SOFC, that is, those occurring in conjunction with other congenital malformations or syndromes. In the literature, SOFCs are found to range from 4.3% to 63.4% depending on the methodology used.63,64 Like other authors,43,64,65 the most frequent anomalies and syndromes involve the skeletal, nervous, and cardiovascular systems.
Seasonality is a well-recognized phenomenon regarding the prevalence of congenital malformations, providing us with clues for etiological research. 66 Although it is still uncertain, some authors, such as us, have been able to demonstrate OFC seasonality, but these studies differ mainly in methodology, with some considering the date of conception,67-69 others considering the date of birth 67 or both. 70 The date of conception is important regarding risk factor exposure, as the first trimester of gestation is clinically relevant to OFC development. 68 Conditions that are influenced by environmental teratogen presence may show seasonal patterns of occurrence. 68
We observed seasonal variation with a 15.4% higher prevalence, when conceptions occurred in the spring period (October, November, and December – Southern Hemisphere) when compared to the fall months (April, May, and June – Southern Hemisphere). Research in different regions of the Northern Hemisphere has also identified the presence of OFC seasonality when conceptions occurred in the spring.68,69 The evidence suggests that there is a multifactorial interaction of exogenous effects (exposure time to sunlight, exposure time to ultraviolet radiation, ambient temperature, pollution, maternal malnutrition, diabetes, obesity, low folic acid intake, teratogens, smoking, drug use, infections, and physical activity) and endogenous (genetic) effects on OFC occurrence.66-70
Conclusion
The prevalence of OFC in SPS Brazil from 2008-2019 was 7.3/10 000 LB, showed a stationary trend in the period, and was higher in rural regions than in metropolitan areas. The identified risk factors were male sex, white race, maternal age ≥35 years, and residence in rural areas. The association between cleft palate and cleft lip is more frequent than in their isolated forms. Nonsyndromic OFC is more frequent than syndromic OFC, and in these, congenital cleft lip malformation (IDC-10: Q380) is the most frequently found pathology. We identified a seasonal pattern in OFC prevalence, in which conceptions occurring during the spring season are, on average, 15.4% higher than those occurring in the fall.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231181007 - Supplemental material for Epidemiologic Characteristics, Time Trend, and Seasonality of Orofacial Clefts in São Paulo State, Brazil. 2008-2019
Supplemental material, sj-docx-1-cpc-10.1177_10556656231181007 for Epidemiologic Characteristics, Time Trend, and Seasonality of Orofacial Clefts in São Paulo State, Brazil. 2008-2019 by Mauricio Giusti Calderon, Victoria Caleffi Oliveira Simoni, Brunna Gonçalves de Souza Ferreira, Adonis Florença de Moraes, Mariana Araújo Gomes, Vivian Sumie Hatakeyama and Edige Felipe de Sousa Santos in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656231181007 - Supplemental material for Epidemiologic Characteristics, Time Trend, and Seasonality of Orofacial Clefts in São Paulo State, Brazil. 2008-2019
Supplemental material, sj-docx-2-cpc-10.1177_10556656231181007 for Epidemiologic Characteristics, Time Trend, and Seasonality of Orofacial Clefts in São Paulo State, Brazil. 2008-2019 by Mauricio Giusti Calderon, Victoria Caleffi Oliveira Simoni, Brunna Gonçalves de Souza Ferreira, Adonis Florença de Moraes, Mariana Araújo Gomes, Vivian Sumie Hatakeyama and Edige Felipe de Sousa Santos in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656231181007 - Supplemental material for Epidemiologic Characteristics, Time Trend, and Seasonality of Orofacial Clefts in São Paulo State, Brazil. 2008-2019
Supplemental material, sj-docx-3-cpc-10.1177_10556656231181007 for Epidemiologic Characteristics, Time Trend, and Seasonality of Orofacial Clefts in São Paulo State, Brazil. 2008-2019 by Mauricio Giusti Calderon, Victoria Caleffi Oliveira Simoni, Brunna Gonçalves de Souza Ferreira, Adonis Florença de Moraes, Mariana Araújo Gomes, Vivian Sumie Hatakeyama and Edige Felipe de Sousa Santos in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-jpg-4-cpc-10.1177_10556656231181007 - Supplemental material for Epidemiologic Characteristics, Time Trend, and Seasonality of Orofacial Clefts in São Paulo State, Brazil. 2008-2019
Supplemental material, sj-jpg-4-cpc-10.1177_10556656231181007 for Epidemiologic Characteristics, Time Trend, and Seasonality of Orofacial Clefts in São Paulo State, Brazil. 2008-2019 by Mauricio Giusti Calderon, Victoria Caleffi Oliveira Simoni, Brunna Gonçalves de Souza Ferreira, Adonis Florença de Moraes, Mariana Araújo Gomes, Vivian Sumie Hatakeyama and Edige Felipe de Sousa Santos in The Cleft Palate Craniofacial Journal
Footnotes
Abbreviations
Contributorship Statement
Conceptualization: M.G.C. and V.C.O.S, Data curation and Investigation: V.C.O.S, B.G.S.F, A.F.M, M.A.G, and V.S.H. Methodology, Formal analysis, and Validation: M.G.C. and E.F.S.S. Writing – original draft: V.C.O.S, B.G.S.F, A.F.M, M.A.G, and V.S.H. Supervision, and Writing – review & editing: M.G.C. All authors read, reviewed, and approved the final manuscript.
Data Availability Statement
The microdata used for this study is administered by the Live Births Information System (SINASC – Sistema de Informação sobre Nascidos Vivos), using data from the Unified Health System Department of Informatics (DATASUS – Departamento de Informática do Sistema Único de Saúde), maintained by the Ministry of Health of Brazil. DATASUS provides open public access to these data for any purpose. www.datasus.saude.gov.br. ![]()
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Published Elsewhere
No.
Research Ethics
The present study involves only the description and analysis of secondary population data obtained from the general population census and birth data. No additional information that is not freely accessible was collected. In particular, no information with individual identification was obtained for this study. Ethics approval was not required.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.