
Abstract
Objective
Surgical treatment of velopharyngeal insufficiency (VPI) includes a wide array of procedures. The purpose of this study was to develop a classification for VPI procedures and to describe variations in how they are performed.
Design/participants/setting/outcomes: We completed an in-depth review of the literature to develop a preliminary schema that encompassed existing VPI procedures. Forty-one cleft surgeons from twelve hospitals across the USA and Canada reviewed the schema and either confirmed that it encompassed all VPI procedures they performed or requested additions. Two surgeons then observed the conduct of the procedures by surgeons at each hospital. Standardized reports were completed with each visit to further explore the literature, refine the schema, and delineate the common and unique aspects of each surgeon's technique.
Results
Procedures were divided into three groups: palate-based surgery; pharynx-based surgery; and augmentation. Palate-based operations included straight line mucosal incision with intravelar veloplasty, double-opposing Z-plasty, and palate lengthening with buccal myomucosal flaps. Many surgeons blended maneuvers from these three techniques, so a more descriptive schema was developed classifying the maneuvers employed on the oral mucosa, nasal mucosa, and muscle. Pharynx-based surgery included pharyngeal flap and sphincter pharyngoplasty, with variations in design for each. Augmentation procedures included palate and posterior wall augmentation.
Conclusions
A comprehensive schema for VPI procedures was developed incorporating intentional adaptations in technique. There was substantial variation amongst surgeons in how each procedure was performed. The schema may enable more specific evaluations of surgical outcomes and exploration of the mechanisms through which these procedures improve speech.
Introduction
Surgical treatment of velopharyngeal insufficiency (VPI) includes a wide array of procedures. Although these procedures have been loosely grouped in reviews and scientific reports,1–7 there is no comprehensive classification or scheme of procedures used in contemporary practice. Further complicating matters are (1) numerous variations in how procedures are executed, and (2) a lack of objective documentation of how each procedure is being carried out. What one surgeon says they are doing may not be how another surgeon envisions what is being done. Ultimately, inaccurate or imprecise procedure descriptions impede transfer of techniques among surgeons and weaken our ability to compare surgical outcomes.
Variations in performing procedures, whether intentional or unintentional, may significantly influence the effectiveness of a procedure. Although we apply scientific principles to practice, surgery is a craft and the conduct of procedures evolves from a combination of experience and awareness of what other surgeons do and why they do what they do. By documenting options within a comprehensive scheme, individual surgeons can reflect on their practice and potentially optimize their procedures. Further, researchers may be able to better understand differing outcomes among the same procedure type if they are aware of the variations in use.
A common framework and vocabulary for VPI procedures will enable surgeons to communicate more effectively and enable researchers to evaluate surgical outcomes more rigorously. The purpose of this study was to develop a schema that supports this objective, by classifying surgical procedures for VPI and the intentional variations in procedure execution.
Methods
This study was approved by Advarra Inc., the Institutional Review Board overseeing all sites involved in the VPI-OPS study.
We began by conducting a focused review of published articles, textbooks, and practice guidelines to develop surgical forms that captured described procedures and known variations (Appendix 1). The objective of the review was to explore contemporary practices, to find variations in conduct of the common procedures, and to trace those procedures to an original description that defines current techniques. We specifically sought literature with adequate details to allow surgeons to reproduce a procedure. We intentionally avoided a comprehensive historic account of procedures performed for VPI. We examined references from key publications to identify origins of procedures.
Following generation of surgical forms that captured described procedures and known variations, these forms were presented to 41 cleft surgeons at 12 centers across Canada and the United States were included. All surgeons reviewed the forms. If a surgeon performed a procedure or variation which they felt was not captured, the forms were revised to be inclusive of their technique(s).
To verify and compare the conduct of procedures, two surgeons observed procedures at each of the participating centers. During each procedure, the surgical observers took systematic notes, asked questions of the operating surgeon to confirm their understanding of the observed technique, and produced a standardized surgical report for each observed procedure. Both surgeons observed procedures at the first two sites. Following each of those visits, notes were compared, and discrepancies were rectified. The surgical observers then independently observed procedures at the remaining sites.
The procedures and variations identified during these site visits were used to further explore and revisit the literature, and subsequently to generate a comprehensive schema. This schema was then reviewed and edited by each of the cleft surgeons participating in VPI-OPS to ensure their surgical techniques were fully captured and appropriately attributed. The final schema and terminology were reviewed and approved by all participating surgeons. The results are herein presented.
Results
Based upon review, site visits, and consensus discussions, procedures following prior palatoplasty could be divided into palate-based surgery, pharynx-based surgery, soft tissue augmentation, and combinations (Figure 1).
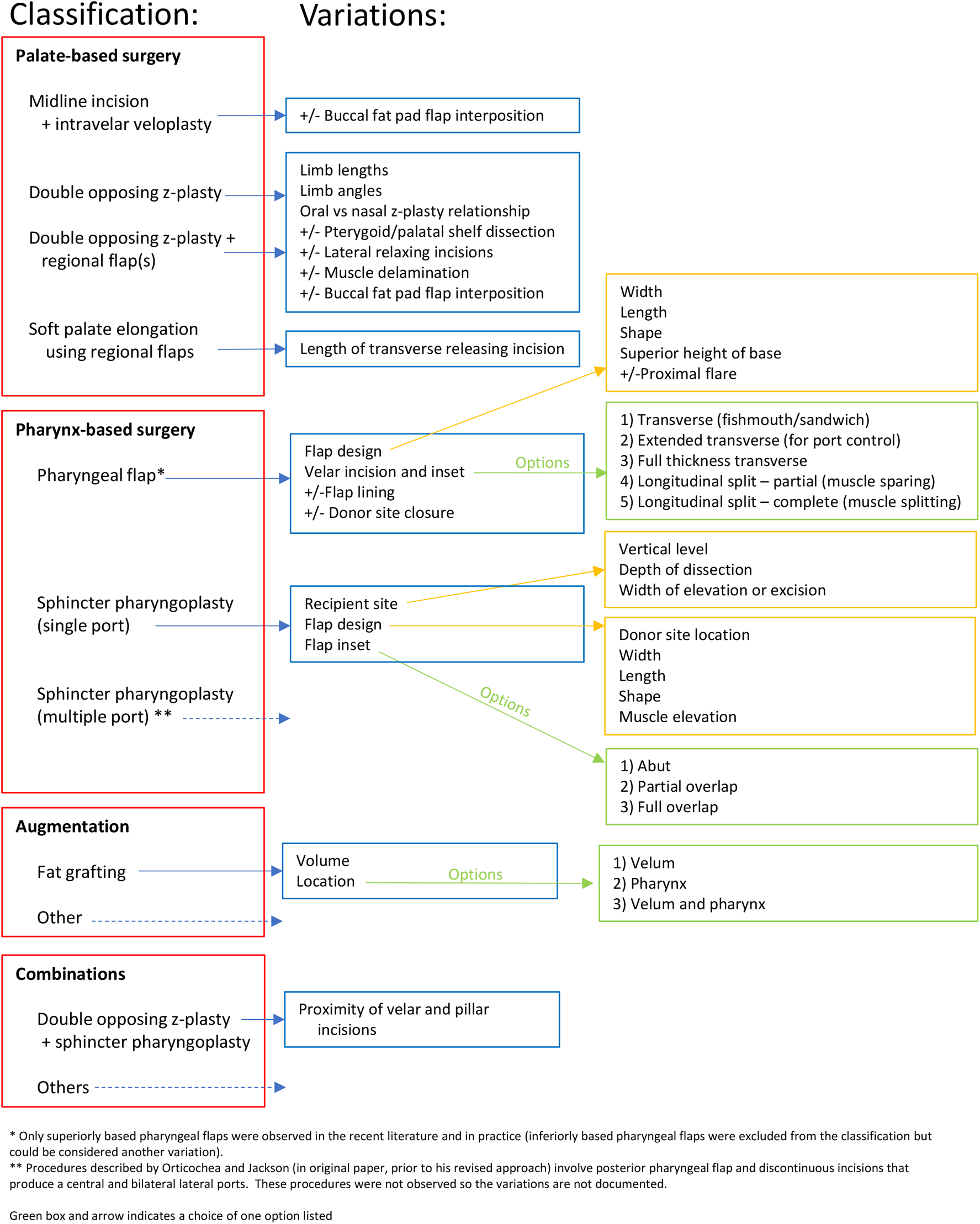
Schema of surgical options for Velopharyngeal insufficiency following cleft palate repair. Classification and intentional variations are outlined.
PALATE-BASED SURGERY
Midline incision with revision intravelar veloplasty
Known as “re-repair”,8–10 the procedure involves a midline incision through oral mucosa, circumferential dissection of levator veli palatini muscles, and retropositioning with repair to form a muscular sling along the posterior extent of the soft palate (see Figure 2). This technique was championed by Sommerlad. 8 Variations in the degree of muscle dissection and mobilization could exist and may be classified according to the scheme outlined by Andrades, 11 however, Sommerlad and Grant have emphasized “radical” or Type 48,9 dissection and that is what was observed. Other variations could include abutting versus overlapping muscle repair and the use of high magnification such as an operating microscope.
Double opposing z-plasty
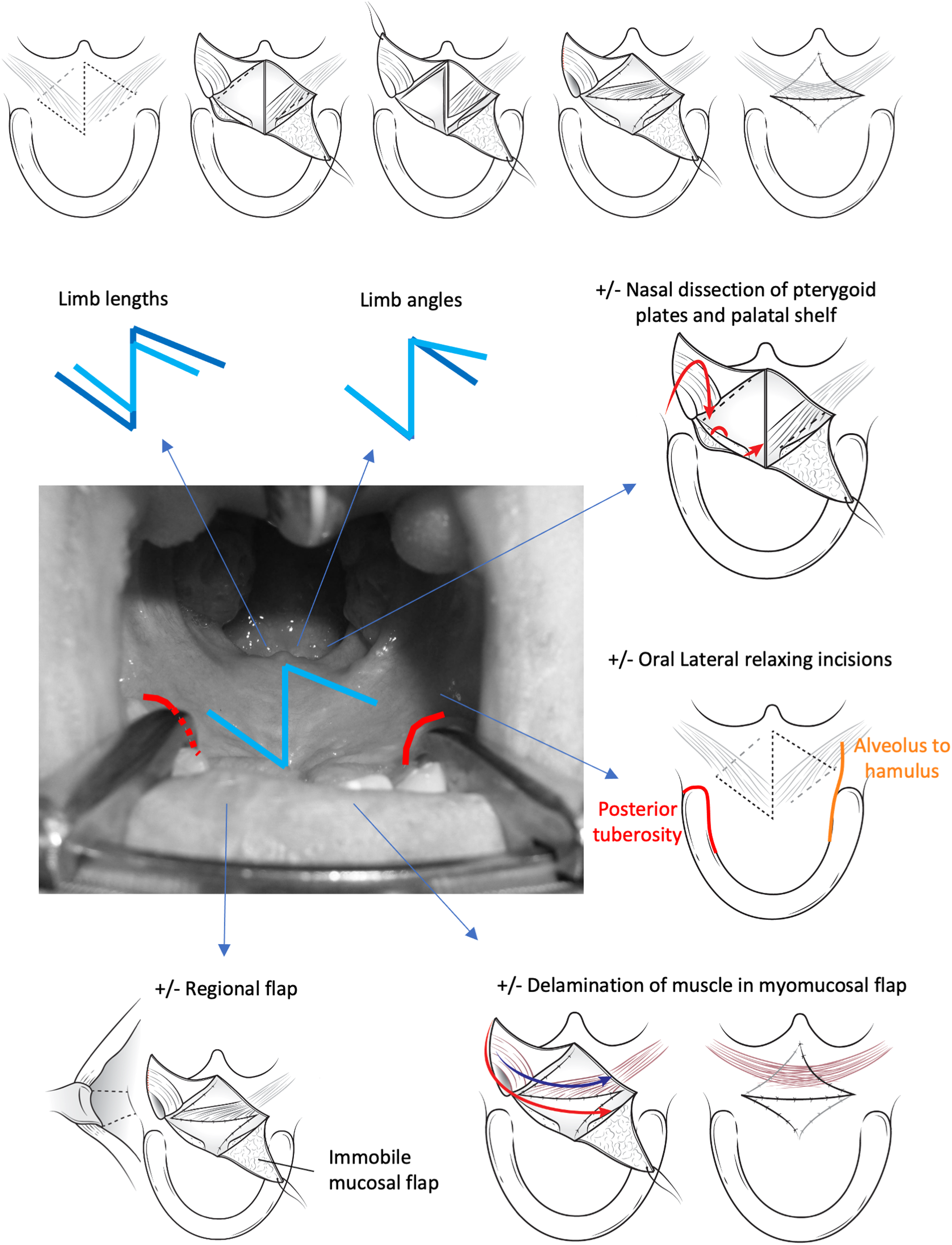
Double opposing z-plasty for VPI12–23 is also known as “secondary Furlow”. It involves a full-thickness midline incision through the oral and nasal mucosa, a releasing incision of the oral mucosa along the posterior border of the hard palate on one side, and a parallel incision of the oral mucosa along the posterior region of the soft palate on the other side (Figure 3). The posteriorly based flap is elevated as a myomucosal flap (the velar muscles are detached from the hard palate and elevated off the nasal mucosa) and the anteriorly based flap is elevated as a mucosal flap. An opposing z-plasty is designed on the nasal side with the posteriorly based myomucosal flap incorporating the velar muscles and the anteriorly based flap involving mucosa only. Flap transposition re-orients the levator veli palatini muscle more posteriorly and elongates the soft palate along the longitudinal axis.
Furlow originally reported the approach for unrepaired cleft palate.
24
His subsequent description included abundant technical details
25
and the application as a secondary procedure followed.6–15 Although the descriptions of the procedure were consistent in the literature,12–21 numerous variations were observed amongst surgeons:
(A) Incisions
Design: Some surgeons planned z-plasties within the available tissues using empiric angles and measured lengths. Other surgeons planned incisions based upon skeletal anatomy including the hamulus for oral side incisions and eustachian tube for nasal side incisions. The hamulus can be palpated as a bony prominence posterior to the alveolar process. The eustachian tube can be visualized posterior to the medial pterygoid plate after the midline nasal mucosa has been split. Limb lengths: Some surgeons designed shorter limbs, within the available tissues, while others designed longer limbs (Figure 3). The rationale for shorter limbs was to keep incisions within soft regions of the velum to take advantage of tissue pliability. The rationale for longer limbs, that could encroach upon some of the hard palate mucosa, was to achieve greater flap transposition and potentially maximize velar length. Limb angles: Some surgeons designed limbs with more acute angles, using empiric angles or landmarks; others designed limbs with more obtuse angles, to maximize transposition and potentially velar length (Figure 3). Some surgeons designed asymmetric limbs with anterior incisions made more acute, to allow easier transposition, and posterior incisions made more obtuse, to maximize velar elongation. Relationship of opposing z-plasties: Some surgeons designed z-plasties that were opposing but equal on both oral and nasal sides. Some surgeons made the nasal side z-plasty smaller to facilitate closure. Some surgeons intentionally offset the oral and nasal z-plasties so that the oral z-plasty was further anterior and the nasal z-plasty was further posterior; this was done so that the lines of closure on each surface would not overlap. (B) Mobilization
Oral lateral incisions: Some surgeons included relaxing incisions along the junction of gingiva and palatal mucosa to reduce tension of flap inset and potentially allow for greater tissue transposition and velar elongation (Figure 3). The posterior design of the relaxing incisions varied: they could extend directly posterior into the soft palate or curve around the posterior alveolar ridge to avoid narrowing the base of the triangular flaps. Nasal pterygoid plate/palatal shelf dissection: Some surgeons included turn-down of the medial pterygoid plate mucoperiosteum (Figure 3)26–28 Starting caudal to the tensor aponeurosis, subperiosteal dissection off the medial surface of the medial pterygoid plate allows the lining to be turned down in a “draw-bridge” manner. The dissection plane can be carried anteriorly to raise nasal mucoperiosteum off the palatal shelves26–28 The additional mobility potentially alleviates tension at inset and allows for a greater transposition (ie, with longer incision limbs). Muscle dissection: In addition to elevation and transposition of the myomucosal flaps, further dissection of the distal levator muscle from mucosa of the myomucosal flap was undertaken by some surgeons (Figure 3). The delamination would allow the muscle to inset further posterior into the “levator tunnel” or the proximal belly of the contralateral levator muscle, while still allowing for the anterior vector of flap movement with inset into the mucosal defect. (C) Closure
A buccal fat pad flap was sometimes added as a middle lamella, either to provide vascularity if there were concerns with the closure or to provide space-occupying soft tissue to reduce fibrosis.
Double Opposing z-Plasty with Regional Flap(s)
When performing double opposing z-plasty, additional regional flaps were added to either the oral or nasal closure if the native tissue was fibrosed or did not transpose easily. Regional flaps included facial artery myomucosal flaps (FAMM) or buccal myomucosal flaps. Use of these flaps29,30 and of buccal fat pad flaps
31
for lining have also recently been reported.
Revision intravelar veloplasty. Through a midline incision, the velar muscles are dissected circumferentially and re-repaired in a transverse orientation thereby providing more sling. Double-opposing z-plasty. Z-plasties on the oral and nasal surfaces of the velum are designed in an opposing manner. Posteriorly based flaps include muscle with mucosa so that transposition produces a more posterior position and orientation. Variations in procedures included limb length, limb angles, oral lateral relaxing incision, nasal pterygoid and palatal elevation, partial delamination of muscle, and the addition of regional tissues.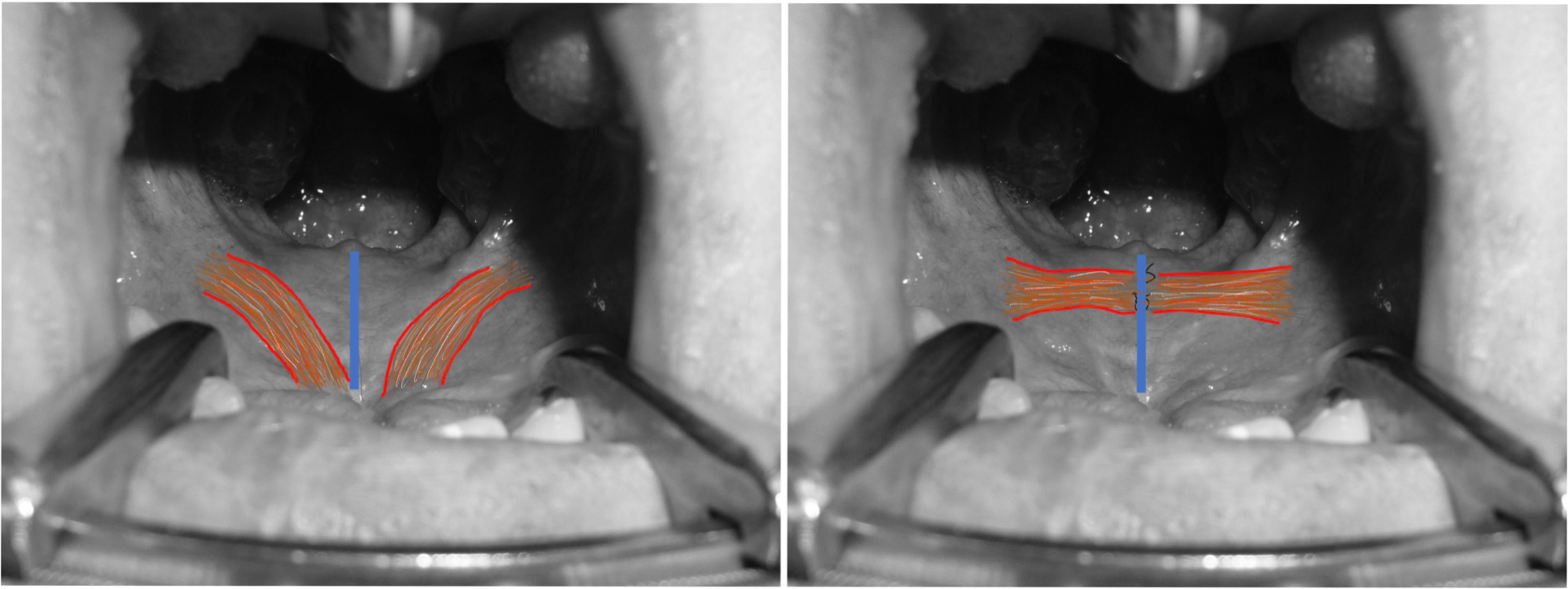
Soft Palate Elongation Using Regional Flaps
Known as “palatal lengthening”,32–36 a transverse incision several millimeters posterior to the hard palate (Figure 4) is taken through the full thickness of the velum so that the velum can be “set-back”. With the velum in a more posterior position, the defect is filled with bilateral buccal myomucosal flaps that are inset in an overlapping fashion to resurface both the nasal and oral aspects of the defect. The procedures observed during this study were similar to that described by Hill, 32 and later popularized by Mann 34 except that the transverse width of the releasing incision varied. The incision was limited to the central two-thirds of the palate by some surgeons, while others took the incisions laterally, below and beyond the alveolus, to facilitate velar release and flap inset. In addition, some surgeons also performed dissection and overlapping repair of the levator muscle, often with midline incision posterior to the releasing transverse incision. 37
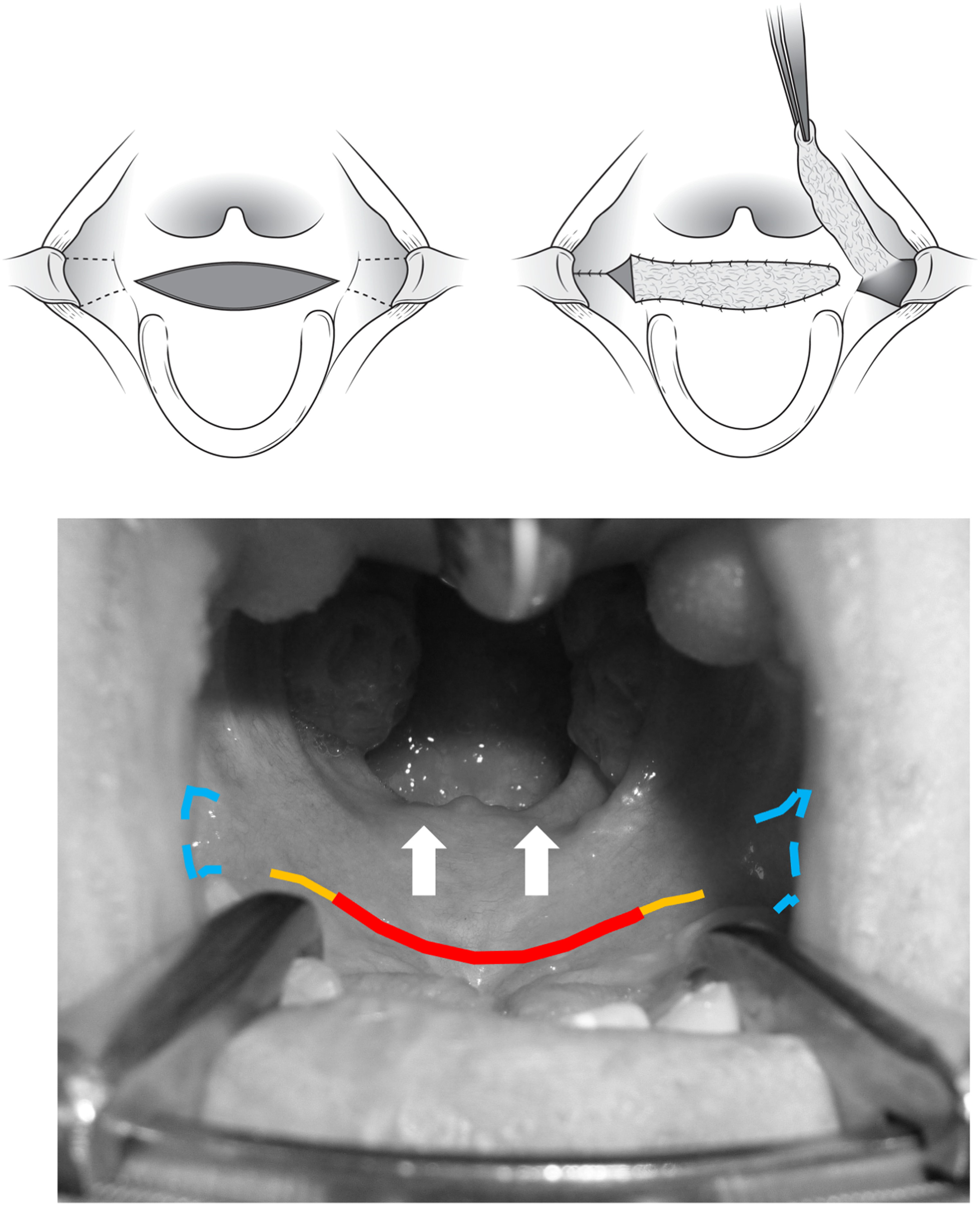
Soft palate elongation with regional flaps. An incision is made posterior to the hard palate to allow the velum to “set back”. The defect is filled by regional flaps to fill both the oral and nasal defects. Variations in the length of the opening incision were observed.
PHARYNX-BASED SURGERY
Pharyngeal flap
Only superiorly based pharyngeal flaps were observed in the recent literature and in practice. The technique by Hogan
38
was therefore selected as a reference for the many variations.
Flap design (Figure 5)
Width: Some surgeons varied flap width according to the perceived need (clinical, endoscopy, imaging), whereas other surgeons designed the flap with a standard width for all patients. Length: Longer flaps were preferred by some surgeons to provide a greater surface area of adhesion or “reach” for inset. Shorter flaps were preferred by other surgeons to produce greater posteriorly directed tension on the velum upon inset. Shape: Surgeons designed the flap either as a rectangle or with a distal triangular taper. The rectangular flap was chosen to match the desired surface of inset into the velum, while the distal triangular taper shape was chosen to facilitate donor site closure. Superior height of base: Most surgeons attempted to make the base as superior as possible. Some surgeons made the base of the flap at the adenoid pad whereas others specified the base of the flap be at C1 or the level of attempted velar contact with the posterior pharyngeal wall. Presence of adenoid tissue and limited visualization were cited as limiting factors, although some surgeons described the incorporation of the adenoid pad, when small, into the flap. Other surgeons consistently performed adenoidectomy (with or without tonsillectomy) prior to pharyngeal flap, to avoid interference in the height of the superior-most flap base design and to reduce variations of speech from adenoid hypertrophy in response to infections or with allergies. Lateral flare of base: Some surgeons designed the flap base as a straight-line projection of the more caudal portion of the flap. Others designed it so that it flared laterally to widen the base with the intention of improving blood supply and controlling the size of the lateral ports. When designing the flare of the base, the eustachian tubes were visualized and incisions were directed toward these orifices. Velar incision and dissection (Figure 5)
Transverse (also known as “fish mouth” or “sandwich”): An incision on the nasal surface of the velum could match the insertion end of the desired flap or could be extended into the posterior tonsillar pillar to provide a further surface of inset for “port control”. Dissection would then be taken through the substance of the soft palate to delaminate and create a pocket to inset the pharyngeal flap. Some surgeons dissected this pocket several millimeters anteriorly from the posterior free margin of the velum, while other surgeons dissected the up to the posterior edge of the hard palate. Other variants included: a transverse nasal incision along the posterior velum combined with a more anterior transverse oral incision, and an intervening tunnel to facilitate inset and adhesion;
39
or a transverse incision through the full thickness of the soft palate just posterior to the hard palate with no tunneling or dissection within the soft palate,
40
with the intention of producing a superior oblique vector of pull from the flap on the velum. Longitudinal velar split: A midline incision of the velum could be made, either in the posterior portion of the velum (to preserve the velar muscles) or through the entire soft palate, including all velar muscles (to provide maximal exposure). Once the velum was split longitudinally, back-cuts could be made in the nasal lining to provide posteriorly based nasal mucosal lining flaps for the pharyngeal flap pedicle with the intention of reducing contraction of the pharyngeal flap. Donor site
The posterior pharynx donor site was most often closed with sutures. The superior extent of closure varied amongst surgeons. A higher level of closure was intended to support the vertical position of the pharyngeal flap base. A lower level of closure was chosen by some surgeons to avoid excessive tension and potential construction of the airway.
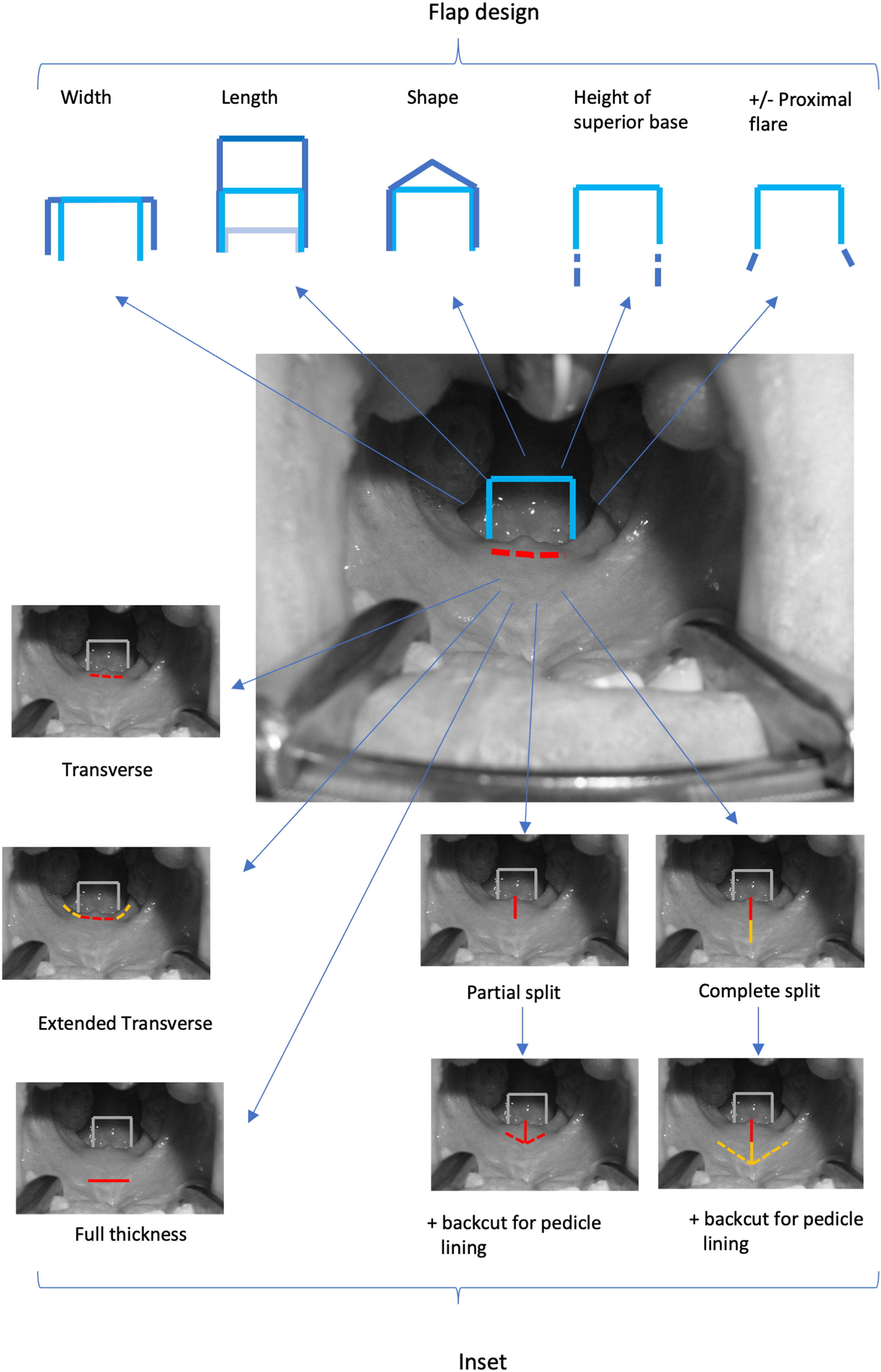
Posteriorly based pharyngeal flap. A flap of posterior pharynx is inset into the velum. Variations in flap design include width, length, shape, height of the superior base, and use of a proximal flare. Variations in recipient include the orientation of incision (transverse split versus longitudinal split), the extent of these incisions, and the use of counter incisions to produce flaps to line the raw surface of the pharyngeal flap.
Sphincter Pharyngoplasty
Descriptions of pharyngoplasty varied widely in the literature. Common to all procedures was the elevation of bilateral superiorly based flaps that contain mucosa and the palatopharyngeus muscle. These flaps are transposed to a horizontal inset along the posterior pharyngeal wall. The description by Hynes 41 involves continuity of the vertical and horizontal incisions so that the pharyngeal circumference is reduced. The flaps are inset along the width of the posterior pharynx at the level of the C2 vertebral axis, thereby potentially augmenting or producing a fullness along the posterior pharynx. This facilitates velopharyngeal closure when the velum moves to contact transferred tissue of the pharyngoplasty. Although the procedure was originally described in the setting of an unrepaired cleft palate 42 Hynes later described it as a procedure following palatoplasty. 43 Variations described by Orticochea 44 and Jackson 45 involved the use an inferiorly based 44 and superiorly based 45 posterior pharyngeal flap, respectively, that receives the lateral flaps and is discontinuous with the incisions used to raise the lateral flaps. These two variations lead to central and bilateral lateral ports. The Orticochea flaps are dissected and inset further inferiorly in the oropharynx (“no further than ½ the height of the tonsils”) with the intention of preserving innervation of muscle. 44 Jackson subsequently modified his approach to inset the flaps further superior in the nasopharynx and to make the incisions for flap elevation and inset continuous with one another, 46 like that described by Hynes.
There existed much disagreement among surgeons on the appropriate attribution of their pharyngoplasty technique. Hynes, Jackson, and Orticochea evolved their techniques and published multiple descriptions. Other surgeons further modified these techniques without renaming them, making it difficult to assign specific procedures to individual surgeons. To avoid the confusion created by this, we describe the anatomy of what is done without attempting to attribute techniques to specific publications.
All of the observed procedures involved contiguous incisions that produced a single central port. (Figure 6):
Design and flap elevation
Vertical level of the recipient site on the posterior pharyngeal wall: Surgeons tended to place the incision as superior as possible but limitations of visualization, presence of adenoid tissue, and prior adenoidectomy influenced the design and level. Some surgeons positioned the posterior wall incision at the arch of the C2 atlas, while others sought to place the incision at the anticipated site of velar contact as estimated on pre-operative imaging. Although not performed by any of the study surgeons, the soft palate can be split to facilitate access for inset. Flap donor location: The posterior tonsillar pillar is defined by the palatopharyngeus as fibers connect the posterior velum to the infero-lateral pharynx. The lateral pharyngeal recess intervenes between the pillar and posterior pharyngeal wall. Incisions for flaps could involve (Figure 6):
The anterior and posterior surfaces of the posterior tonsillar pillar The edge of the posterior tonsillar pillar and the lateral pharyngeal recess The posterior surface of the tonsillar pillar (sparing the free edge of the mucosa of the pillar) and further posterior along the lateral pharyngeal recess Flap width and length: These were varied by surgeon preference to match the available surgical anatomy and to provide adequate tissues for the desired reconstruction. Flap shape: The distal end of the flaps could be “squared off” or tapered (to facilitate donor closure). A “club shaped” flap (distal portion widened) was used by some surgeons to augment the contralateral side in the case of an asymmetric closure pattern Muscles elevated: While incorporation of the palatopharyngeus muscle in the flaps was common to all surgeons, the intended inclusion of superior constrictor and salpingopharyngeus was variable. Given the limited exposure, we could not confirm or refute muscles elevated. Recipient site and inset
Depth of the recipient site: The transverse limb on the posterior pharyngeal wall could be incised directly so that tissues cephalic and caudal to the incision could be raised. Alternatively, a strip of mucosa along the posterior wall could be excised to produce a site of adhesion, with the intention to avoid descent of the flaps once incised. In both scenarios, the incisions/excisions could include mucosa only or muscle and mucosa. Width of the recipient site: Attempts were sometimes made to control the 3-dimensional configuration of tissues via the width of the transverse limb. When the raw surface of this limb was made narrow, more of a protuberant “shelf” was immediately produced. When the width of the raw surface was wider, a smoother “bump” was produced. Flap inset: Once transposed, the flaps could be inset abutting, partially overlapping, or fully overlapping. The intention of the latter was to produce a smaller central port. Donor site
All surgeons closed donor sites, but the superior extent of closure varied. When the flap base was designed wide or superiorly (toward the torus tubarius) closure required greater movement of the lateral pharyngeal wall and closure was tailored to the desired tension (sometimes leaving areas to heal by secondary intention).
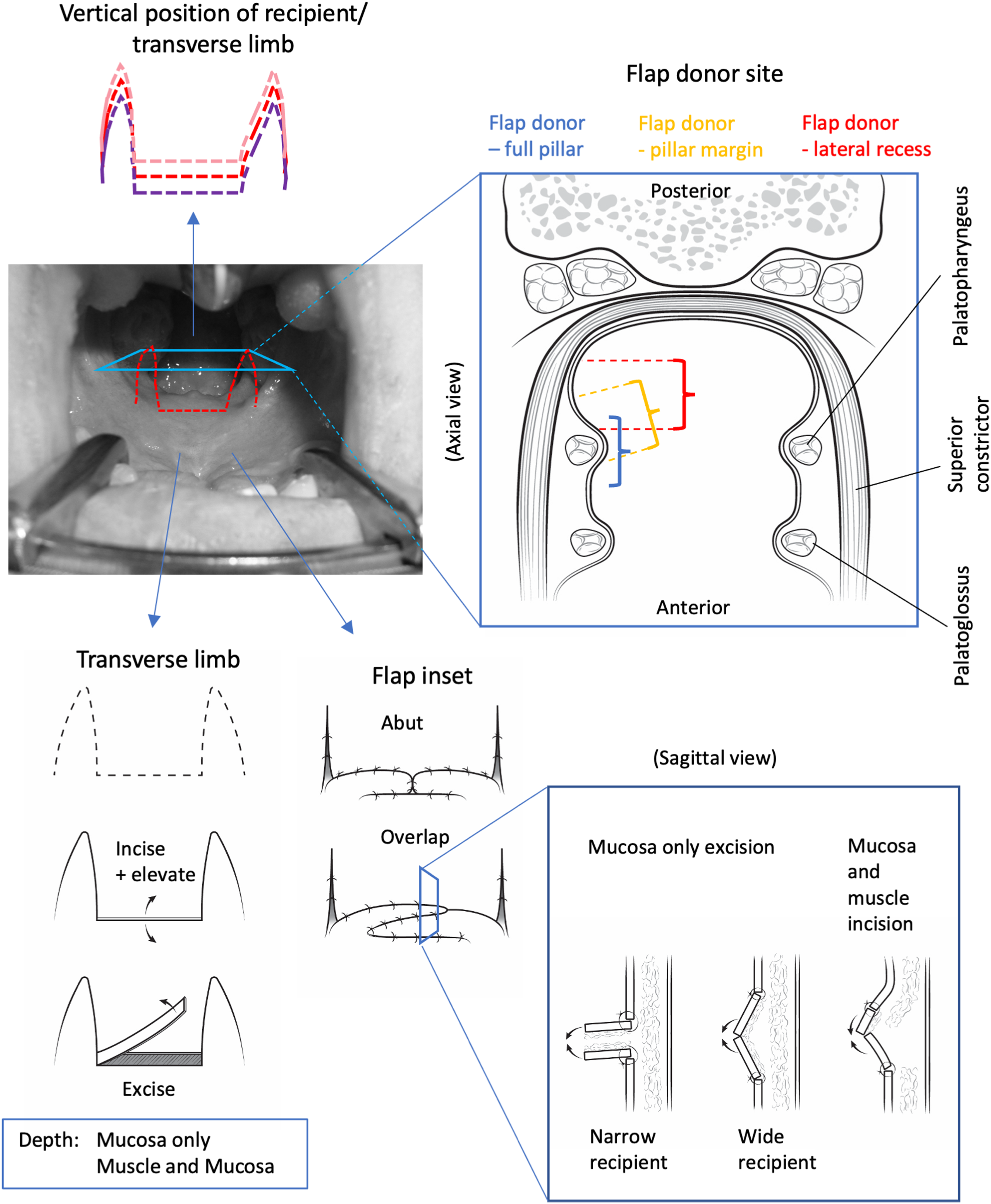
Sphincter pharyngoplasty. Bilateral superiorly based flaps are transposed and inset into the posterior pharynx. Variations include flap length and width, vertical position of transverse limb, the flap donor sites, the recipient site incision vs excision, and the relative inset of flaps into the recipient site.
SOFT TISSUE AUGMENTATION
Augmentation of velopharyngeal soft tissue to facilitate velopharyngeal closure has been described using microfat grafting. Sites can include the soft palate, posterior and lateral pharyngeal walls, or both.47,48 Although favorable results in selected scenarios have been reported, there have been concerns raised over the long-term safety of this approach 47 and alterations of grafted fat volume that vary with a patient's overall body habitus. We did not observe any surgeons performing injections; however, the option was acknowledged as a consideration. Although injection or insertion of other materials have been described, none of the surgeons endorsed current use of them.
COMBINATIONS
Combined double opposing z-plasty palatoplasty with sphincter pharyngoplasty has been described49,50 and was observed in use. The observed procedures varied little from that described in the literature. Variations may exist in the proximity of the nasal mucosa incisions of the palatoplasty with the vertical incisions of the sphincter pharyngoplasty flaps for transposition given that those incisions converge. When placed too close together, the incisions could limit flap perfusion. When placed too far apart, the vertical level of the sphincter could be too low.
One variation of combined double opposing z-plasty with sphincter pharyngoplasty reported in the literature involved tunnelling de-mucosalized flaps into the posterior pharynx where incisions would otherwise be placed with a more conventional sphincter pharyngoplasty. 51
Several additional surgical combinations are described in the literature, although none were observed on site visits or noted by the surgeons involved. Reported combination procedures include: Revision intravelar veloplasty combined with sphincter pharyngoplasty; 52 double opposing z-plasty combined with pharyngeal flap;53,54 and V-Y advancement or “push-back” palatoplasty with pharyngeal flap.55–57
Discussions
Management of VPI involves numerous variations in evaluation and management, with limited consensus. 58 There is no standard of practice for cleft centers and most surgeons work in relative isolation. Given the relative infrequency of VPI, especially at centers where favorable outcomes of primary palatoplasty are achieved, cleft surgeons may have limited experience treating VPI. The creation of a schema that encompasses the procedures performed in contemporary practice, along with intentional variations in how these procedures are executed, provides surgeons an opportunity to compare their technique(s) to those used by other surgeons. Understanding what other surgeons are doing and how they are performing procedures is valuable for the evolution of surgical craft.
The proposed classification follows the grouping of procedures used in previous reviews1–7 We have formalized these groupings and outlined a logical sequence in which each can be varied. For example, secondary palatoplasty ranges from revision of intravelar veloplasty to double opposing z-plasty that includes regional flaps. Depending upon the scope and context of study, those procedures may be grouped together or could be examined separately.
While researchers may question the relevance of the many variations, they may, in part, explain some of the inconsistencies in treatment results and account for some of the “error” in comparing procedures. 59 Awareness of what those variations are can help to better control studies or explain discrepancies that arise. Studying the anatomic impacts of these variations could also improve our understanding of how surgical interventions change speech resonance.
Terminology in the literature describing procedures to treat VPI following cleft palate repair was confusing. For example, the term “pharyngoplasty” is not only used to describe procedures for VPI, but also for procedures that alter the pharynx and are used to treat such conditions as obstructive sleep apnea. Even within the scope of cleft care, “pharyngoplasty” sometimes includes pharyngeal flap procedures and sometimes does not. Some argue that the term pharyngoplasty should not be applied to pharyngeal flap given that the procedure may produce alterations of the velum. We therefore specifically used the descriptive term “pharynx-based surgery” to include procedures performed in the region of the pharynx.
Another source of confusion is the use of eponyms to describe procedures. While some surgeons have described procedures in the literature and documented subsequent modifications, others have made undocumented modifications, or their procedures have been modified by other surgeons. The proposed schema therefore uses nomenclature that is descriptive of the procedures and avoids eponyms.
While the initial descriptions of procedures were published decades ago, surgical evolutions continue, often without documentation. Surgical procedures in the velopharyngeal region are particularly difficult to document because of the limited access and visualization for image capture combined with the 3-dimensional nature of the anatomy. Landmarks, regions, and anatomic subunits are difficult to define, and alterations achieved surgically are difficult to document. In addition, most technical descriptions in the literature involve a single surgeon's approach narrated using their personal account. This study attempted to overcome many of these limitations by conducting in-person site visits and surgical observations. This enabled us to gain unique insights on how surgeons were executing procedures, where they varied their technique from what is described in the literature, and where their approach was similar to or different from other surgeons. These insights gained through direct observation enabled us to expand the current literature 4 by detailing the many technical variations used by a diverse group of surgeons across Canada and the United States.
While the surgical methods to treat VPI vary considerably in their intended mechanisms of action, each has been reported to be effective in normalizing speech and associated with variable failure rates. Multiple mechanisms have been hypothesized to explain how these procedures improve speech. Palate-based procedures correct the levator muscle configuration to make it more effective in elevation of the palate, and some of these procedures provide length to the velum to facilitate velopharyngeal closure. Pharyngeal-based procedures reduce the pharyngeal aperture through closure or contracture of flap donor sites and obliterate either the lateral recesses or the central region of the velopharynx. The mechanisms by which palatal and pharyngeal procedures improve speech may also overlap; for example, changes in lateral pharyngeal wall motion have been described following both secondary palatoplasty and pharyngeal flap . 57 The convergence of palate-based and pharynx-based procedures is highlighted by the convergence of palatoplasty and sphincter incisions along the posterior velum when combined double opposing z-plasty and sphincter pharyngoplasty procedures are undertaken. Given the common mechanism, there may be a continuum in the mechanism between procedures that provides benefit. In addition, there may be variations in how a given procedure alters speech depending upon how the procedure is carried out. For example, some methods of pharyngeal flap inset could produce significant alterations of the velum and pharynx whereas others may only alter the pharynx. Further anatomic studies, potentially with the use of dynamic MRI, may provide insights on each procedure's mechanism of action. In turn, those could help to further modify the schema.
Limitations
This study was a qualitative exploration of both the literature and clinical practice. No attempt was made to describe the prevalence of individual procedure utilization. Moreover, no information was collected on effectiveness of the procedures described. These questions remain to be explored in future investigations.
Although our audit of surgical procedures for VPI is unique, the schema may not reflect practices elsewhere. We sought to describe current practice in Canada and the United States, and thus no attempt was made to review the non-English literature or to observe surgeons from other countries. Nonetheless, in a survey of surgical practices in the UK and Ireland similar procedures were reported. 4 The schema presented may be improved by future work that intentionally includes a distinctly different population or different sampling methods.
While the scheme does not include the wider array of historical practices, our intention was to reflect contemporary procedures. Some of the procedures identified during the literature review were not employed by surgeons in our study. These procedures, such as the Orticochea pharyngoplasty (which we have called a multi-port pharyngoplasty), have been included in the schema but it was not possible to describe their variations in the present study. This is indicated by the dashed arrows in Figure 1.
Finally, the mechanism through which pharygoplasties described by Hynes improve speech is debated. While some believe the transposed muscle produce a dynamic sphincter, others believe that the tissue serves to augment the posterior pharyngeal wall. We have followed systematic reviews 6 and the general convention of referring to the procedure as “sphincter pharyngoplasty.” On review of descriptions by Hynes 43 and Jackson's revised procedure, 46 their intention was to produce a sphincter. Ultimately, as we learn more from post-operative anatomic studies, we will be able to adjust the schema as needed.
Future Directions
This study was conducted as part of a larger project, the Velopharyngeal Insufficiency Outcomes Prediction Study (VPI-OPS) which aims to compare the effectiveness of different surgical treatments of VPI. The schema presented here will be used to categorize the procedures performed on VPI-OPS participants, and to guide exploration of any variations in outcomes among surgeons.
Conclusions
A comprehensive schema for classifying VPI surgical procedures was developed. There was substantial variation amongst surgeons in how each procedure was performed. The schema and variations may allow surgeons to better study surgical outcomes and the mechanisms through which these procedures improve speech.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231181359 - Supplemental material for Surgery for Velopharyngeal Insufficiency Following Cleft Palate Repair: An Audit of Contemporary Practice and Proposed Schema of Techniques and Variations
Supplemental material, sj-docx-1-cpc-10.1177_10556656231181359 for Surgery for Velopharyngeal Insufficiency Following Cleft Palate Repair: An Audit of Contemporary Practice and Proposed Schema of Techniques and Variations by Raymond W. Tse, Kathleen C. Sie and Travis T. Tollefson, Oksana A. Jackson, Richard Kirshner, David M. Fisher, Randall Bly, Jugpal S. Arneja, John P. Dahl, Magdalena Soldanska, Thomas J. Sitzman in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
Research reported in this publication was supported by the National Institute Of Dental & Craniofacial Research of the National Institutes of Health under Award Number U01DE029750. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
This study was facilitated by the VPI-OPS Executive Committee that include Erica Weidler Bainbridge, Adriane Baylis, Jamie Perry, Stacey Ishman, Raymond Tse, and Thomas Sitzman.
The sites involved and supporting the study include Phoenix Children's Hospital, University of California – Davis, University of Alabama – Birmingham, Children's Hospital of Philadelphia, Children's Healthcare of Atlanta, University of Iowa, Rady Children's Hospital, Penn State Hershey Medical Center, Seattle Children's Hospital, The Hospital for Sick Children, and Nationwide Children's Hospital. This project was the culmination of efforts and involvement of the entire VPI-OPS surgeon group that includes: Travis Tollefson, Craig Senders, Gregory Pearson, Ibrahim Khansa, Jonathon Grischkan, Richard Kirschner, John Grant, Joseph Williams, Magdalena Soldanska, Colin Brady, Amanda Gosman, Sam Lance, Oksana Jackson, Joseph Napoli, Jesse Taylor, Jordan Swanson, Scott Bartlett, David Low, Thomas Samson, Don Mackay, Catherine Henry, Mark Fisher, Deborah Kacmarynski, Karen Wong, David Fisher, Terence Kwan-Wong, John Phillips, Christopher Forrest, Jugpal Arneja, Erika Henkelman, Sally Hynes, Saoussen Salhi, Randall Bly, Kathleen Sie, Jonathon Perkins, Jake Dahl, Russell Ettinger, Craig Birgfeld, Richard Hopper, Nicole Kurnik, and Davinder Singh. We would like to acknowledge all these surgeons for their thoughtful discussions of surgical technique and their critical review of the manuscript. Thanks also to Jemère Ruby (jemere.ruby@gmail.com) for assistance with medical illustrations.
Conflicts and Disclosures
None
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Foundation for the National Institutes of Health, (grant number U01DE029750).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.