
Abstract
Objective
To explore the impact of directional laterality in complete Unilateral Cleft Lip (UCL) amongst the global cleft surgeon community
Design
Cross-sectional survey study.
Setting
Global distribution of online survey distributed in English and Spanish.
Participants
Cleft surgeons from around the world.
Main outcome measures
Survey participant perception of the impact of laterality on: (1) cleft presentation (2) surgical challenge and (3) surgical outcomes.
Results
Responses were received from 453 cleft surgeons located in 54 countries around the world. 221 (49%) had previously considered differences in patients presenting with a left- versus right-sided UCL. 95 (21%) considered right-sided clefts more difficult to reconstruct, 37 (8%) reported left-sided clefts to be more difficult and 321 (71%) reported no difference in difficulty between the cleft sides. Higher volume cleft surgeons, characterised by those reporting cleft as their principal area of practice and performing >20 cleft operations per year, were more likely to have both previously considered differences in laterality in cleft and to report right-sided unilateral cleft lip to be more difficult to primarily reconstruct. 395 (87%) did not consider surgical outcomes to be influenced by cleft laterality.
Conclusions
This survey reports perceptions on cleft laterality from a large body of global surgeons and suggests a trend for increased difficulty in right-sided compared to left-sided cleft lip reconstruction, where such laterality-associated difficulty is perceived.
Introduction
There are many variables that influence the surgical approach to complete Unilateral Cleft Lip (UCL) regardless of technique and one such variable is the sidedness of the cleft, hereafter also referred to as ‘laterality’. Laterality in complete UCL presents as a non-random directional asymmetry, with twice as many people born with a left-sided cleft compared with a right-sided cleft1,2 and this is a globally recognised phenomenon. 3 Despite this, little has been researched into the opinions of cleft surgeons regarding the perceived effect of laterality.
There may be several reasons for why laterality may impact cleft care and, in particular, surgical intervention. With the increased frequency of left-sided cleft lips, surgeons may have greater familiarity with operating on this side for primary repair – in effect a unilateral field advantage.4,5 In addition, the majority of people are right-handed and this is thought to influence perception of lateralisation on both an individual and population basis, although the extent of this remains unknown. 6 Eye dominance, a phenomenon distinct from brain dominance, may also modulate visuospatial attention. 7 Intrinsic factors to the cleft may also play a role in laterality effects. A recent study has reported anthropometric differences between left- and right-sided cleft lips that may influence surgical management and outcomes. 8 To explore all these concepts further, we sought to survey a body of cleft surgeons globally to establish whether the laterality of complete UCL impacted their perception, practice, and surgical outcomes in complete UCL reconstruction.
Methods
Survey Design and Distribution
A novel survey instrument was initially developed with reference to published guidance 9 by a panel with experience in survey methodology, appraisal of cleft outcomes and global cleft surgery. The panel consisted of a senior global cleft surgeon, two post-FRCS surgical residents and three Global Surgery Fellows from five different institutions worldwide. To identify whether cleft laterality influenced the practice of cleft surgeons, questions were mapped to the three broad domains of (1) cleft presentation (2) surgical challenge and (3) surgical outcomes. Consensus agreement among members of the panel produced a draft instrument that was subsequently piloted, and feedback incorporated into the final survey. The final survey comprised 22 questions that explored the demographics, professional background and proportionate cleft workload, handedness, and beliefs about the impact of cleft laterality in the three aforementioned domains. It was deemed to represent a Quality Improvement project by our ethical review board and thus was certified as not requiring formal ethical clearance. The survey was trialled for bias and translated into English (Appendix A) and Spanish (Appendix B). Respondents had the opportunity to add free text and all responses were anonymised.
Surgeons around the globe, undertaking repair of complete UCL independently, were eligible to participate in the survey. The survey was circulated in electronic format every 2–5 days over a 30 day period in April / May of 2021 using the SmartSurvey tool. 10 The survey was distributed via media platforms but restricted to surgical fora and global cleft organisational networks only. As this survey was circulated on media portals, a formal non-responder bias was not undertaken.
Statistical Analysis
All data were compiled through the SmartSurvey tool in real time and findings reported according to the CHERRIES checklist for web-based surveys. 11 Responses were reported as proportions and the association of variables to the three main domains as percentage differences. The use of inferential statistics was purposefully avoided because the variables were not strictly independent of one another, thereby precluding the ability to infer causation. 12 For completeness, however, further statistical analysis can be found in Supplement 1 on the association of binomial variables with respect to beliefs on laterality, reporting on odds ratios, confidence intervals and p values. Statistical analysis was conducted using the R Project for Statistical Computing, version 4.0.5. 13
Results
Demographics
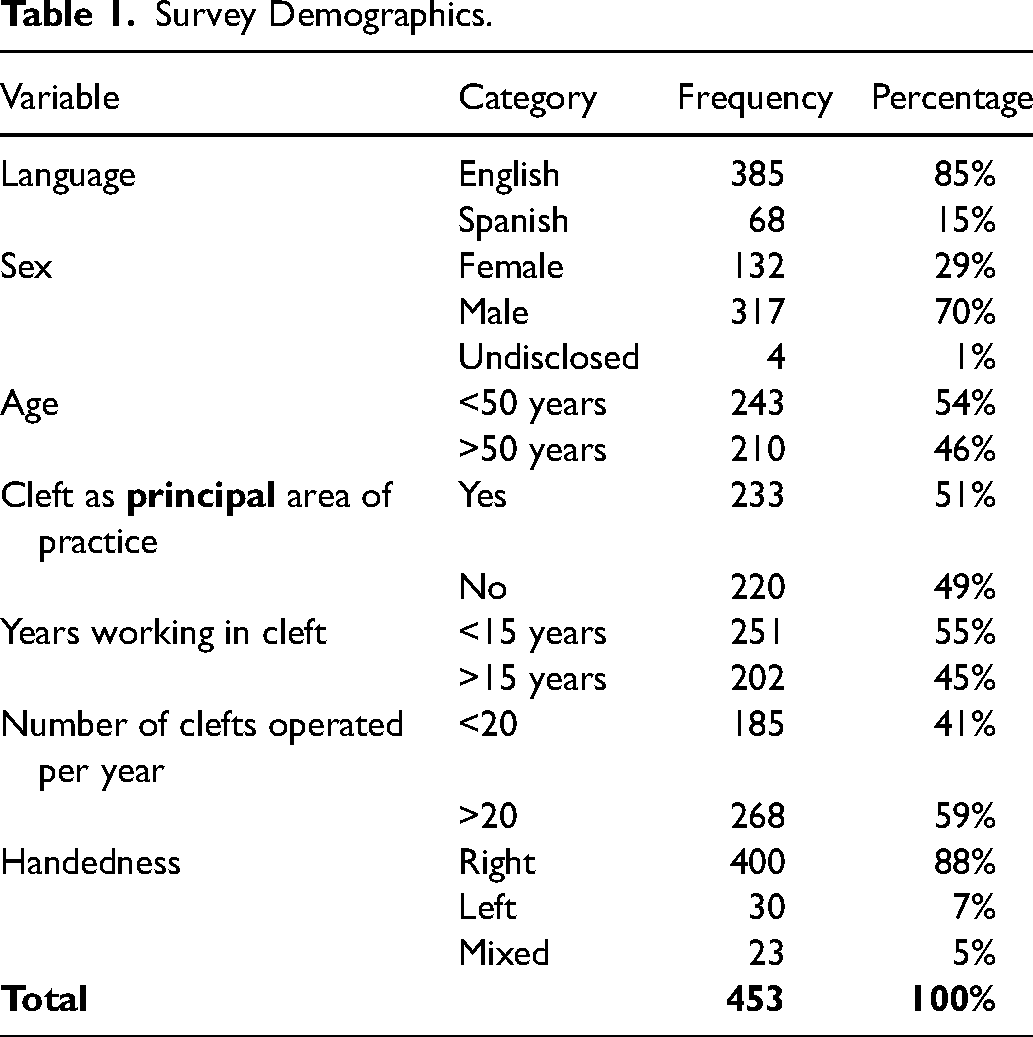
453 completed responses were received with demographic data described in Table 1. 29% of respondents identified as female and 70% as male, with 1% preferring not to specify their gender assigned at birth. 17% of surveys were undertaken in Spanish. The locations of respondents’ practice spanned 54 countries and was dominated by North America (16.8% of respondents), as depicted in Figure 1. The average age of respondents was 50.1 years (mode 41–50 years). 88% of respondents claimed right-handed dominance, 7% left-handed dominance with 5% claiming mixed-handedness.
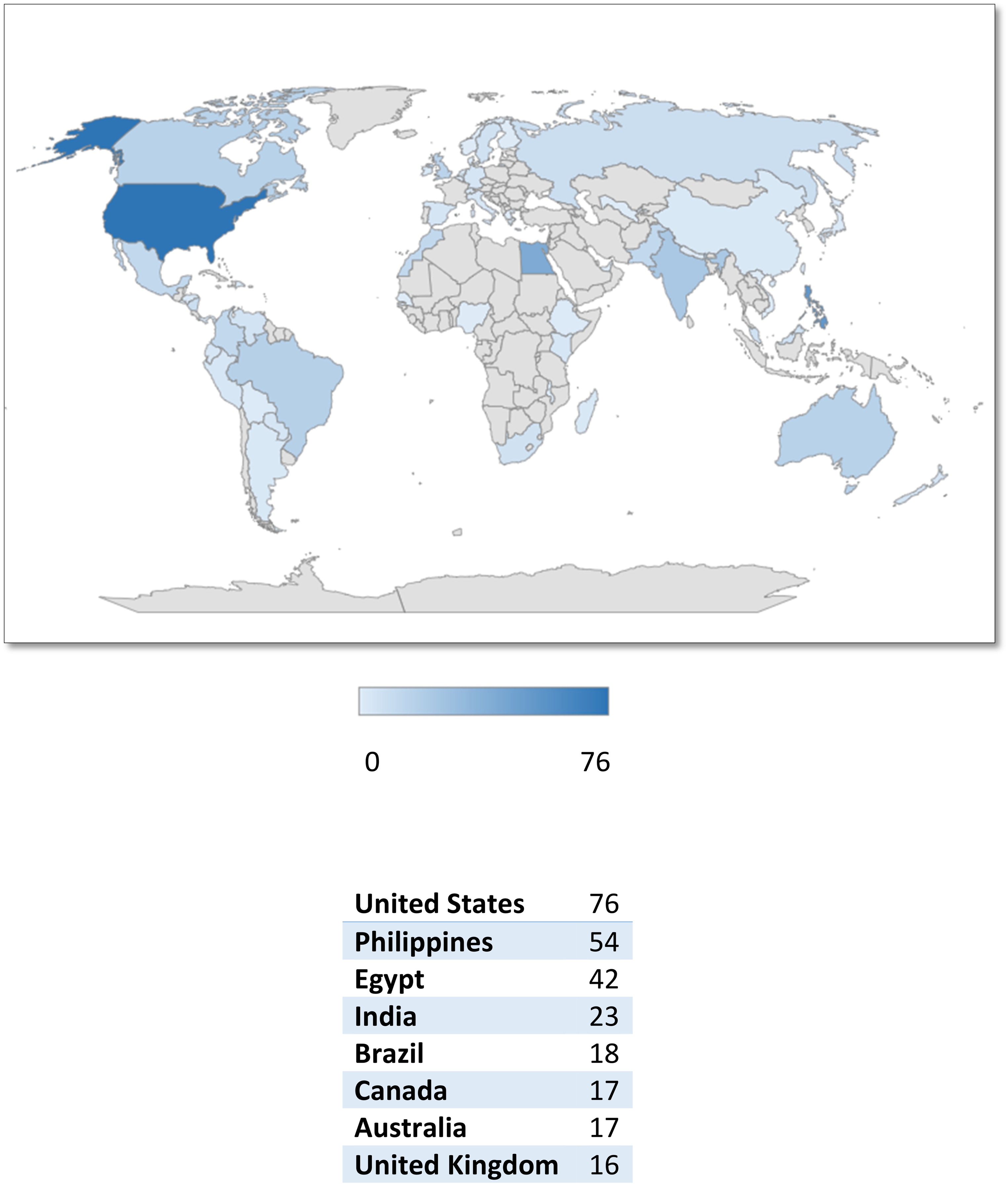
Global distribution of respondents’ surgical practice.
Survey Demographics.
Respondents’ surgical training spanned five main surgical specialties with the majority having trained in Plastic Surgery (80.3%) followed by Oral & Maxillofacial Surgery (13.7%) (Figure 2). 21.4% had been undertaking cleft surgery independently for over 25 years with over 60% of respondents operating independently for over a decade. 59% of respondents undertook more than 20 primary CL procedures per annum. 51% of overall respondents considered cleft as the principal focus of their practice.
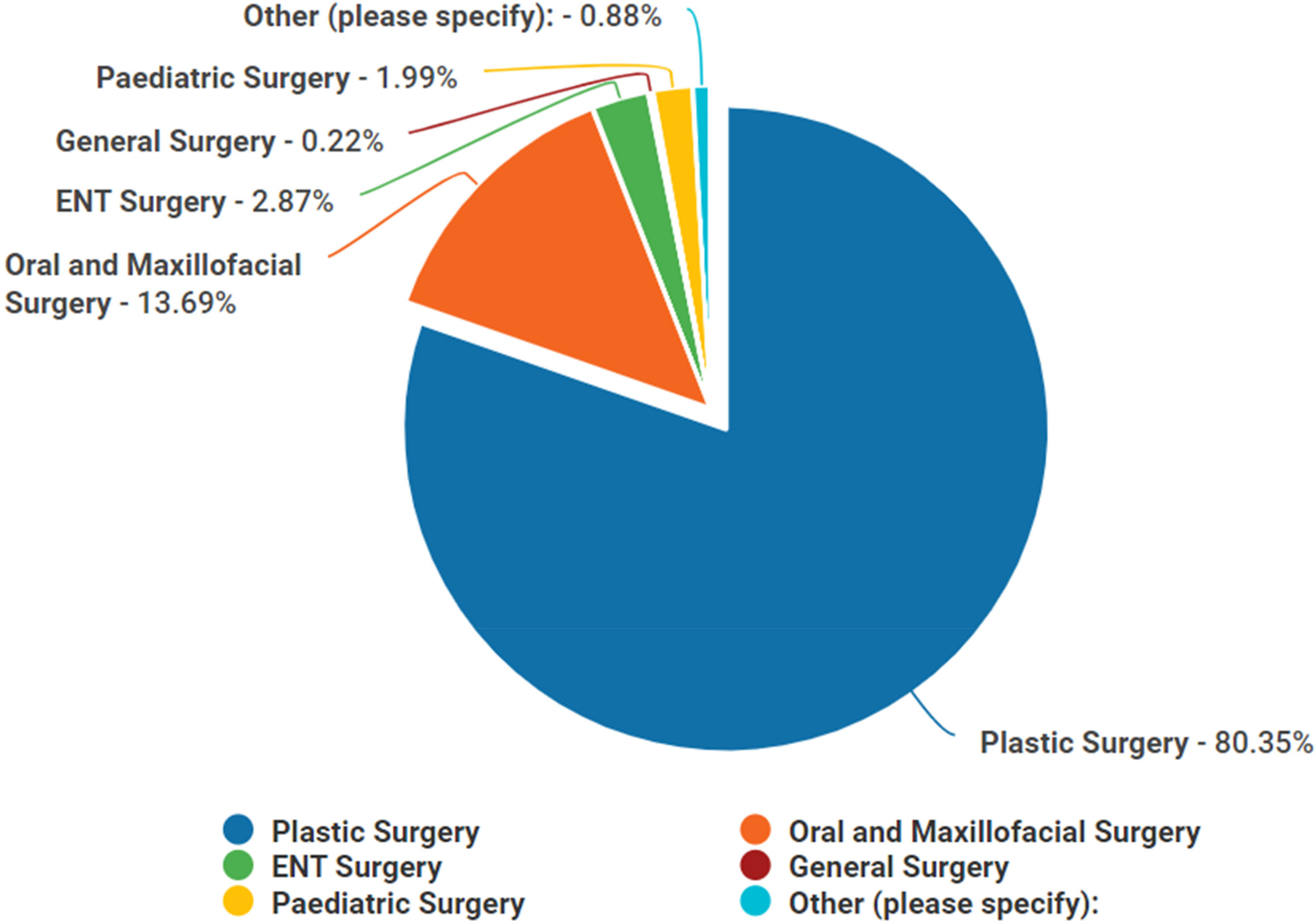
Background specialty of respondents.
Beliefs About Cleft Laterality
The following three domains of surgical cleft experience were explored:
Had the respondents considered laterality differences in cleft presentation before? Did cleft laterality impact upon perceived surgical difficulty in lip reconstruction? Did cleft laterality impact of upon surgical outcomes following lip reconstruction?
Of the 453 respondents, 221 (49%) had previously considered differences to exist between patients presenting with a right- versus left-sided complete UCL. 232 (51%) respondents had not previously considered laterality. One such respondent stated in the free text:

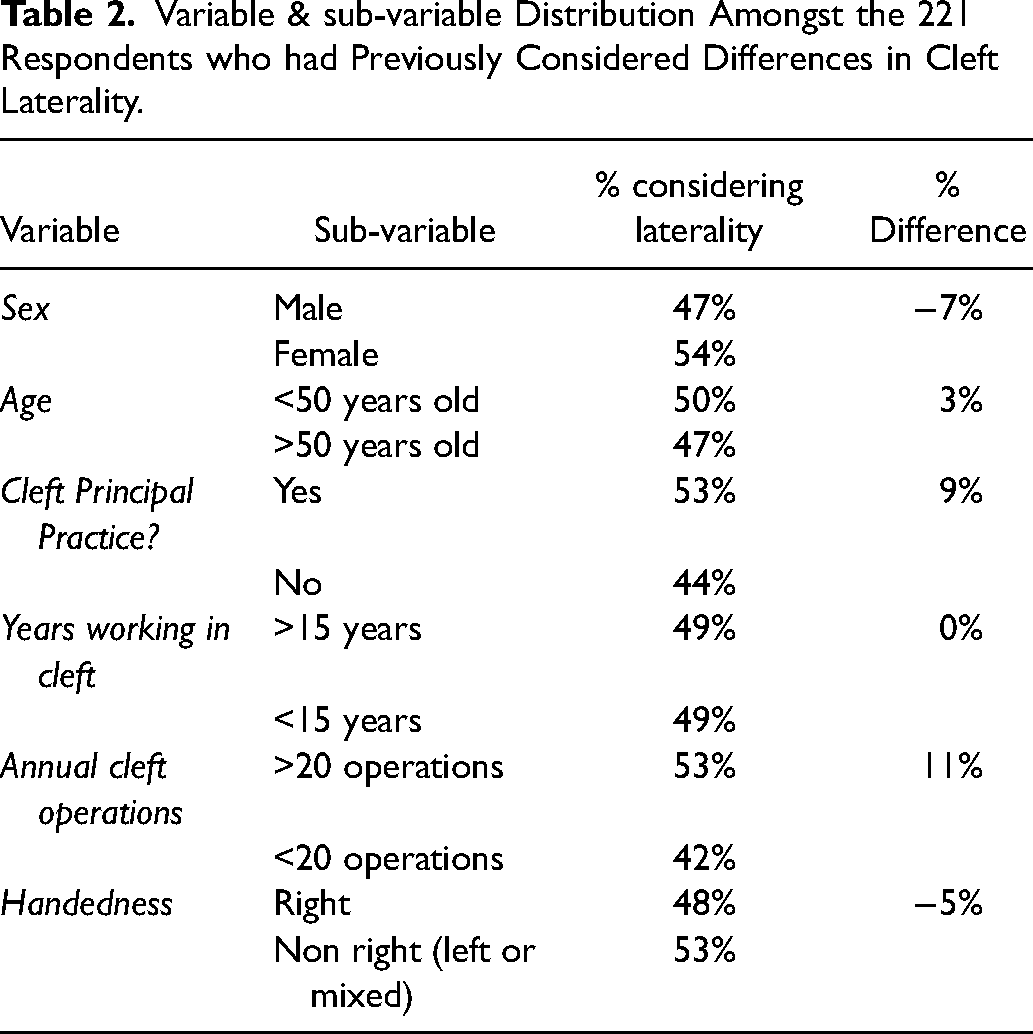
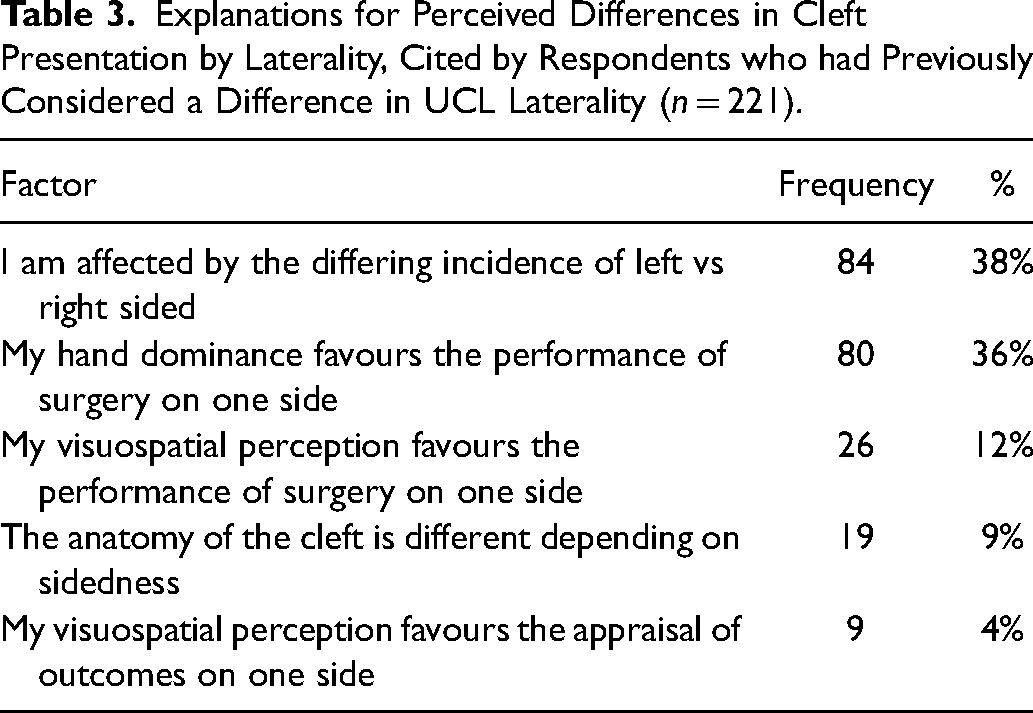
When analysing the consideration of differences in laterality, the greatest percentage difference between those that had considered this phenomenon and those that hadn’t related to cleft being their principal area of practice and higher volume cleft operating of more than 20 clefts per year (Table 2). The most common explanations for the belief that differences existed were the increased frequency of left- compared to right-sided clefts and the hand dominance of surgeons favouring one side (Table 3).
Variable & sub-variable Distribution Amongst the 221 Respondents who had Previously Considered Differences in Cleft Laterality.
Explanations for Perceived Differences in Cleft Presentation by Laterality, Cited by Respondents who had Previously Considered a Difference in UCL Laterality (n = 221).
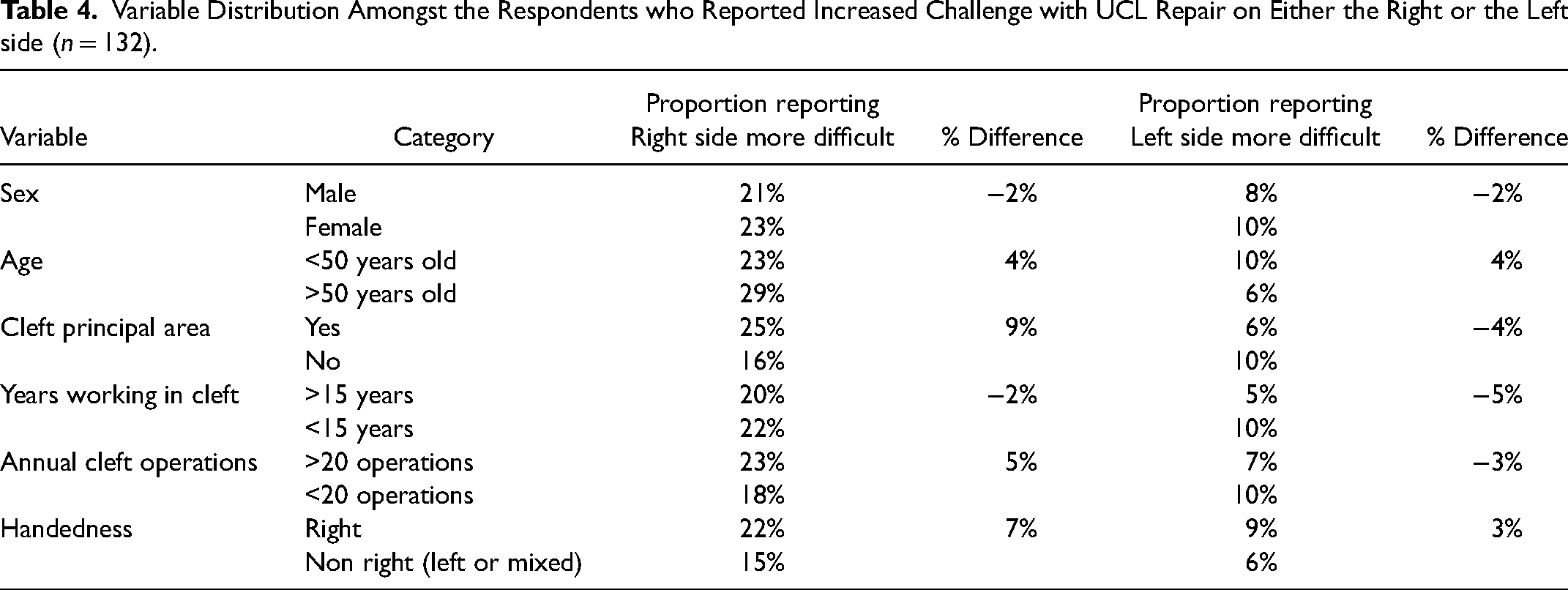
Of the 453 respondents, 95 (21%) considered right-sided clefts more difficult to reconstruct, 37 (8%) reported left-sided clefts to be more difficult and 321 (71%) reported no difference in difficulty between the cleft sides. Table 4 reports the variable distribution amongst the 132 respondents who reported more difficulty for either a right- or a left-sided lip reconstruction. Cleft as a principal area of practice and a higher volume of annual cleft operations were associated with finding a right-sided cleft repair more difficult. The opposite was true for finding a left-sided cleft repair more difficult.
Variable Distribution Amongst the Respondents who Reported Increased Challenge with UCL Repair on Either the Right or the Left side (n = 132).
395 of the 453 respondents (87%) did not consider their surgical outcomes to be influenced by cleft laterality. Of the minority who did consider an impact of laterality on outcomes, 46 (10%) reported worse outcomes in patients with right-sided UCL compared to 12 (3%) reporting worse outcomes in patients with left-sided UCL. Small sample size precluded sub-variable analysis amongst respondents who did report a difference in outcomes.
Discussion
Summary of Findings
If one considers the null hypothesis that the laterality of UCL does not influence or impact any aspect of diagnosis, treatment, or outcome then the results of this study challenge this based upon the enduring observations of the cleft surgical fraternity. In this survey of global cleft surgeons, we report 49% having previously considered differences in clinical presentation between patients with a left- versus right-sided UCL. A higher proportion of respondents found right-sided clefts lips more difficult to repair than left-sided cleft lips (21% vs 8%). Higher-volume cleft surgeons, characterised by those reporting cleft as their principal area of practice and performing >20 cleft operations per year, were more likely to have both previously considered differences in laterality in cleft and to report right-sided UCL to be more difficult to primarily reconstruct.
Strengths and Weaknesses
The strength of this study is the large sample size of cleft surgeons located within a wide range of countries from around the world which, in a niche surgical specialty such as cleft, is likely to be represent a substantial body of global opinion regarding cleft laterality. The main weaknesses of this study are the range of bias's inherent to survey design that threaten validity. 14 We attempted to minimise sampling bias by enhancing accessibility via the online survey design, use of global cleft networks for dissemination and translation into Spanish. It is always possible that inadvertent non-response bias may have skewed our results as respondents who have an interest in cleft laterality may have been more likely to have considered differences in laterality previously. Reporting bias was reduced by our use of descriptive statistics and avoidance of inferential analysis, in accordance with expert statistical advice. Additionally, our survey enquired about fellowship experience, but it became apparent that interpretation of the formality of such experience was highly subject to interpretation and likely influenced by healthcare setting. As an alternative, we elected to substitute absolute numbers of primary UCL repair procedures and self-reported principality of focus as more accurate parameters of overall experience.
Comparison with Previous Studies
The phenomenon of directional asymmetry in UCL has been previously described, with repeated epidemiological analysis of international cleft registries demonstrating that left-sided cleft lips occur twice as commonly than right-sided cleft lips.3,15 From an embryological perspective, the human body demonstrates lateralised patterning during development of major viscera and parts of the brain. 16 From a pathological perspective, other pathologies share a left-sided predominance with cleft, such as pre-auricular skin tags, congenital hip dysplasia and absent forearm or hand1,17 as well as brain anomalies. 18 Combined phenomena even exist; the incidence of non-right handed dominance amongst patients with left-sided cleft lip is significantly different to patients with right-sided cleft lip. 19 Previous authors have hypothesised that right-sided clefts may have a distinct aetiology to left-sided clefts,20,21 echoing similar hypotheses for other congenital malformations of paired structures that have a non-random propensity to affect a particular side. 22 Causal pathway theories include genetic differences, vascular mechanisms and a multifactorial threshold of both exogenous and endogenous factors. 23 Indeed, potential genetic modifiers of cleft laterality have already been identified. 24
Data from previous studies have highlighted patient perceptions of their UCL reconstruction with respect to laterality, with patients born with right-sided clefts being more likely to request revisional surgery. 25 In addition, other studies have demonstrated that clinicians asked to assess cleft lip reconstructions were more likely to consider right-sided clefts to present with poorer outcomes. 26
Interpretation and Implications
This study reports the important survey finding, that when laterality was considered by surgeons, right-sided clefts were more often considered to be difficult to repair compared to left sided clefts. Possible explanations for this finding can be considered into factors extrinsic and intrinsic to the cleft itself. Extrinsic factors include the lower incidence of right-sided cleft, the handedness of a surgeon and different visuospatial perceptions associated with right- or left-brain dominance. Intrinsic factors include severity of the cleft phenotype.
Of particular interest, higher volume cleft surgeons, defined as performing >20 cleft operations annually and identifying primarily as cleft surgeons, were more likely to have considered the effects of laterality and more likely to consider right-sided cleft lips more difficult to reconstruct. It would be reasonable to expect that the increasing experience and expertise of higher volume surgeons should mitigate the impact of extrinsic factors of cleft incidence and surgeon-handedness, much like they do with handedness-associated complication rates in other surgical specialties.4,28 Instead, we notice the opposite phenomenon, from which we infer that intrinsic factors may play a more significant role in the perceived difficulty of operating on right-sided clefts.
There have been indications in the literature to suggest that right-sided clefts may be more likely to represent a more severe phenotype compared to left-sided cleft lips. Right-sided cleft lips were found to have a higher proportion of soft tissue hypoplasia in the lateral lip element, a finding that has underpinned a classification of hypoplasia in lips to help define this further in the future 27 It has also been suggested that right-sided clefts are associated with a greater proportion of additional congenital anomalies and poorer educational outcomes. 20 Collectively, these findings suggest that additional (extended) phenotypic features may be associated with – and intrinsic to - right-sided clefts, contributing to their greater surgical challenge.
Interestingly, the proposed explanations cited by surgeons who had previously considered laterality effects were predominantly extrinsic in nature - namely difference in frequency of right- vs. left-sided clefts and hand dominance of the surgeon. Whilst it might be expected that a right-handed surgeon might consider the repair of a right-sided cleft more challenging, for reasons of both hand dominance and cleft frequency, it was notable that the proportion of non-right-handed surgeons who considered right-sided clefts more challenging to repair was greater than the corollary of those right-handed surgeons who found left-sided clefts more difficult to repair. This suggests that the extrinsic factor of handedness is unlikely to provide the complete answer for why right-sided clefts are considered more difficult to reconstruct.
Anatomical differences due to laterality were identified as a perceived factor in just under 5% of respondents who had considered laterality, demonstrating that intrinsic differences in cleft morphology by laterality is not yet a widely recognised phenomenon despite demonstrable objective anthropometric evidence, albeit published recently. 8
Conclusion
This survey represents a global enquiry into the beliefs of laterality on surgical care of patients with UCL. It has identified over 200 surgeons that perceive an overall impact of cleft laterality in their work and identifies a potential interplay between intrinsic and extrinsic factors in that perception. A consistent finding is the belief that right-sided clefts present a greater surgical challenge than left-sided clefts amongst those that subscribe to a laterality impact in surgery. This might be considered attributable to extrinsic factors, such as the increased frequency of right-handed surgeons and the relatively infrequency of right-sided clefts. Further cohort analysis, however, reveals that the perception of greater right-sided cleft difficulty is more likely to be held by high-volume surgeons, which is a counterintuitive finding if one considers that increasing experience should be expected to mitigate extrinsic factors.
There is increasing evidence that right-sided clefts may have a distinct aetiology and be associated with poorer outcomes. A thorough and systematic investigation into the influence of cleft laterality on various domains of cleft care is warranted, as it appears that laterality of cleft presentation is associated with intrinsic variables that may have been underestimated.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231181904 - Supplemental material for The Implications of Laterality in Unilateral Cleft Lip Reconstruction: A Global Survey of Cleft Surgeons
Supplemental material, sj-docx-1-cpc-10.1177_10556656231181904 for The Implications of Laterality in Unilateral Cleft Lip Reconstruction: A Global Survey of Cleft Surgeons by Ambika Chadha and Daniel Bradley, Matthew Fell, Maria Fernanda, Atenas Bustamante, David Chong in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656231181904 - Supplemental material for The Implications of Laterality in Unilateral Cleft Lip Reconstruction: A Global Survey of Cleft Surgeons
Supplemental material, sj-docx-2-cpc-10.1177_10556656231181904 for The Implications of Laterality in Unilateral Cleft Lip Reconstruction: A Global Survey of Cleft Surgeons by Ambika Chadha and Daniel Bradley, Matthew Fell, Maria Fernanda, Atenas Bustamante, David Chong in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-3-cpc-10.1177_10556656231181904 - Supplemental material for The Implications of Laterality in Unilateral Cleft Lip Reconstruction: A Global Survey of Cleft Surgeons
Supplemental material, sj-docx-3-cpc-10.1177_10556656231181904 for The Implications of Laterality in Unilateral Cleft Lip Reconstruction: A Global Survey of Cleft Surgeons by Ambika Chadha and Daniel Bradley, Matthew Fell, Maria Fernanda, Atenas Bustamante, David Chong in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-4-cpc-10.1177_10556656231181904 - Supplemental material for The Implications of Laterality in Unilateral Cleft Lip Reconstruction: A Global Survey of Cleft Surgeons
Supplemental material, sj-docx-4-cpc-10.1177_10556656231181904 for The Implications of Laterality in Unilateral Cleft Lip Reconstruction: A Global Survey of Cleft Surgeons by Ambika Chadha and Daniel Bradley, Matthew Fell, Maria Fernanda, Atenas Bustamante, David Chong in The Cleft Palate Craniofacial Journal
Footnotes
Acknowledgements
We thank the global cleft organisations that allowed us to use their networks to disseminate this survey. We thank Professor Susan Donath at the University of Melbourne for statistical advice.
Data Access
Please contact the authors if you would like to access the data. Access will be granted for reasonable usage.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.