
Abstract
Objective
Given prior craniofacial research reporting higher risk for negative social interactions, this study aimed to explore experiences of stigma described by children with cleft lip and/or palate (CL/P).
Design
Qualitative interviews were conducted with children in three sessions (totaling 90–180 min) using creative activities in their homes and/or and walking interviews in their neighborhood. Interview transcriptions were interpreted primarily with thematic analysis following theoretical frameworks of the stigmatization process and self-stigma concept.
Setting
Participants were recruited through Operation Smile Colombia. Interviews took place at children's homes and neighborhoods within three Colombian regions (Boyacá, Bogotá and Cundinamarca).
Participants
Children (N = 12) with CL/P aged between 6–12 years were interviewed.
Results
Themes fit within the stigmatization process, starting with labeling and stereotyping, such as a range of mockery, and group separation by peers highlighting their not belonging and being socially ‘other’. Status loss themes included negative appraisals of cleft-related differences and being perceived as ‘ill’ and ‘imperfect’. Social exclusion themes reflected limited social interactions and loneliness. Self-stigma themes included shame about speaking with peers and anticipation of negative social interactions.
Conclusions
The study results suggest that the process of stigmatization and self-stigma adversely affect social interactions for children with a cleft in multiple ways. Healthcare practitioners and policy makers can help address the potential consequences of stigma by implementing interventions at micro, meso and macro levels.
Introduction
Many studies suggest that children with cleft lip with or without cleft palate (CL/P) are frequently the object of negative social responses1–6 including teasing, bullying and staring.3,5–9 These social responses can have negative impacts on children's mental and physical health and contribute to significant disadvantages in their life opportunities, including education.5,9–12
One way of examining these negative responses and impacts is through the concept of stigma. One group of authors describe stigma as a process that occurs within a context of power imbalance and composed of five key elements: labeling, stereotyping, separating those labeled from “us”; status loss and discrimination. 13 Those who are stigmatized may be likely to incorporate labels and stereotypes as aspects of themselves, a process known as self-stigma.13,14 Within this act of internalizing stigma, the stigmatized person absorbs negative messages or ideas about their attributes and comes to believe them and adopt them as part of their identity.13,15 Growing evidence shows that self-stigma is a significant source of social disadvantage and emotional and psychological stress. 15 Negative expectations by others may result in less positive interactions and social avoidance worsening mental and physical health and quality of life. Stigma is also associated to poor therapeutic adherence and help seeking.16,17
Despite awareness among researchers and healthcare practitioners that children and young people with CL/P are frequently stigmatized with serious social and emotional consequences, little is known about their experiences of stigma.1,2 Related, children and young people are under-represented in stigma research particularly in global south contexts. 18 This is concerning as the prevalence of CL/P is high in many Latin American counties. 19
Colombia is a middle-income country located at the northwest of South America. It is the third largest country in this region with a population of around 50 million. 20 Orofacial clefts are one of the most frequent birth conditions in this country with a birth prevalence of 6.0 per 10 000 live births. 21 In relation to healthcare system, Colombia's General System of Social Security in Health entails a universal health insurance model with two main insurance programs: the contributory plan covers employes and those able to pay and the subsidized plan provides health insurance coverage for those on low incomes. 22 Although cleft care is covered by the national healthcare system, international non-governmental organizations (NGOs) offer specialized care and support. NGOs are perceived as providing high quality and comprehensive care as opposed to the regular treatment offered by Colombia's health system. 23
Qualitative research available on cleft-related stigma has mainly been conducted with parents of children with a cleft and focused on the social costs of having a child with a bodily difference,24,25 rather than experiences of children themselves. The paucity of N research on children's experiences of stigma is a research gap addressed by this study. By drawing on children's own stories, this paper examines their experiences of stigma following two theoretical frameworks: the stigmatization process 26 and self-stigma.
Methods
Design
This qualitative study aimed to explore children's experiences of stigma drawing on their own accounts. Qualitative research allows a contextual, in depth and individual exploration of how people make sense of their experiences, life circumstances and social worlds.27,28 This research is further informed by an understanding of children as social agents, able to participate actively in the research process and talk about their own experiences.29–33
Participants
Participants were recruited through Operation Smile Colombia. Children aged between 6 and 12, with any form of cleft (cleft lip, cleft lip and/or palate, cleft palate, alveolar cleft), were invited to participate in the research. Children with additional craniofacial diagnoses along with a cleft, such as microtia, were also eligible to participate. All children had completed cleft surgery prior to the study. Those with a diagnosis of malnutrition or a major health condition were excluded.
Twenty children with cleft lip and/or palate (CL/P) took part in the study with the majority of the sample being from urban areas from strata 1-2 and 3-4 according to the socio-economic stratification system in Colombia. This is a system which classifies neighborhoods in Colombia from one to six. The most socio-economic deprived areas correspond to strata one and two. Middle-class is equivalent to strata four, while the most affluent population is strata six. Qualitative research does not seek to epidemiological representativeness 34 and the sample was considered sufficient to generate and explore in-depth qualitative accounts of living with CL/P. Inclusion in the subgroup of 12 participants analyzed in this study was determined by those who reported on stigma. Table 1 summarizes some socio-demographic features, ages and types of cleft of our sample.
Characteristics of the Sample.
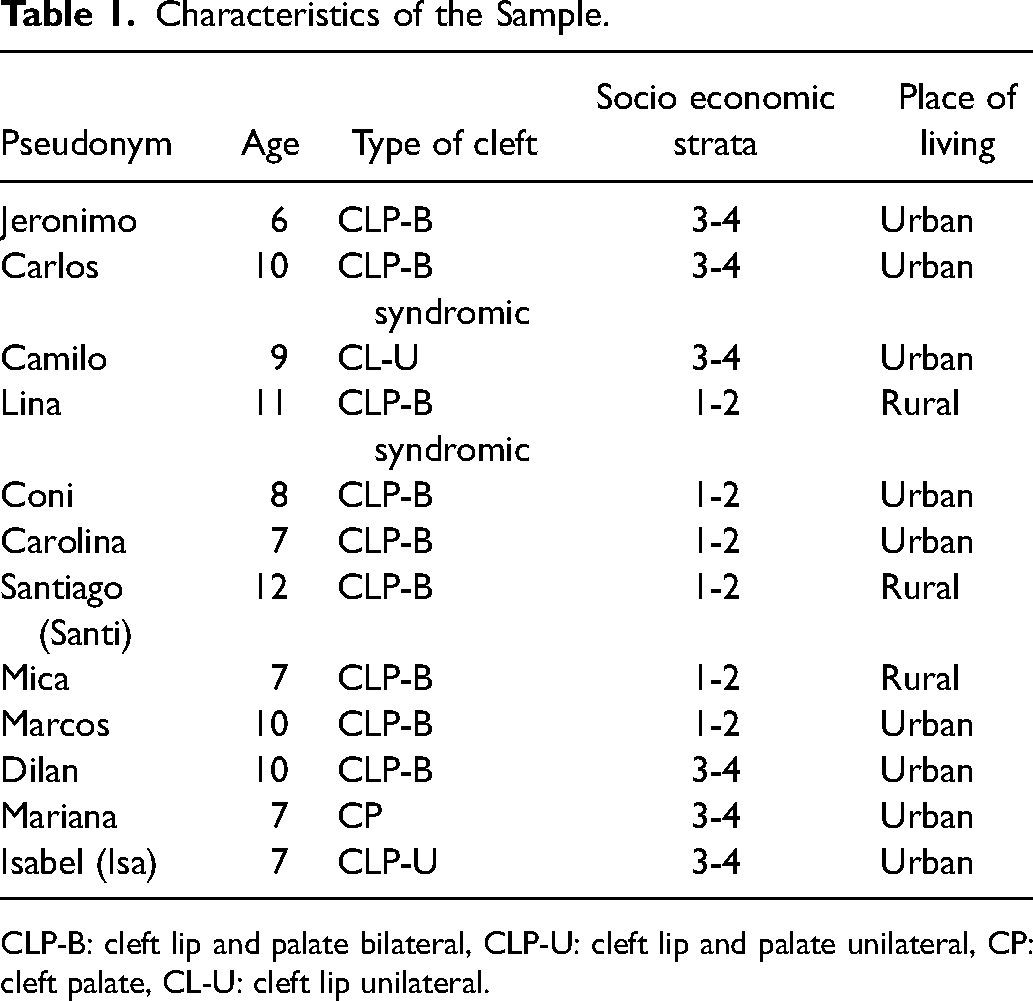
CLP-B: cleft lip and palate bilateral, CLP-U: cleft lip and palate unilateral, CP: cleft palate, CL-U: cleft lip unilateral.
Data Generation
Data was generated through face-to-face semi structured interviews with children over three different encounters. Interviews took place between 2–4 weeks apart. The time across the three visits was between 90 and 180 min. Each interview lasted around 45 min. This paper focuses on interview topics related to the social experiences of having a visible facial difference. Qualitative interviews were completed in combination with some creative tools. Visual vignettes and drawings were used to prompt children to talk about topics such as school lives and friendships.
Body maps were used as we were interested in looking at how children felt and understood their bodies and to explore their views of their bodies as a whole, not only self-image. Existing research has documented how self-image of people with orofacial clefts may be affected by negative public attitudes about their physical appearance, which can have a negative effect on self-esteem. 35 While self-image is a term commonly used in psychology which refers to how people look at themselves and contributes to establish one's self-concept,36,37 this study focused on self-stigma as the processes through which labels and stereotypes are incorporated as part of people's identities.13,15 Some children also made a visual representation of their lives using different materials (pencils, crayons, paper, photographs, etc) and in different formats (photo story, book, poster, timeline, digital presentation). They included key life episodes and stories recounted in the interviews.
The interviews (and tools) were designed to be flexible to children's preferences and socio-cultural backgrounds, and we also ensured that communication with them was at their level of understanding. Children decided whether their parents were present or not in the interviews and whether interviews would be audio recorded. All children agreed with interviews being audio recorded. Seven children (pseudonyms used throughout the study of Lina, Carolina, Camilo, Mariana, Santi, Isa and Jeronimo, invited one of their parents to be present in one of the interviews, particularly for the first encounter and the walking tour. Five children (Dilan, Coni, Carlos, Marcos and Mica) decided to talk without them, stating that they did not need ‘any help’ from their parents.
Two different interviews approaches were offered: home-based interviews and walking interviews. The walking format was offered for the second and/or third encounters. Most children chose to have a combination of home and walking interviews; two chose only home. While home based interviews offered children a familiar and comfortable setting to speak of their experiences, walking interviews provided them the opportunity to share their stories in an outdoor and dynamic context. Walks were planned by children in agreement with their parents or caregivers and entailed tours guided by the children to places significant to them around their homes/neighborhoods. In many cases, these tours gave children opportunities to speak of their experiences as they offered a comfortable and relatively more private setting, particularly when the home was noisy and lacked privacy. The interactional and dynamic nature of the walking tours also prompted participants to connect with significant places and landscapes, something that facilitated the process of recalling memories. 38 Although some children's schools were located in their neighborhoods, interviews did not take place at schools.
Analysis
Interviews were transcribed verbatim in Spanish and then translated into English. Data including transcripts and fieldwork notes, which were analysed through incorporating the listening guide, 39 larger contextual factors beyond children's narratives 40 and thematic analysis 27 led by Author A. Results were interpreted based on theories of stigmatization and self-stigma. Each interview transcript was read a number of times, focusing on how the participant spoke of themselves and in relation to others, 39 building a picture of their experiences.
A coding scheme was developed from the emergent themes that were identified from the multiple readings of transcripts. NVivo (QSR International) was used to facilitate coding and data management. Further development of the themes drew upon literature from childhood studies, medical sociology and two stigma models: the stigmatisation process 26 and self-stigma.13,14 To do this, mind maps of relevant themes were constructed which included some coded extracts from the transcripts and links with key literature (see Figure 1).
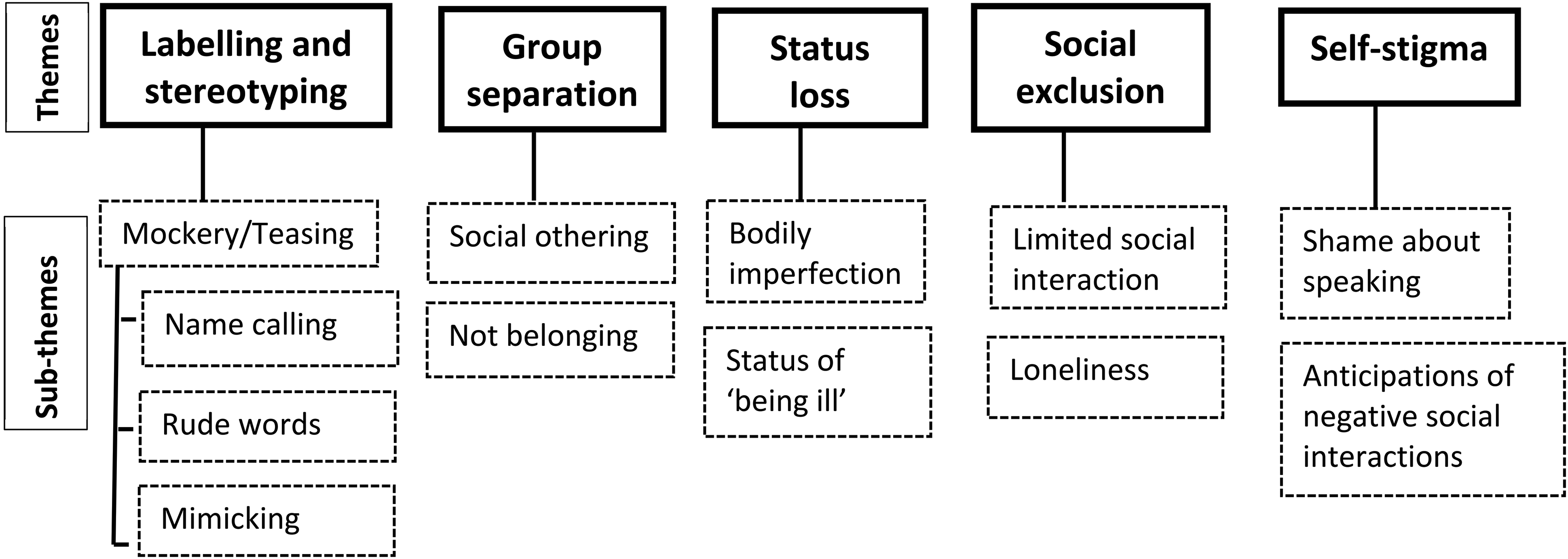
Thematic map. This map illustrates themes and subthemes that emerged during data analysis.
Ethics
The study was approved by the Ethics Committee of an university in the UK. This was in conjunction with local research approval (Operation Smile- Colombia). Participation was voluntary and consent was obtained from children and their parents at different points of the research. During the interviews, the children were also encouraged to indicate if there was a topic they did not want to discuss.
Participants’ confidentiality was protected by the anonymization of their names (pseudonyms), no sharing details of their places of living, encryption of transcripts and their works with creative tools. However, this confidentiality had some limitations in two cases where children's wellbeing was at risk of harm. One child disclosed a long term history of domestic abuse against their mother in our first interview. Following procedures set out in the study protocol, the case was reported to the social worker of Operation Smile. Another participant reported explicit physical and emotional abuse from their mother, which was observed in our encounter. The case was reported to the social worker and the participant was excluded from the study following social worker's advice (this participant is not included in the initial sample of 20).
Results
In this section we present the different forms of stigma experienced by 12 participants based on Link and Phelan's theory: labelling and stereotyping, separation us from them, status loss, discrimination and self-stigma. 13
Labelling and Stereotyping
Almost half of the participants reported events where both visible facial differences and speech were the object of labels and stereotypes. These episodes occurred at children's school. The shape of their nose, the tone and the intelligibility of their speech were the features more frequently labeled and stereotyped, giving way to mockery, which included name calling, rude gestures, speech mimicking and the use of pejorative terms in reference to their bodily differences: ‘…They’re children kinda cruel you know… when they are mad at me they call me smashed nose …’
(Marcos, 10 year old boy with CL/P)
‘…There's a boy and a girl uhmm they annoy me all the time and they’re like: … “hummm hum hummm”… [mimicking his speech].’
(Dilan, 10 year old boy with CL/P)
In addition to nose shape and speech, less visible facial differences were also targets of mockery. Features such as missing teeth, gingival hyperplasia and minor upper lip scars were commonly labelled and stereotyped. Name-calling and rude gestures were also frequently used. For example, an 8-year-old girl with CL/P Coni recounted an episode where her dental issues (congenital missing teeth and gingival hyperplasia) led to name-calling by school peers: ‘…Well, one day, we all were in the cafeteria and I was eating… and Mateo came to me, and Sergio (brother) and Julian too… and Julian was like: “hi! Brain-shaped mouth. I just remember that and I feel like Ím gonna cry now.’
Jeronimo, a 6-year-old boy with CL/P, spoke of a similar encounter in which the name calling did not explicitly relate to CL/P, although this was how he interpreted it: Jeronimo: ‘…Uhmm one day a boy at school told me I was a fool …and he also told me I was an ugly and dirty pig …
Interviewer: ‘Why do you think he told you those things?
Jeronimo: ‘Uhm, ‘cause of my mouth.’
Although labelling and stereotyping frequently took the form of obvious negative comments or gestures, in other cases these actions were less explicit. For example, while being prompted by a card showing the sad face of a child, one boy said: ‘He might be sad because uhmm… he feels bad ‘cause he can’t walk or maybe he doesn’t like something… or…maybe somebody mocks him.’
(Santi, 12 year old boy with CL/P and unilateral microtia)
He further commented that he is widely called a name he does not understand the meaning of, which could be similar to pejorative terms used when people have missing body parts, as Santi also has unilateral microtia.
Separating ‘them’ from ‘us’ and Status Loss
Labelling and stereotyping led to apparent group separation and status loss. Similar to Santís case, other children spoke of how some bodily differences and medical treatments, such as speech therapies, were linked to the social labels of imperfection and illness that was perceived as separating them: ‘The thing is… I feel this [downward pointing nose] like a weight on my shoulders, ‘cause at times they [peers] mock you and criticise you all the time … they say: “we were born perfect and you weren’t” and that hurts me.’
(Marcos 10 year old boy with CL/P)
‘… you know that I was operated on, right?… so they [peers] often say that I’m ill…and that I need the doctor and so on… but that's not true, ‘cause I’m not ill or things like that, I just go to the speech doctor [speech therapies] and that's it.’
(Mariana, 8 year old girl with CP)
Discrimination
Participants spoke of both subtle and overt episodes of discrimination. The contexts where these discriminatory episodes occurred most frequently were breaktimes, group play and class activities. A clear experience of discrimination was reported by Jeronimo in his second interview. He said that his peers did not accept him in soccer matches because of his ‘mouth’ referring to his lip differences. However, in other cases, the link between exclusion or rejection and social labels was less explicit. Many of those who reported mockery and restrictions in their social interactions linked their social struggles to peer's bad mood and rude behaviors, instead of discrimination. For example, talking about the reasons for being ‘mostly alone’ in the breaktime. One girl mentioned a strict hierarchical system of play restricting her from being part of playing groups: Well, sometimes they [peers] make a circle and talk between them… and then… when they have a decision… someone says to me: “no, you can’t play ‘cause I’m the boss and I decide who can play and who can’t” …’
(Carolina 7 year old girl with CL/P)
Similar to Carolina, Isa linked her difficulties in making friends to the complexity of managing her peers’ emotions: Interviewer: ‘OK, tell me how do you make friends?’
Isa: ‘It's difficult;
Interviewer: ‘Oh really? Why?’
Isa: (long pause)
Interviewer: ‘What's the most difficult part of making friends?’
Isa: (lengthier pause) ‘Someone gets angry with me and… then we can’t become friends … I don’t play with anybody…I just go up, ‘cause my classroom is upstairs… and I take my lunch …I sit on the floor next to my classroom door.’
(Isa, 8 year old girl with CL/P)
Mica and Carlos also reported spending the breaktime alone. While Mica, 7-year-old with CL/P, related a more direct example of discrimination during breaktime of peers’ insulting her by calling her ‘stupid’, Carlos, a 10-year-old with CL/P, related more subtle social exclusion in that he did not have ‘too many friends’ to be with in the recess.
Self- Stigma
Given their experiences with mockery, many participants were aware that their speech and facial differences might contribute to negative social responses, such as name calling. This awareness often led to feelings of shame and concerns about how they would be appraised by others particularly within new social encounters. For example, Marcos, Coni and Dilan reported feeling ‘nervous’ about negative social responses about their physical appearance and speech during their first days at school.
Anxiety and anticipation of negative responses made some children avoid social interaction, particularly instances in which they had to speak. Feeling ‘embarrassed’ about speaking, Dilan narrated how he avoided speaking with peers in the nursery when he was younger, which resulted in limited social interaction: (Doing his life story book and seeing family photos)
Interviewer: ‘What about bad life times, have you had any bad time in your life…do you remember one?’
Dilan: ‘Uhmm when uhmm this one [points out a nursery photo-he is dressed up for the nursery graduation ceremony] when I was a baby…
well, uhmm ‘cause … I mean I didn’t like that time, uhmm I felt shame,,,
well, because I didn’t… I didn’t speak to anyone”
Interviewer: ‘You didn’t?’
Dilan: ‘I didn’t, I just played by my own.’
(Dilan, 10 year old boy with CL/P)
Participants anticipated social negative judgments in the common actions of speaking with others and meeting new people. Dilan's feeling of shame about speaking to his peers suggests a lack of self-confidence, a frequent consequence of internalized stigma. 13
However, stigma-self-awareness seemed to equip some children to manage and resist stigma. Aware of stereotypes and negative public attitudes associated to his CL, 9-year-old Camilo narrated how he avoided conversations when other peers asked the reasons for his lip scar: Camilo: ‘…the other day a new child came to the school… he was like: “why do you have that (lip scar)?”’ [looking annoyed]
Interviewer: ‘What did you say to him?’
Camilo: ‘…I said: “ehh it's a scar” and I walked away …’
Interviewer: ‘Why did you walk away? Don’t you like to talk about that?’
Camilo: ‘…well…with you I feel safe. But with other people.. uhmm no at all …‘cause talking about this with them (peers) uhmm… they’re too gossipy!’ [grabbing his face to show annoyance].
Camilo's narrative illustrates how, by regulating information about his cleft, he felt he protected himself from potential negative comments. Likewise, Isa's and Marcos’ awareness that their visible differences could be the target of mockery made them keep features of their cleft and treatment as private aspects of themselves. (Additional results related to how children resist and manage stigma are presented in a separate paper).
Children's awareness of some labels made them feel supported. ‘Being special,’ a term 11-year-old Lina, who was born with syndromic CL/P, used in reference to her speech difficulty, held a positive meaning for her. Lina explained that being special meant that she could have help from peers when teachers did not understand her speech: Lina: ‘Sometimes… well uhmm… when they [teachers] dońt understand what I say …for example some new teachers dońt know me very well … so they [peers] repeat to them what I said.’
Interviewer: ‘Oh ok… do you like that?’ [having help from peers when the teacher does not understand her speech]
Lina: ‘Yeah! I do… that means they [peers] are listening to me and they understand me when I speak!.’
For Lina, being ‘special’ meant that she could have support from peers when she was struggling with communication, something that made her feel heard and feel more confident in her communication. This potentially led her to feel more, rather than less, socially included.
Discussion
Despite the awareness that children and young people with different types of orofacial clefts face stigma,2,5,24,41,42 there is a lack of research about children's experiences with these complex social dynamics and a better understanding can help healthcare providers to address children's and young people's needs. This child-centred study responded to this gap by offering a detailed exploration of children's experiences of stigma in the light of two concepts: the stigmatization process 26 and self-stigma, also known as stigma self- awareness or self-consciousness. 14
Children's narratives show that stigma entails a complex, multi-component process with negative impacts on their social lives. The process of stigmatisation included the construction of labels and stereotypes, such as speech difficulties, nose shape and lip differences being identified (labelling) and appraised negatively by peers (stereotyping). Within this process of status loss, examples from the participants illustrated that those in the stigmatized group (them) are deemed less valuable and competent by the stigmatizer, reducing them ‘from a whole and usual person to a tainted and discounted one’ 43 (p3). Status loss can have a negative impact on people's opportunities, mostly notably access to education, employment, social relationships and support.15,44 Echoing this, this study demonstrates how children who are labelled and stereotyped also experience social interactional issues: difficulties in making friends and belonging to play groups. Although most of the participants did not explicitly link their social issues with labels and stereotypes towards their bodily differences, it is important to remember that social othering and discrimination often occur in subtle forms that create social distance.45,46 It is also important to note that labels and stereotypes are not only constructed on physical and functional differences such as post-surgical scars, nasal shape and hypernasal speech, but also include other differences, such as participating in speech therapy. Providers need to be mindful of how efforts to address differences can also contribute to stigma in some cases. Furthermore, it is also important to examine whether and how cleft-related stigma impacts on children's involvement in treatments and therapeutic adherence. 47
Interventions operating at the intrapersonal level such as those focused on enhancing coping strategies of stigmatized groups may increase people's self-esteem and sense of belonging. 48 Additionally, addressing misconceptions and taboos about the origin of orofacial clefts can be the focus of intervention aimed at social norms on both interpersonal and structural levels.
Anticipating and fearing labels, stereotypes and exclusion, some children may avoid social interaction particularly in instances where their differences are likely to be assessed negatively, such as speaking with peers and new social encounters (eg, start of school term). This is reflective of how self-stigma leads to feelings of anxiety, shame and subsequently avoidance of socio-relational encounters.13,49 Self-presentational concerns about appearance are commonly experienced by people with visible facial differences who internalize stigma. 50
Colombia has made significant progress in making policies and programs to promote and ensure social inclusion of communities that have been historically discriminated against.51,52 Despite this strong legislation in theory, the participants’ experiences of stigma raises questions about the extent to which this policy of inclusion is effectively implemented in practice. It is worth highlighting that children did not speak of teachers’ actions to minimize or penalize mockery or name calling. This denotes an absence of school strategies to educate peers about differences. Future research could explore the extent to which policies of inclusion are being effectively implemented in the school context.
The complexity of stigma illustrated throughout this paper highlights the corresponding complexity in designing and implementing strategies to tackle these social dynamics. Children's experiences of stigma occurred at three main levels: individual (self-awareness stigma), interpersonal and institutional (peer culture, school). This suggests that cleft-related stigma prevention and response needs to be operationalized at multiple levels. There is clearly a need to involve multiple sectors and disciplines (eg, education, governments, policy makers, public health, social sciences, medicine) to generate and ensure more inclusive social structures. 52
Strengths and Limitations
The most significant contribution of this research is the characterization of children's experiences of stigma in a global south setting, drawing on their own stories and accounts. This is both a novel aspect and key contribution of this study as the views of children and young people with this condition remain underexplored within orofacial clefts research and clinical practice. We have also demonstrated that children can talk about aspects of their lives by their own and able to engage in research if appropriate methodological approaches are used.
This research has some limitations. This study was conducted within a global south setting (Colombia) and as such within a particular socio-cultural context. Given that health-related stigma and their effects on people's lives may vary with social-cultural contexts 53 the stigma experiences discussed in this paper might not reflect young people groups from other parts of the world. The limited generalisability of the findings particularly in the global north, it is also a call for further work which examines stigma elsewhere. In addition, the data was interpreted through two theories of stigma that may not be applicable across settings. This research focused on exploring children's experiences, rather than examining the influence of education levels, cultural and socio-economic locations on their experiences. Future research should aim to examine the impact of structural factors such as the role of socio-cultural location on how stigma is experienced on how stigma is experienced.
Conclusion
In conclusion, this study furthers understanding of stigma related to CL/P drawing on children's own accounts. It also demonstrates how the complex social dynamics of stigma adversely affects children's social interaction and their opportunities to form relationships. Healthcare practitioners and policy makers can help address the potential consequences of stigma for individuals with a cleft at micro, macro, and meso levels.
Footnotes
Acknowledgements
Special thanks go to the participants and their families for their time, trust and openness to share their stories. We would also like to thank the administrative staff, the social worker, speech therapists, psychologists and consultants of Operation Smile Colombia for their help and support during the recruitment stage of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.