
Abstract
Keywords
Introduction
Lower lip clefts were first reported in 1819 by Couronne. 1 Tessier 2 published a comprehensive description of craniofacial clefts (Insert Fig 1), which is widely accepted today. In this classification, he had described a mandibular midline cleft and numbered it as 30, assuming there may be clefts that may be discovered later, radiating from the central lower lip.
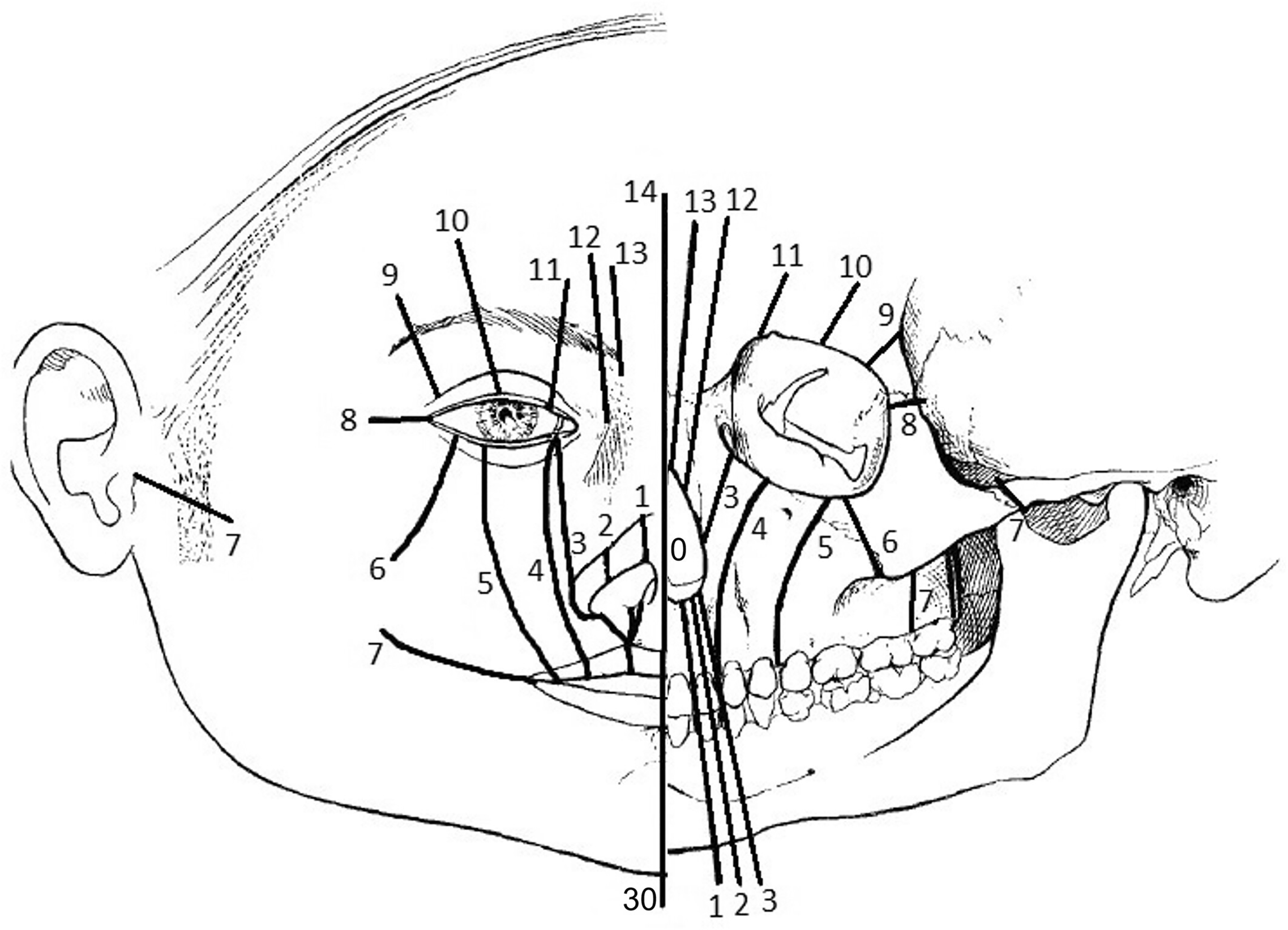
Tessier classification of craniofacial clefts.
Mandibular clefts are extremely rare, and less than 100 cases have been reported in the literature. 3 Only four others have reported paramedian clefts of the lower lip of varying degrees, and the reports are few and far apart.4–7
Moreover, of the previous reports of paramedian clefts of the lower lip, only one other 7 did not give a history of association with any syndrome or boney involvement. In this case report, we reveal the second case of an isolated paramedian cleft of the lower lip.
Case Report
A one-year-two-month-old male patient presented to us with both parents complaining of a discontinuity of the lower lip on the right side. There were no other complaints of poor weight gain, missing teeth in the lower jaw, congenital cardiac anomalies, breathing or hearing difficulties or any other features suggestive of a cleft palate. All developmental milestones were achieved as per the timeline. (Insert Image 2)

Preoperative pictures.
The parents do not give any history of clefts or syndromes in the family or any history of consanguinity.
The pregnancy was realized after five months of amenorrhea in a 22-year-old female. The mother gives a history of taking oral Aceclofenac on twelve occasions for recurrent headaches and was even given two intra-muscular doses of Diclofenac for the same. When the headaches did not resolve after conservative management, the neurologist advised a computed tomography (C.T.) scan of the brain, which was reported as normal.
Antenatal supplements were started only after the diagnosis of the pregnancy after 20 weeks of gestation.
The child was delivered at 35 weeks+2 days of age through an emergency caesarean section due to reduced foetal movements. The child had respiratory distress for the first 13 h of life, for which he was placed in an oxygen hood and tapered. Then, the child was stabilized and shifted to the mother's side.
On the third day of life, the patient's abdomen ultrasound revealed a mild dilatation of the right pelvicalyceal system and ureter due to the vesiculo- ureteric system and left undescended testes.
Brief Description of the Cleft and Management
A full thickness cleft of the lower lip was located to the right of the midline. It presented as a discontinuity of the red line and notching of the vermilion. The white roll was continuous but there was a mild peaking at the site of the cleft. The extent resembled that of a microform cleft.
There was also a supero-inferior discrepancy in the height of the vermilion and the lower lip at rest was mildly shifted to the left. The underlying boney continuity was maintained.
The child was operated under general anaesthesia. Zs were marked on the mucosal surface and a back cut on the skin surface to break the scar and slightly rotate the lesser segement. The markings for the vermilion were done, preserving as much dry vermilion as possible to ensure sufficient bulk. Few abnormal muscle attachments to the mucosa were dissected, and muscles were re-oriented and sutured. The mucosa and skin were closed using resorbable sutures. The triangles of the Z on the mucosal surface were interposed in order to correct the supero-inferior deficiency of the vermilion. (Insert Images 3–5)

Z-plasty for mucosa to correct supero-inferior discrepancy.

Back cut for skin.

1 week post operative pictures.
The child was discharged after an overnight observation. The results were satisfactory as is seen in the post operative images (Insert online image 6).
Discussion
Mandibular midline clefts are a rare entity and may vary significantly in the extent of the deformity ranging from a simple notch in the vermillion to a complete cleft of the lip involving the tongue, the chin, the mandible, the median supporting structures of the neck and the manubrium sterni. 8 Paramedian clefts are an even rarer entity, with only 4 cases described in the literature.4–7
The etiology of the paramedian cleft has several hypotheses. The most accepted model of lower lip development hypothesizes the merging of the mandibular processes of the 1st pharyngeal arch in the midline, between the fifth to seventh week.
Warbrick 9 (1952) hypothesized that the mandible consists of three depressions during the embryological period. Any disturbance in the formation of the process causes these depressions to persist, leading to a paramedian cleft. This theory resonates with the theory of epithelial augmentation by mesodermal migration.
Oostrom 10 hypothesized during the early embryonic period (<17 mm crown rump length), the mandibular processes occur as outgrowths of the 1st pharyngeal arch which is the only arch that develops during this period. The mandibular processes do not fuse but merge during the late embryonic period (17–60 mm crown rump length) during which the formation of the lip, alveolus, mandible and symphysis occur and any disturbance during this time may cause lower lip/ mandibular clefts of varying degrees.
Another theory was given in 2012 in a histological study of a human foetus with bilateral clefts of the lower lip, Vastradis 11 et al. suggested that developmental events occurring in the lower lip region are overlooked and may not occur in a manner similar to the mandible. On the 32nd day post conception, there are four prominences which can be seen in the region of the future lower lip—2 anterior and 2 lateral. Each of these are separated by a groove. By the 38th post conception day, the 2 shallower lateral furrows disappear due to underlying mesenchymal proliferation. The lack of this proliferation and fusion of the lateral process to the anterior center could possibly result in paramedian clefts of the lower lip.
A second theory is the Amniotic Band Syndrome 12 (A.B.S.), wherein bands in the amniotic fluid constrict around the foetus resulting in slits, necrosis or amputation of organs. This may occur even at a later stage of embryonic development. The malformation's severity varies—ranging from a cutaneous fissure to life-threatening visceral malformations. However, there are no other compatible findings of A.B.S., such as amputations or hand or foot malformations in our case.
Stapedial artery hematoma was hypothesized as a cause in the most recent report of a paramedian cleft of the lower lip. 7 However, it is unlikely that it would result in only a mild clefting of the lower lip and as rightly stated, it is more an effect than a cause.
The only other report of the isolated paramedian cleft of the lower lip describes a pregnancy during which a multi-fetal pregnancy reduction was carried out and attributes this as the cause for the cleft of the lower lip, stating that the introduction of transabdominal/ transvaginal needles during the pregnancy could be to blame.
To delve into the etiology of our case—we think it may be multifactorial. The mother has consumed non-steroidal anti-inflammatory drugs (N.S.A.I.D.s) during her early pregnancy. Several studies 13 link in early pregnancy to orofacial clefting, which could be a possible and most likely, cause.
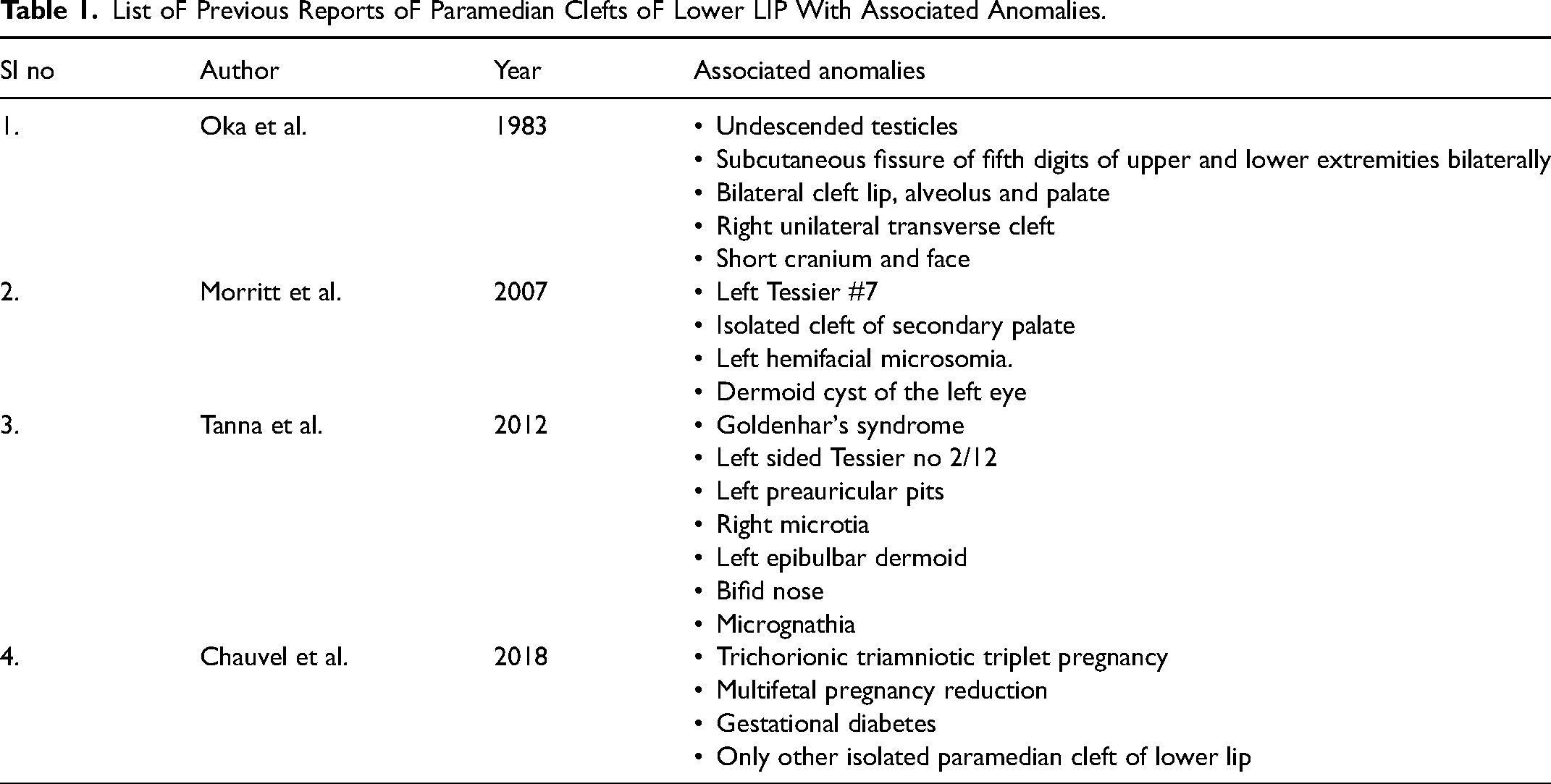
She was also exposed to radiation during the first trimester. Moreover, she was unaware of the pregnancy until the 5th month and was also not on antenatal supplements until the fifth month. All these factors compounded may have contributed to the etiology of this cleft (Table 1).
List oF Previous Reports oF Paramedian Clefts oF Lower LIP With Associated Anomalies.
Conclusion
The authors present the second report of an isolated atypical paramedian soft tissue cleft of the lower lip with a brief description of the possible etiology of this cleft along with its surgical management.
Footnotes
Consents
Valid written consent to publish this case report was obtained from the caregiver.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.