
Abstract
Objective
To perform a morphometric analysis of the upper cervical spine (UCS) by means of cone-beam computed tomography (CBCT) for the diagnosis of malformations or craniocervical instabilities in patients with cleft lip and palate (CLP) and class III malocclusion.
Materials and Methods
A total of 72 CBCTs from adult patients (48 male and 24 female) with Angle Class III malocclusion were divided into three groups: 1) Unilateral cleft lip and palate (UCLP) (n = 29; male = 65.5%; age = 24, 2 ± 4.2 years); 2) Bilateral cleft lip and palate (BCLP) (n = 18; male = 83.3%; age = 26.4 ± 6.0 years); 3) Control group (CON) (n = 25; male = 56.0%; age = 27.8 ± 9.3 years). The version 11.7 of the Dolphin® software (Chatsworth, California, USA) was used to evaluate the morphometric measurements and anomalies of the UCS. Data were analyzed by descriptive and inferential statistics (p ≤ 0.05).
Results
For the UCLP, BCLP and CON groups, respectively, the measures were: atlantodental interval (2.1 ± 0.5; 2.1 ± 0.4; 2.0 ± 0.3 mm), basion-opisthion (35.9 ± 3.2; 36.4 ± 3.0; 34.7 ± 1.9 mm), hyoid-C3 (34.5 ± 3.7; 34.5 ± 5.2; 35.3 ± 4.5 mm), and hyoid-sella (108.1 ± 9.8; 111.3 ± 9.2; 109.7 ± 10 mm); clivus-canal angle (152.3 ± 13; 150.3 ± 10; 150.7 ± 10°) and Torg-Pavlov index (1.0 ± 0.2; 1.0 ± 0.1; 1.1 ± 0.2). Potentially unstable anomalies and malformations were more prevalent in the UCLP group (34,4%).
Conclusion
Subjects with UCLP presented compressive or unstable anomalies on upper cervical spine, more frequently than controls and BCLP, despite the lack of statistically significant differences among groups. Future studies could increase the safety of patients and healthcare professionals specialized in craniofacial anomalies.
Keywords
Introduction
Cleft lip and palate (CLP) are the most prevalent craniofacial anomalies affecting 0.45 each 1.000 life births. 1 Aesthetic alterations, breathing problems, speech difficulties, maxillofacial deformity, hearing disorders and psychosocial issues are associated to CLP. 2 A higher occurrence of bony anomalies on upper cervical spine (UCS) in subjects with CLP has been reported by several authors.3–5
There is still no agreement related to the occurrence of UCS deformities in CLP patients. However, the most frequently mentioned is the fusion, that occurs when a specific vertebral unit has an abnormal bony junction with other vertebrae. Also, among the abnormalities with failure on UCS segmentation, the Klippel-Feil syndrome (KFS) stands out, in which the congenital fusion of multiple cervical vertebrae, can be associated to CLP. 6
Another anomaly is the posterior arch deficiency, also known as spina bifida, described as a failure on the formation of vertebral spine posterior element (spinous process and lamina). There are reports showing that the prevalence of these malformation on the cervical spine may be up to three times higher in CLP patients, especially in unilateral cleft lip and palate patients (UCLP). 7
Previous study, based on cephalography, described the presence of 64.5% of UCS malformations in patients with CLP and up to 63% of vertebral fusion in bilateral cleft lip and palate patients (BCLP). 8 On the other hand, another report, using the same methodology, showed that 19.29% of cleft patients, presented cervical vertebrae anomalies, while only 4.4% of the general population had anomalies of craniovertebral junction. In addition, Uğar et al. (2001), in a sample composed by 111 subjects with CLP, identified that 18.2% presented cervical vertebrae anomalies; highlighting that 10 subjects showed more than one anomaly. Posterior arch deficiency was found in 7.7% and fusion in 12.1%. Regarding the non-cleft sample, 9.1% showed cervical vertebrae anomalies, 5% posterior arch deficiency and 4.1% fusions. 9
Due to the high anatomical complexity, the UCS images may be wrongly interpreted if they are not analyzed by professionals properly trained. The tomographic three-dimensional studies enable a complete evaluation of bony structures of the UCS. 10 Nevertheless, in a study that the UCS of patients with CLP was evaluated by CBCT, the only significant difference observed was a higher incidence of subdental cartilaginous remnants in BCLP patients. 11
Cleft treatment includes an extensive series of surgeries, in which, hyperextension of the cervical spine is often required. Some UCS malformations, especially the atlantoaxial dislocation (AAD), when exposed to prolonged cervical hyperextension, can lead to severe neurological damage.12–14 Therefore, it must be highlighted the necessity of a greater understanding of the occurrence of UCS malformation in CLP patients.
Materials and Methods
The present study was approved by Institutional Review Board of the Hospital for Rehabilitation of Craniofacial Anomalies - University of São Paulo, USP Brazil.
For this retrospective study, cone-beam computed tomography were obtained at Hospital for Rehabilitation of Craniofacial Anomalies - University of São Paulo, USP Brazil, and selected during the period of June 6th, 2021, to June 11th, 2022.
A total of 72 CBCTs were analyzed from a sample composed by patients with Angle Class III malocclusion (48 male and 24 female), distributed in three distinct groups:
Control Group (CON): 25 tomographies (male: 56.0%; medium age: 27.8 ± 9.3 years) with Angle Class III maxillomandibular discrepancy and without cleft. Unilateral Cleft Group (UCLP): 29 tomographies (male: 65.5% medium age: 24.2 ± 4.2 years) with unilateral incisive trans-foramen cleft. Bilateral Cleft Group (BCLP): 18 tomographies (male: 83.3%; medium age: 26.4 ± 6.0 years) with bilateral incisive trans-foramen cleft.
All patients presented Angle class III malocclusion, which is characterized by mandible protrusion (prognathism), maxilla retrusion, or a combination of these components.
15
For the inclusion of the CBCTs on the study, the following criteria were taking into consideration: subject with complete skeletal maturity, Angle Class III maxillomandibular discrepancy and absence of evident syndrome. Adequate visualization of the UCS vertebrae C1, C2 and C3, and the cranium base, represented by the basion and opisthion point (Figure 1).
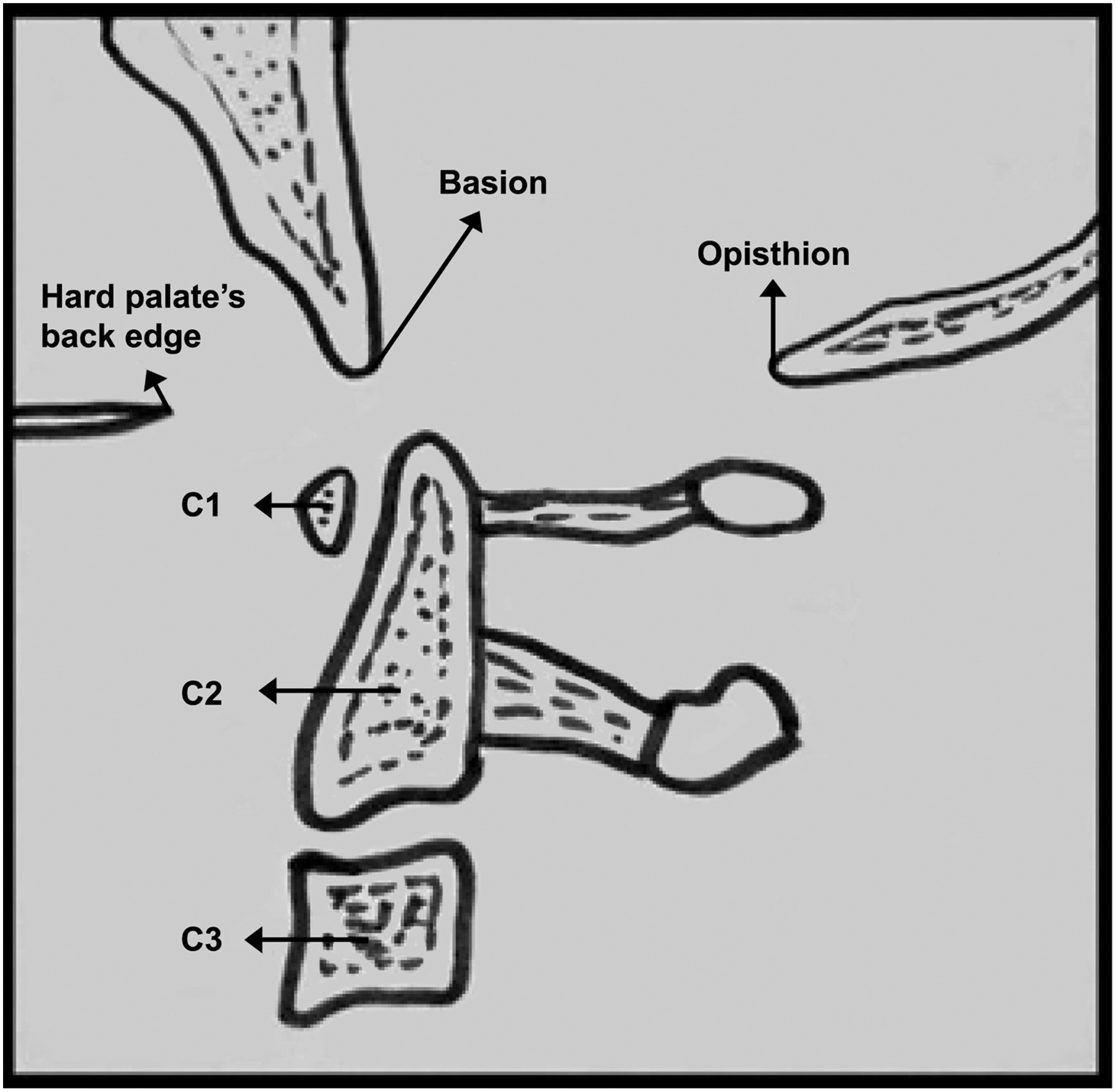
Anatomical points of the cranium base and the upper cervical spine vertebrae.
The cone-beam computed tomography images were obtained by the ISI-iCAT Imaging System (Next Generation i-CAT® Norwood, Massachusetts, USA). Tomographic studies had the following specifications: 0.25 voxels resolution, 13 cm of vision field and 26.7 s of exposition time, 120Kv, 37.07 mA, in DICOM format (Digital Imaging and Communications in Medicine). For the measurements, Dolphin software version 11.7 was employed (Dolphin Imaging, Chatsworth, California, USA). All CT scans were requested by members of medical and dental staff for clinical reasons. An orthopedic surgeon, specialist in spine surgery, evaluated all CT scans in two different moments, with a minimum interval of two weeks. The mean results of each measurement were considered for statistical analysis.
The CT scans evaluations were performed through subjective visual analyses, and by anatomical measurements objectively. The following descriptive parameters were analyzed: basilar impression, congenital stenosis of cervical canal, fusion of the vertebrae posterior arch, fusion failure of the vertebral bodies, segmentation failures of vertebral bodies and the presence of instability between the cranium base and the first and second cervical vertebra. Additionally, the following objective measurements were performed:
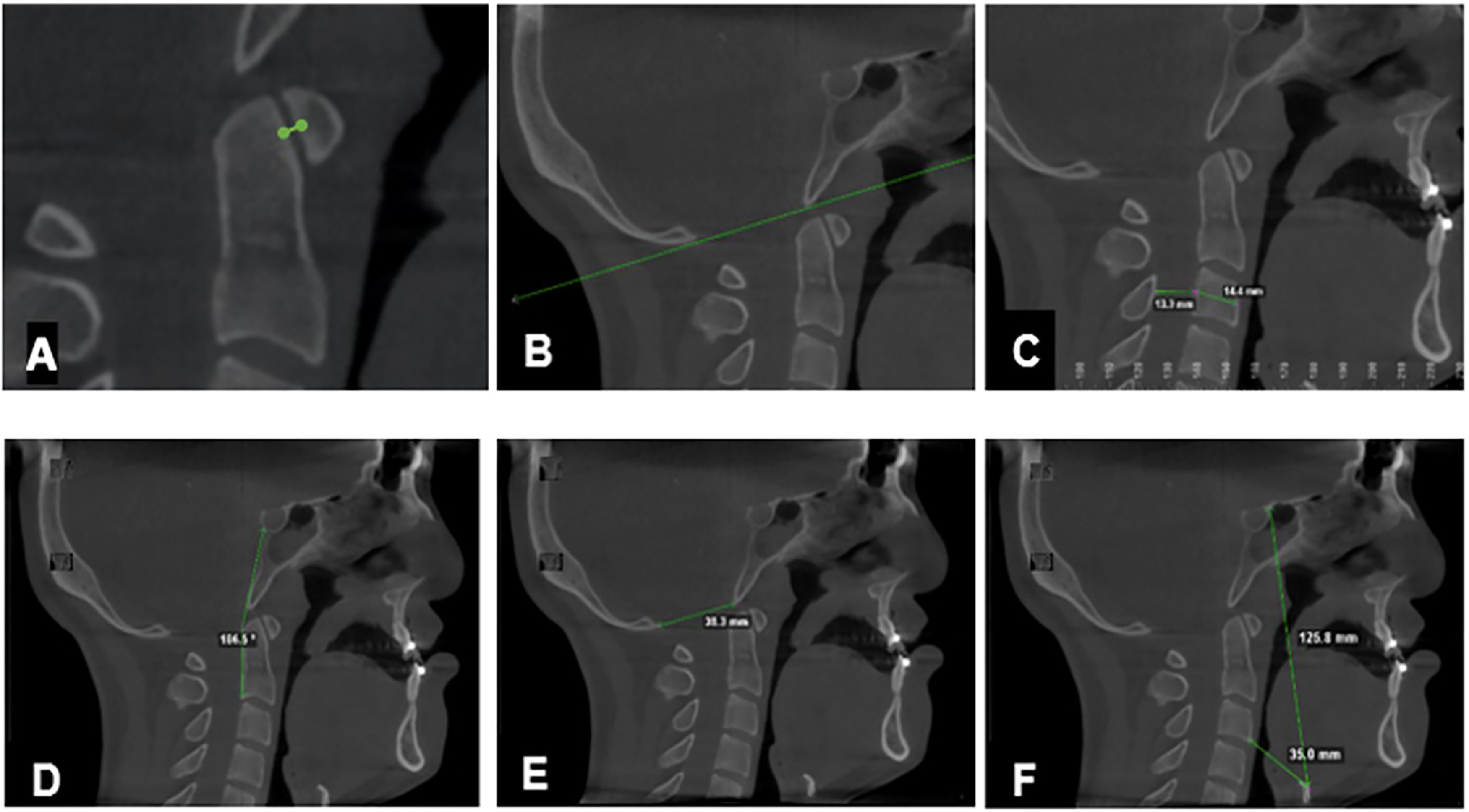
Anatomical measurements. (A) Atlantodental interval (ADI), (B) McRae line, (C) Torg-Pavlov Index, (D) Clivus-canal angle (CCA), (E) Distance between the basion inferior point to the inferior opisthion point (foramen magnum), F) Distance measured from the sella turcica up to the upper-anterior polo of the hyoid bone and, the distance between the lower-anterior polo of C3 and the upper-anterior polo of hyoid bone.
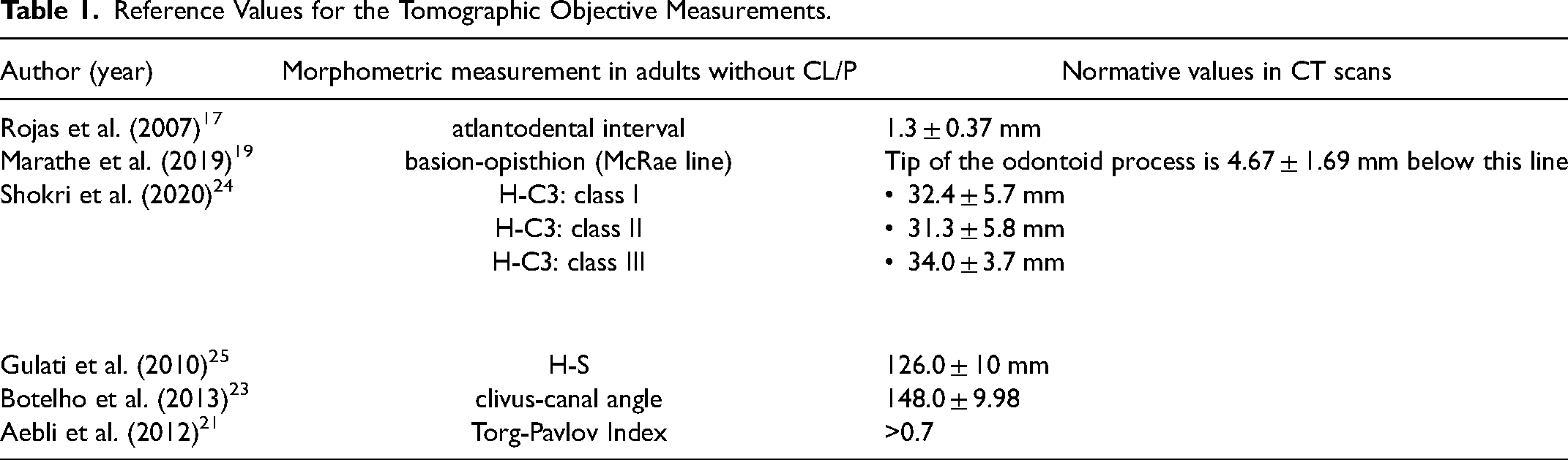
Reference values and examples of the objective measurements performed are depicted in Table 1 and Figure 2 respectively.
Reference Values for the Tomographic Objective Measurements.
All the data and measurements were obtained in two different times (T1 and T2), with a minimum interval of two weeks on from the other. The reproducibility between evaluations was calculated by the Intraclass Correlation Coefficient – ICC 26 which used the following punctuation: ICC < 0.40; weak agreement, ICC 0.4-0.75; moderate agreement and ICC > 0.75 strong agreement.
Comparison between groups, were analyzed by the ANOVA test (data with normal distribution). The differences detection by means of multiple comparations among groups was assessed by Tukey test. For the normal qualitative variables, the association was assessed by the Chi-square test (P < .05).
Results
No significant statistical differences were observed regarding the morphometric variables among the groups. For the UCLP, BCLP and CON groups, the measures were, respectively: atlantodental interval (2.1 ± 0.5; 2.1 ± 0.4; 2.0 ± 0.3 mm), basion-opisthion (35.9 ± 3.2; 36.4 ± 3.0; 34.7 ± 1.9 mm), hyoid-C3 (34.5 ± 3.7; 34.5 ± 5.2; 35.3 ± 4.5 mm) and hyoid-sella (108.1 ± 9.8; 111.3 ± 9.2; 109.7 ± 10 mm); clivus-canal angle (152.3 ± 13; 150.3 ± 10; 150.7 ± 10o) and Torg-Pavlov Index (1.0 ± 0.2; 1.0 ± 0.1; 1.1 ± 0.2).
The clivus-canal angle analysis showed that only one patient with basilar impression had an average angle of 143.8°; all other presented angles higher than 150°, without any characteristic of basilar impression or Arnold Chiari Syndrome. Only one patient showed CCA extremely high (average 192.9°); due to a gross deformity of the clivus.
Atlantodental interval (C1-C2) instability analysis depicted that, two patients from the UCLP group showed measures above 3 mm, which can be classified as possible craniovertebral instability (6,9%). From the total of 72 CBCTs evaluated, nine showed potentially unstable anomalies on UCS (12,5%).
Although the Torg-Pavlov index average did not present significant difference among groups, a total of six patients were diagnosed with absolute congenital stenosis of the vertebral canal, two patients were from the CON group (8%) and four from the UCLP (13,8%). No alterations were observed on the BCLP patients.
Regarding the basilar invagination, in only one patient from the BCLP group (5,5%), the McRae line was exceeded by the odontoid process of the second cervical vertebra (Table 2).
Compressive or Unstable Anomalies Observed on Upper Cervical Spine.
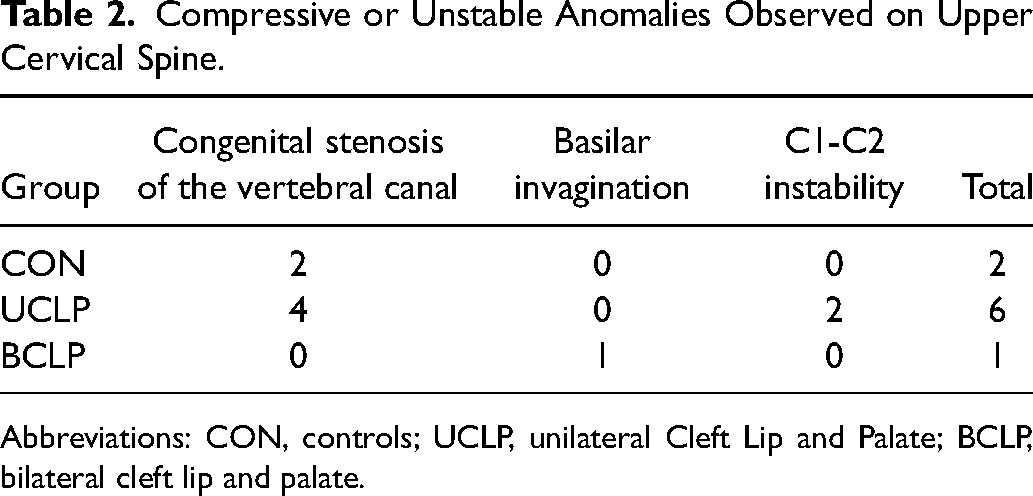
Abbreviations: CON, controls; UCLP, unilateral Cleft Lip and Palate; BCLP, bilateral cleft lip and palate.
Regarding the evaluated malformations, in CON group only one patient showed closure failure of C1 posterior arch (4%). In UCLP group, four patients showed UCS malformations (13,8%), such as one closure failure of C1 posterior arch (3,4%), two clivus deformity (6,8%) and one segmentation failure type KFS with fusion of C1-C2 (3,4%). Among the patients of BCLP group, two of them (11,1%) showed three UCS anomalies such as one double segmentation failure type KFS that was a fusion of C3-C4 and C4-C5 with absence of C1 anterior arch (5,5%), other a single segmentation failure type KFS that was fusion of C2-C3 (5,5%). (Table 3). Considering that 48 individuals included in the study presented CLP, the percentage of unstable anomalies, regarding specifically only patients with CLP, were for the UCLP e BCLP group respectively 12,5% and 2%.
Upper Cervical Spine malformations.
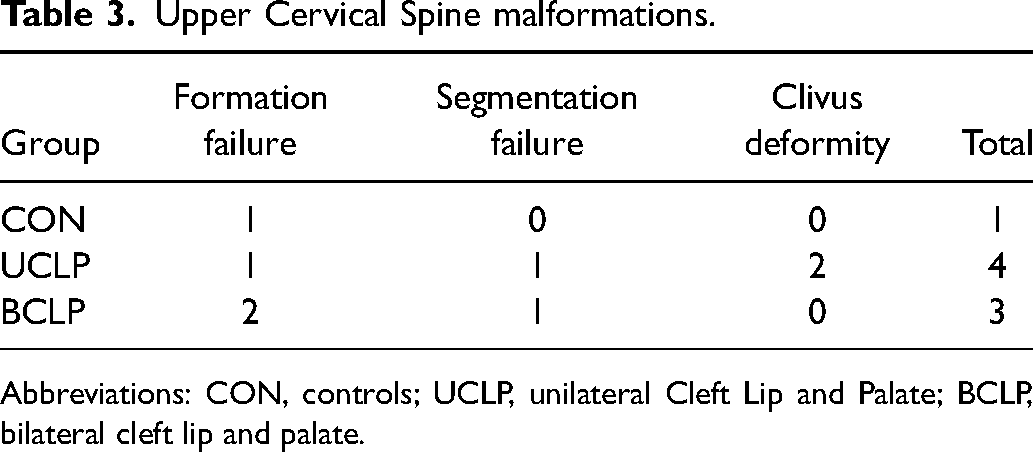
Abbreviations: CON, controls; UCLP, unilateral Cleft Lip and Palate; BCLP, bilateral cleft lip and palate.
Discussion
The association between CLP and UCS anomalies is based on the embryogenesis of the involved structures. Clinical studies and metanalyses reported on literature, observed that subjects with CLP have higher probability to present UCS deformity.5,7,9,27 On a systematic review conducted by Berrocal et al., 28 the most frequent anomalies were posterior arch deficiency, followed by cervical spine fusion.
In order to investigate the presence of UCS deformities in patients with CLP, the preferential method should be the CBCT. Compared to traditional computed tomography (CT), CBCT has a shorter exposure time, and lower radiation dose; and in comparison, with lateral cephalograms, despite a higher radiation dose, CBCT has an increased image quality, which is relevant for areas with high anatomical complexity, like the cervical spine.29–32 Computed tomography has also higher diagnostic specificity (100%) than lateral cephalograms (36%) for atlanto axial dislocation (AAD) diagnosis.13,14,32 The cost-effectiveness, ability to be performed rapidly, high sensitivity, and specificity make Computed Tomography the ideal screening tool for the assessment ADI measurements and AAD occurrence.17,32
On the present study, 12.5% of CLP subjects showed potentially unstable anomalies on UCS, within the range reported on literature (4.1%—38.67%).5,7,9,11,27,31 The primary outcome was to evaluate not only the anatomical and developmental aspects, but also verify the presence of compressive and unstable anomalies with a potential risk of neurological damage, during the surgical procedures, such as congenital stenosis of vertebral canal, basilar invagination and C1-C2 instability. These anomalies, in surgeries that demands UCS hyperextension, can lead to the development of trans-operatory neurological injuries.12–14 Patients with AAD, that can occur in prolonged neck extension, tend to be asymptomatic, although they can present local pain with restriction of neck movements, sphincter disturbances, myelopathy, lower cranial nerve palsy, respiratory distress, quadriplegia or death if not treated.12–14 On a study performed by Aebli et al., 21 congenital stenosis of the vertebral canal evaluated by the Torg-Pavlov index, was identified as risk factor for acute medullar injury, after a small trauma on the cervical spine. These potential and severe neurological deficits highlight the relevance of cautious evaluation of the UCS in patients with CLP.
The basilar invagination is another anomaly of the craniovertebral junction that can be congenital or degenerative, in which the odontoid process prolapses on the limited space of the foramen magnum and can also lead to neurological damage. Although frequently observed on the rheumatoid arthritis, it is most seen in congenital conditions such as the Chiari malformation, syringomyelia, Klippel-Feil syndrome and hydrocephaly, and it can cause severe compression of the spinal medulla. 33 On the present study, one patient of BCLP was identified with basilar invagination.
Regarding objectives measurements, one could argue that the head position during CT scans could have affected the atlantodental interval (ADI) values and, therefore, could not be compared definitively to the norm. However, the ADI is normally constant in distance during movement of the head. 13 The distance from the anterior node of the atlas to the dens, is normally lower than 3 mm in adults, and this distance varies by less than 1 mm with neck flexion or extension.13,14 According to Rojas et al., 17 CT scans, with patients in neutral position, ADI was found to be normal when it was lower than 2 mm in both sexes (1.3 ± 0.37 mm). In this context, we could consider that our ADI measurements were appropriately obtained, in neutral position, using the cutoff values proposed in the literature. The present study was retrospective in design and no CT scans were taken for research purposes only. It is of paramount importance to highlight that despite some patients presented ADI values above the cutoff value, the participants did not complained of symptoms related to atlantoaxial dislocation, by the time of their medical appointments, as registered in their charts, that justified any further investigation of cervical pathologies.
The rationale of measuring hyoid bone position lies on the fact that Hyoid-Sella and Hyoid-C3 distance shows the superior-inferior, and anterior-posterior position of this bone in relation to craniofacial landmarks easily identified through CT scan analysis. These anatomical boundaries could be assessed to detect modifications in the orthostatic biomechanics between hyoid bone and cervical spine; and compensatory interrelationships with the stomatognathic system regarding the function and stability of the craniomandibular system.34–36 In addition, hyoid bone position in the sagittal plane is linearly correlated with motion of the head, jaw and vertebrae. It relates closely to the curvature of the cervical spine (lordosis, straight or kyphosis), and its position with regard to the cervical column showed less variability than the hyoid position relative to the maxilla and the mandible. 34 In the present study no correlations could be performed between ADI and H-C3, and H-S due to the sample size. One of the study limitations, lies on the reduced sample size and the retrospective design. However, it must be highlighted the homogeneity of the sample regarding age, body mass index, type of occlusal pattern (class III). Additionally, all CBCT scans were performed in the same equipment with a standardized protocol. Future prospective studies with a uniform distribution of cleft subtype, and clinical follow up, with neurological pre and postoperatively evaluation, can clarify the clinical relevance of routinely UCS evaluation in patients with CLP.
Conclusion
Subjects with UCLP presented compressive or unstable anomalies on upper cervical spine, more frequently than controls and BCLP, especially considering congenital stenosis of vertebral canal and C1-C2 instability, despite the lack of statistically significant differences among groups; whilst the BCLP group, presented the only case of basilar invagination. Careful preoperative assessment through CBCT and management of UCS of patients with CLP should always be employed, especially in surgeries that require cervical hyperextension.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by CAPES PRODOC and Universidade de São Paulo.