
Abstract
Objective
To assess the effect of secondary alveolar bone grafting (SABG) on maxillary growth in patients with unilateral cleft lip or palate (UCL/P)
Design
Systematic review and Meta-analysis
Methods
Pubmed, Cochrane Library, Embase, Scopus, Web of Science and manual search was performed to assess the maxillary growth following SABG in UCL/P patients
Patients and Participants:
Non-syndromic patients with UCL/P
Main Outcome Measure:
Comparison of maxillary growth between patients with UCL/P who underwent SABG and UCL/P patients who had not undergone SABG or non-cleft control
Results
39 of the identified 233 articles were assessed for inclusion and exclusion criteria after duplicate removal and title and abstract reading. 7 articles (1 prospective, and 6 retrospective studies) were included in the qualitative analysis and 2 articles were subjected to quantitative analysis. Four studies had a low risk of bias and three studies had a moderate risk of bias. Meta-analysis revealed a significant reduction of SNA and no significant difference in ANB in the SABG group compared to the non-cleft control group(I2 = 0%). There was no significant difference in ANB between SABG and non-cleft control; however, results showed high heterogeneity(I2 = 83%). Meta-analysis of SNA and ANB showed no significant difference between SABG and the cleft control group; however, there was high heterogeneity.
Conclusions
The studies showed a low to moderate risk of bias. SABG causes inhibition of maxillary growth in patients with cleft lip or palate when compared to patients with non-cleft control. Due to high heterogeneity, comparison to cleft control showed insufficient evidence.
Introduction
Cleft lip or palate (CL/P) is one of the most common craniofacial deformities in humans resulting due to failure of fusion of maxillary and medial nasal processes. 1 The risk factors responsible include gene anomalies involving IRF6, CH8q24, VAX1, FGFR2, BMP4, maternal risk factors, smoking, alcoholism, pre-gestational diabetes, gestational diabetes, maternal age >40 years, folate deficiency, zinc deficiency, teratogens such as valproic acid, phenytoin, retinoic acid and pesticides. 2
Protocols define the sequence and timing of the procedures including pre-surgical orthopaedics, lip surgery, primary closure of the alveolar defect, palate repair, ENT monitoring, speech therapy, orthodontic treatment, alveolar bone grafting (ABG) and revision surgeries and their importance in the management of patients with cleft lip and palate. 3
Alveolar bone graft has become a cornerstone procedure in the overall management of patients with cleft lip and palate. ABG is utilized to fill the bony gap, provide sufficient bone for eruption, stabilize the overall dental arch, provide bony support for the teeth adjacent to the cleft area, close the residual oro-nasal fistula, establish a nasal skeletal base, floor of the nose, functional nasal airway; and provide adequate bone stock for the future placement of an osseointegrated dental implant in cases where the permanent lateral incisor is missing. 4 Based on the timing, the ABG can be classified as either primary (<2 years of age), early secondary (2–5 years of age) or secondary (>5 years of age). 5 Grisius et al. 6 modified this classification by adding early secondary (2–5 years), secondary (6–12 years), and late secondary (>12 years) ABG. Tsuha M, et al. 7 defined early SABG at 4 to 7 years of age before the eruption of lateral incisors versus late SABG at 8 to 12 years of age before the eruption of maxillary permanent canines”.
Primary alveolar bone grafting has been associated with restriction of anterior–posterior maxillary growth and hence has less preference than secondary alveolar bone grafting.8–10 In these children, retrusion of the midfacial skeletal, dental and soft tissue occurs and becomes more obvious over time as the surrounding structures develop. 11 This midface retrusion can result in compromised facial aesthetics, dental arch relationships and speech. However, there is also concern regarding the effect of SABG on maxillary growth. Postsurgical scar tissue in the lip and/or palate of cleft patients inhibits the normal growth of the maxilla after undergoing SABG.12–14 Early secondary ABG resulted in slight constriction of the maxillary dental arch.15,16 Brattström et al. 17 and Levitt et al. 18 reported that alveolar bone grafting resulted in impaired maxillary growth and suggested that it would be preferable to delay ABG procedure after 9 years of age. On the contrary, Shi and Losee 14 and Gesch et al. 19 stated that SABG did not produce obvious surgery-related inhibition of the maxillary growth. Timing of SABG was also a factor in the restriction of maxillary growth, according to Fudalej et al., 15 performing an early secondary ABG around 6 years of age, compared with 9 years of age, could potentially compromise maxillary growth similar to primary ABG.
To date, there is insufficient evidence regarding SABG which assessed the skeletal tissue, soft tissue and dentoalveolar changes during maxillary growth and development in patients with cleft lip or palate. Hence, the purpose of the systematic review is to investigate the effects of secondary alveolar bone grafting on maxillary growth and development in patients with cleft lip or palate.
Material and Methods
Registration of Protocol
The systematic review was carried out following the preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines and registered with the international prospective register of systematic reviews (PROSPERO) with the registration number (CRD42021249061).
Eligibility Criterion and Study Selection
The PRISMA flow diagram gives an overview of the selection process (Figure 1). The articles that assessed the maxillary growth and development following secondary alveolar bone grafting (SABG) on non-syndromic patients with cleft lip or palate were included for review. All skeletal tissue, dental tissue and soft tissue growth parameters were assessed and compared to control groups. Studies that have evaluated primary, tertiary and quaternary alveolar bone grafting were excluded.
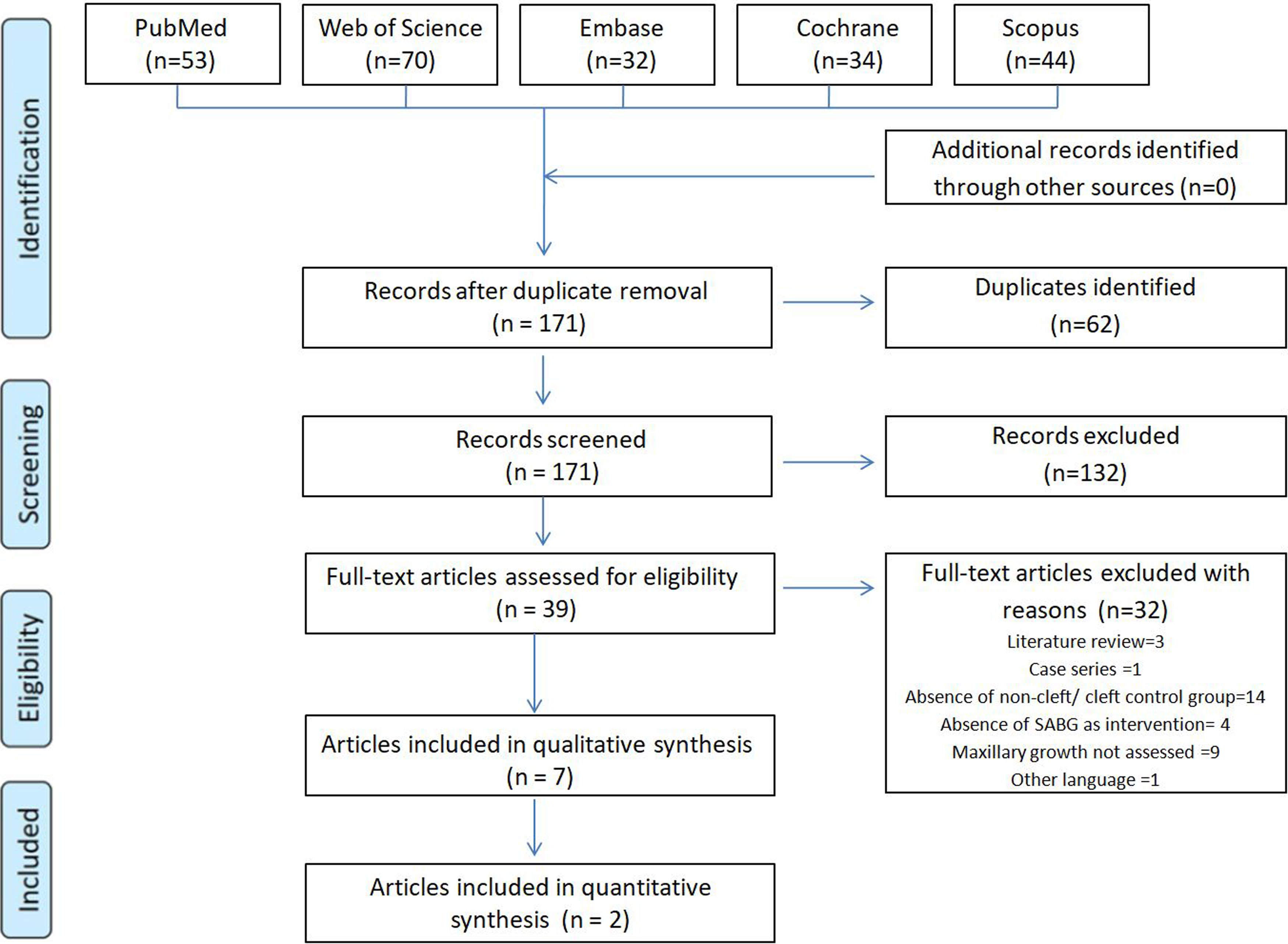
PRISMA flow diagram of study selection.
All the eligible randomized clinical trials, quasi-randomized studies, and prospective and retrospective studies were included. The case reports, case series, descriptive and preliminary studies, in vitro studies, abstract papers, review articles, studies without control patients, patients with syndromes, and studies published other than in the English language were excluded from this systematic review.
Information and Sources
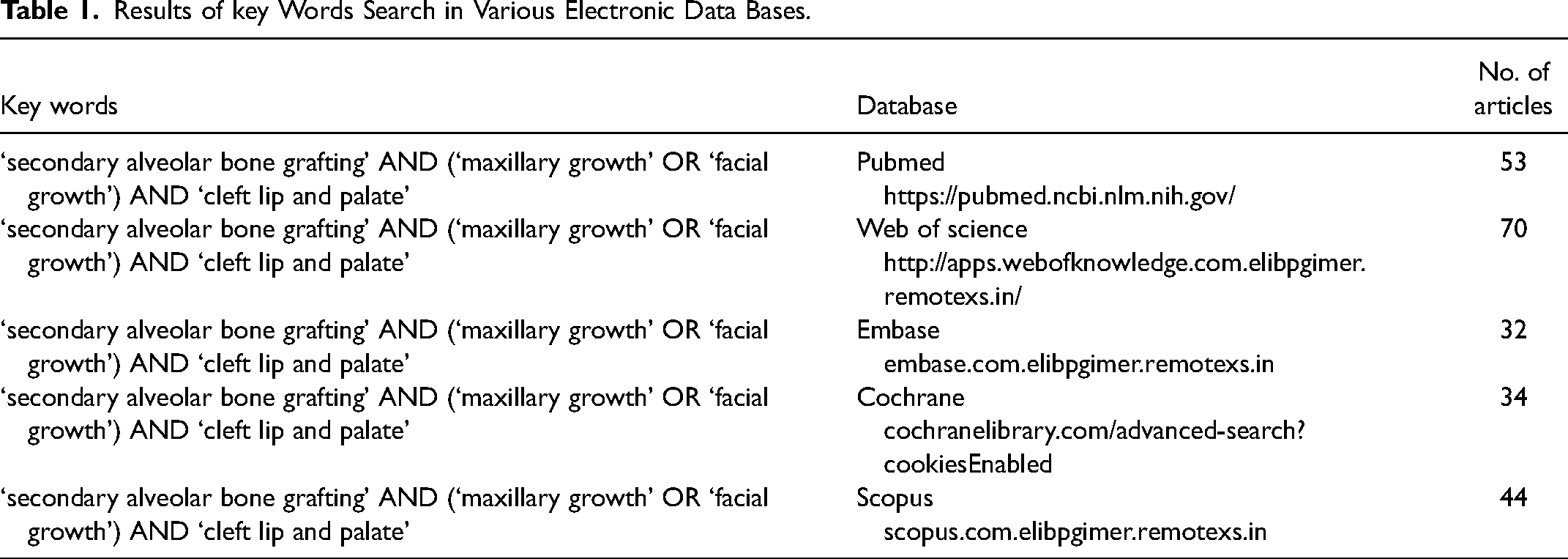
The systematic review includes the literature search from the electronic databases viz. Pubmed, The Cochrane Library, Embase, Scopus, and Web of Science as the primary sources until 31st April 2022. The “Medical Subject Headings (MeSH) terms” included were “secondary alveolar bone grafting”, “maxillary growth”, “facial growth”, “cleft lip and palate”, midface growth”, “craniofacial development”, “craniofacial morphology”, “facial form”, “nasomaxillary growth”, and “facial development”. The electronic search was supplemented with a manual search.
Search Strategy
The relevant articles obtained from key words search in various electronic databases were included after the title and abstract search followed by the removal of duplicates. The relevant articles were selected by the 2 calibrated reviewers independently according to the agreed criteria. The articles were included in the review according to the inclusion and exclusion criterion after full-text reading. The inclusion/exclusion criteria were discussed between the two reviewers and the resolution of disagreements was done by a discussion with a third investigator to resolve any issues. The search process and inclusion of articles were thus done after evaluation by two investigators independently as depicted in Figure 1. Table 1 shows the search strategy of various electronic databases. A manual search supplemented the rigorous electronic search by 2 investigators involved and calibrated.
Results of key Words Search in Various Electronic Data Bases.
Quality (Risk of Bias) Assessment
Two examiners evaluated the risk of bias and the quality assessment in individual studies using ROBINS-I Tool. 20 Seven domains of bias were evaluated which included confounding bias, bias in the selection of participants into the study, bias in the classification of interventions, bias due to deviations from intended intervention, bias due to missing data, bias in the measurement of outcomes and bias in the selection of reported result. The overall risk of bias was calculated according to the risk of bias in each domain.
Data Extraction
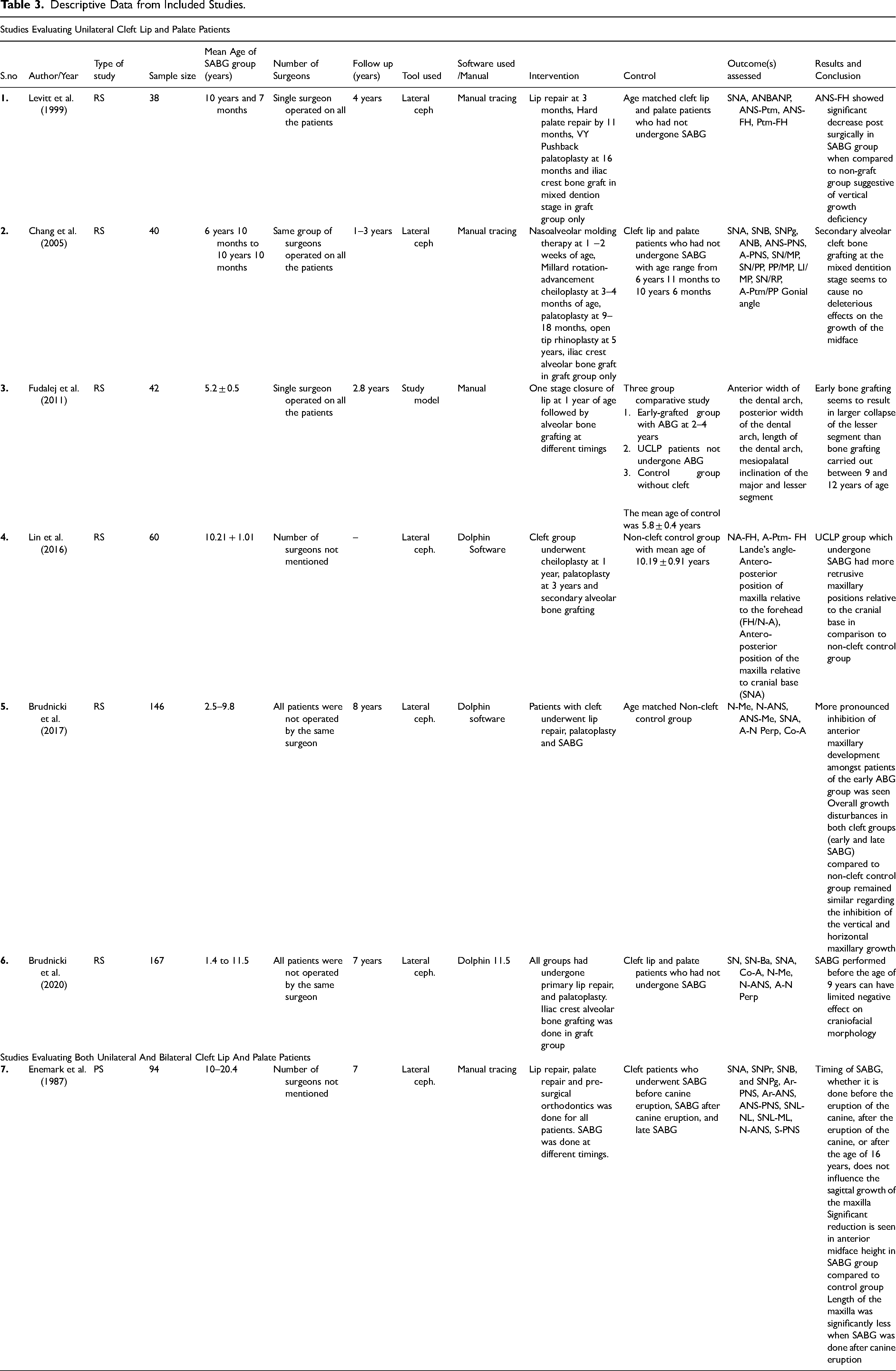
The data extraction was done by two reviewers independently. The following data were collected from included studies: authors; year of publication, study design, sample size; control sample, methods of measurement, follow-up time; age range, gender, result and conclusions. The parameters taken for the comparative evaluation were changes in skeletal tissue, soft tissue and dental tissue. Descriptive data of the included studies as depicted in Table 2.
ROBINS-1 Tool (Sterne et al. 2006) for Quality Assessment.
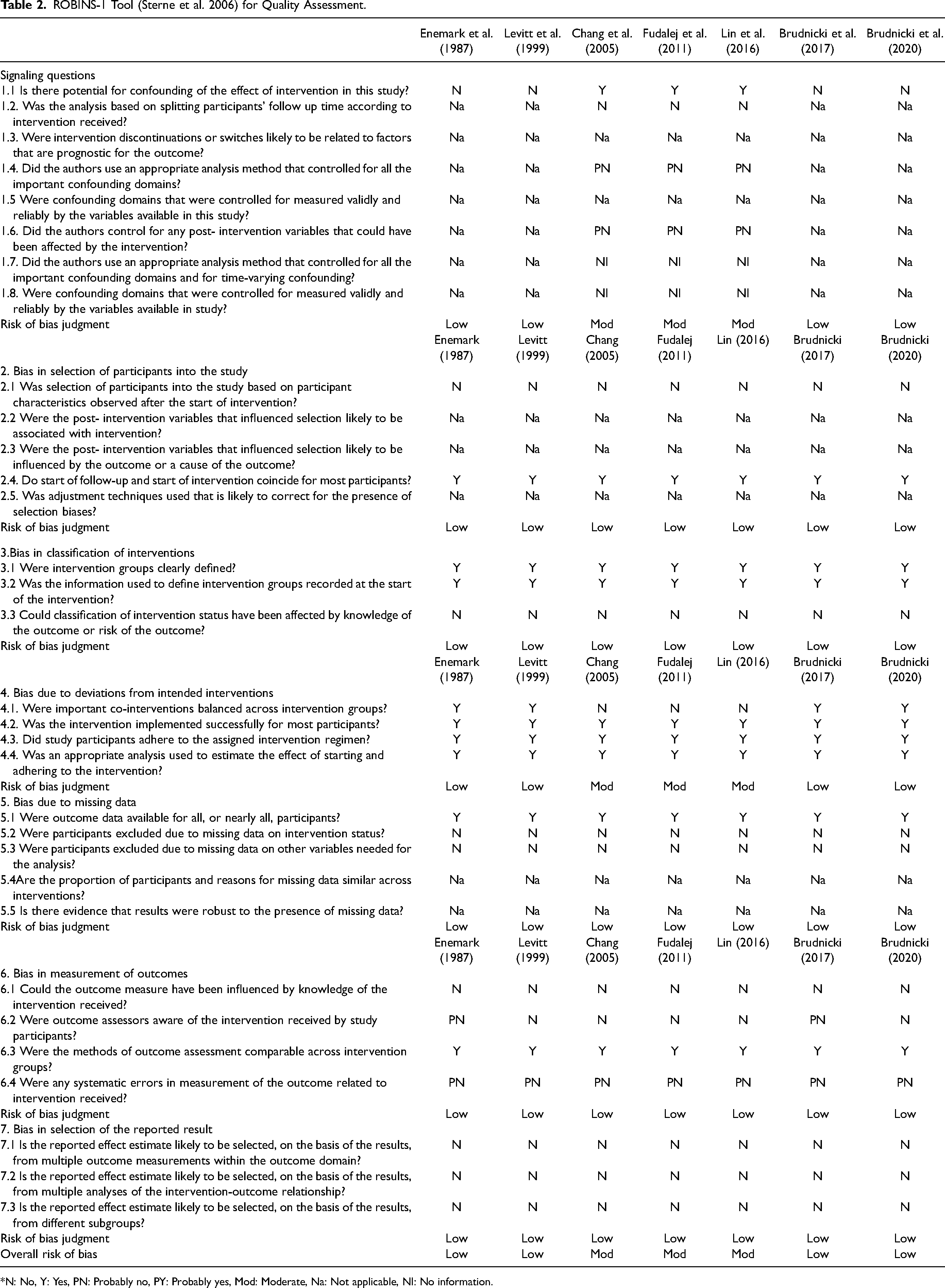
*N: No, Y: Yes, PN: Probably no, PY: Probably yes, Mod: Moderate, Na: Not applicable, NI: No information.
Data Analysis
Data were statistically pooled and meta-analysis was performed using Review Manager (RevMan), Version 5.3. Copenhagen: The Nordic Cochrane Centre, the Cochrane Collaboration, 2014. The Mean Difference (MD) and Standard Error (SE) of individual studies were combined using the inverse variance weighted approach. The trials with comparable interventions, subjects and outcomes were pooled and Mean Differences (MD) with their associated 95% confidence intervals (CI) were chosen to express results as an effect measure. The treatment effect was weighted (weighted mean difference (WMD) using calculations based on a random effects model. Wherever heterogeneity was high, sensitivity analysis was performed.
Results
A total of 233 articles were identified from various databases based on the keywords given in Table 1. 62 articles were removed as duplicates. The independent reviewers found 132 articles non-relevant to the topic. A total of 39 articles were selected after the removal of duplicates and title and abstract reading. Out of 39, three were literature reviews, 1 case series, the control group (cleft/ non-cleft) was absent in 14 articles, maxillary growth was not assessed in 9 studies, SABG was not the intervention group in 4 articles and 1 article was in a language other than English. Seven articles were selected after the full-text examination. Seven studies including six retrospective studies and one prospective study was included in this review. Six studies used lateral cephalograms for comparison whereas the study by Fudalej et al. 15 was conducted on study models. All the studies have mentioned that the investigators who evaluated the lateral cephalogram and models were calibrated except the study by Enemark et al. 21 There were no randomized clinical trials which satisfied the inclusion criteria. The parameters used for quantitative assessment were soft tissue, dental and skeletal changes on lateral cephalograms and dental changes on study models. Most of the studies have mentioned the protocol of surgical lip and hard palate repair. Table 3 shows the details of the procedures conducted in patients enrolled in the studies included in the review before SABG. Fudalej et al. 15 and Brudnicki et al. 22 mentioned in the studies that presurgical orthopaedics was not used in any of the patients. Chang et al. 21 reported that all the infants underwent nasoalveolar molding at 1 to 2 weeks. The studies by Chang et al. 21 and Enemark et al. 20 reported orthodontic treatment (transverse correction) before SABG. The aim of SABG as reported by most of the studies was to provide support for cleft-adjacent teeth, to stabilize the maxillary segments, to support the alar bases, and to enable expansion of the inter-premaxillary suture
Descriptive Data from Included Studies.
Risk of Bias Assessment of Selected Studies
Two examiners evaluated the risk of bias and the quality assessment in individual studies using ROBINS-I Tool. 19 Four studies had low risk of bias and three studies had moderate risk of bias. The level of evidence was found to be fairly good. There were no concerns regarding the applicability of the selected articles. No articles were eliminated after the ROBINS-I Tool application.
Changes in Maxillary Growth Between SABG and Cleft Control Patients
Enemark et al., 20 Levitt et al., 17 Chang et al. 21 and Brudnicki et al. 22 compared the changes in maxillary growth in patients with cleft lip and palate with and without SABG as shown in Table 3. According to Levitt et al. 17 and Chang et al., 21 there was a non-significant decrease in SNA and ANB between SABG and the cleft control group. The study by Brudnicki et al. 22 found that SNA was lesser in patients with cleft who had undergone SABG in comparison to the cleft control group suggestive of more maxillary retrusion in the SABG group.
Meta-analysis of two studies (Chang et al., 21 Brudnicki et al. 22 ) was performed to assess the mean difference in linear measurements (SNA, ANB) between SABG and Cleft Control group. Figure 2A shows a forest plot of the combined results for SNA. The results showed no significant difference in SNA between the SABG and cleft control group (MD = -1.16; 95% CI = -4.01 to −0.99). However, this outcome showed high heterogeneity (I2 = 74%). Figure 2B shows a forest plot of the combined results for ANB. The results showed no significant difference in ANB between the SABG and Cleft control group (MD = -0.52, 95% CI = -3.73 to 4.77). However, this outcome also showed high heterogeneity (I2 = 89%).
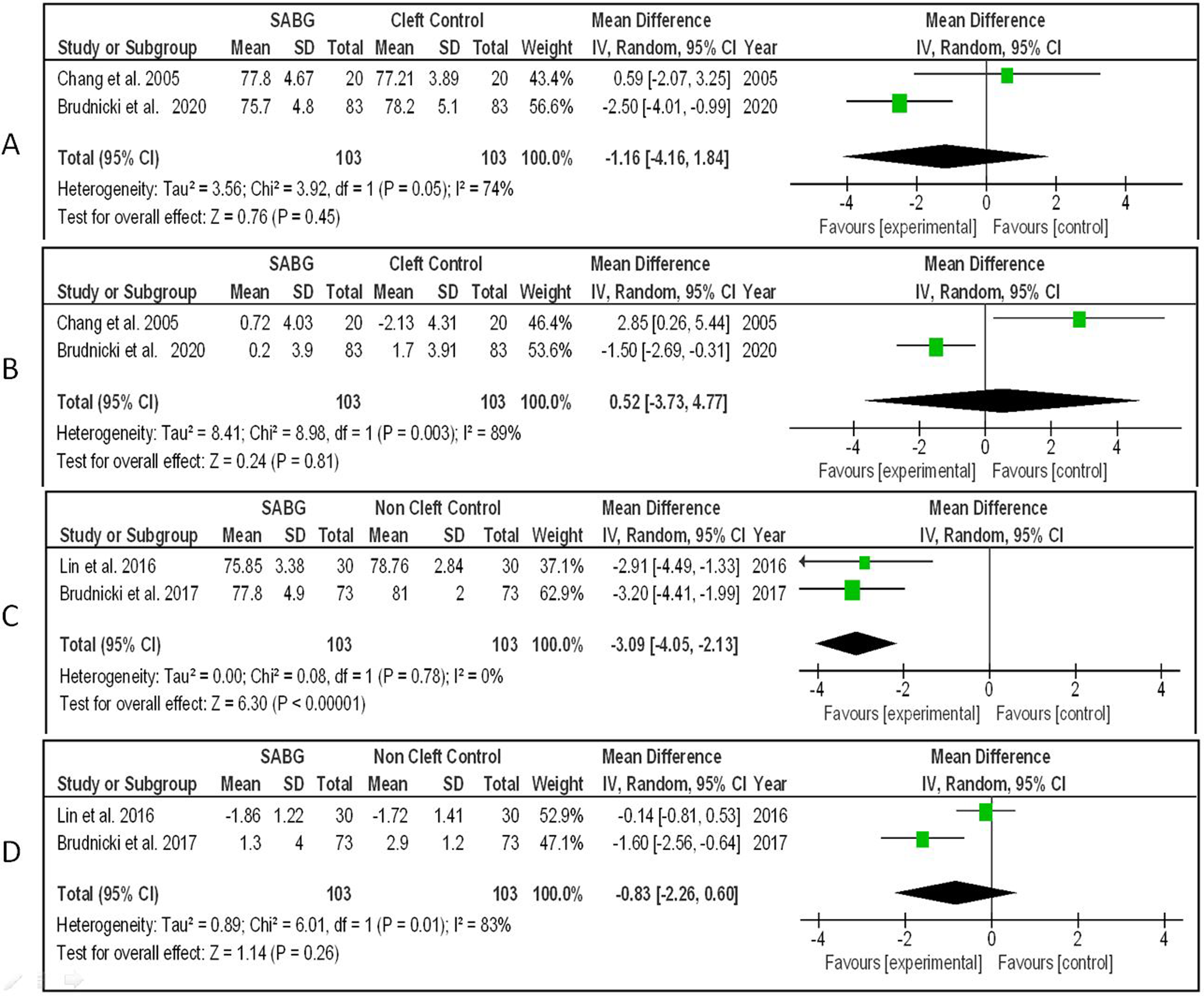
A. Forest plot comparing SABG and cleft control for SNA; 2B: forest plot comparing SABG and cleft control for ANB; 2C: forest plot comparing SABG and non-cleft control for SNA; 2D: forest plot comparing SABG and non-cleft control for ANB.
Chang et al. 21 and Brudnicki et al., 22 found a non-significant decrease in the mean differences in the ANS-PNS between SABG and cleft control group. Levitt et al., 17 showed significantly decreased changes in the sagittal linear parameter; ANP (Point A- Nasion Perpendicular distance) in the SABG group compared to the cleft control group. The vertical linear parameters ANS-Ptm and ANS-FH decreased and Ptm- FH increased non-significantly in the SABG group compared to the cleft control group. Chang et al. 21 found a decrease in ANS-PNS in the SABG group in patients with UCLP. Enemark et al. 20 assessed patients with UCLP and BCLP and showed a non-significant increase in SNA and a significant increase in N-ANS in patients with SABG performed before and after the canine eruption in comparison to the cleft control group whereas in the study by Brudnicki et al., 22 there was a decrease in N-ANS in SABG group in comparison to cleft control group.
Changes in Maxillary Growth Between SABG in CLP Patients and non-Cleft Control
Lin et al. 23 and Brudnicki et al. 24 have evaluated the changes in maxillary growth between SABG in UCLP patients and non-cleft control as depicted in Table 3. According to Lin et al. 23 and Brudnicki et al. 24 there was a significant reduction in SNA between SABG and non-cleft control group. According to Brudnicki et al. 24 there was a significant reduction in ANB between SABG and the non-cleft control group while in the study by Lin et al., 23 the reduction in ANB was non-significant.
Meta-analysis of two studies (Lin et al., 23 Brudnicki et al. 24 ) was performed to assess the mean difference in linear measurements (SNA, ANB) between SABG and non-cleft control group. Figure 2C shows a forest plot of the combined results for SNA. The results show a significant trend of SNA reduction in the SABG group in comparison to the non-cleft control group (I2 = 0%) (MD = -3.09, 95% CI + -4.05 to −2.13). Figure 2D shows a forest plot of combined results for ANB. The results showed high heterogeneity (I2 = 83%) and no significant difference of ANB between SABG and non-cleft control (MD = -0.83, 95% CI = -2.26 to 0.60).
In the study by Lin et al., 23 there was a significant reduction in N-A, A-Ptm, and FH/N-A between SABG and the non-cleft control group. In the study by Brudnicki et al., 24 there was a significant decrease in N-ANS, A-N-Perp and Co-A in the SABG group in comparison to the non-cleft control group.
Fudalej et al. 14 compared SABG to both cleft control and non-cleft control. The inter canine width, length of the dental arch, inclination of major segment and inclination of lesser segment significantly increased in non-cleft control while there was a significant reduction when SABG was performed. The intermolar width was significantly increased when SABG was performed at 9–11 years. The intermolar width was decreased in non-cleft control but was statistically non-significant. This search shows the sparse availability of studies on the assessment of maxillary growth after SABG.
Discussion
Secondary alveolar bone graft is a widely accepted procedure in the overall management of patients with cleft lip and palate providing sufficient bone for stabilization of the dental arch. However, the effect of SABG on maxillary growth is controversial. Enemark et al., 21 Lin et al., 24 Brudnicki et al. 25 and Bittermann et al. 26 reported that alveolar bone grafting resulted in impaired maxillary growth. On the contrary, Chang et al., 22 Shi and Losee, 14 Levitt et al., 18 Brudnicki et al. 23 and Gesch et al. 19 had found no surgery-related inhibition of the maxillary growth following SABG. Patients were followed up for 3 years in the studies by Levitt et al., 18 Chang et al., 22 and Fudalej et al. 15 Follow-up of 7 years was done in studies by Enemark et al., 21 Brudnicki et al. 23 and Brudnicki et al. 25
Studies by Meazzini et al., 27 Power and Matic, 28 Caganova et al. 29 and Jabbari et al. 30 evaluated the changes in maxillary growth between SABG and gingivo-alveoloplasty procedures in lateral cephalograms. According to studies by Meazzini et al., 27 Power and Matic 28 and Jabbari et al., 30 SNA was higher in patients who had undergone SABG than those who had undergone gingivo-alveoloplasty. The present systematic review was conducted as no systematic review and meta-analysis has investigated the effects of secondary alveolar bone grafting on maxillary growth and development in patients with cleft lip and palate.
Changes in Maxillary Growth Between Patients with Cleft lip and Palate with and Without SABG
In the study by Enemark et al., 21 there was a reduction in SNA in the SABG group compared to the cleft control group which might be attributed to the post-operative scar tissue as a restrictive factor for maxillary growth. Similarly, a reduction in SNA in the SABG group was also seen in studies by Levitt et al. 18 and Brudnicki et al. 23 Whereas Chang et al. 22 showed no significant changes in the SNA between the SABG group compared to the cleft control group.
Meta-analysis of two studies (Chang et al., 22 Brudnicki et al. 23 ) showed no significant difference in ANB between SABG and cleft control group and the results showed high heterogeneity. ANB depicts the maxillo-mandibular sagittal relationship. Forward maxillary growth is inhibited by post-operative scar tissue. Inhibited maxillary growth obstructs the forward growth of the mandible as well.
Chang et al. 22 and Enemark et al. 21 assessed the length of the maxilla between SABG and the cleft control group with contradictory results. In the study by Enemark et al., 21 the length of the maxilla was significantly increased in the SABG group compared to the cleft control group. This may be attributed to the early orthodontic treatment in the SABG group after surgery. However, in the study by Chang et al., 22 the length of the maxilla was higher in the cleft control group but was statistically non-significant. This could be attributed to the surgically induced scar tissue after SABG surgery which impaired maxillary growth.
Studies by Enemark et al. 21 and Brudnicki et al. 23 assessed the height of the maxilla between SABG and the cleft control group. Both studies revealed that the height of the maxilla was reduced in the SABG group compared to the cleft control group. The decreased vertical growth could be because of the extensive mobilization of the palatal mucosa during SABG surgery. Hence, maxillary growth appears to be reduced in patients with cleft lip and palate who had undergone SABG compared to patients who had not undergone graft procedures.
Changes in Maxillary Growth Between Patients with Cleft lip and Palate with SABG and non-Cleft Control Group
Lin et al. 24 and Brudnicki et al. 25 have evaluated the changes in maxillary growth between SABG in patients with CLP and non-cleft control groups. In the study by Lin et al. 24 SNA and ANB were reduced in the SABG group compared to the non-cleft control group which is similar to the study by Brudnicki et al. 25 Similarly, maxillary length and maxillary height were decreased in the SABG group compared to the non- cleft control group. Reduced values of SNA, ANB, maxillary length and maxillary height in the SABG group can be attributed to both altered growth potential in patients with cleft lip and palate in comparison to non-cleft and also to the inhibition of innate growth potential because of post-operative scar tissue formation. Brudnicki et al. 25 claimed that craniofacial growth potential in patients with a cleft is different and variable than in the population without a cleft. Lin et al. 24 suggested cleft defects, surgical trauma and scar contracture have significant negative effects on maxillary growth. This growth inhibition due to surgical trauma is similar in all patients of cleft lip and palate with or without SABG. Hence, maxillary growth appears to be reduced in patients with cleft lip and palate compared to non-cleft control. The differences in growth between cleft patients who received a bone graft and non-cleft patients may be due to intrinsic differences and not to the bone grafting procedure. The comparison with non-cleft control may not suggest the effect of SABG on growth appropriately. The patients with UCLP Class III compared with the noncleft Class III group showed no differences in any cephalometric measurements, thus concluding there may be other intrinsic factors responsible for maxillary retrusion than SABG. 31
The study by Fudalej et al. 15 compared the changes in the maxillary dental arch growth changes in patients with unilateral cleft lip and palate who had undergone SABG at different ages, non-cleft control group and Cleft Control. The inter canine width was the least when SABG was performed at 2–4 years. Intermolar width did not change significantly when SABG was performed at different timings. The length of the dental arch was the lowest when SABG was performed at 9–11 years. This might be attributed to the lower regeneration potential of patients at higher ages.
There may be differences in the growth for patients with cleft treated at different centres with variable surgical protocols. 32 The studies included in the review had different protocols for soft tissue closure, presurgical nasoalveolar molding, and orthodontic treatment before SABG. These confounding factors may be responsible for the difference in the growth response in patients from different centres.
Most of the studies suggested that early SABG had more deleterious effects on craniofacial growth than late SABG. Moreover, there is less skeletal retrusion after 9 years of age. One of the main objectives of SABG is also the eruption of lateral incisors and canines into the arch. Thus it is advisable to conduct SABG before the canine eruption to minimize skeletal effects and benefit the arch dimensions. According to Shetye PR 33 most of the vertical and transversal growth in the maxilla is completed by 7–9 years of age, so it may be recommended to evaluate each case after the eruption of central incisors concerning the space available for an eruption for lateral incisor and canines to decide the timing of bone grafting. It is also advisable to avoid the loss of any tooth and to plan SABG accordingly.
The advantage of the alveolar bone graft is to support the lateral incisor and eruption of the maxillary canine with the closure of oro-nasal fistulas which was confirmed in the SR and Meta-analysis. This SR confirmed that the surgical intervention and placing of SABG compromised maxillary growth when compared to a non-cleft control.
Thus the comparison of the growth of patients with cleft lip and palate with and without SABG is more viable. Table 2 included data from 1987–2020 in which techniques and operators have changed over the 33 years. Over the years surgical techniques have improved as has our expertise in the design and conduct of Systematic Reviews, RCTs and Meta-analyses.
Indeed data is heterogeneous, but there is an obvious trend in the selected papers (Table 3) which points out the more inhibiting effects of early bone grafting (4–7y) compared to later (8–12y). So, while we may not have the evidence to support the advantage of a later (8–12) SABG, we certainly do not have any evidence whatsoever that early (4–7y) is justified regularly.
Limitations
In this systematic review, language restriction was applied. Only English publications were included; thus, studies in other languages could be missing in this review. The follow-up period varied among the studies included in this review. There are no RCTs that investigated the long-term outcome of the procedure. Thus, future studies should be planned to assess the long-term effect of SABG on maxillary growth.
Conclusion
The studies showed a low to moderate risk of bias. Hence within the domain of this systematic review, it can be concluded that SABG causes inhibition of maxillary growth and development in patients with cleft lip or palate when compared with patients with non-cleft control. Due to high heterogeneity, comparison to cleft control showed insufficient evidence. RCTs on homogenous samples are required to draw conclusive evidence.
Footnotes
Ethical/consent statement
Is not applicable and not required.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.