
Abstract
Objective
Cleft lip repair (CLR) can be complicated by hypertrophic scar or keloid. Botulinum toxin type A (BTA) may improve postoperative scarring by reducing muscle tension and cytokine activity at the scar site. This systematic review analyzes the available evidence regarding the effect of BTA on scar quality after CLR.
Design
The search was conducted in 6 different databases in accordance with PRISMA guidelines (PubMed, Scielo, Embase, Scopus, Web of Science, and Cochrane) using “botulinum toxin” and “cleft lip” as keywords.
Setting
Academic hospital
Patients
Exclusive to patients who underwent CLR and BTA injection
Outcome measures
Mean visual analog scores (VAS), mean Vancouver scar scale (VSS), scar width, and BTA or CLR-related complications.
Results
Five studies for a total of 216 patients met inclusion criteria. Four studies reported on primary CLR during infancy while 1 study recruited older patients seeking revision. All patients had BTA (range: 1-2 units/kg) injected in the orbicularis oris muscle. One study documented BTA injections in additional perioral muscles. All 4 studies that measured scar width and had a saline control arm found a significant decrease in width with BTA injection. Improvement of VAS and VSS with BTA was reported in 3 of 5 studies and 2 of 5 studies, respectively. There were no reports of complications associated with BTA or CLR.
Conclusion
The existing studies support the use of BTA injection to improve scar quality following CLR with low concern for complication. Further investigations with a greater number of patients are necessary.
Introduction
Cleft lip is one of the most common congenital craniofacial malformations worldwide, with an estimated prevalence of 0.3 cases in every 1000 births. 1 Standard of care for patients with cleft lip in developed countries includes surgical repair, which is commonly performed between 3 and 6 months of age. Despite the development and advancement of various techniques, postnatal reconstruction of the upper lip inevitably results in a scar (Figure 1), portions of which may be perpendicular to the relaxed tension skin lines. 2

Bilateral complete cleft lip/palate (BCCLP): normal 5-year postoperative scar.
Cleft lip repair (CLR) can be complicated by the abnormal hypertrophic scarring (HS) (Figure 2). This undesirable postoperative result is more commonly observed in specific populations, with Asian and Hispanic patients reported to have 3 to 4 times the rate of 1-year postoperative HS compared to Caucasian patients. 3 HS may exhibit excessive erythema, elevation, widening, and stiffness; these issues are particularly problematic when they are located on visible parts of the body, most importantly the face. 4 Poor postoperative scarring after CLR can lead to revisional operations with further potential surgical risk, stress, and medical expenditures. 3 The mean cost of secondary revision for cleft lip in the United States was $8393 in 2009, and patients with private insurance were 71% more likely to receive additional surgical procedures than patients with Medicaid. 5 Therefore, interventions that improve postoperative scarring and reduce the need for secondary revisions would be of significant benefit to patients and society.

Bilateral complete cleft lip/palate (BCCLP): hypertrophic scar 9 month after primary repair.
Wound tension at surgical closure has been well-described to negatively impact healing and scar quality.4,6 Minimizing skin tension after CLR can be difficult in infants, as agitation and feeding may exacerbate the mechanical tension on the healing wound and aggravate scar formation. A variety of preventative modalities have been utilized independently or in combination, including presurgical orthodontia, postoperative microporous taping, silicone sheets, tissue adhesive, application of Logan's bow, and use of topical mediators.7,8
Secondary interventions to improve scarring following CLR have also been described. These techniques include, but are not limited to, CO2 laser and intense pulsed light therapy, fat grafting, percutaneous scar release by needle, injectable hyaluronic acid, intralesional steroid injection, scar massage, and surgical revision.8–10 Results have been mixed and the efficacy of these treatments is not universally acknowledged.
The medical use of botulinum toxin has been extensively explored in the literature since first described in 1978 in the treatment of oculomotor dysfunction. 11 Botulinum toxin type A (BTA) cleaves presynaptic SNARE proteins at neuromuscular junctions, leading to the inhibition of acetylcholine release into the synaptic cleft and transient paralysis of muscles. 12 It is suspected that the paralysis and chemo-denervation of treated muscles decrease the tensile forces acting on the wound.13,14 The reduced muscle activity also decreases the release of neuro-inflammatory mediators such as substance P, calcitonin gene-related peptide (CGRP), and glutamate, which can blunt the inflammatory response and reduce peripheral pain sensation. 12 Today, BTA is used to manage diverse pathologies including muscular dystonia, hyperhidrosis, bladder spasm, migraine headaches, and other forms of neuralgia.15–17
Following these descriptions of BTA for the treatment of medically functional problems, this intervention has since been applied to aesthetic issues. While BTA has been used to improve the appearance of facial rhytids since the 1980's, the concept of targeted muscle paralysis to improve scar quality was first promulgated in 2000 by Holger and associates using a primate model.14,18 In 2006, Tollefson and colleagues described BTA to improve postoperative scarring after CLR. 19 Following this report, a number of providers have documented their experience in using BTA to improve CLR-associated scarring. All these studies have involved relatively few patients and employed a variety of protocols. Therefore, the purpose of the current investigation is to systematically review these reports and provide potential guidelines for current use and future studies on the effects of BTA on scarring after CLR.
Methods
Search Methods
A systematic review of the literature was performed per the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines in the following electronic databases: PubMed, Embase, Scopus, Web of Science, and Cochrane library. The search strategy was conducted in February of 2022 using MESH terms and equivalents to “Botulinum Toxin” (or BOTOX, BoNT) or “Maxillofacial Abnormalities”, and “Cleft lip” (Scar).
Study Criteria and Selection
Original articles in English, Spanish, and Portuguese that reported outcomes of CLR using BTA were selected. Literature reviews, systematic reviews, meta-analyses, opinion articles, letters, and book chapters were excluded. Two independent investigators (H.H and P.M) performed the screening. Articles were first selected based on the abstract and titles relevant to the use of BTA and CLR. Each reviewer then performed a full-text evaluation of the remaining articles using inclusion and exclusion criteria. Conflicts were identified and resolved by the two authors, with input from the senior author (A.K.O.).
Review Software
The review and selection of articles were processed on Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org.
Data Extraction
The following data was extracted by two of the authors (H.H and P.M) from the included studies: Author/Year, Type of Study, Primary outcome, Location of Study, Number of Intervention Subjects, Number of Control subjects, Diagnosis, Primary Procedure, Surgical Technique, Gender, Mean Age at Surgery, Moment of Botox Injection, Dilution, Dosage. Inconsistencies of extracted data were checked by two additional authors (E.M.R and A.E.R).
Risk of Bias Assessment
Two authors (P.M and E.M.R) independently assessed the potential risk of bias of the studies included using the RoB 2.0 tool and MINORS criteria.20,21 RoB 2.0 tool assesses bias through a set of questions evaluating bias arising from the randomization process, deviations from intended interventions, missing outcome data, measurement of outcome, selection in reported results, and overall bias. The three categories of detected bias are low risk, some concerns, and high risk for bias. For the MINORS criteria, the ideal score is 24 for comparative studies so scores of 0-8 were defined as low quality, 9-16 as moderate quality, and 17-24 as high quality.
Results
Search Results
The initial literature search identified 1924 studies, of which 979 were unique (Covidence removed initial duplicate records and 1 duplicate was removed by the reviewers during abstract screening). The title and abstracts were reviewed and articles pertaining to the use of BTA for CLR were selected. Ultimately, a full-text review of 17 articles was completed. Following the exclusion criteria, 5 articles were deemed eligible (Figure 1).
Study Characteristics
The 5 studies included 216 patients of which 4 studies were randomized controlled trials (RCT) and 1 was a clinical study (Table 1). Four of the 5 studies reported outcomes after primary CLR2,22–24 while 1 reported on secondary cleft lip revision. 25 Three of the 5 studies described patients with unilateral cleft lip (UCL), accounting for 144 procedures,2,23,24 and 1 study did not specify the number of patients with either diagnosis. 25 For primary CLR, the mean age at surgical intervention ranged from 3.13 to 8.91 months in the BTA group, and from 3.17 to 7.0 months in the control group. For revision CLR, the mean age at surgical intervention was 24.70 years old in the BTA group, and 21.78 years old in the control group. 22 While ethnicity was not directly reported, 3 studies were from Taiwan, 1 study was from Mexico, 1 study was from India. Among the RCTs, 83 patients with CLR were treated with BTA compared to 78 patients treated with a normal saline placebo. Lu et al. compared 2 BTA interventions of 4 versus 6 points injections in 55 patients. 25 The follow-up duration was 6 months in 4 studies. One study performed a 3-6 month follow-up duration, 23 and 1 study had a follow-up to 12 months. 25 Outcomes were measured with both Vancouver scar scale (VSS) and scar width in 5 of the 5 studies. Visual analog scale (VAS) was additionally used in 3 of the studies. Risk of bias was assessed with the RoB 2.0 tool for randomized trials (Supplemental Figure 1) 3 of the 4 studies were low risk and 1 study Lu et al. had some concerns. MINOR criteria for the study by Navarro-Barquin et al. was moderate quality of evidence.
Study and Patient Characteristics.
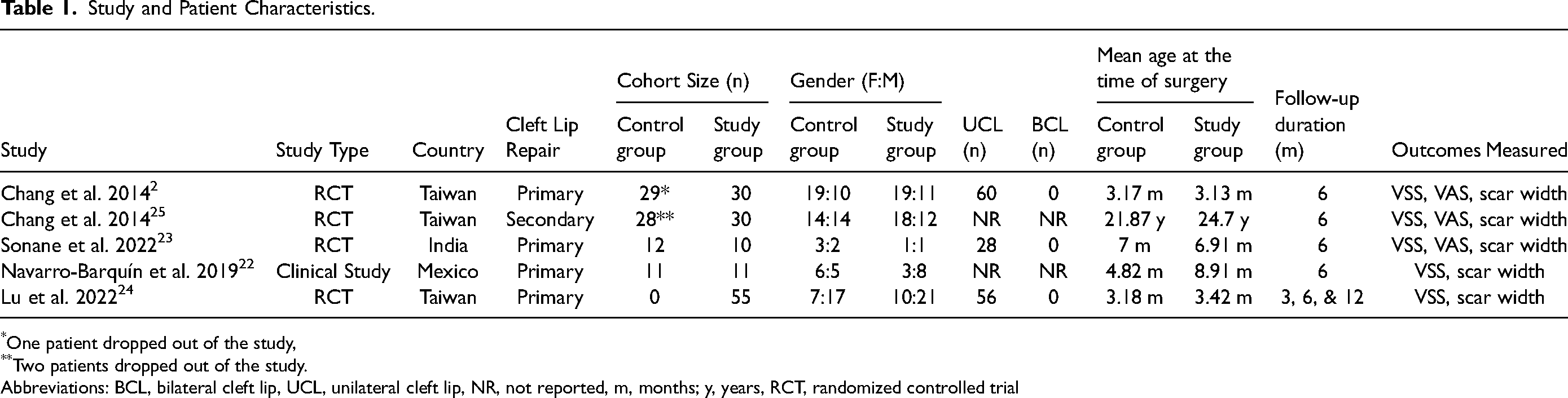
One patient dropped out of the study,
Two patients dropped out of the study.
Abbreviations: BCL, bilateral cleft lip, UCL, unilateral cleft lip, NR, not reported, m, months; y, years, RCT, randomized controlled trial
Surgical Technique and Experimental Interventions
All infants received BTA with a range dose of 1-2 units/kg injected in the orbicularis oris muscle (Table 2). Additional injections in other perioral muscles were performed in the study by Lu et al. 24 In 4 studies, patients received BTA during or immediately following CLR,2,23–25 whereas 1 study reported preoperative injections 7-10 days prior to surgery. 22 The Millard modified-rotation advancement CLR was used in 3 of the 5 studies.2,24,25 Tennison-Randall technique was used in 2 of the 5 studies.22,23 A summary of the surgical technique utilized, timing, location, dosage, and dilution of BTA is found in Table 2.
Surgical Techniques and Experimental Intervention.
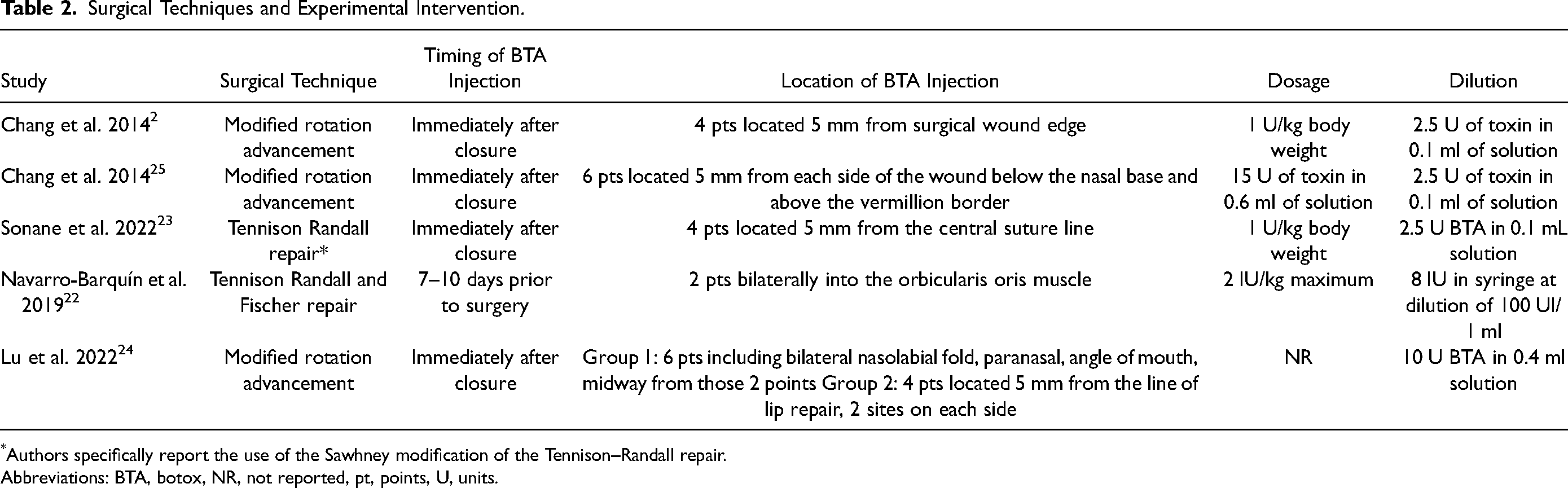
Authors specifically report the use of the Sawhney modification of the Tennison–Randall repair.
Abbreviations: BTA, botox, NR, not reported, pt, points, U, units.
Outcomes of Botox Injection
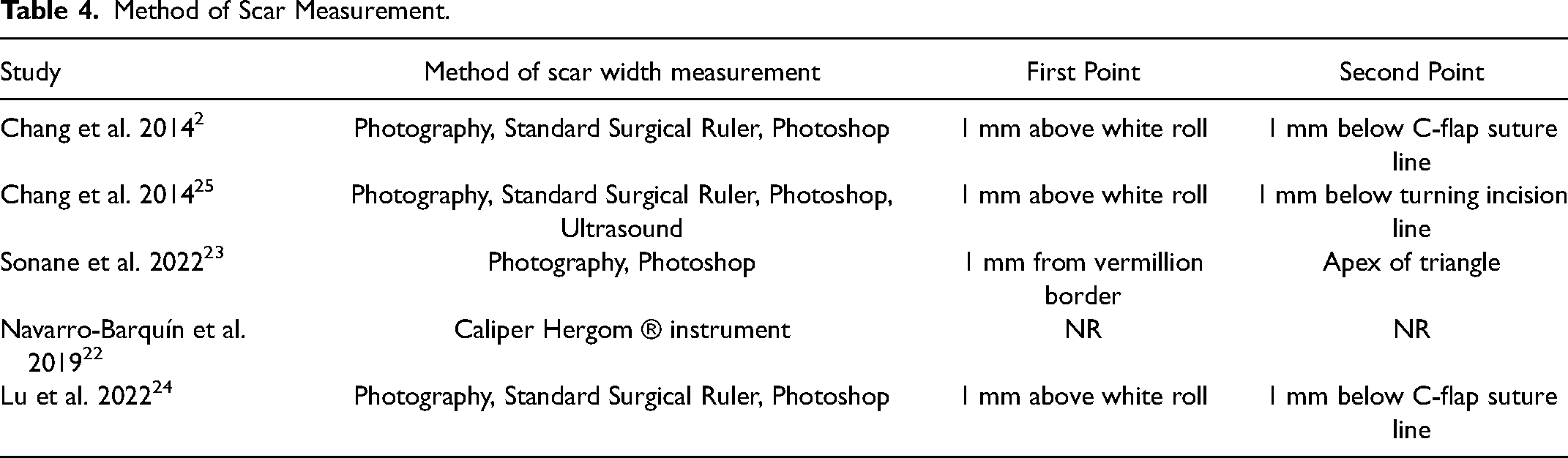
To determine the scar width, four studies used a standard surgical ruler or photoshop (CS5 extended version 12.0; Adobe Systems Inc, San Jose, California) 26 using the methods described by Navarro-Barquin et al. and a Caliper Hergom ®. 22 Outcomes of BTA injections versus controls, when available, are summarized in Table 3. Three studies reported the mean VAS measurements and found a significant reduction score with the utilization of BTA (Table 4).2,23,25 Five of the studies measured VSS, of which 1 did not include a saline control group.2,22–25 Of the 5 studies, 2 reported significant VSS improvement with BTA.22,25 Lu et al. did not include a saline control group 24 ; however, the authors reported improvement in patients that received BTA injections at additional muscle sites.
Outcomes of Botox Injection.
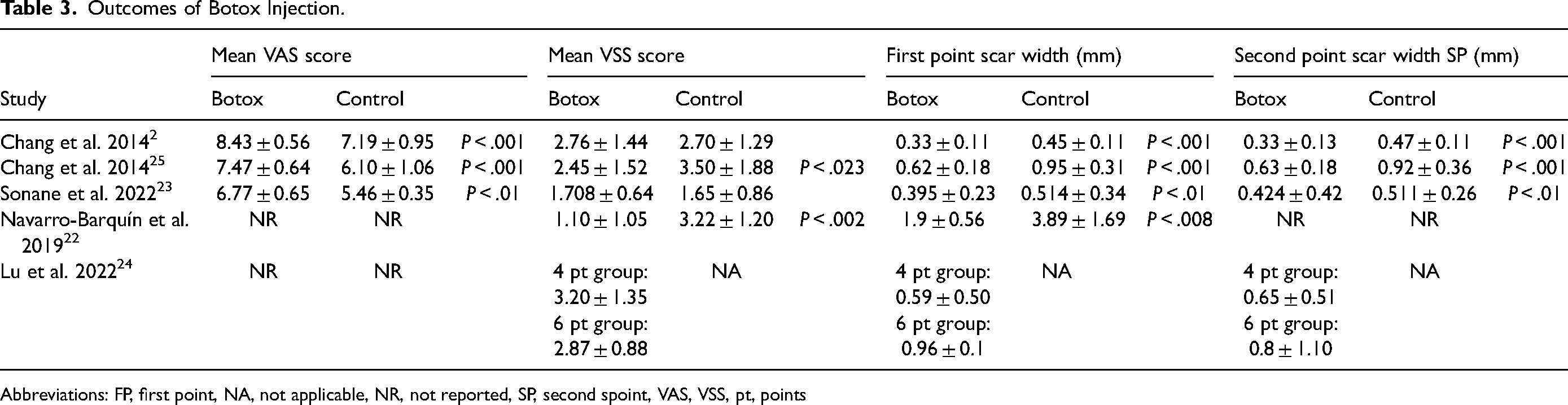
Abbreviations: FP, first point, NA, not applicable, NR, not reported, SP, second spoint, VAS, VSS, pt, points
Method of Scar Measurement.
All 4 studies that compared scar width at 6 months with BTA versus normal saline reported a significant reduction in scar width with BTA.2,22,23,25 Of note, Lu et al. did not observe a significant difference in VSS or scar width. However, both groups in their study received BTA injections. 24 There were no reports of complications associated with botulinum toxin injection or surgery.
Discussion
In this systematic review, we analyzed the current literature regarding the use of BTA for CLR, a relatively novel but promising adjuvant approach to potentially improve postoperative scar quality. BTA is thought to improve scar quality in CLR through 2 mechanisms. First, and most acknowledged, is through decreased mechanical tension by chemoimmobilzation of perioral muscles.13,14,27,28 The second mechanism is through the inhibition of TGF-b1/SMAD and ERK pathways.29,30 Jeong et al. evaluated the expression of myofibroblast markers in hypertrophic scar fibroblast cell lines, which revealed decreased cell proliferation and decreased gene expression of myofibroblasts marker alpha-smooth muscle actin when treated with BTA compared to controls. 30 Li et al. had similar results when analyzing cell proliferation and collagen expression. 29 The authors additionally found that BTA had a dose-dependent inhibition of collagen and fibroblasts treated with TGF-b1, an important cytokine for HS formation. 29
There is currently no established consensus over the timing, technique, or dosage of BTA injection in patients undergoing cleft lip procedures. A systematic review performed by Wang et al. assessed patients with 15-50 units of BTA for facial scars due to facial trauma, surgery, complex wounds, and scar revisions in patients aged 12-60 years old, 31 whereas Chang and colleagues (2014) used 15 units injected into 6 points in adult patients who had secondary revision for cleft lip deformity. 25 The 4 studies with pediatric patients ranged from 2 to 6 injection points.2,22–24 In regard to timing, 4 studies reported BTA injections immediately after wound closure2,23–25; the remaining study described preoperative BTA injections prior to cheiloplasty. 22 The differences in BTA injection limit, cumulative analysis, and standardization of practice should be considered in the methodology of future studies.
Our systematic review revealed that studies to date are inconsistent in determining scar quality, with VAS, VSS, and scar width being the most widely reported parameters in studying CLR and BTA injection. In the studies that used VSS and VAS, the raters were blinded to the groups. Sonane et al. blinded 5 individuals (2 consultants and 3 plastic surgery trainees) and took the mean of 2 scores, 23 Lu et al. blinded 2 surgeons to the group, 24 Chang et al. used 5 independent examiners (2 attendings and 3 laypersons) in both studies,2,25 and Navarro et al. had an independent evaluator assess VSS. 22 VAS and VSS are photograph-based subjective assessments that are observer dependent and consider factors such as scar height, thickness, pliability, surface area, texture, pigmentation, and vascularity. 32 VSS assesses vascularity, height/thickness pliability and pigmentation, and is used widely in burn scar assessment. 33 VAS has 4 dimensions, including pigmentation, vascularity, acceptability, and observer comfort. Both scales have demonstrated high observer reliability and internal consistency when compared to expert panel evaluation.34–36 While objective measurements like scar width may help to determine the extent or degree of scar proliferation, the method of determining scar width was variable. Chang et al. used ultrasonography to measure scar width in revision surgeries 25 while other studies used photographs2,19,23,24 and 1 study used a Caliper Hergom ®. 22 Future studies should focus on providing reproducible landmarks to improve consistency and mitigate error.
Length of follow up to evaluate the effects of BTA injection on CLR scar outcome varied in the studies included in our review, with some studies reporting up to less than a month from BTA injection/CLR2,19,25 while others documented their findings at 6-12 months. 24 Lu et al. found that lip scar quality was worst at 3 months to 6 months after CLR, with improvement noted at 12 months. 24 Given that the effects of BTA are shown to be present at up to 6 months after injection and Lu's findings, future studies should report follow up of at least 1 year after CLR.
Our results suggest that the dosage of 1-2 units/kg of BTA is well tolerated in children and adults undergoing CLR or revision surgery as there were no reports of significant side effects or complications. In fact, higher doses of BTA have been safely administered in children in cases of sialorrhea, neurogenic bladder, lower limb spasticity, and congenital muscular torticollis.37–39 The safety of BTA is further supported by a recent systematic review by Wang et al. of BTA use in facial scars and facial wounds due to various etiologies. 23 The study included 210 patients and were treated with 15-50 units of BTA, with injection timing varying study to study. 23 The authors concluded that the addition of BTA at higher doses compared to those used for cleft lip scarring improved efficacy in the treatment of facial scars and did not result in any reported adverse events. Although reassuring, data from larger patient cohorts is necessary to further investigate risks, if any, associated with BTA use in this context, with a focus on any potential negative impact on feeding in this infant population.
In addition to safety concerns, the cost of BTA may be problematic, as it is unlikely to be covered by insurance for this indication. At our institution, the wholesale cost for BTA is roughly $15 per unit. The cost of BTA for CLR can be estimated using the recommended average dosage at 1-2 units per kg for BTA in CLR, the average age of CLR of 6 months, and average weight (kg) at 6 months between 7-8 kg. We determined the estimated cost to be an average of $240 (2 u/kg at 8 kg, 16 units total to be used), $15 × 16 units). Though initial patient and insurance charges would be greater, they would likely be significantly less than the cost of a secondary revision, exceeding $8000 in 2009. 5
The primary limitation of this systematic review is the relative few number of studies that have been published to date, as well as the small number of patients per study. In addition, the variability in the study design and methods of the published literature prevented our ability to perform grouped analyses. While 4 of the 5 studies had intervention groups that compared BTA to normal saline control, 1 study compared 2 different BTA interventions. When including the patients in both intervention groups from the latter study, the total sample size of the BTA intervention group was 136 patients, with no cases of BCL reported. While work examining BTA for UCL is growing, the utility of BTA in BCL remains uncharted. Three studies reported size of cleft for both groups prior to repair and none had significant differences.2,22,24 Future studies should record the size of cleft prior to repair, or at least specify whether the defect was complete/incomplete and whether any presurgical orthodontia was performed.
Conclusions
The presence of a hypertrophic scar is a feared complication of cleft lip repair, which can adversely impact child development and exacerbate social stigma and discomfort for the patient. Our systematic review of the limited number of relatively small studies demonstrates that BTA injection is effective in improving scar quality after cleft lip procedures and has no adverse effects. More studies with a greater number of patients and length of follow-up are necessary to focus on the effects of BTA on scarring after cleft lip repair in patients of diverse ethnicities and determine an optimal injection protocol in terms of timing, the number of injections, and dosage.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656231190535 - Supplemental material for Botulinum Toxin to Improve Scar Quality in Cleft Lip Repair: A Systematic Review
Supplemental material, sj-docx-1-cpc-10.1177_10556656231190535 for Botulinum Toxin to Improve Scar Quality in Cleft Lip Repair: A Systematic Review by Paul F. Martinez, Ashley E. Rogers, Esperanza Mantilla-Rivas, Helena Hughes, Daniela Melo Leal, Md Sohel Rana, Monica Manrique, Gary F. Rogers and Albert K. Oh in The Cleft Palate Craniofacial Journal
Supplemental Material
sj-docx-2-cpc-10.1177_10556656231190535 - Supplemental material for Botulinum Toxin to Improve Scar Quality in Cleft Lip Repair: A Systematic Review
Supplemental material, sj-docx-2-cpc-10.1177_10556656231190535 for Botulinum Toxin to Improve Scar Quality in Cleft Lip Repair: A Systematic Review by Paul F. Martinez, Ashley E. Rogers, Esperanza Mantilla-Rivas, Helena Hughes, Daniela Melo Leal, Md Sohel Rana, Monica Manrique, Gary F. Rogers and Albert K. Oh in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Presentation
The work contained in this manuscript was presented at ASPS Plastic Surgery The Meeting 2023, Oct 27-30, 2023, Boston Massachusetts.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.