
Abstract
Objective
There is only one study in the literature in which 3D evaluation of sphenoid sinus volume in patients with cleft lip and palate was used. This shows that this issue has not been adequately evaluated. The present study aimed to compare the volume of the sphenoid sinuses in patients with cleft lip and palate on cone-beam computed tomography images, and to compare them with healthy controls. The high variability of sphenoid sinus volumes poses a risk for iatrogenic lesions during surgical procedures. Because the degree of pneumatization due to increased volume increases the likelihood of exposure of vital neurovascular structures such as the internal carotid artery, maxillary nerves, and optic nerves.
Design
Retrospective cohort study.
Setting
University Hospital.
Patients
A total of 64 patients (32 cleft palate, 32 controls) over 18 years of age who had sphenoid sinuses in the image area were included in our study.
Outcomes
Sphenoid Sinus Volume.
Results
When the groups were compared in terms of total sinus volume, there was a statistically significant difference between them. Total sinus volume was significantly mean 2.806,87 mm lower in patients with cleft lip and palate compared to the healthy group (P = .015).
Conclusion
To be aware this lower volume of the sphenoid sinus in cleft lip and palate patients will be useful for the surgical approach to sphenoid sinus. However, the literature on the subject is insufficient, more comprehensive clinical and radiological studies are needed on a larger sample.
Introduction
Cleft lip and palate (CLP) has a multifactorial etiology and is one of the most common malformations of the head and neck region. Most cases are nonsyndromic, with an incidence of 700/1. 1 This congenital pathology may cause malocclusion, nutritional, speech, auditory and esthetic problems in the patient. There are also studies showing that it causes anomalies in the paranasal sinuses. 2
The relationship between CLPs and the maxillary sinus has been of interest to some investigators as they think that the drainage pathways of the maxillary sinus may be affected in these patients. 3 There are also studies in the literature that argue that the sinuses are also affected in CLPs due to embryological reasons. 4 Since the sphenoid sinus is anatomically distant from the lips and palate, there are not many studies evaluating the relationship between them.
The sphenoid sinus is one of the paranasal sinuses that shows a lot of variation. These variations can affect vital structures. Pneumatizations, which are common variations, may involve important structures such as the pituitary gland, optic nerve, and internal carotid artery. Detection of these conditions is very important in the prevention of surgical complications.5,6
The high variability of sphenoid sinus volumes poses a risk for iatrogenic lesions during surgical procedures. Because the degree of pneumatization due to increased volume increases the likelihood of exposure of vital neurovascular structures such as the internal carotid artery, maxillary nerves, and optic nerves. 7
Cone-beam computed tomography (CBCT) is the primary technique used in the three-dimensional examination of head and neck bones and pathologies. 8 It allows visualization of paranasal sinuses, airway and intracranial structures outside the dentoalveolar area in a wide FOV range. 9 In addition, CBCT has advantages over CT such as shorter time, less radiation and lower cost. 10 The European Commission's guidelines on radiation protection of CBCT (SEDENTEXCT) recommend that CBCT, which is used in many head and neck pathologies, should be strictly examined and evaluated for patients with CLP. 3
With the increasing use of CBCT in dentistry, CBCT scanning is routinely performed in patients with CLP prior to alveolar bone graft procedures. 3 In the literature, there is only one study in which the 3-dimensional evaluation of the sphenoid sinus volume in patients with cleft lip and palate was used. 11 This shows that this issue has not been adequately evaluated. In addition, this study in the literature was conducted with pediatric patients. 11 In our study, measurements were made in adult patients. Since the sphenoid sinus in children has not reached the adult volume, our study was planned for adult patients. In this study, we compared the volume of the sphenoid sinuses on CBCT images in patients with CLP and healthy controls to evaluate the effect of CLP on sphenoid sinus volume in adult patients.
Material Method
This study was carried out in accordance with the principles of the Heslinki Declaration with the approval of the Istanbul University Faculty of Dentistry Clinical Research Ethics Committee (No: 516, 16.04.2021) The CBCT images of patients who reffered to the Department of Dental and Maxillofacial Radiology for any reason were analyzed. A total of 64 patients (32 cleft palate, 32 controls) over 18 years of age who had sphenoid sinuses in the image area were included in our study. Inclusion criteria of patients in our study included: (1) CBCT images where the sphenoid sinus enters the image region, (2) 18-55 years old, (3) Non-syndromic patients. Exclusion criteria included: (1) agenesis of the sphenoid sinuses, (2) 0-17 years of age, (3) patients undergoing head and neck surgery, (5) pregnancy. The tomography images of the retrospectively evaluated patients were obtained with the Scanora 3Dx brand CBCT device (Scanora® 3Dx, Soredex, Tuusula, Finland). The minimum FOV size of the device is 50 × 50 mm and the maximum FOV size is 240 × 165 mm. According to the selected FOV, the voxel size is between 0.1-0.5 mm and the slice thickness is between 0.1-0.3 mm.
Segmentations for sinus volume measurement were evaluated using ITK SNAP 3.8.0 software with automatic 3D segmentation. 12 CBCT images of the patients whose tomographies were taken were obtained in DICOM (Digital Imaging and Communications in Medicine) format and then uploaded to the software. Then, 3D segmentation (Segment 3D) was selected by setting the ROI (the region to be measured) using the “Snake Segmentation Mode” for the segmentation of the sphenoid sinuses. The thresholding of the sphenoid sinus was adjusted on the 3D segmentation screen. The system was painted with automatic segmentation of the relevant region. Segmentation of the right and left sphenoid sinuses was made using different colored labels. The volume measurement was calculated in mm3 from the “Volumes and Statistics” tab under the “segmentation” menu in the software (Figure 1). Three researchers measured using ITK-SNAP. The researchers who took the measurements had 5, 3, and 2 years of experience. One of the researchers had 30 years of experience. This researcher also supervised the measurements. For the volume measurement made by the researchers, the ICC (intraclass correlation coefficient) was calculated as 0.938 in the right sphenoid sinus measurements and 0.967 in the left phenoid measurements. The agreement between researchers is statistically significant.
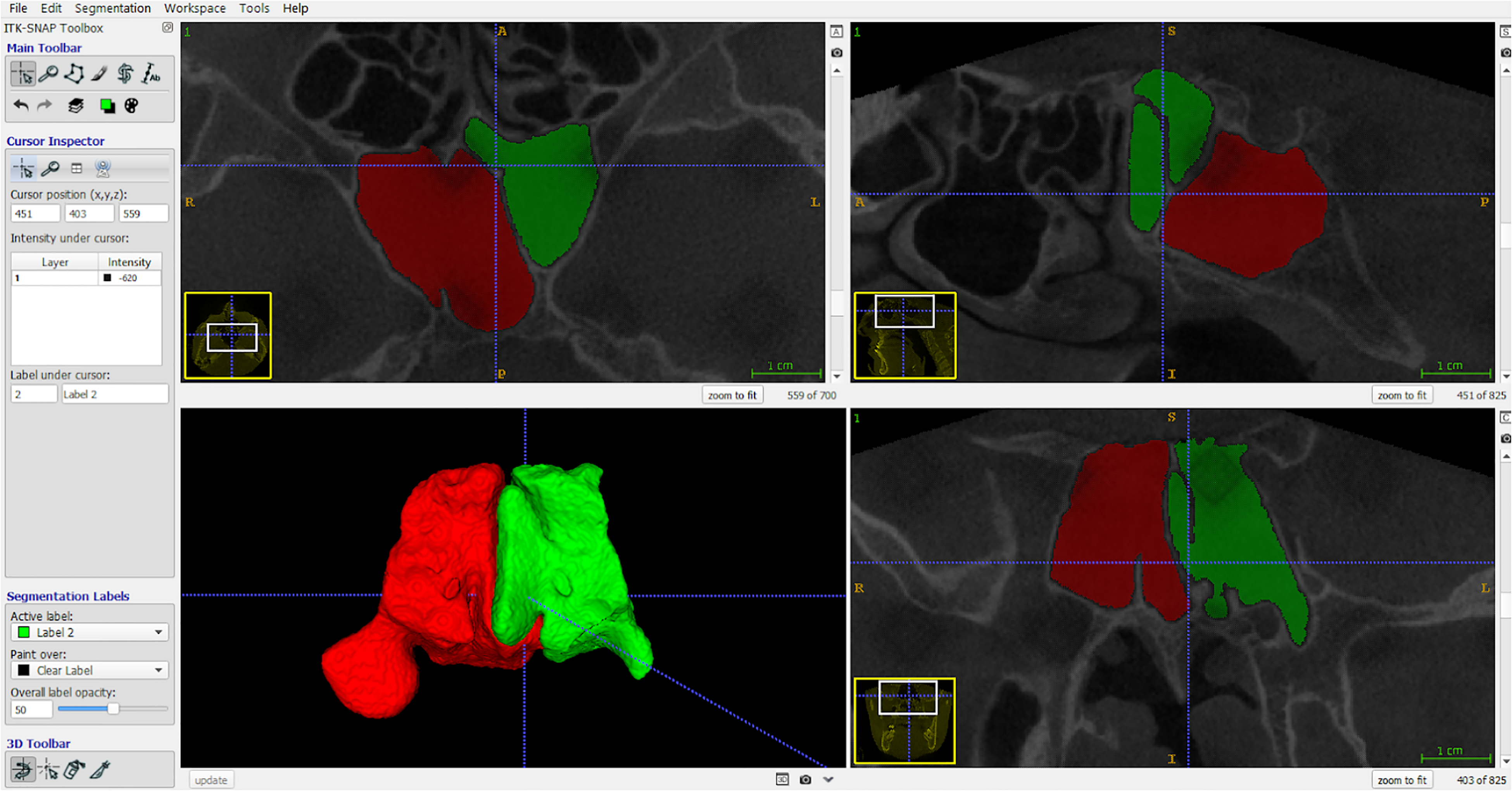
Sphenoid sinus volumes 3D segmented with ITK-SNAP software (red: right sphenoid sinus, green: left sphenoid sinus).
SPSS 21.00 (Statistical Package for Social Sciences, IBM Inc., USA) software was used for statistical analysis in our study. Descriptive statistics of continuous variables are given as mean standard deviation, minimum and maximum. Normality control of continuous variables was done with Saphiro-Wilk test. Student-t test was used for data suitable for normal distribution and Mann-Whitney U test was used for data not suitable for normal distribution in the evaluation of difference between groups. The Kruskal Walis test was used to compare three or more groups. Spearman correlation test was applied for the relationship between the variables. Statistical significance was determined at the 0.05 level.
Results
There was no significant difference in demographic characteristics between the two patient groups included in the study (Table 1).
Demographic Data by Groups.
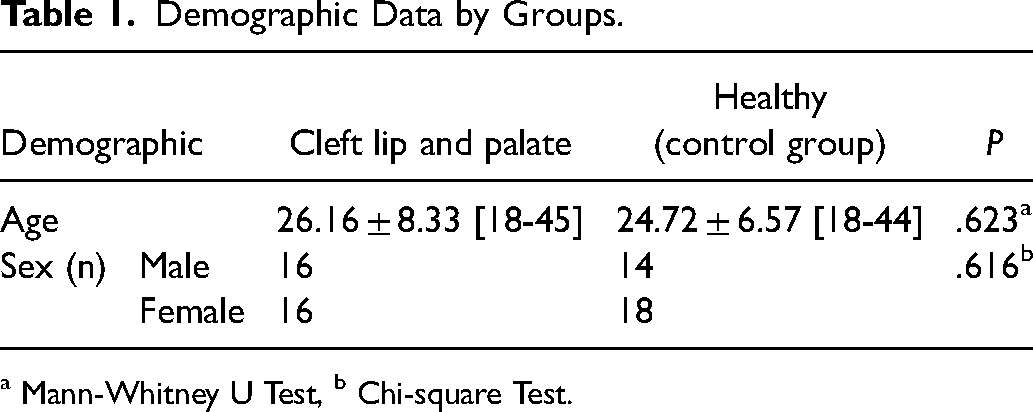
a Mann-Whitney U Test, b Chi-square Test.
The results obtained by comparing the right and left sphenoid sinus volumes of patients with cleft lip and palate and healthy patients are given in the table (Table 2). Right sphenoid sinus volumes of patients with cleft lip and palate were found to be 1222.53 mm3 lower than healthy individuals, while left sphenoid sinus volumes were found to be 833.56 mm3 higher.
Comparison of Groups According to Right and Left Sphenoid sinus Volumes.
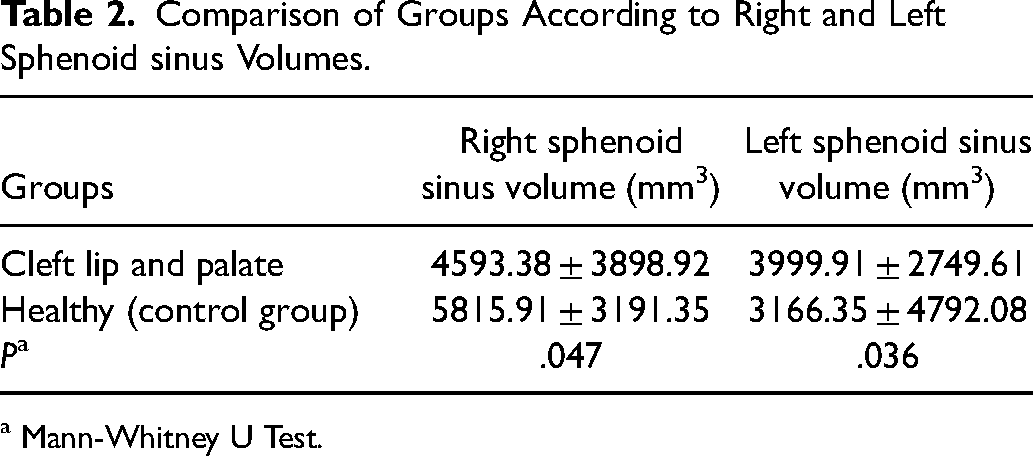
a Mann-Whitney U Test.
The results obtained by comparing the total sinus volumes of patients with cleft lip and palate and healthy patients are given in the table (Table 3). When the groups were compared in terms of total sinus volume, there was a statistically significant difference between them (p = 0.015). Total sinus volume was found to be 2806.87 mm3 lower in patients with CLP compared to the healthy group.
Comparison of Total sinus Volumes of Patients with Cleft lip and Palate and Healthy Patients.
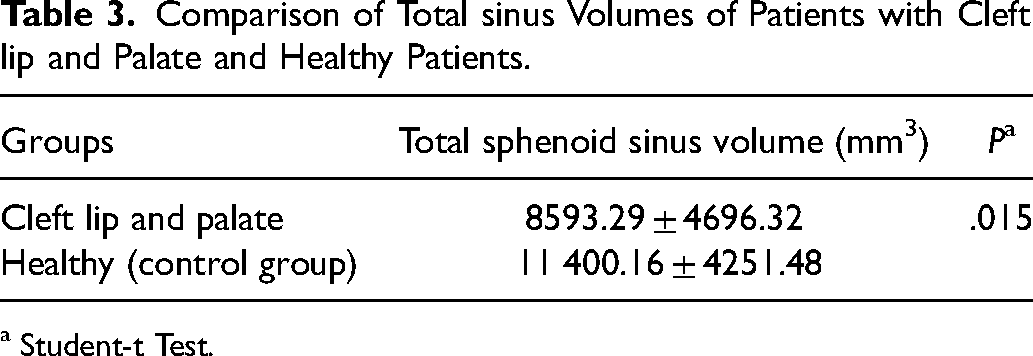
a Student-t Test.
When the right and left sphenoid sinus volumes were evaluated in terms of genders, there was no statistically significant difference between male and female genders (p > 0.05).
When the patients with cleft lip and palate were evaluated according to the cleft side (right cleft, left cleft and bilateral cleft) in terms of right and left sphenoid sinus volumes, no significant difference was found between the groups (p > 0.05).
Considering the correlation between right and left sphenoid sinus volumes, no statistically significant correlation was found (p > 0.05).
Discussion
The present study demonstrated that the sphenoid sinus volume of CLP patients was smaller than the control group. However, no difference was found in the cleft and non-cleft sides of the CLP patients and in the right and left sides of the control group. 13 There is no study focusing on sphenoid sinus volume in patients with CLP. Our study is a valuable pilot study to guide surgeons to choose the safest surgical route/method to prevent possible complications in patients with CLP. 13
Morphological knowledge of the sphenoid sinus has an important clinical value for the detection of sinus pathologies and the planning of surgical treatments. 13 The pneumatization process of the sphenoid sinuses begins around the age of 3-4 and lasts until puberty, reaching its peak between the ages of 12-16. The whole process usually ends in the third decade of life. 14 Sphenoid sinus volume measurement in the healthy population with the semi-automatic procedure has already been tested in the previous publication. It has been reported in the literature that there is no statistically significant difference in the measurement of paranasal sinus volumes between manual and semi-automatic segmentation methods. 15
By contrasting reconstructions produced by CBCT with those produced by micro-CT, the gold standard in 3D dental research, accuracy has already been evaluated. 16 Both the reference method, micro-CT, with an isotropic voxel size of 41 µm, and CBCT with an isotropic voxel size of 76 µm produced similar volumetric data. Voxel size has been shown to have a significant impact on CBCT image quality as well as scanning and reconstruction timeframes. Data on how voxel size affects the metric accuracy of reconstructions, however, are yet scarce.17,18
The paranasal sinuses of patients with CLP may develop differently in the embryonic period or the change in airflow passing through the nose and sinuses due to nutritional problems may cause a change in the sinus volume. 19 In the literature, maxillary sinus volume was found to be significantly lower on the cleft side compared to the non-cleft side in patients with unilateral CLP.19,20 In addition, there are studies reporting that maxillary sinus volume is lower in patients with CLP than in the control group.3,21,22 On the other hand, there are also studies that did not find a significant difference in maxillary sinus volume between patients with CLP and the control group. 23
Morphological knowledge of the sphenoid sinus has important clinical value in detecting sinus pathologies and planning surgical treatments. The sphenoid sinus is regarded as a structure of substantial clinical value because of its tight relationship with essential neurovascular and endocrine structures such the pituitary gland, internal carotid artery, optic nerve, and cavernous sinus. It is crucial when designing surgical approaches to both intra- and extrasellar diseases due to its anatomical placement. 24
Although there is a study evaluating the extensive pneumatization of the sphenoid sinus in CLP patients, one of the strong points of our study is the 3-dimensional measurement of the volume of the sphenoid sinus. 19 To our knowledge, there is only one study in the literature evaluating the sphenoid sinus volume in patients with CLP. 11
Similar to Tunç et al. the volumes of sphenoid sinus on the cleft side were not significantly different than the non-cleft side (P > .05) in patients with unilateral CLP. 11 While in the study of Tunç et al. the mean volumes of sphenoid sinuses of patients with unilateral CLP were not significantly different from healthy individuals (P > .05), in the present study the mean volumes of sphenoid sinuses were significantly lower than healthy individuals (P < .05).
To our knowledge, there is no study in the literature evaluating the sphenoid sinus volume in patients with CLP. Although there is a study evaluating the extensive pneumatization of the sphenoid sinus in CLP patients, one of the strong points of our study is the 3-dimensional measurement of the volume of the sphenoid sinus. 25 The smaller volume of the sphenoid sinus in patients with CLP is a new finding, but the cause is unknown. More work is needed to confirm and explain these findings. The limitation of our study is the limited sample size, it is recommended that further studies be conducted in more different races. The results of this study can guide surgeons about these possible vascular or anatomical differences that may pose a risk during transsphenoidal surgery.
Conclusion
To be aware this lower volume of the sphenoid sinus in CLP patients will be useful for the surgical approach to sphenoid sinus. However, the literature on the subject is insufficient, more comprehensive clinical and radiological studies are needed on a larger sample.
Footnotes
Statements and Declarations
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
This retrospective study was approved by the clinical research ethics committee of Faculty of Dentistry in Istanbul University (File no: 2021/516).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.