
Abstract
Objective
This study aimed to identify risk factors for NSCLP by analyzing polymorphisms in IRF6 rs2013162 and MTHFR A1298C rs1801131 in the Deutero Malay Population in Indonesia.
Setting
DNA isolation from venous blood samples was done followed by PCR and PCR-RFLPs method.
Patients/Participants
115 NSCLP subjects and 120 healthy control subjects.
Main Outcome Measure(s)
The odds ratio (OR) determined to evaluate the risk factors is the main outcome measure.
Material and Methods
The study is a case-control design using samples from the venous blood of 115 NSCLP subjects and 120 healthy control subjects. After DNA was extracted, the PCR-RFLPs method was performed using the DdeI restriction enzyme on 100 blood samples of the IRF6 rs2013162 group and Mboll restriction enzyme on 135 blood samples of the MTHFR A1298C rs1801131 group. The Chi-Square test was used with the Exact Fisher alternatives, depending on the expected count value.
Results
The results showed that the T mutant allele (OR = 4.125, P < .05) and GT genotype (OR = 21.00, P < .05) of IRF6 rs2013162 and the C mutant allele (OR = 3.781, P < .05), AC genotype (OR = 5, P < .05) and CC genotype (OR = 9,681, P < .05) of the MTHFR A1298C is associated to a greater risk of NSCLP.
Conclusions
IRF6 rs2013162 and MTHFR A1298C rs1801131 gene polymorphisms are strongly associated with NSCLP among the Deutero Malay population in the Indonesian population.
Introduction
Cleft lip and palate (CLP) is one of the most common birth malformations. The incidence of this disorder reaches 1 in 700 to 1000 live births worldwide, with untreated cases coming to 5000-6000 issues per year. 1 Based on the etiology, CLP disorders are divided into syndromic and non-syndromic. Syndromic CLP disorders (SCLP) clinically show malformations (usually two or more) and syndromes that appear in other body areas. In contrast, non-syndromic CLP disorders (NSCLP) are without malformation conditions or other syndromes. 2 CLP disorders can include a cleft lip (CL), cleft palate (CP), and unilateral or bilateral CLP. CLP disorders can affect speech mechanisms, delayed growth and development, nutritional problems, malocclusion, impaired hearing function, psychological problems, and reduced self-confidence, resulting in low quality of life. 3
The etiology of NSCLP cannot be defined yet, but several studies have investigated the involvement of genetic and environmental factors (multifactorial). Recent epidemiological data suggest NSCLP disorders have unique etiologic characteristics, including a strong genetic influence.
4
Some candidate genes involved in NSCLP disorders are Interferon Regulatory Factor 6 (
The IRF6 gene will regulate epithelial-mesenchymal transformation (EMT) and apoptosis during palatal fusion by activating the TGFβ3 gene. In addition, the IRF6 gene regulates the degradation of the Δp63 protein, which will induce p21 expression and apoptosis of medial edge epithelium (MEE). 6 IRF6 gene polymorphisms can produce non-functional proteins that affect DNA binding domains and cause negative effect domains, resulting in a severe phenotype, as in the case of NSCLP. 7 Our previous study has revealed other IRF6 polymorphisms (rs2235371 and rs rs642961) are the risk factor for certain phenotypes in the Deutero Malay Population in Indonesia8,9 and we were interested to analyze another IRF6 polymorphism to be associated with NS CLP among Deutero Malay population in Indonesia such as IRF6 rs2013162 that has not been analyzed among NSCLP in Deutero Malay population in Indonesia. Deutero Malay is the majority of the population in Indonesian population, so it is important to analyze this polymorphism in this population. IRF6 rs2013162 polymorphism is a substitution of base G into T (c.459 G > T), causing a change of TCG (serine amino acid) codon into TCT (serine amino acid) in the protein strand. In a study by Lu, Liu, Xu, Li, Jiang, Li, Zhao, Liu, Sui and Ma 10 in 2013 in North Eastern China, there was a significant change between IRF6 rs2013162 and NSCLP abnormalities (P = .002), which means that IRF6 rs2013162 is associated with NS CLP in North Eastern China. This variant is also associated with NS CLP in Iranian 11 and Pakistani. 12
The MTHFR gene is also one of the essential enzymes regulating folate metabolism in gene mutation conditions. The strengthening process between dihydrofolate and S-adenosyl methionine can stop its activity. 13 The MTHFR A1298C rs1801131 polymorphism is a substitution of base A into C that converts the amino acid glutamate (GAA) into alanine (GCA) at the residue 429thof the protein resulting in a decrease of MTHFR activity without affecting serum homocysteine levels. 14 According to a study performed by Rochmah, Suwarsi, Harumsari, Sosiawan, Fatimah-Muis and Faradz 15 in 2017, MTHFR A1298C rs1801131 polymorphism showed significant results in increasing the risk of CLP in the Sasak Tribe, Lombok, Indonesia.
The study of IRF6 rs2013162 and MTHFR A1298C rs1801131 polymorphisms has not been widely carried out in the Deutero Malay population among the Indonesian population, so we are interested in studying IRF6 rs2013162 and MTHFR A1298C rs1801131 polymorphisms associated with the risk of NSCLP disorders in Deutero Malay Population among Indonesian people, which is the largest population in Indonesia.
Materials and Methods
This study is a molecular epidemiological study with a case-control design and was approved by the Research Ethics Commission with the number 1484/UN6.KEP/EC /2019 and 367/UN6.KEP/EC/2021. All the participants signed an informed consent.
Subjects of Study
Sampling was done by consecutive sampling method by using 120 patients with NSCLP and 115 healthy controls without a family history of NSCLP. The PCR-RFLPs procedure was performed on 100 samples from the IRF6 rs2013162 gene group and 135 samples from the MTHFR A1298C rs1801131 gene group. All the sample from venous blood DNA isolation was done using the manual method from Home Brew, then 0.5 μl of DNA sample was used as a template for PCR.
DNA Extraction
DNA extraction using Promega kits (Madison, Wisconsin, USA) and all procedures followed the manufacturer's instructions.
IRF6 rs2013162 and MTHFR A1298C rs1801131 Genotyping
The PCR mixture with a total volume of 25 μL consisted of 0.5 μL of DNA, 1 μL of forwarding primer, 1 μLof reverse primer, 10 μL of Nuclease Free Water, and 12.5 μL PCR Mix. Then, the tube containing the PCR mixture was put into the Thermalcyler machine with PCR conditions. The temperature of the denaturation stage was 93 °C for 1 min, the annealing stage temperature was 59 °C for IRF6 rs2013162 and MTHFR A1298C, the extension stage temperature was 72 °C for 1 min, and the first cycle in the denaturation stage was added to 5 min, while the extension stage added up to 3 min, and the total cycle was 35 cycles. The primer for IRF6 rs2013162 was 5′CCCTGGGATGAGAAGGATAA3′ (forward) and 3′ACCTCTGACTCCCACTTGCT5′ (reverse), 16 and for MTHFR A1298C was 5′CTTTGGGGAGCTGAAGGACTACTAC3′ (forward) and 3′CACTTTGTGACCATTCCGGTTTG5′ (reverse). 14 The optimal PCR results were evaluated using 2% agarose gel electrophoresis. The 100 bp DNA ladder marker from the universal ladder was used as a marker of DNA size. The amplified DNA fragments stained with ethidium bromide were then visualized using a UV transilluminator. After optimal PCR results were obtained, PCR-RFLPs were performed using the DdeI restriction enzyme to evaluate the IRF6 rs1801131 polymorphism and MboII to evaluate MTHFR A1298C rs1801131 polymorphism. The PCR-RFLP mixtures were incubated at 37 °C for three h. The results of PCR-RFLPs were re-evaluated by using 3% agarose gel electrophoresis. The results of PCR-RFLPs will be evaluated by the Sanger sequencing method from some samples that revealed each genotypes of the polymorphisms to evaluate the PCR-RFLPs results. The DdeI will produce 2 bands of T mutant allele (62 and 202 bp), then 1 band of G allele (264 bp). The MboII will produce 5 bands of A allele (56, 31, 30, 28, and 18 bp), then 4 bands of C mutant allele (84, 31, 30, and 18). The PCR-RFLP methods have been previously used to genotype these polymorphisms in other studies.14,16
Statistical Analysis
The Chi-Square test was used to analyze alleles and genotype frequencies of IRF6 rs2013162 and MTHFR A1298C rs1801131 between patients and control subjects. Fisher's Exact test will be used as another alternative. Hardy-Weinberg equilibrium (HWE) was analyzed between two groups. The odds ratio (OR) will be determined from the contingency table to evaluate the risk factor of IRF6 rs2013162 and MTHFR A128C rs1801131 in NSCLP. Then, if P ≤ .05, it means that it is statistically significant or significant, and if P > .05, it means that it is not statistically significant.
Results
For IRF6 rs2013162, there were 100 samples consisting of 50 NSCLP (9 cleft lip only (CLO), 7 cleft palate only (CPO), 23 unilateral CLP, 11 bilateral CLP), and 50 controls. For MTHFR A1298C, there were 135 samples consisting of 65 NSCLP (10 CLO, 10 CPO, 40 unilateral CLP, and 5 bilateral CLP) and 70 controls. As a general study, sex and age were not analyzed in detail for this time. The optimal PCR products and PCR-RFLPs results are described in Figure 1. For IRF6 rs2013162, the optimal PCR product was a single band of 264 bp. PCR-RFLPs resulted in the feature of GG genotype (264 bp), GT genotype (264, 202, and 62 bp), and TT genotype (202 and 62 bp). For MTHFR A1298C, the optimal PCR product was a single band of 162 bp. PCR-RFLPs resulted from the feature of AA genotype (56 bp, 31 bp, 30 bp, 28 bp, and 18 bp), AC genotype (84 bp, 56 bp, 31 bp, 30 bp, 28 bp, and 18 b) and CC genotype (84 bp, 31 bp, 30 bp, and 18 bp).
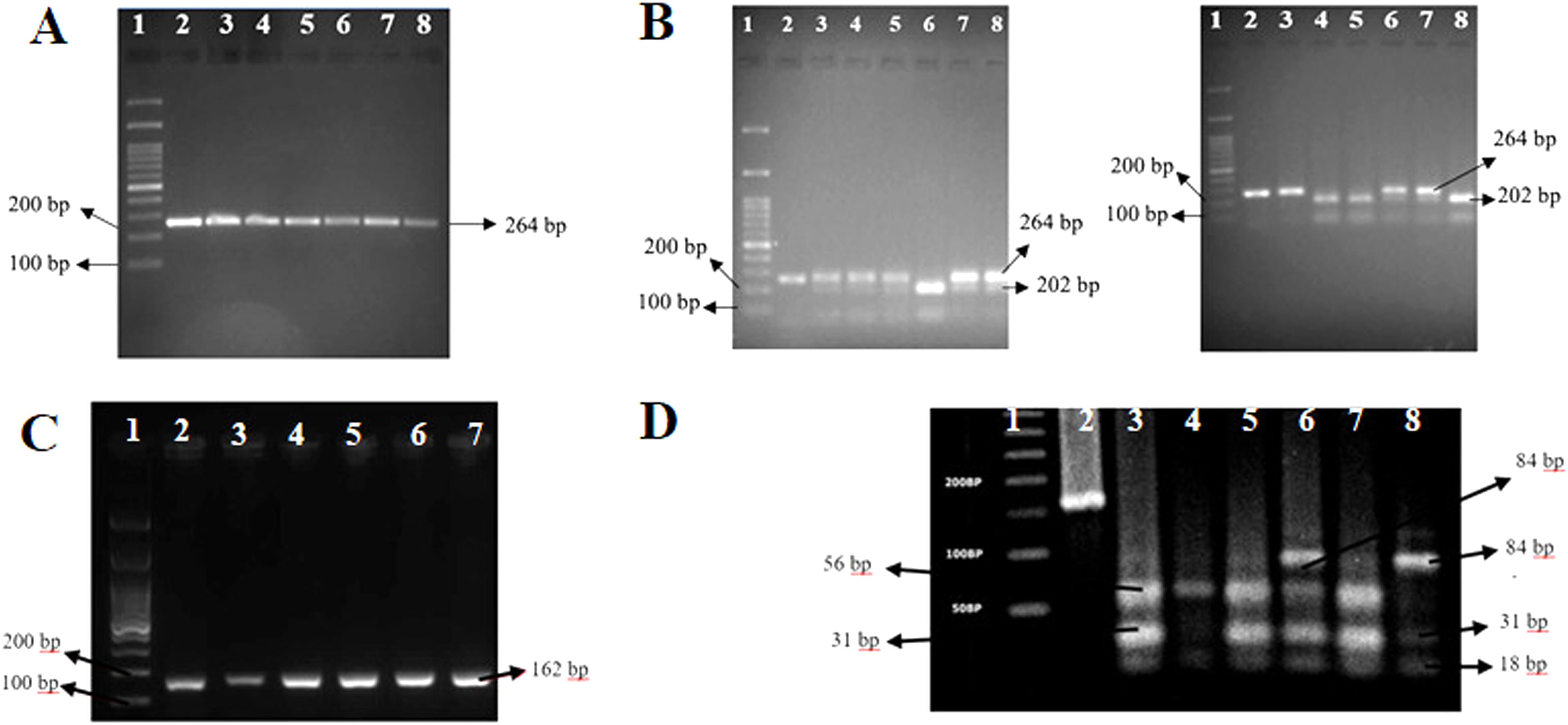
PCR products and RFLPs of IRF6 rs2013162 gene (A and B) and MTHFR A1298C rs1801131 gene (C and D). (A) Optimal PCR product results of IRF6 rs2013162. Line 1 shows a DNA Ladder of 100 bp. Line 2-8 DNA bands from optimal PCR products (264 base pairs (bp). (B) Results of PCR-RFLPs of IRF6 rs2013162 by using DdeI restriction enzymes. A. Line 1 shows a DNA ladder of 100 bp. Line 2, DNA products for control (uncut). Line 3 shows GT genotype (mutant heterozygous) (264, 202, and 62 bp). Line 6 shows TT genotype (mutant homozygous) (202 and 62 bp). B. Line 3 shows GG genotype (wild type) (264 bp). (C) Optimal PCR product results of MTHFR A1298C rs1801131. Line 1 shows a DNA Ladder of 100 bp. Line 2-7 show DNA bands from optimal PCR products (162pb). (D) Results of RFLPs -PCR products by using MboII restriction enzyme. Line 1 shows a DNA ladder of 100 bp. Line 3, 5, and 7 show the AA genotypes (wild type) (56 bp, 31 bp, 30 bp, 28 bp, and 18 bp). Line 6 shows AC genotypes (mutant heterozygous) (84 bp, 56 bp, 31 bp, 30 bp, 28 bp, and 18 bp). Line 8 shows the CC genotype (homozygous mutant) (84 bp, 31 bp, 30 bp, and 18 bp).
Figure 2 shows the PCR-RFLPs of Sanger sequencing performed. HWE analysis between two groups is presented in Table 1. In both polymorphisms, only in control groups were in HWE frequencies as there were only in control groups differences of frequencies that were not statistically significant (P > 0,05) between genotype variables (Table 1). There were limitations of our study that in NSCLP group both polymorphisms were not in HWE frequencies. The distribution of alleles and genotypes of each gene in the NSCLP and control groups are presented in Table 2. In IRF6 rs2013162, the risk/mutant allele (T) showed a higher frequency among cases than controls and had 4125 times as a risk factor to cause NSCLP (OR = 4215; 95% CI 2122-8108). GT heterozygous mutant genotype showed a similar result as the risk genotype and had 21,00 times to cause NSCLP (OR = 21,00; 95% CI 7530-58,563). Both allele and genotype were highly significant. In MTHFR A1298C rs1801131, a considerable risk/mutant allele (C) was observed to cause NSCLP 3, 781 times (3781; OR = 3781; 95% CI 2225-6426) as a risk factor to cause NSCLP and showed higher frequency in cases than controls. AC heterozygous mutant genotype showed a similar result as the risk genotype and had 5,00 times to cause NSCLP (OR = 5,00; 95% CI 0.027–1.878), and interestingly, CC homozygous mutant genotype showed elevated risk factor to cause NSCLP (OR = 9681; 95% CI 5048-434 907). Both AC and CC genotypes were highly significant.
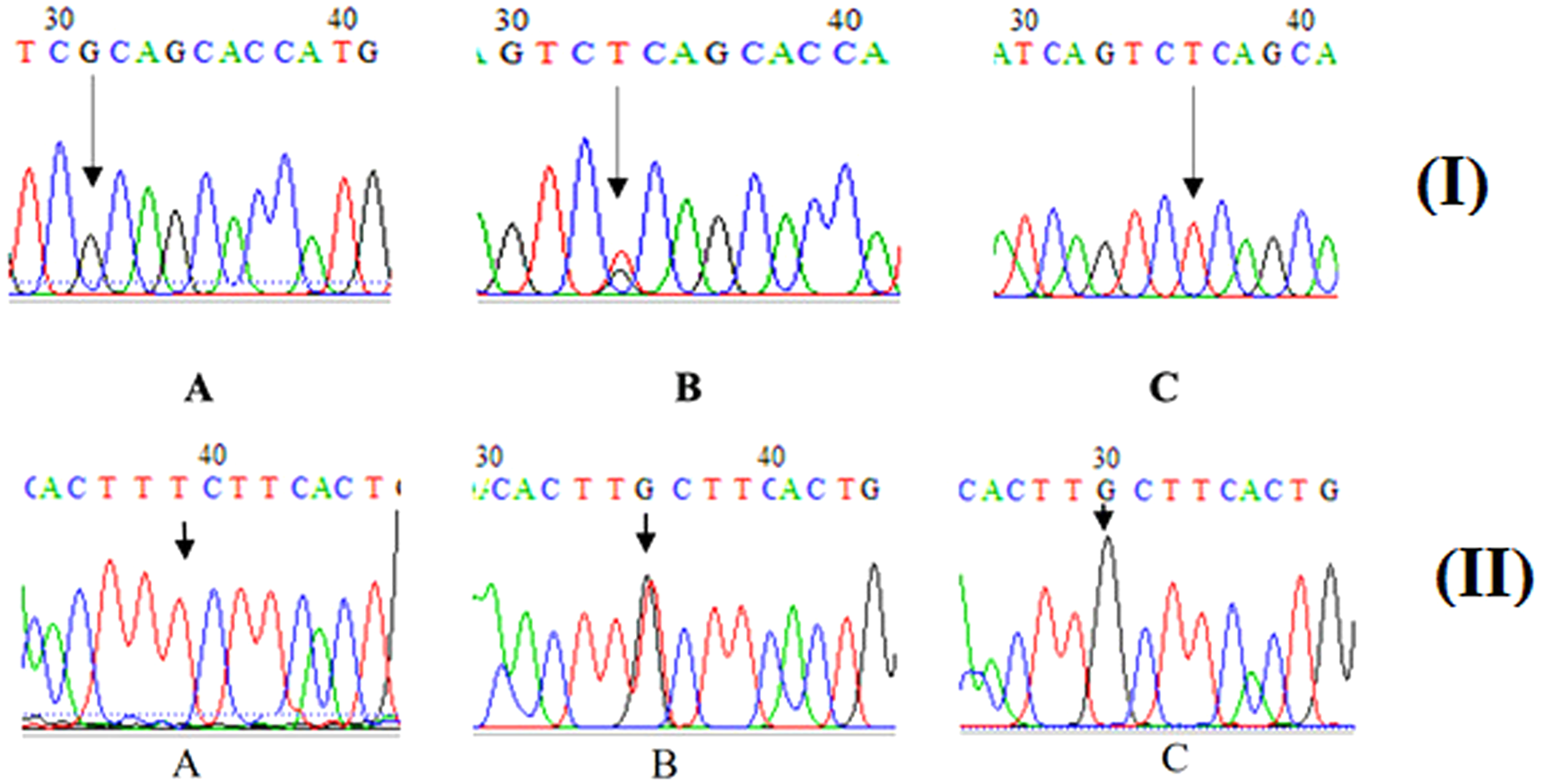
(I) Sequencing of IRF6 rs2013162 gene. A. GG genotype (wild type), B. GT genotype (mutant heterozygous), C. TT genotype (mutant homozygous). (II) Sequencing of MTHFR A1298C. A. AA genotype (wild type). B. AC genotype (heterozygous mutant). C. CC genotype (homozygous mutant).
Chi Square for HWE Analysis in NSCLP and Control Groups in IRF6 rs2013162 and MTHFR A128C.
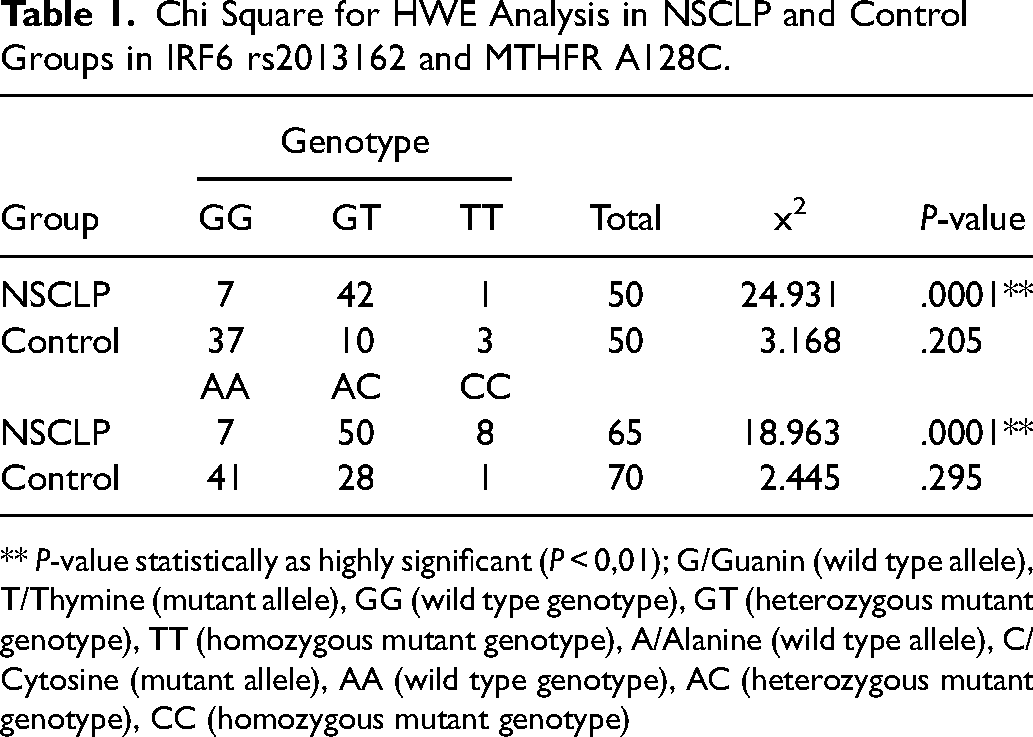
** P-value statistically as highly significant (P < 0,01); G/Guanin (wild type allele), T/Thymine (mutant allele), GG (wild type genotype), GT (heterozygous mutant genotype), TT (homozygous mutant genotype), A/Alanine (wild type allele), C/Cytosine (mutant allele), AA (wild type genotype), AC (heterozygous mutant genotype), CC (homozygous mutant genotype)
Genotypes and Alleles Distribution for IRF6 rs2013162 and MTHFR A1298C rs1801131.
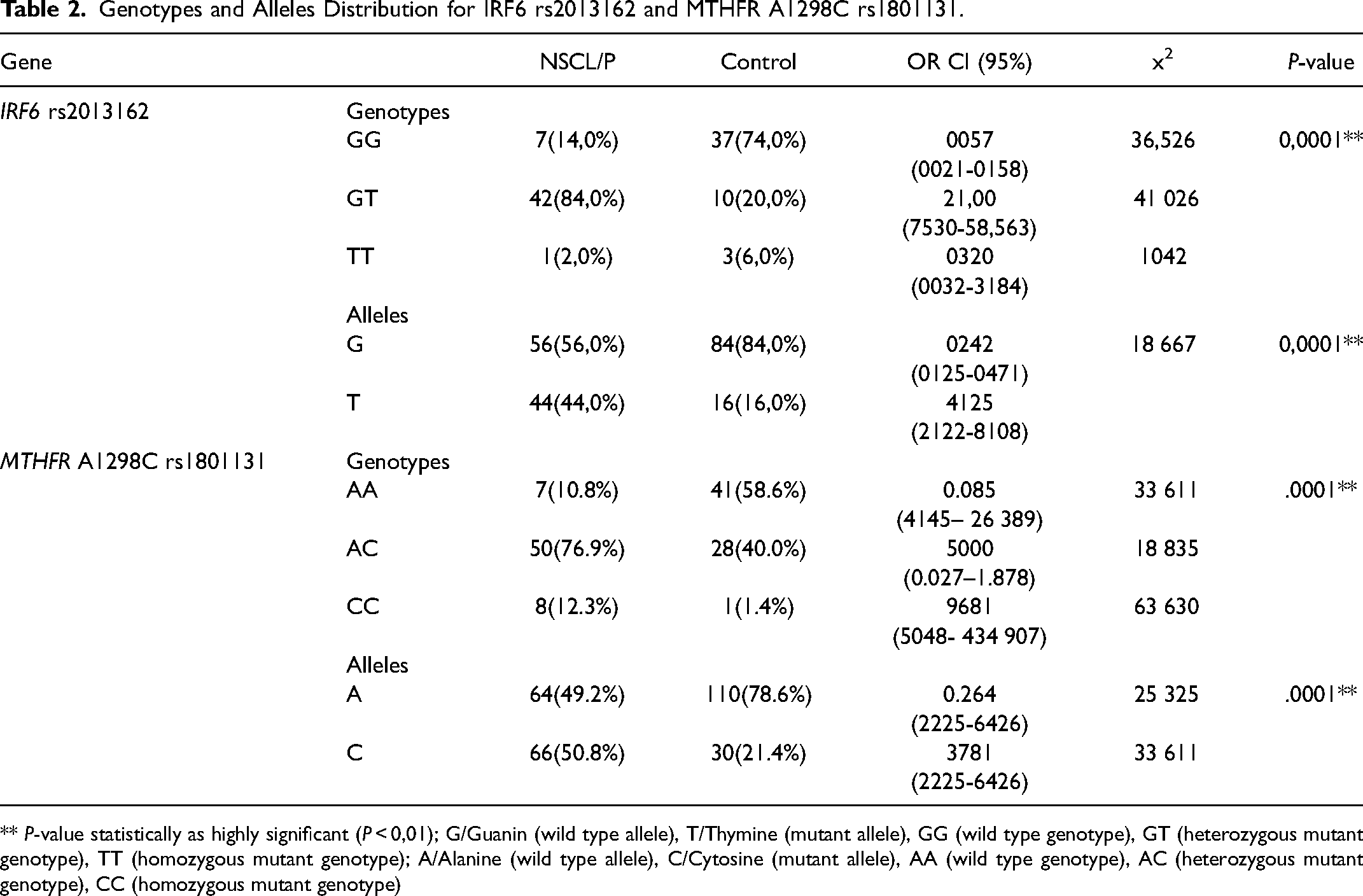
** P-value statistically as highly significant (P < 0,01); G/Guanin (wild type allele), T/Thymine (mutant allele), GG (wild type genotype), GT (heterozygous mutant genotype), TT (homozygous mutant genotype); A/Alanine (wild type allele), C/Cytosine (mutant allele), AA (wild type genotype), AC (heterozygous mutant genotype), CC (homozygous mutant genotype)
Table 3 compares each genotype, TT, GT, and GG The case-control analysis revealed significant differences in genotype comparison of TT and GT, GT and TT (P < 0,05), highly significant in comparison of GT and GG (P < 0,01), and not significant in comparison of TT and GG (P > 0,05). The NSCLP subjects (n = 50). TT genotype was found only in 1 subject, and it was only 2% found when compared with all 50 subjects of NSCLP. GT genotype was found in 42 subjects, which means that there were 84% compared to all 50 subjects. The TT genotype was found in 3 subjects, and it was 6% found when compared with all 50 subjects of control. GT genotype was found in 10 subjects, meaning there was 20% compared to all 50 subjects. The GG genotype was found in 7 subjects, which means that there were 14% compared to all 50 subjects. From all control subjects (N = 50), TT genotype was found in 3 subjects, and 6% was found when compared with all 50 subjects of control, GG genotype was found in 37 subjects, which means that there were 74% when compared with all 50 subjects. GT genotype was found in 10 subjects, and it was 20% found when compared with all 50 subjects of control, GG genotype was found in 37 subjects, which means that there were 74% when compared with all 50 subjects. TT genotype was found only in 1 subject, which means that there was 2% compared to all 50 subjects.
The Comparison of TT, GT, and GG Genotypes of IRF6 rs2013162.
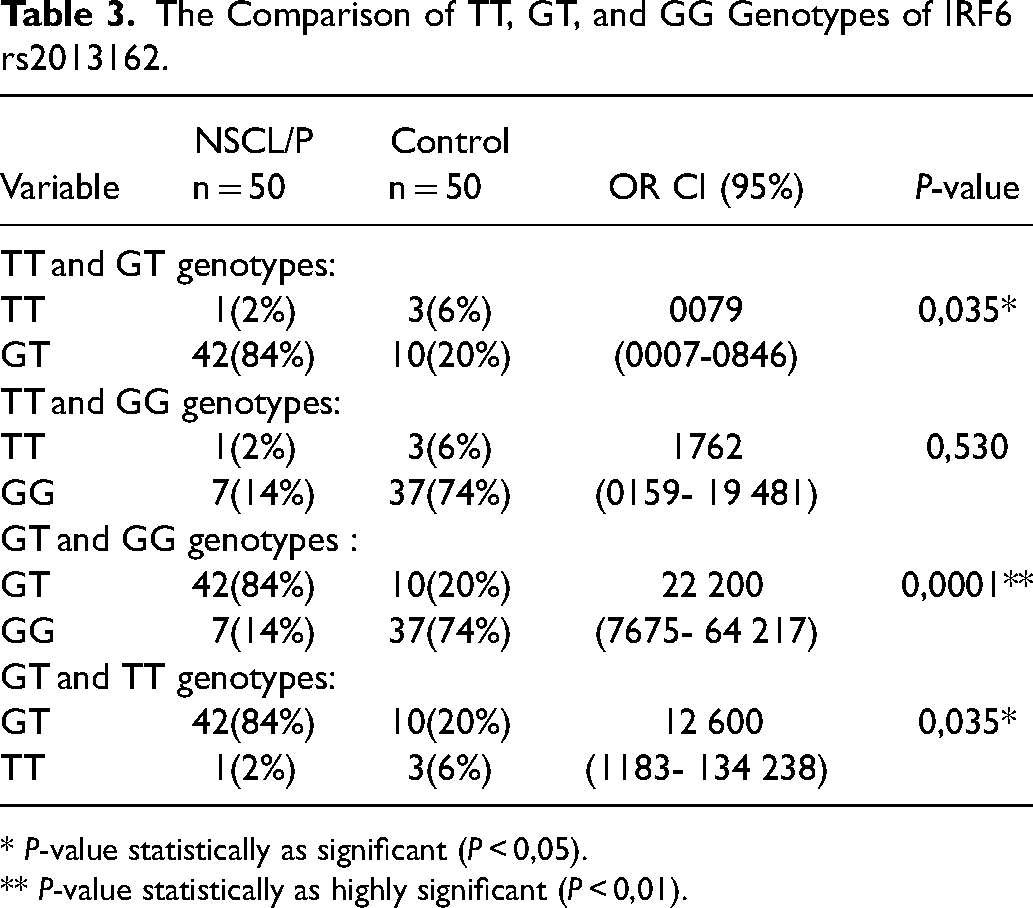
* P-value statistically as significant (P < 0,05).
** P-value statistically as highly significant (P < 0,01).
Table 4 compares each genotype AC, AA, and CC of MTHFR A1298C rs1801131. Case-control analysis revealed highly significant in comparison to AA and AC, AA and CC (P < 0,01), and not substantial in comparison to AC and CC (P > 0,05). We made this comparison to evaluate the role of each genotype in detail. Interestingly, the CC heterozygous mutant genotype had a higher risk of causing NS CLP than the AC heterozygous mutant genotype. When AC was compared with AA as the wild-type genotype, the risk was 10 459 (OR = 10 459; 95% CI 4145- 26 389). Then, when CC was compared with AA, the risk was higher of causing NSCLP (OR = 46 857; 95% CI 5048- 434 907). They were highly significant.
The Comparison of AC, AA, and CC Genotypes of MTHFR A1298C rs1801131.
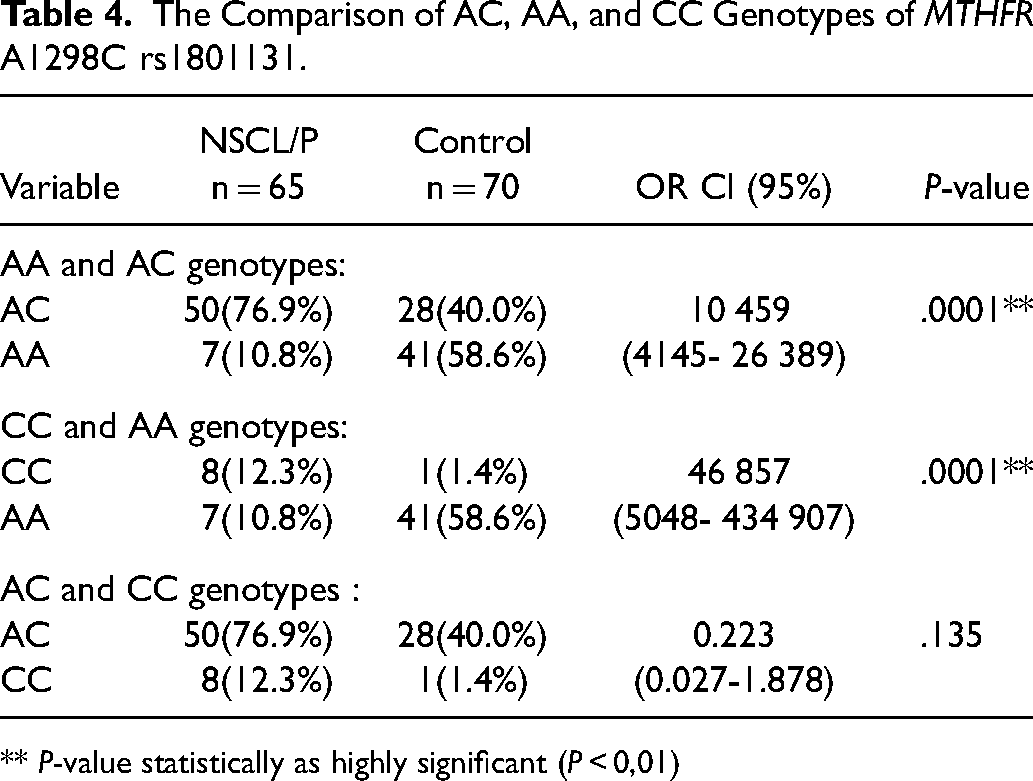
** P-value statistically as highly significant (P < 0,01)
Discussion
According to our result, the T mutant allele and GT heterozygous mutant genotype of IRF6 rs2013162 were highly significant to be associated with NSCLP among the Deutero Malay population in Indonesia (Table 2), especially in the GT genotype which can increase the risk of NSCLP by 21 times (OR = 21,00, P < 0,0001). In another study by Xu, Han, Lu, Feng and Dai 17 in North Eastern China in 2016, it was also found that the T allele was significantly higher in CLP patients compared to controls (P = .025). This finding suggests that IRF6 rs2013162 is also a risk allele for NSCLP in the northeastern Chinese population. A study by Lu, Liu, Xu, Li, Jiang, Li, Zhao, Liu, Sui and Ma 10 in 2013 also found a significant change between rs2013162 and NSCLP (P = .002). A significant result was also found in Saudi Arabia by Alamoudi, Sabbagh, Innes, Edris, Butali, Alnamnakani, Rabah, Hamdan, Alhamlan, Abdulhameed, Farsi, Hassan and Mossey 18 (P = .018). In contrast to the study by Ibarra-Arce, García-Álvarez, Cortés-González, de Zarate-Alarcón, Flores-Peña, Sánchez-Camacho, Arenas-Díaz, Romero-Valdovinos and Olivo-Díaz 19 in 2015 in Mexico, it was found that there was no significant result of IRF6 rs2013162 as a risk factor for NSCLP (P = 0,843). We also compared genotypes to evaluate significant differences among genotypes (Table 3-4).
The IRF6 gene is located on the short arm of chromosome 1 (1q32,2-q41) and is composed of 9 exons. It is a transcription factor that provides instructions for making a protein that plays an essential role in every development, including lip and palate formation. The IRF6 rs2013162 gene is located in the exon five regions. The role of IRF6 polymorphism in exon five associated with NSCLP is still clearly unknown. Exons’ mutations or polymorphisms can cause protein products’ disturbances. 20
In contrast to polymorphisms in exons, polymorphisms in introns can also influence NSCLP pathogenesis as they can cause troubles in the splicing process which will interfere with transcription and translation processes. Disruption in this splicing process can change the strand site exons or introns. Nevertheless, for most of these polymorphisms, it is unlikely. Usually, when an intronic polymorphism is associated with a phenotype it is because this polymorphism is in linkage disequilibrium with other polymorphisms in the region. More extensive studies of silent and missense mutations in various diseases have been associated with point mutations like this IRF6 rs2013162. 21
In this study, the AC genotype of MTHFR A1298C rs1801131 had a 5 times risk associated with NSCLP (P = .0001**) compared to controls, but when we made a comparison between genotypes, there were exciting results between AA and AC genotypes where AA genotype will increase the risk of NSCLP 10 459 times than AC genotypes (Table 2), also between CC and AA genotype where CC genotype will increase the risk of NSCLP 46 857 times than AA genotypes. We assumed that C mutant allele might create a dose effect in this polymorphism. It suggests that MTHFR A1298C rs1801131 is also strongly associated with the incidence of NSCLP in the Deutero Malay population among the Indonesian population. The MTHFR A1298C is a point mutation in exon 7. Homozygous status (CC genotype) will influence DNA methylation. 22 In another study by Ngantung and Yusuf 23 in 2014 in Manado, Indonesia, it was found that there was a contribution between the MTHFR A1298C rs1801131 gene and NSCLP, but this study did not include the Deutero Malay population in general. Another survey by Rochmah, Suwarsi, Harumsari, Sosiawan, Fatimah-Muis and Faradz 15 in 2018 in Lombok, Indonesia, revealed that MTHFR A1298C polymorphism increases the risk of NSCLP in the Sasak tribe, Lombok, Indonesia (P = .036). There was also a study by Abdollahi-Fakhim, Estiar, Varghaei, Sharafi, Sakhinia and Sakhinia 24 in 2015 in Iran showed significant results in the A1298C gene in NS CLP, but in contrast with the study by Zhao, Ren, Shen, Zhang and Zhou 25 in 2014 in China, which showed no association between the MTHFR A1298C polymorphism on NSCLP (P = .001). MTHFR A1298C is located in exon 7. However, the role of this polymorphism in NSCLP pathogenesis, especially in exon regions, cannot be explained yet, especially among the Deutero Malay population in Indonesia. Specific environmental factors may have contributed to this result, so further investigation is crucial for the subsequent study.
The MTHFR is located on the short arm of chromosome 1 (1p36.3), comprises 11 exons and ten introns, and acts as a key regulatory enzyme in folate and homocysteine metabolism. MTHFR deficiencies can cause hyperhomocysteinemia with homocystinuria or mild hyperhomocysteinemia. 26 The MTHFR A1298C will eventually result in substituting amino acids glutamate (GAA, GAG) into alanine (GCU, GCC, GCA, GCG). 24 Abnormalities in the MTHFR gene and nutritional deficiencies can lead to methionine deficiency and homocysteine accumulation. 27 Homocysteine is made when a cell breaks down the amino acid methionine. The folate-methionine reaction pathway is involved in the making of DNA, the methylation of DNA, and the balance between oxidation and reduction in cells. Methionine is used by the human body to make proteins. Methionine derived from food is converted to S-adenosylmethionine (SAM) by the S-adenosyl methionine synthase enzyme. SAM is the primary methyl donor in the methylation process and functions in the transmethylation process, namely the methylation of macromolecules, phospholipids, myelin, choline, and catecholamines. 28
MTHFR gene polymorphism is one of the most studied aspects of the MTHFR gene. The A1298C polymorphism, a frequent single nucleotide variation in MTHFR, has slightly affected the enzyme's activity. The MTHFR A1298C polymorphism at the 429 amino acid position reduced MTHFR activity without changing serum homocysteine levels. 29 Homocysteine will indirectly cause oxidative stress through decreased transcription, translation, and catalytic activity of glutathione peroxide (GPx) and superoxide dismutase (SOD). 30 Homocysteine has the potential to break down protein disulfide bonds that change the structure and function of proteins. 31
The A1298C polymorphism of the MTHFR gene disrupts folate metabolism. Together with low folate intake, this polymorphism will cause an increase in homocysteine levels, making it dangerous for pregnant women. 32 Maternal hyperhomocysteinemia may be a risk factor for having NSCLP offspring. 33 Some studies have also revealed that maternal MTHFR A1298C showed a relationship with NSCLP in some populations. Still, in this study, we did not include maternal from NSCLP patients suggests that MTHFR A1298C possibly has an effect in patients with NSCLP out of maternal factor, or all the NSCLP subjects in this study may have maternal MTHFR A1298C also, so further study is needed to evaluate the mothers of NSCLP subjects in this study.
Conclusion
Based on the results of our study, IRF6 rs2013162 and MTHFR A1298C rs1801131 gene polymorphisms are clearly associated with NSCLP among the Deutero Malay population in the Indonesian population.
Footnotes
Acknowledgements
The authors thank to Indonesian Cleft Lip and Palate Foundation: Yayasan Pembina Penderita Celah Bibir dan Langit-langit (YPPCBL) in Bandung Indonesia.
Author Contributions
Guarantors of the integrity of the entire study, SLN, AMM; study concepts/study design or data acquisition or data analysis/interpretation, all authors; manuscript drafting or manuscript revision for important intellectual content, all authors; manuscript final version approval, all authors; clinical studies, TT, RSD, AA, and SR.; statistical analysis, BAG; and manuscript editing, all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The Research Ethics Committe of Padjadjaran University, No. 1484/UN6.KEP/EC/2019 and 367/UN6.KEP/EC/2021.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.