
Abstract
Objective
Children with cleft lip and/or palate (CL/P) are at increased risk for Sleep Disordered Breathing (SDB), particularly Obstructive Sleep Apnea (OSA). At our institution, routine screening for SDB is performed using the Chevrin Pediatric Sleep Questionnaire (PSQ). This analysis is a practice audit looking at the outcomes of screening children with CL/P.
Design/Setting/Patients/Participants
A single-center, retrospective analysis was done of all non-syndromic patients with CL/P over the age of 36 months over a 4-year period. Children with known OSA were eliminated from analysis.
Main Outcome Measures
Univariate logistic regression was used to assess predictors for SDB (PSQ score > 8) amongst various patient, disease, and treatment characteristics. Outcomes of those screened were tracked.
Results
Of the 239 patients in the study cohort, 43 (18%) had positive PSQs. These subjects were more likely to have class III dental occlusion with maxillary retrusion (OR = 2.65, 95% CI: 1.2–5.8, p = 0.02). There were no differences amongst age, type of cleft, Veau classification, BMI, or history of pharyngeal surgery. One third of the group did not complete recommended testing. Twenty-five subjects with positive sleep screening underwent subsequent polysomnography and 21 (84%) had OSA.
Conclusion
Routine screening reveals a significant proportion of patients with CL/P with symptoms suggestive of OSA. While several patients did not complete confirmatory testing, those who completed a PSG had a high rate of identification of OSA. After excluding children with known OSA, patients with SDB are also likely to have class III dental occlusion and maxillary retrusion.
Keywords
Introduction
Thought to be secondary to either congenital or acquired anatomical differences, children afflicted with cleft lip and/or palate (CL/P) are at an increased risk of sleep disordered breathing (SDB) compared to non-affected peers.1–5 The importance of identifying these at-risk children has been well documented.1,2 SDB, most notably Obstructive Sleep Apnea (OSA), is associated with the development of comorbidities including learning disabilities, cardiopulmonary dysfunction, and growth restriction. 3
While this increased prevalence of SDB in children with clefts has been well established, there is a paucity of reports investigating which demographic, anatomic, or surgical qualities are associated with SDB.2–5 Outcomes associated with the diagnosis and treatment of SBD in this unique population are lacking.
It is standard practice at our clinic to administer the validated Chevrin Pediatric Sleep Questionnaire (PSQ) to all patients over the age of 36 months seen for comprehensive interdisciplinary team evaluation. 6 The PSQ is an easily administered tool and has been validated to serve as a surrogate to identify children with CL/P who may be at risk for SDB.4,6,7 At our institution, children with positive sleep scores (defined as a PSQ score >8) are referred for evaluation by a sleep specialist and formal polysomnography (PSG) testing. Although PSG is the gold-standard in diagnosis of SDB, there are many barriers that would preclude a formal polysomnogram for routine screening of SDB.
The aim of this study was to audit the outcomes using the PSQ to identify risk factors in children with non-syndromic CL/P who evidenced SDB as identified with positive PSQs (score >8), and to assess the outcome of care for those children.
Methods
Following Institutional Review Board approval, the medical records of all patients seen at our region's multidisciplinary cleft lip and palate center from January 1, 2015 to June 1, 2019 were retrospectively reviewed. Inclusion criteria included all patients older than the age of 36 months with a completed PSQ. PSQs were administered and filled out by the patient's primary caretaker at each multidisciplinary center visit or follow up. Patients with a history of a syndrome other than isolated Van der Woude syndrome, those with a diagnosis of Pierre Robin Sequence or micrognathia with known history of obstructed breathing, and subjects without a recorded sleep questionnaire were excluded from the final cohort. The following data were extracted and compiled into a single dataset: age, gender, body mass index (BMI), ICD 10 code cleft diagnosis, type of cleft (isolated cleft lip, isolated cleft palate, cleft palate and cleft lip; bilateral vs. unilateral), Veau classification, dental occlusion angle classification, nasal airway patency (left and right), University of Pittsburgh Weighted values for Speech Symptoms associated with VPI score, history of failure to thrive, ADD/ADHD diagnosed by a physician, history of learning disabilities, history of a palatoplasty, history of sphincter-pharyngoplasty or pharyngeal flap, PSG and results if applicable. In children with a PSG-confirmed diagnosis of OSA, treatment characteristics – use of nightly continuous positive airway pressure (CPAP), adenotonsillectomy (T&A), and/or septorhinoplasty – and subsequent post-treatment PSQ scores were collected. In the cohort of children who had positive PSQ but did not complete the recommended PSG, reasons for non-completion were determined, and subsequent PSQ scores and outcomes were recorded.
Descriptive statistics for the study cohort were calculated. Using a positive sleep questionnaire score (>8) as the primary outcome of interest, a univariate logistic regression analysis was conducted to assess the association between each risk factor and SDB. Odds ratio (OR) estimates with 95% confidence intervals (CI) were calculated for each risk factor. The association between PSQ scores and Apnea-Hypopnea Index (AHI) on subsequent PSG (when applicable) were tested using Pearson correlation. To assess the efficacy of treatment in children diagnosed with OSA via PSG, we analyzed how many children had normal questionnaire screening (<8), indicating improvement of symptoms on follow up after the intervention. All statistical analyses were performed using SAS v9.4 (SAS institute, Cary, NC). p < 0.05 was considered statistically significant.
Results
Demographics and Risk Factors
Two-hundred seventy-eight children were seen in our cleft clinic during the study period. Thirty-nine patients did not meet inclusion criteria and were excluded from our final analysis. Forty-three patients had PSQ scores greater than eight, herein referred to as positive or the SDB group. One hundred ninety-six patients had PSQ scores of less than 8.
With respect to demographics, the SDB group was not significantly different from the negative PSQ group. The mean age was 145 months (range: 36–216 months) and 127 months (range: 36–312 months), respectively. Genders were equally distributed in both groups. Of those with a positive PSQ, 65% were noted to have cleft lip and palate, 22% had an isolated cleft palate, and 13% had an isolated cleft lip. In the group with a negative PSQ, 43% had a cleft lip and palate, 40% had an isolated cleft palate, and 17% had an isolated cleft lip. Figure 1 illustrates these differences.
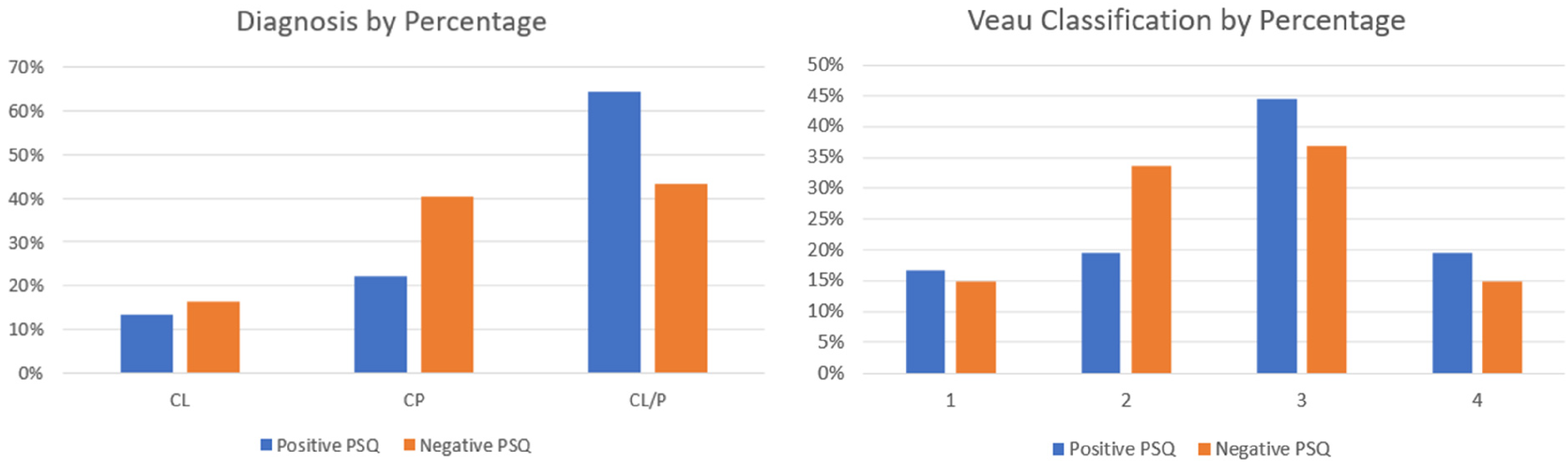
Left) Prevalence of cleft diagnosis comparing relative percentage of positive PSQ >8 and negative PSQ <8. Right) Prevalence of Veau classification comparing relative percentage of positive PSQ >8 and negative PSQ <8.
On univariate regression analysis, patients with positive sleep scores were 2.7 times more likely to have class III occlusion compared to those with negative sleep scores (OR = 2.65; CI: 1.21–5.81; p = 0.02). Of note, no significant differences in the type of cleft, Veau classification (I-IV), or surgical history of speech surgery (sphincter-pharyngoplasty, pharyngeal flap, or revision palatoplasty) was seen between those with positive and negatives PSQs. Twenty-seven children had a BMI > 25 (9%); elevated BMI was not found to be associated with positive sleep scores (OR = 1.05; CI: 0.99–1.12; p = 0.083). Patients with positive sleep questionnaires were nearly six times more likely to have a diagnosis of ADD/ADHD compared to those with negative sleep scores (OR = 5.90; CI: 2.64–13.2; p < 0.0001). The comprehensive univariate regression analysis is detailed in Table 1.
Univariate analysis estimating association of risk factors with a positive Pediatric Sleep Questionnaire score (> 8).
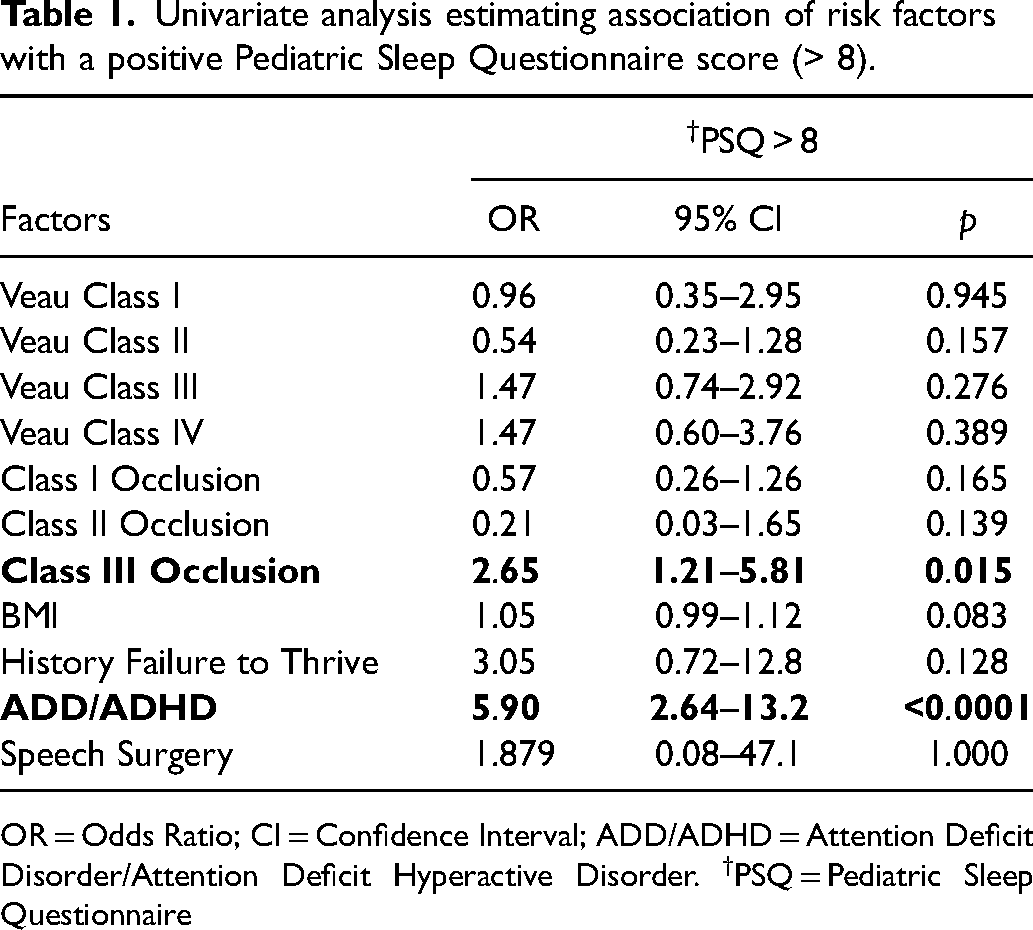
OR = Odds Ratio; CI = Confidence Interval; ADD/ADHD = Attention Deficit Disorder/Attention Deficit Hyperactive Disorder. †PSQ = Pediatric Sleep Questionnaire
All forty-three children with a positive PSQ were referred for specialist evaluation and assessment for polysomnography testing. Thirteen subjects never completed the appointment. Five patients were evaluated by the sleep specialist but deferred PSG testing. Twenty-five subjects with a positive PSQ went on to complete a polysomnography. Of those, 21 (84%) subjects were confirmed to have OSA (AHI > 1). The median AHI recorded was 3.1 (range: 0.2–20). There was no correlation found between the magnitude of PSQ scores and AHI (p = 0.162). Nine patients in the study cohort with normal PSQs underwent PSG testing due to parental preference and/or physician discretion. The median AHI in this group was noted to be 0.98 (range: 0.5–4.7), and 6 children were found to have OSA despite a negative sleep screen score. A flow diagram of our cohort through this care pathway is illustrated in Figure 2.
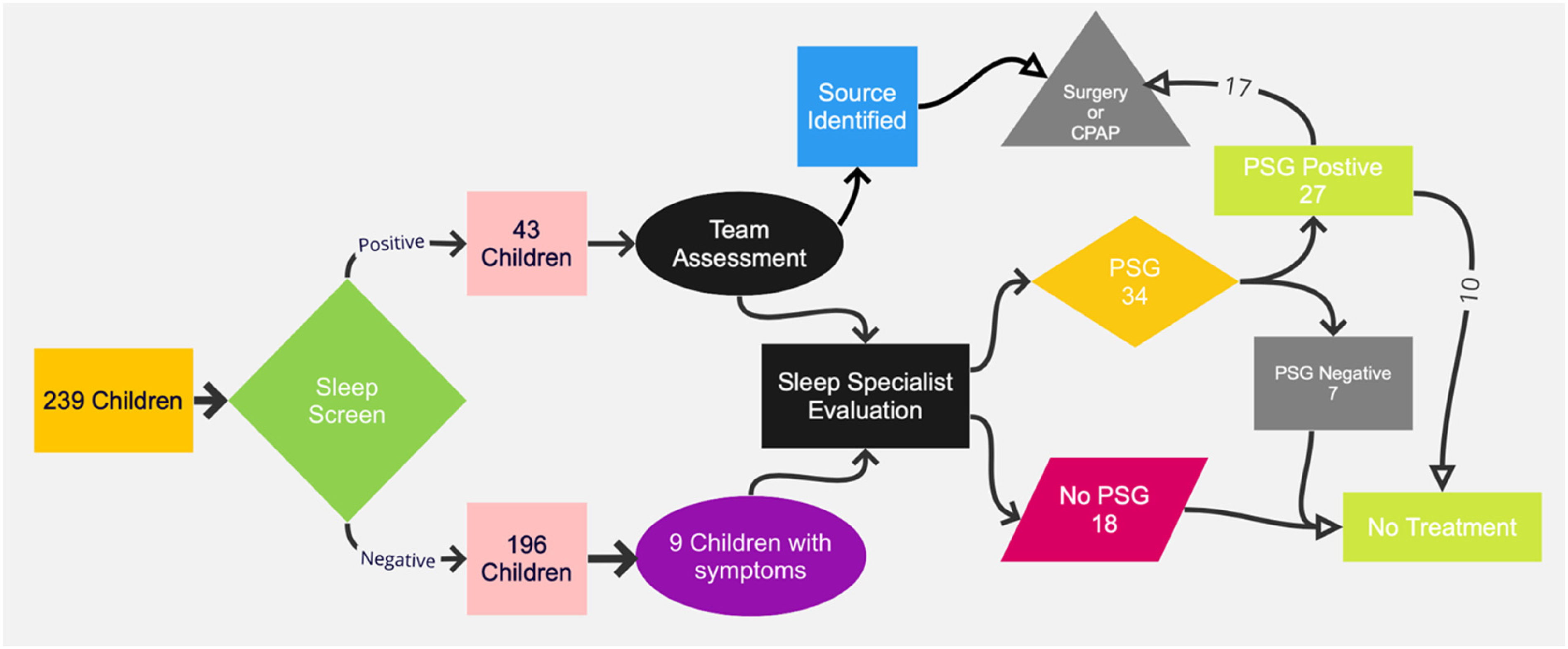
Flow diagram of all children evaluated in this study. There were 239 children screened, 43 had a score greater than 8, all of which were assessed in a team-based approach. If the source of SDB was not obvious, these children were referred for formal PSG, an additional 9 children with negative sleep screening scores were also referred. Of those referred, 34 completed the study, 27 were found to have OSA and 17 went on for treatment. Eighteen children referred did not undergo PSG, nor were they treated.
Three treatment modalities were utilized for patients at our center affected by SDB: adenotonsillectomy (T&A), septorhinoplasty, and/or CPAP. Choice of intervention was guided by the anatomic cause of the obstruction and polysomnography results. A shared decision-making model, incorporating the preferences of the family and the recommendations of the cleft team were utilized for each patient. Of the 27 children with PSG-confirmed OSA (21 with positive PSQ and 6 with negative PSQ), 17 patients received one or more treatment modalities for their SDB (63%). Thirteen were treated with a adenotonsillectomy, and 1 child underwent both adenotonsillectomy and septorhinoplasty. Three patients utilized CPAP therapy alone. Ten families chose not to receive treatment for their OSA.
Follow-up PSQ scores were available for 12 of the 17 children with PSG-confirmed OSA following treatment; 9 subjects (75%) had subsequent negative PSQ scores on follow up and 3 subjects still had positive sleep screening scores. In the 10 patients who did not receive treatment, subsequent sleep screen score was only available for one child, which was negative.
Discussion
The increased prevalence of SDB in persons with CL/CP is extensively supported in the literature, as are the adverse effects of SDB on the health and well-being of affected children.2,3,5 To the authors’ knowledge, this is the first report to assess the risk and magnitude of clinical factors associated with SDB symptomatology in the CL/P population using positive sleep screenings as an outcome metric. Furthermore, this report adds to the current body of literature by reporting success rates of various treatment options for SDB in non-syndromic children with CL/CP.
While polysomnography remains the current standard for diagnosis of OSA, various obstacles to care may prevent patients from obtaining formal testing. In-laboratory PSG testing requires patients to spend the night in a sleep facility, uses expensive equipment, and requires the presence of a trained technologist. A limited number of available sleep labs, the high cost of testing and insurance coverage may render PSG impractical for certain patients. 8 These obstacles may be even more pronounced for families impacted by healthcare disparities.9,10 As a result, routine PSG for screening may not be feasible, and the need for novel and surrogate screening tools, such as the PSQ, have emerged. Our center administers the PSQ at each multidisciplinary team visit and uses these datapoints as both a maker of potential issues with sleep and to observe improvement in symptomology following intervention.
In our analysis, we observed that patients with positive PSQs had 2.7 times increased odds of having class III occlusion compared to those with negative screens. Prior investigations have demonstrated that midface hypoplasia and retrognathic mandibular position are associated with SDB, particularly in children with syndromic craniofacial anomalies.2,5,11 In our SDB cohort with class III occlusion, 84% were noted to also display maxillary retrusion. Class II occlusion was not significantly associated with positive PSQ scores in our study, which most likely reflects exclusion of children with Pierre Robin Sequence and known airway obstruction in infancy.
SDB was found in some children with all cleft classifications, including those with isolated cleft lip, indicating routine screening of all children is valuable. However, a screening questionnaire does not negate the value of parental observation. In this group, we found that parental concerns regarding observed sleep was accurate 67% of the time in identifying OSA in the context of a normal PSQ. Parental observation of apneic breathing, in absence of other symptoms, may warrant formal PSG study as well.
Patients in our cohort with positive sleep screen questionnaires were nearly 6 times more likely to have a diagnosis of ADD/ADHD compared to the controls. This aligns with a multitude of reports concluding that patients afflicted with SDB have a higher incidence of learning and attention disabilities.3,5,9,10 Additional studies have demonstrated that children with cleft palates display higher rates of cognitive impairments compared to unaffected children.12–15 While causality has not been demonstrated, the clear association with problems with behavior, learning and cognitive function support early recognition and treatment of SDB.
Treatment guidelines for SDB exist for children without CL/P; however, there are no clear recommendations for children with cleft lip and or palate. 3 Analyzing post-treatment PSGs in patients with CL/P and OSA, Muntz et al. concluded that adenotonsillectomy is the most effective modality. 11 Similar to our own study, these findings are limited by the small cohort size and lack of standardized definitions of treatment success. Our treatment is tailored to the anatomic issue. In many cases, this is tonsillar or adenoid hypertrophy, and tonsillectomy/adenoidectomy is the treatment of choice. While there is concern that adenoidectomy may precipitate VPI, we consider adequate airway to be the more pressing priority. Individualized surgical planning, which might include tonsillectomy only, or partial adenoidectomy, is important. Parents are fully informed about this risk, and speech is monitored closely postoperatively. In this cohort, no child undergoing adenoidectomy required secondary speech surgery. Patients with CL/P can have significant septal deviation. Our preference is to wait until near full nasal growth to correct this when possible. In cases in which surgical correction is inadvisable or when surgery is declined, CPAP may be attempted. Although only a subset of our patients underwent treatment for OSA, the subsequent reduction in PSQ scores suggests that intervention may improve symptoms in majority of patients.
There are additional considerations in analyzing treatment outcomes in this population. The heterogeneous and overlapping etiologies of OSA may confound inferences on treatment effectiveness. For example, adenotonsillar hypertrophy may resolve with age in the absence of treatment. In the CHAT study by Macus et al., children with OSA were randomized to early adenotonsillectomy or close observation without intervention. The authors found that 46% of children had significant improvement in symptoms and quality of life without intervention over a 7-month study period. 16 Moreover, interventions are likely influenced by caregiver preference. While CPAP may be an effective treatment, in our experience it is infrequently chosen by families, and compliance can be problematic.
Of interest, nine children were diagnosed with OSA through PSG, but declined recommended treatment. Within this group, one child showed improvement in their follow up sleep score questionnaire, with a score < 8. The most common reason for deferment of treatment was parental choice for no surgery. An additional reason was a diagnosis of nasal septal deviation in a child who was felt to be too young for septoplasty, and parental refusal of CPAP. In those circumstances, treatment was planned for the early teen years.
There are several limitations to this study that should be acknowledged. Most notably, our analysis utilizes the assumption that a positive PSQ signifies a patient with SDB. The PSQ has previously been demonstrated to predict moderate-to-severe OSA in otherwise healthy children with a sensitivity of 83% and a specificity of 87%. 6 Silvestre et al. was the first to support its utility in the non-syndromic CL/P population. 4 In a recent article, Solis et al. calculated the sensitivity and specificity of PSQ for identifying AHI ≥ 5 on PSG in children with non-syndromic palatal clefting was 100% and 50%, respectively. 17 In our cohort of patients with positive PSQs who underwent subsequent PSG, 84% were found to have OSA. Nonetheless, false negative PSQs may underestimate SDB in our cohort. The sensitivity and specificity of the PSQ in our cohort cannot be calculated without all patients undergoing PSG testing. Future prospective studies with formal PSG testing in both positive and negative PSQ cohorts should be performed to estimate high-fidelity statistical parameters of the screening.
Conclusions
It is imperative that children with CL/P are screened for SBD, since untreated disease is associated with negative sleep, health, and quality of life endpoints. In this retrospective, single center cohort of children with CL/P, routine screening for SDB identified a high percentage at risk, and subsequent polysomnography supported the diagnosis of OSA in 84% of these patients. This group had a higher prevalence of ADD and/or ADHD in contrast to their peers. While micrognathia and class II dental have previously been identified as risk factors for obstructive apnea, our study demonstrated that patients with class III occlusion and maxillary retrusion are also likely to have SDB. In addition, parental observation of obstructed breathing, even with a normal PSQ, was accurate in the majority of patients in this study. A high index of suspicion is warranted all children with CL/P and the results of the PSQ may aid in shared decision making. Additional investigation is required to better evaluate treatment outcomes and guide future recommendations in this unique patient population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was approved by the Cooper University Hospital Institutional Review Board – ID Number 16–041 and approved on 10/13/2016. All patients and/or their guardians provide consent for participation in the study on their first cleft and craniofacial multidisciplinary care visit.
The data presented in this report has not been published elsewhere. The data herein was presented in-part at Plastic Surgery the Meeting 2020 and Northeastern Society of Plastic Surgery 2022.